

Key Points
Questions
Among active military with posttraumatic stress disorder (PTSD), are 10 sessions of prolonged exposure therapy (a trauma-focused cognitive behavioral therapy) delivered over 2 weeks (massed therapy) more effective than minimal contact and noninferior to 10 sessions delivered over 8 weeks (spaced therapy) for reducing PTSD symptom severity, and does spaced therapy reduce PTSD symptom severity more than present-centered therapy (PCT)?
Findings
In this randomized clinical trial (N = 366 active military with PTSD), massed therapy showed greater decrease in PTSD symptom severity than minimal contact and was noninferior to spaced therapy. There were no differences in PTSD symptom severity reduction between spaced therapy and PCT.
Meaning
Massed therapy was noninferior to spaced therapy for reducing PTSD symptoms in active military personnel, although the reductions in PTSD symptom severity with all treatments were relatively modest.
Abstract
Importance
Effective and efficient treatment is needed for posttraumatic stress disorder (PTSD) in active duty military personnel.
Objective
To examine the effects of massed prolonged exposure therapy (massed therapy), spaced prolonged exposure therapy (spaced therapy), present-centered therapy (PCT), and a minimal-contact control (MCC) on PTSD severity.
Design, Setting, and Participants
Randomized clinical trial conducted at Fort Hood, Texas, from January 2011 through July 2016 and enrolling 370 military personnel with PTSD who had returned from Iraq, Afghanistan, or both. Final follow-up was July 11, 2016.
Interventions
Prolonged exposure therapy, cognitive behavioral therapy involving exposure to trauma memories/reminders, administered as massed therapy (n = 110; 10 sessions over 2 weeks) or spaced therapy (n = 109; 10 sessions over 8 weeks); PCT, a non–trauma-focused therapy involving identifying/discussing daily stressors (n = 107; 10 sessions over 8 weeks); or MCC, telephone calls from therapists (n = 40; once weekly for 4 weeks).
Main Outcomes and Measures
Outcomes were assessed before and after treatment and at 2-week, 12-week, and 6-month follow-up. Primary outcome was interviewer-assessed PTSD symptom severity, measured by the PTSD Symptom Scale–Interview (PSS-I; range, 0-51; higher scores indicate greater PTSD severity; MCID, 3.18), used to assess efficacy of massed therapy at 2 weeks posttreatment vs MCC at week 4; noninferiority of massed therapy vs spaced therapy at 2 weeks and 12 weeks posttreatment (noninferiority margin, 50% [2.3 points on PSS-I, with 1-sided α = .05]); and efficacy of spaced therapy vs PCT at posttreatment.
Results
Among 370 randomized participants, data were analyzed for 366 (mean age, 32.7 [SD, 7.3] years; 44 women [12.0%]; mean baseline PSS-I score, 25.49 [6.36]), and 216 (59.0%) completed the study. At 2 weeks posttreatment, mean PSS-I score was 17.62 (mean decrease from baseline, 7.13) for massed therapy and 21.41 (mean decrease, 3.43) for MCC (difference in decrease, 3.70 [95% CI,0.72 to 6.68]; P = .02). At 2 weeks posttreatment, mean PSS-I score was 18.03 for spaced therapy (decrease, 7.29; difference in means vs massed therapy, 0.79 [1-sided 95% CI, −∞ to 2.29; P = .049 for noninferiority]) and at 12 weeks posttreatment was 18.88 for massed therapy (decrease, 6.32) and 18.34 for spaced therapy (decrease, 6.97; difference, 0.55 [1-sided 95% CI, −∞ to 2.05; P = .03 for noninferiority]). At posttreatment, PSS-I scores for PCT were 18.65 (decrease, 7.31; difference in decrease vs spaced therapy, 0.10 [95% CI, −2.48 to 2.27]; P = .93).
Conclusions and Relevance
Among active duty military personnel with PTSD, massed therapy (10 sessions over 2 weeks) reduced PTSD symptom severity more than MCC at 2-week follow-up and was noninferior to spaced therapy (10 sessions over 8 weeks), and there was no significant difference between spaced therapy and PCT. The reductions in PTSD symptom severity with all treatments were relatively modest, suggesting that further research is needed to determine the clinical importance of these findings.
Trial Registration
clinicaltrials.gov Identifier: NCT01049516
This randomized trial compared the effects of prolonged exposure therapy (10 sessions over 2 weeks vs 8 weeks) vs present-centered therapy vs minimal contact on posttraumatic stress disorder (PTSD) symptom severity among active duty military personnel.
Introduction
Posttraumatic stress disorder (PTSD) affects 10% to 20% of military personnel returning from deployments to Iraq and Afghanistan1,2,3 and is often chronic and debilitating.4,5 The psychological and physical toll of PTSD is substantial,6 highlighting the need to develop effective treatments. Prolonged exposure therapy for PTSD is a manualized, trauma-focused cognitive behavioral therapy that has empirical support in civilians7 and veterans.8,9 However, knowledge about the efficacy of prolonged exposure therapy among active duty military personnel is limited to case studies.10 One barrier to implementation of prolonged exposured therapy in the military is treatment length (8-15 weeks), which can conflict with military obligations. A shorter course of therapy could hasten amelioration of PTSD, with the added benefit of facilitating military readiness. Massed (daily) prolonged exposure therapy (massed therapy) has been demonstrated to be as effective as weekly sessions for treatment of agoraphobia,11 obsessive-compulsive disorder,12 and panic disorder.13,14 A randomized clinical trial (RCT) in civilians with PTSD found 1 week of daily cognitive therapy equivalent to 3 months of weekly sessions.15 Thus, massed therapy was expected to be noninferior to typical spaced prolonged exposure therapy (spaced therapy).
In the current RCT, it was hypothesized that, among active duty military with PTSD, (1) massed therapy would result in lower symptom severity than a minimal-contact control (MCC) condition at 2-week follow-up (given the intensity of massed therapy, 10 sessions delivered over 2 weeks, its effects were hypothesized to increase through 2 weeks after end of treatment); (2) massed therapy would be noninferior to spaced therapy (10 sessions delivered over 8 weeks, an established treatment, although never tested in an active duty sample) at 2-week and 12-week follow-ups; and (3) spaced therapy would result in lower symptom severity than present-centered therapy (PCT; 10 sessions delivered over 8 weeks) at posttreatment assessment.
Methods
Institutional review boards at Brooke Army Medical Center, University of Texas Health Science Center at San Antonio, and University of Pennsylvania approved the protocol. Participants provided written informed consent and self-reported their race, ethnicity, and other demographic characteristics to permit evaluation of the representativeness of the sample. The study protocol and statistical analysis plan are included in the Supplement.
Participants
Inclusion criteria were active duty military, activated Reservist, activated National Guard, or veterans who had deployed to Operation Enduring Freedom/Operation Iraqi Freedom/Operation New Dawn, ages 18 to 65 years; PTSD diagnosis according to the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR),16 assessed via PTSD Symptom Scale Interview (PSS-I)17; exposure to a DSM-IV-TR criterion A combat-related traumatic event (PTSD could be indexed to a noncombat-related event); and command support to attend treatment. Exclusion criteria were current bipolar or psychotic disorders, alcohol dependence, moderate to severe traumatic brain injury, suicidal ideation, or other disorders warranting immediate attention.
Procedures
The randomization sequence was entered by a study statistician into a secure, web-based application using SAS version 9.4 (SAS Institute Inc), which was accessed by the project coordinator on enrollment of each participant. Randomization was originally planned as 3:11:11:11 for MCC:massed therapy:spaced therapy:PCT. On January 5, 2012, enrollment in MCC was accelerated by changing the ratio to 1:1:1:1 to allow for preliminary massed therapy vs MCC comparison per Department of Defense request. After 40 participants were randomized to receive MCC, randomization to MCC was discontinued on March 19, 2014, and subsequent participants were assigned to receive massed therapy, spaced therapy, or PCT (1:1:1). Sensitivity analyses were performed to determine if the results were affected by the different randomization patterns. Randomization pattern was dummy coded and then added as a moderator to the analyses. There were no significant main effects or interactions involving randomization pattern, suggesting that the results did not differ between randomization patterns. On September 11, 2015, the analyses were presented to the Department of Defense external advisory board for review. The study team decided to publish the results of the entire study concurrently.
PTSD symptom severity was assessed by independent evaluators blinded to treatment condition, before and after treatment, and at 2-week, 12-week, and 6-month follow-up. The MCC condition terminated at 2-week follow-up. Symptom severity was also assessed every session by self-report for spaced therapy and PCT, and every other session for massed therapy. After the 2-week follow-up, participants in the MCC group were offered their choice of the other treatments. Data were collected from January 2011 to July 2016, when target enrollment was met and the final data point was collected.
Primary PTSD Measure: PTSD Symptom Scale–Interview
The PTSD Symptom Scale–Interview (PSS-I)17 is a 17-item clinical interview that evaluates DSM-IV PTSD symptom frequency and severity and can provide DSM-IV-TR PTSD diagnosis (score range, 0-51; higher scores indicate greater PTSD symptom severity). Test-retest reliability (0.80) and interrater reliability (κ = 0.91) are excellent.17 In the current sample, internal consistency averaged α = .79.
The minimal clinically important difference (MCID) has not been previously established for the PSS-I. As recommended,18 the MCID for PTSD was calculated as one-half of the SD at baseline (ie, one-half of 6.36, or 3.18). The PSS-I was used to assess PTSD symptom severity and PTSD diagnostic status.
Secondary PTSD Measure: PTSD Checklist–Stressor-Specific
The PTSD Checklist–Stressor-Specific (PCL-S)19 is a 17-item self-report measure assessing PTSD severity (score range, 17-85; higher scores indicate greater PTSD severity). Internal consistency is α = .89 to .97, and test-retest reliability is 0.96 at 2 to 3 days. The internal consistency for the present sample was α = .88.19 The MCID for the PCL-S is 7.9.20
Additional Measures
Veterans RAND 12-Item Health Survey
The Veterans RAND 12-Item Health Survey (VR-12)21 is a 12-item measure that includes physical and mental components, which were used as baseline covariates in the analyses.
Adverse Events
Clinically significant untoward changes in physical or mental health were recorded by study staff as possible adverse events for safety evaluation.
Interventions
Massed Prolonged Exposure Therapy
Prolonged exposure therapy22 is a manualized cognitive behavioral therapy consisting of imaginal exposure (repeated recounting of the most disturbing traumatic memory) followed by processing thoughts and feelings related to the imaginal experience; in-vivo exposure (approaching trauma-related situations), psychoeducation about PTSD, and controlled breathing training. Between sessions, participants listened to audio recordings of the imaginal recounting daily and completed in-vivo exercises. Daily sessions were administered on 10 consecutive weekdays over a 2-week period.
Spaced Prolonged Exposure Therapy
Spaced therapy was implemented in the same way as massed therapy, except that the 10 sessions were delivered over 8 weeks: 6 once weekly, and 2 twice weekly during the first and last weeks. This is consistent with how prolonged exposure therapy has been implemented with civilians and veterans in previous studies; prolonged exposure therapy is typically delivered in 8 to 15 once- or twice-weekly sessions.
Present-Centered Therapy
Present-centered therapy is a non–trauma-focused, manualized treatment that controls for nonspecific therapeutic factors.23 Ten 90-minute sessions were scheduled similarly to spaced therapy and focused on current life problems that may or may not be PTSD-related. Therapists helped participants identify stressors and discussed them in a supportive, nondirective manner.
Minimal-Contact Control
The MCC condition consisted of 10- to 15-minute therapist telephone calls once weekly for 4 weeks. Participants were asked about their well-being, offered support as needed, and received contact information in case symptoms worsened.
Therapist Training and Supervision
Therapists were 2 credentialed psychologists and 1 credentialed social worker who had completed a 4-day prolonged exposure therapy workshop, a 2-day PCT workshop, and 2 supervised cases of prolonged exposure therapy and PCT. Therapy sessions were videotaped for purposes of supervision and treatment-adherence monitoring. Weekly consultation calls for prolonged exposure therapy and PCT were conducted separately.
Data Analysis
Sample sizes were determined before data collection using NCSS-PASS version 2005 (NCSS). A sample size of 110 was calculated for massed therapy and spaced therapy to achieve power 90% or greater for their noninferiority test (assuming a standardized difference of d = 0.4 [2.5 units on PSS-I]).24 Sample size for PCT was set to equal that for spaced therapy. A sample size of 40 for MCC was calculated to provide power 90% or greater to detect a medium effect size (d = 0.50 [3.1 units on the PSS-I]).25 Pattern mixture modeling was used to evaluate the effects of missing data26 and to provide a sensitivity analysis for the effect of missing data. This approach compares growth curve parameters of participants with complete vs missing data.
Linear mixed models and generalized linear mixed models were used to analyze the data, using SPSS version 23 (IBM SPSS). These models are intent-to-treat and calculate results based on available data without imputation of missing data.27 Piecewise models, with separate slopes during treatment and follow-up, were used for analyses. Per protocol, analyses included the covariates baseline level of outcome, age, sex, and baseline mental and physical functioning. In each analysis, nonsignificant covariates (defined as P > .05) were removed and final models recomputed.
Significance for the superiority tests (hypothesis 1 [massed therapy would be more effective that MCC], and hypothesis 3 [spaced therapy would be more effective than PCT]) at the primary assessment points was set at P < .05 (2-sided). Superiority tests were conducted by examining differences between treatment conditions in the decrease in symptom severity from baseline (as indicated by the treatment × time interaction), and treatment condition differences at the relevant assessment point. Follow-up analyses examining each hypothesis at all posttreatment assessments were corrected for multiple tests using the Benjamini-Hochberg correction.28
For hypothesis 2 (massed therapy would be noninferior to spaced therapy), a noninferiority analysis was conducted, with the 1-sided α set at .05. To be noninferior, the upper bound of the 1-sided 95% CI of the difference between treatments must be less than the noninferiority margin. In noninferiority trials, the noninferiority margin should be a proportion of the difference between the effect of the established treatment (spaced therapy) and the control group (MCC).29 To be conservative, 50% of the posttreatment effect of the established treatment was used,29 which was smaller than the MCID for the primary outcome (PSS-I) and the secondary outcome (PCL-S). The efficacy of spaced therapy has not previously been established in active military personnel.
Effect sizes were calculated following the method of Feingold,30 or t-to-d conversion, as appropriate.
Results
Preliminary Analyses
Participants were 370 military personnel at Fort Hood, Texas. Four participants were removed from the analyses; data analyses included 366 participants. Figure 1 shows patient flow and participation in the trial. Demographic characteristics are reported in Table 1. Means for all outcomes at all end points are reported in Table 2. During treatment, the number who did not complete their assigned treatment was n = 0 for MCC, n = 15 (13.6%) for massed prolonged exposure therapy, n = 27 (24.8%) for spaced prolonged exposure therapy, and n = 13 (12.1%) for PCT. Of the 27 who did not complete spaced prolonged exposure, 1 mistakenly received massed prolonged exposure therapy and 1 was withdrawn from the study by the study team before session 2 for no longer meeting study criteria. Thus, there were 25 dropouts in spaced prolonged exposure (no significant differences in dropout among active treatments). At 6-month follow-up, dropout was n = 48 (43.6%) for massed therapy, n = 53 (48.6%) for spaced therapy, and n = 48 (44.9%) for PCT (no significant group differences). Participants with missing data did not significantly differ from completers on baseline variables. Further, pattern mixture modeling found no significant differences in the change in outcome over time between participants with missing data and those without missing data.
Figure 1. Flow of Participants Through the Study.
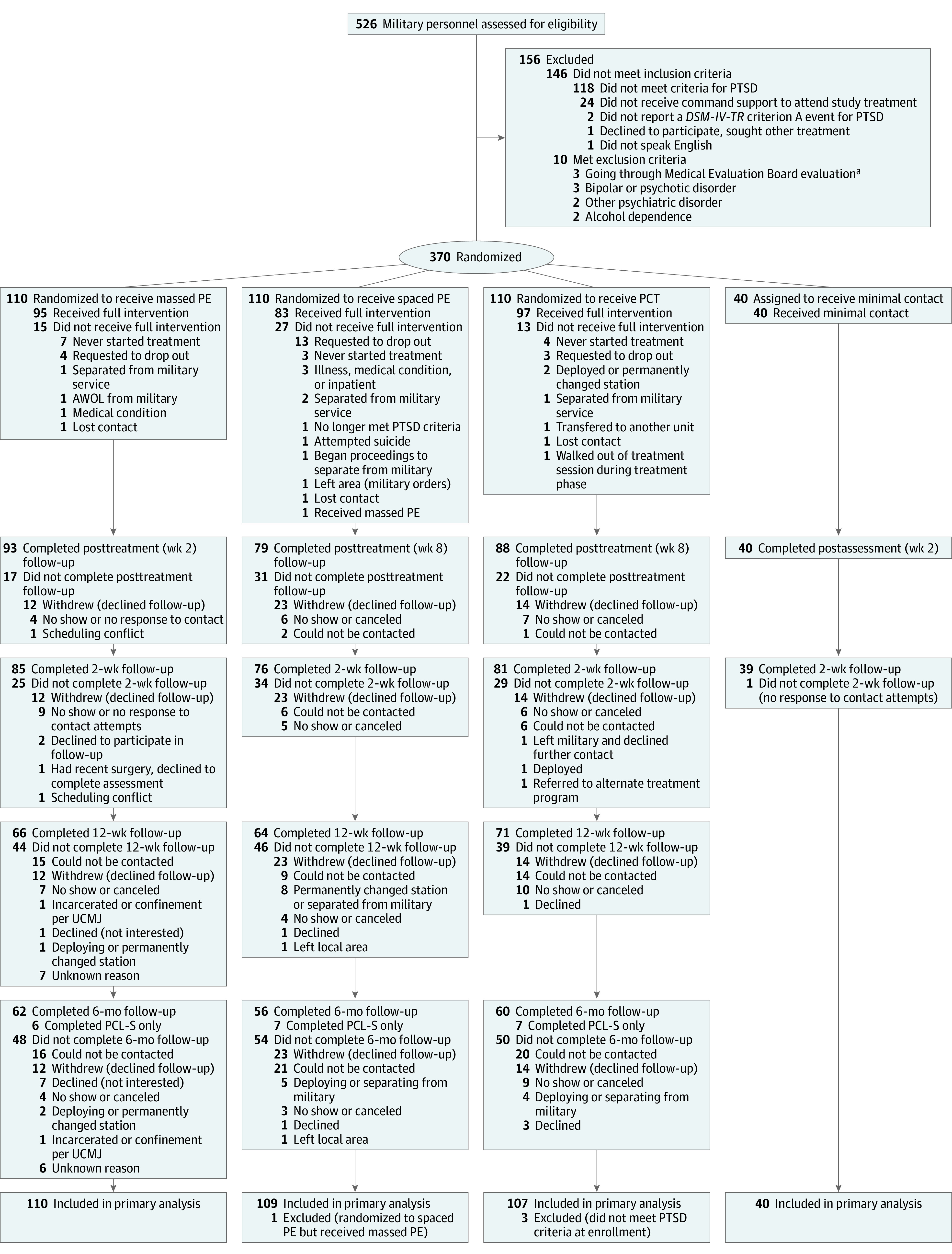
PCL-S indicates PTSD Checklist–Stressor-Specific; PCT, present-centered therapy; PE, prolonged exposure therapy; UCMJ, Uniform Code of Military Justice.
aA formal evaluation to determine whether a medical condition will impede a service member’s ability to continue serving in full duty capacity in his or her office, grade, or rank.
Table 1. Demographic and Clinical Characteristics of Participants by Treatment Condition.
| No. (%) | ||||
|---|---|---|---|---|
| Prolonged Exposure Therapy | PCT (n = 107) | MCC (n = 40) | ||
| Massed (n = 110) | Spaced (n = 109) | |||
| Demographic Characteristics | ||||
| Age, mean (SD), y | 32.65 (7.54) | 32.89 (7.05) | 32.54 (7.45) | 32.70 (7.68) |
| Sex | ||||
| Men | 94 (85.5) | 99 (90.8) | 91 (85.0) | 38 (95.0) |
| Women | 16 (14.5) | 10 (9.2) | 16 (15.0) | 2 (5.0) |
| Marital status | ||||
| Not married | 34 (30.9) | 28 (25.7) | 31 (29.0) | 11 (27.5) |
| Married or cohabiting | 76 (69.1) | 81 (74.3) | 76 (71.0) | 29 (72.5) |
| Education | ||||
| High school | 26 (23.6) | 38 (34.9) | 32 (29.9) | 21 (52.5) |
| College experience | 82 (74.5) | 69 (63.3) | 72 (67.3) | 18 (45.0) |
| Postgraduate | 2 (1.8) | 2 (1.8) | 3 (2.8) | 1 (2.5) |
| Ethnicity | ||||
| Hispanic | 19 (17.3) | 20 (18.3) | 24 (22.4) | 8 (20.0) |
| Non-Hispanic | 91 (82.7) | 89 (81.7) | 83 (77.6) | 32 (80.0) |
| Race | ||||
| Asian | 1 (0.9) | 2 (1.8) | 0 | 0 |
| Black | 29 (26.4) | 28 (25.7) | 22 (20.6) | 7 (17.5) |
| White | 67 (60.9) | 62 (56.9) | 68 (63.6) | 27 (67.5) |
| Other | 13 (11.8) | 17 (15.6) | 17 (15.9) | 6 (15.0) |
| Military Grade | ||||
| Enlisteda | ||||
| E-1 to E-3 | 0 | 2 (1.8) | 0 | 0 |
| E-4 to E-6 | 82 (74.5) | 86 (78.9) | 85 (81.7) | 32 (80.0) |
| E-7 to E-9 | 20 (18.2) | 18 (16.5) | 17 (16.3) | 7 (17.5) |
| Warrant officer | 3 (2.7) | 1 (0.9) | 1 (1.0) | 0 |
| Officer | 5 (4.5) | 2 (1.8) | 1 (1.0) | 1 (2.5) |
| No. of times deployed | ||||
| 1 or 2 | 64 (58.2) | 64 (58.7) | 66 (61.7) | 24 (60) |
| ≥3 | 46 (41.8) | 45 (41.3) | 41 (38.3) | 16 (40) |
| Time in military, mean (SD), y | 11.88 (6.57) | 11.01 (6.30) | 10.68 (6.19) | 10.53 (6.36) |
| Clinical Characteristics, Mean (SD) | ||||
| Depressive symptomsb | 29.12 (10.63) | 29.21 (9.61) | 27.59 (9.62) | 26.43 (9.44) |
| Alcohol usec | 5.10 (4.87) | 5.57 (5.15) | 5.37 (5.07) | 6.6 (5.19) |
| Physical functioningd | 40.57 (11.10) | 37.39 (11.24) | 39.79 (10.80) | 39.34 (11.63) |
| Mental functioningd | 31.71 (11.56) | 32.73 (9.88) | 33.11 (9.70) | 35.86 (10.91) |
| No. of psychotropic medications in use per de | ||||
| None | 60 (54.5) | 64 (58.7) | 55 (51.4) | 28 (70.0) |
| 1 | 27 (24.5) | 27 (24.8) | 23 (21.5) | 5 (12.5) |
| 2 | 18 (16.4) | 13 (11.9) | 17 (15.9) | 6 (15.0) |
| ≥3 | 5 (4.5) | 5 (4.6) | 12 (11.2) | 1 (2.5) |
Abbreviations: MCC, minimal-contact control; PCT, present-centered therapy.
E-1 to E-3, junior enlisted officers; E-4 to E-6, junior noncommissioned officers; E-7 to E-9, senior noncommissioned officers.
Assessed by Beck Depression Inventory II. Scores of 20-28 reflect moderate depressive symptoms; scores of 29 or greater reflect major depressive symptoms.
Assessed by Alcohol Use Disorders Identification Test; scores less than 8 indicate low risk of alcohol use disorder.
Assessed by Veterans RAND 12-Item Health Survey. Higher scores indicate better health.21
Obtained at baseline.
Table 2. Outcomes for the 4 Treatment Conditions for All Time Pointsa.
| Time Point | Mean (95% CI) | |||
|---|---|---|---|---|
| Prolonged Exposure Therapy | PCT (n = 107) | MCC (n = 40) | ||
| Massed (n = 110)b | Spaced (n = 109)c | |||
| Primary Outcome | ||||
| PSS-I | ||||
| Baseline | 25.20 (23.81-26.59) | 25.31 (23.95-26.66) | 25.96 (24.69-27.23) | 24.83 (23.00-26.66) |
| Posttreatment assessment | 18.80 (17.51-20.09) | 17.96 (16.60-19.33) | 18.65 (17.33-19.96) | 23.06 (21.23-24.89) |
| 2-wk follow-up | 18.82 (17.59-20.04) | 18.03 (16.71-19.34) | 18.69 (17.44-19.94) | 21.41 (19.56-23.26) |
| 12-wk follow-up | 18.88 (17.70-20.07) | 18.34 (17.04-19.64) | 18.91 (17.73-20.09) | NA |
| 6-mo follow-up | 18.97 (17.17-20.78) | 18.77 (16.88-20.67) | 19.21 (17.41-21.01) | NA |
| Secondary Outcomes | ||||
| PCL-S | ||||
| Baseline | 56.47 (54.46-58.48) | 55.37 (53.40-57.34) | 54.77 (52.82-56.73) | 55.38 (52.52-58.25) |
| Posttreatment assessment | 41.95 (40.04-43.86) | 40.98 (38.95-43.02) | 43.45 (41.51-45.38) | 51.58 (48.72-54.45) |
| 2-wk follow-up | 42.09 (40.24-43.94) | 41.20 (39.21-43.18) | 43.48 (41.56-45.40) | 49.25 (46.35-52.14) |
| 12-wk follow-up | 42.80 (40.94-44.65) | 42.25 (40.26-44.24) | 43.67 (41.48-45.87) | NA |
| 6-mo follow-up | 43.78 (41.26-46.31) | 43.72 (41.13-46.31) | 43.94 (40.71-47.16) | NA |
| Diagnosis of PTSD, % (95% CI) | ||||
| Baseline | 100 (NA) | 100 (NA) | 100 (NA) | 100 (NA) |
| Posttreatment assessment | 54.5 (46.9-62.0) | 51.4 (43.0-59.8) | 59.7 (51.1-67.7) | 80.0 (68.3-88.1) |
| 2-wk follow-up | 55.0 (48.0-61.8) | 52.3 (44.3-60.1) | 59.7 (51.8-67.2) | 77.1 (65.0-85.9) |
| 12-wk follow-up | 57.2 (50.7-63.5) | 56.7 (49.1-64.0) | 60.2 (52.9-67.1) | NA |
| 6-mo follow-up | 60.3 (48.6-70.9) | 62.7 (50.2-73.6) | 60.8 (48.3-72.1) | NA |
Abbreviations: MCC, minimal-contact control; NA, not applicable; PCL-S, PTSD Checklist–Stressor-Specific; PCT, present-centered therapy; PSS-I, Posttraumatic Stress Scale–Interview.
Data are from the mixed-model analyses (MLM). Because different pairs of groups were included in the analysis for different hypotheses, MLM calculated different covariances between groups and time points, resulting in slightly different estimated mean scores for the spaced prolonged exposure therapy group depending on the hypothesis (2 or 3) being tested. This did not occur for PCT or MCC, since they were only involved in 1 comparison each. For massed prolonged exposure therapy, the means for comparison with MCC were calculated from a subsample of 75 of the total (n = 110) because those 75 were recruited concurrently with the sample for MCC. The massed prolonged exposure therapy means for comparing massed therapy with spaced therapy were from the entire sample (n = 110) for massed therapy. For massed therapy, the elapsed time between baseline and the posttreatment assessment and follow-up assessments was 6 weeks less than for spaced prolonged exposure therapy and PCT, because the treatment phase in massed prolonged exposure therapy lasted 2 weeks, while the treatment phase for spaced prolonged exposure therapy and PCT lasted 8 weeks.
Data obtained from analysis of hypothesis 2.
Data obtained from analysis of hypothesis 2.
There were no significant treatment group differences on baseline variables.
Treatment Adherence
The mean number of sessions completed were 9.04 (SD, 2.60) for massed therapy, 8.59 (SD, 2.68) for spaced therapy, and 9.10 (SD, 2.53) for PCT. Participants in the MCC group completed a mean of 1.86 (SD, 0.35) calls during the first 2 weeks and 1.68 (SD, 0.64) the second 2 weeks. Three randomly selected videos from each participant were reviewed for treatment adherence by independent raters. Adherence was 96.36% for prolonged exposure therapy elements and 92.63% for PCT elements.
Massed Therapy vs MCC
Because MCC underwent accelerated recruitment, its sample was completed before completion of the full massed therapy sample. Thus, the sample for the massed therapy vs MCC analysis was limited to participants in the massed therapy group who were recruited and randomized during the same time frame as participants in the MCC group (n = 75 of n = 110 in the massed therapy group).
Primary Outcome
PSS-I scores decreased during treatment (ie, over 2 weeks) for massed therapy, then leveled off at 8 weeks (Figure 2A). Small decreases in PSS-I scores in the MCC group continued through follow-up. Decreases in PSS-I scores from baseline to 2-week follow-up (week 4) were significant for both massed therapy (decrease, 7.13; t216 = 7.66; P < .001; d = 1.04) and MCC (decrease, 3.43; t296 = 2.87; P = .004; d = 0.33); the decreases were significantly greater for massed therapy compared with MCC (treatment × time interaction, 3.70 [95% CI, 0.72 to 6.68]; t298 = 2.44; P = .02; d = 0.28) (Table 3). Participants in the massed therapy group had lower mean PSS-I scores than participants in the MCC group at 2-week follow-up (17.62 vs 21.41, respectively; difference, 3.79 [95% CI, 1.41 to 6.17]; t272 = 3.14; P = .002; d = 0.56) (Table 3).
Figure 2. Estimated Mean Scores for the Primary Outcome Measure (PSS-I) at All Time Points.
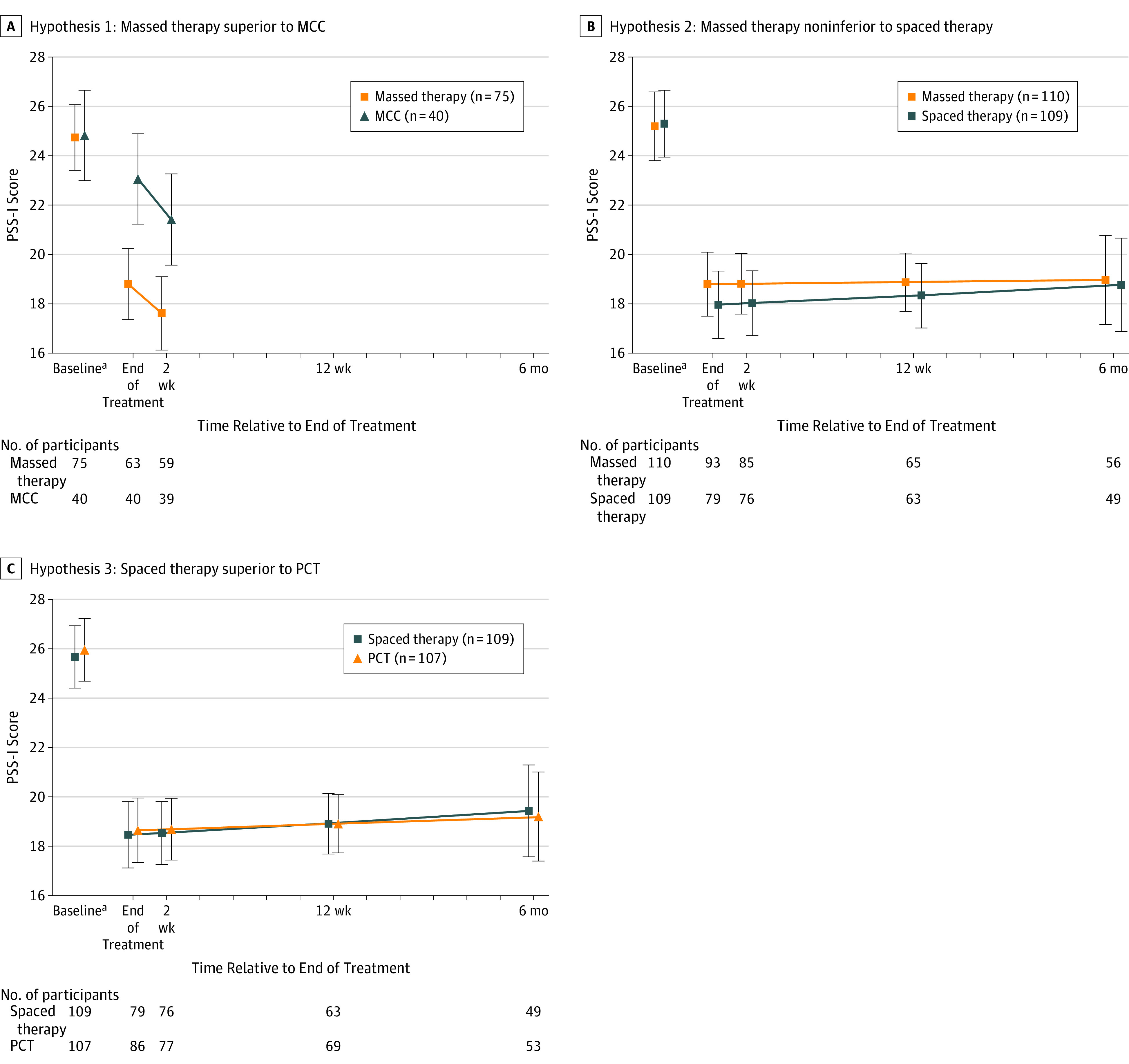
Piecewise models with separate slopes during treatment and follow-up were used for mixed-model analyses of Posttraumatic Stress Scale–Interview (PSS-I) scores, and the following variables were included as covariates: baseline PSS-I, age, sex, and baseline mental and physical functioning. Final models were recomputed by dropping nonsignificant covariates in each analysis. Data are from the mixed-model analyses (MLM). Because different pairs of groups were included in the analysis for different hypotheses, MLM calculated different covariances between groups and time points, resulting in slightly different estimated mean scores for the spaced prolonged exposure therapy (spaced therapy) group depending on the hypothesis (2 or 3) being tested. This did not occur for present-centered therapy (PCT) or minimal-contact control (MCC), since they were only involved in 1 comparison each. For massed prolonged exposure therapy (massed therapy), the means for comparison to MCC were calculated from a subsample of 75 of the total n=110 because those 75 were recruited concurrently with the sample for MCC. The massed therapy means for comparing massed therapy with spaced therapy were from the entire sample of n=110 for massed therapy. The full range of scores on the PSS-I is 0-51. Error bars indicate 95% CIs from the mixed-model analyses.
aThe elapsed time between baseline and end of treatment was 2 weeks for massed therapy and MCC and 8 weeks for spaced therapy and PCT.
Table 3. Mean PSS-I Scores (Primary Outcome) at the Primary Time Points for Hypothesis 1 (Massed Therapy Superior to Minimal-Contact Control)a.
| Time Point | Massed Prolonged Exposure Therapy (n = 75) | Minimal-Contact Control (n = 40) | Between-Group Difference in Change (95% CI) | P Value | ||
|---|---|---|---|---|---|---|
| Mean PSS-I Score (95% CI) | Within-Group Change (95% CI) | Mean PSS-I Score (95% CI) | Within-Group Change (95% CI) | |||
| Baseline | 24.74 (23.41-26.08) | 24.83 (23.00-26.66) | ||||
| 2-wk follow-up | 17.62 (16.12-19.11) | 7.13 (5.30-8.96) | 21.41 (19.56-23.26) | 3.43 (1.07-5.78) | 3.70 (0.72-6.68) | .02 |
Abbreviation: PSS-I, Posttraumatic Stress Scale–Interview.
Data are from the mixed-model analyses. For massed prolonged exposure therapy, the means for comparison with minimal-contact control (MCC) were calculated from a subsample of 75 of the total (n = 110) because those 75 were recruited concurrently with the sample for MCC.
Secondary Outcomes
Decreases in both PCL-S scores and the rate of PTSD diagnosis from baseline to 2-week follow-up were significant for massed therapy (PCL-S decrease, 15.52; t298 = 10.95; P < .001; d = 1.27; diagnosis decrease, 45.4%; t310 = 2.62; P = .009; d = 0.30), but only PCL-S score decreases were significant for MCC (PCL-S decrease, 6.13; t292 = 3.37; P = .001; d = 0.39) (Table 2). These decreases were significantly greater for massed therapy than for MCC on the PCL-S (treatment × time interaction, 9.38 [95% CI, 4.85 to 13.92]; t294 = 4.07; P < .001; d = 0.47), but massed therapy did not differ significantly from MCC on decreases in diagnosis. At 2-week follow-up, massed therapy had significantly lower mean PCL-S scores (40.28 vs 49.25 for MCC; difference, 8.96 [95% CI, 5.25 to 12.68]; t263 = 4.75; P < .001; d = 0.89) and lower mean rates of PTSD diagnosis (54.6% vs 77.1% for MCC; difference, 22.5% [95% CI, 7.5% to 32.8%]; t310 = 2.81; P = .005; d = .32) (Table 2).
Nineteen of the 75 participants in the massed therapy group (25.3%) reported a total of 25 adverse events during treatment; 12 of these adverse events were study-related. Thirteen of the 40 participants in the MCC group (32.5%) reported a total of 20 adverse events during treatment; 1 of these was study-related. Few participants experienced adverse events that resulted in emergency department visits or hospitalization during the intervention period (n = 3 [4%] participants for massed therapy, n = 4 [10%] for MCC); 1 suicide attempt occurred in the MCC group.
Massed Therapy vs Spaced Therapy
Primary Outcome
The difference in mean PSS-I scores between massed therapy and spaced therapy at the 2-week follow-up was 0.79 (massed therapy was worse than spaced therapy [1-sided 95% CI, −∞ to 2.29]; P = .049 for noninferiority) (Figure2B, Figure 3, and Table 4). The upper bound of the 1-sided 95% CI was less than the noninferiority margin of 2.3 (Figure 3), indicating that the comparison of massed therapy with spaced therapy met criteria for noninferiority at 2-week follow-up (4 weeks from treatment inception for massed therapy, 10 weeks for spaced therapy). At 12-week follow-up (14 weeks for massed therapy, 20 for spaced therapy), the difference in mean PSS-I scores between massed therapy and spaced therapy was 0.55 (1-sided 95% CI, −∞ to 2.05; P = .03 for noninferiority), meeting criteria for noninferiority at 12-week follow-up.
Figure 3. Difference Between Massed and Spaced Prolonged Exposure Therapy on Primary Outcome Measure (PSS-I) at 2-Week and 12-Week Follow-up.

Range of possible scores on the Posttraumatic Stress Scale–Interview (PSS-I), 0 to 51. Boxes indicate the mean difference between massed prolonged exposure therapy (massed therapy) and spaced prolonged exposure therapy (spaced therapy); error bars indicate the 1-sided 95% CIs around the means. For massed therapy to be noninferior to spaced therapy, the upper bound of the 1-sided 95% CI for the difference between treatments (massed therapy minus spaced therapy) must be less than the noninferiority margin (2.3, blue dotted line).
Table 4. Mean PSS-I Scores (Primary Outcome) at the Primary Time Points for Hypothesis 2 (Massed Therapy Noninferior to Spaced Therapy)a.
| Time Point | Massed Prolonged Exposure Therapy (n = 110) | Spaced Prolonged Exposure Therapy Group (n = 109) | Difference Between Means (95% CI) | P Value | ||
|---|---|---|---|---|---|---|
| Mean PSS-I Score (95% CI) | Within-Group Change (95% CI) | Mean PSS-I Score (95% CI) | Within-Group Change (95% CI) | |||
| Baseline | 25.20 (23.81 to 26.59) | 25.31 (23.95 to 26.66) | ||||
| 2-wk follow-up | 18.82 (17.59 to 20.04) | 6.38 (3.77 to 9.00) | 18.03 (16.71 to 19.34) | 7.29 (4.61 to 9.95) | 0.79 (−1.01 to 2.60)b | .39 |
| 12-wk follow-up | 18.88 (17.70 to 20.07) | 6.32 (3.74 to 8.89) | 18.34 (17.04 to 19.64) | 6.97 (4.31 to 9.62) | 0.55 (−1.23 to 2.32)c | .54 |
Abbreviation: PSS-I, Posttraumatic Stress Scale–Interview.
Data are from the mixed-model analyses (MLM). Because different pairs of groups were included in the analysis for different hypotheses, MLM calculated different covariances between groups and time points, resulting in slightly different estimated mean scores for the spaced therapy group depending on the hypothesis (2 or 3) being tested. The massed therapy means were from the entire sample (n = 110) for massed therapy. For massed therapy, the elapsed time between baseline and the posttreatment and follow-up assessments was 6 weeks less than for spaced therapy because the treatment phase for massed therapy lasted 2 weeks, while the treatment phase for spaced therapy lasted 8 weeks.
For the noninferiority analysis, the 1-sided 95% CI (see Methods) was −∞ to 2.29 (P = .049).
For the noninferiority analysis, the 1-sided 95% CI (see Methods) was −∞ to 2.05 (P = .03).
Secondary Outcomes
For the secondary outcomes, noninferiority margins were defined as 5.56 for change in PCL-S score and 14.3% for rate of PTSD diagnosis. At 2-week follow-up, the difference in PCL-S scores between massed therapy and spaced therapy was 0.90 (1-sided 95% CI, −∞ to 3.17]; P < .001 for noninferiority). The PTSD diagnosis difference was 2.7% (1-sided 95% CI, −∞ to 13.8%; P = .043 for noninferiority). At 12-week follow-up, the difference in PCL-S scores between massed therapy and spaced therapy was 0.55 (1-sided 95% CI, −∞ to 2.82; P < .001 for noninferiority). The difference in rate of PTSD diagnosis was 0.5% (1-sided 95% CI, −∞ to 11.5%; P = .02 for noninferiority). Since the 1-sided 95% CIs were less than the noninferiority margins, massed therapy was considered noninferior to spaced therapy for the secondary outcomes.
Noninferiority at Other Assessments
For the primary outcome (PSS-I), post hoc analyses revealed that the 1-sided 95% CI for the difference between massed therapy and spaced therapy was less than the noninferiority margin at posttreatment assessment and 6-month follow-up, suggesting noninferiority. Similarly, for the secondary outcomes, the 1-sided 95% CIs for the difference between treatments was less than their noninferiority margins at both posttreatment and 6-month follow-up.
A total of 59 participants in the spaced therapy group (54.1%) reported adverse events (115 events) during treatment, whereas 50 participants in the massed therapy group (46.7%) reported adverse events (96 events). The number of study-related adverse events was not significantly different in the spaced therapy vs massed therapy groups (23 vs 12, respectively; P = .04). During treatment, 7 participants in both the spaced therapy group (6.42% of participants) and the massed therapy group (6.36%) experienced adverse events that resulted in emergency department visits or hospitalization.
Spaced Therapy vs PCT
Primary Outcome
Decreases in PSS-I scores from baseline to posttreatment assessment (8 weeks after baseline) were significant for both spaced therapy (decrease, 7.21; t401 = 8.39; P < .001; d = 0.84) and PCT (decrease, 7.31;t394 = 8.62; P < .001; d = 0.87), and the decreases were not significantly different between conditions (treatment × time interaction, 0.10 [95% CI, −2.48 to 2.27]; t398 = 0.08; P = .93) (Table 5). Changes in mean levels of PSS-I did not differ significantly between the spaced therapy and PCT groups at posttreatment follow-up (ie, week 8) (Figure 2C).
Table 5. Mean PSS-I Scores (Primary Outcome) at the Primary Time Points for Hypothesis 3 (Spaced Therapy Superior to PCT)a.
| Time Point | Spaced Prolonged Exposure Therapy (n = 109) | PCT (n = 107) | Between-Group Difference in Change (95% CI) | P Value | ||
|---|---|---|---|---|---|---|
| Mean PSS-I Score (95% CI) | Within-Group Change (95% CI) | Mean PSS-I Score (95% CI) | Within-Group Change (95% CI) | |||
| Baseline | 25.67 (24.41 to 26.94) | 25.96 (24.69 to 27.23) | ||||
| Postttreatment assessment | 18.46 (17.12 to 19.81) | 7.21 (5.52 to 8.90) | 18.65 (17.33 to 19.96) | 7.31(5.64 to 8.96) | 0.10 (−2.48 to 2.27) | .93 |
Abbreviations: PCT, present-centered therapy; PSS-I, Posttraumatic Stress Scale–Interview.
Data are from the mixed-model analyses (MLM). Because different pairs of groups were included in the analysis for different hypotheses, MLM calculated different covariances between groups and time points, resulting in slightly different estimated mean scores for the spaced therapy group depending on the hypothesis (2 or 3) being tested. This did not occur for PCT.
Secondary Outcomes
Decreases from baseline to posttreatment follow-up for PCL-S scores and rates of PTSD diagnosis were significant in the spaced therapy group (PCL-S score decrease, 14.91; t1462 = 21.64; P < .001; d = 1.13; PTSD diagnosis decrease, 46.4%; t1155 = 7.04; P = <.001; d = 0.41) and the PCT group (PCL-S score decrease, 11.33; t1425 = 16.94; P < .001; d = 0.90; PTSD diagnosis decrease, 40.3%; t1155 = 6.35; P < .001; d = 0.37). The PCL-S score decrease for spaced therapy was significantly greater than the decrease for PCT (treatment × time interaction, 3.58 [95% CI, 1.70 to 5.47]; t1445 = 3.73; P < .001; d = 0.34), but the decrease in PTSD diagnosis was not significantly different between conditions. Consistent with these data, levels of PCL-S symptoms at posttreatment follow-up were lower for spaced therapy than for PCT (difference, 2.98 [95% CI, 0.23 to 5.72]; t262 = 2.14; P < .03; d = 0.26) (Table 2). However, there were no significant differences between conditions in PTSD diagnosis at posttreatment follow-up.
Spaced Therapy vs PCT at Follow-up Assessments
On the primary outcome (PSS-I), there were no significant differences between spaced therapy and PCT at any of the time points (Table 2), regardless of whether P values were corrected for multiple tests. Similarly, there were no significant treatment condition differences at any of the time points for the secondary outcomes (PCL-S and PTSD diagnosis). Fifty of the 107 participants in the PCT group (46.7%) reported 96 adverse events during treatment; 1 of these adverse events was study-related. Eight participants in the PCT group (7.5%) experienced adverse events that resulted in emergency department visits or hospitalization during the intervention.
Discussion
To our knowledge, this is the first RCT examining the efficacy of prolonged exposure therapy for combat-related PTSD in active duty military personnel, and the first to examine an intensive, massed prolonged exposure therapy format in this population. As hypothesized, massed therapy (10 sessions over 2 weeks) resulted in lower PTSD symptom severity than MCC at 2-week follow-up and was noninferior to spaced prolonged exposure therapy (10 sessions over 8 weeks) at posttreatment follow-up on reductions in PTSD symptom severity. A potential advantage of massed therapy was the low dropout rate (13.6%), increasing the possibility that patients will benefit from a full dose of treatment.31
The hypothesis that massed therapy would be noninferior to standard spaced therapy was supported. Thus, the concern that daily prolonged exposure therapy would be too emotionally taxing was not supported. The noninferiority of massed therapy to spaced therapy is particularly important for the military, because 2-week treatment not only is associated with more rapid symptom improvement but also may reduce interference with the demanding military schedule. In addition, military installations that lack clinicians with expertise in evidence-based treatments can more feasibly refer patients with PTSD to clinical experts at another installation for 2 weeks rather than for 2 to 3 months of standard treatment.
The hypothesis that spaced therapy would result in lower symptom severity than PCT was not supported. Spaced therapy was not significantly different than PCT on the primary outcome of interviewer-assessed PTSD symptom severity or on the rate of PTSD diagnosis. Spaced therapy did show lower self-reported PTSD symptom severity than PCT at posttreatment follow-up on a secondary outcome (PCL-S score), but this difference was small (3 points, less than one-half the MCID) and was nonsignificant at later follow-up. PCT as delivered in this study exceeds usual care at many military treatment facilities (eg, PCT had 90-minute weekly sessions, manualized treatment, problem solving). Nonetheless, the results suggest that trauma-focused treatment may not be necessary for PTSD improvement in active duty military personnel.
The efficacy of massed therapy and spaced therapy in this military sample was lower than previous findings for intensive cognitive therapy in civilians with PTSD.15 Similarly, the efficacy of spaced therapy in this study was lower than that of spaced therapy in civilians (7- vs 16-point reductions in PSS-I score32). These results are similar to 2 RCTs of cognitive processing therapy for PTSD in military personnel that also found that treatment was less efficacious for military personnel than for civilians.33,34 This suggests that well-established evidence-based treatments for PTSD may be less efficacious for active duty military personnel with PTSD and that modifications to these treatments, or alternative treatments, may be needed to achieve better outcomes. It is also possible that some active duty personnel had less time to complete treatment homework or may have more incentives to retain PTSD symptoms than other PTSD populations.
This study has several limitations. First, the design did not include an active 2-week comparison treatment for massed therapy. However, because this was the first study to evaluate intensive prolonged exposure therapy in military personnel, the use of an MCC condition was required by the Department of Defense external advisory board and supported by the respective institutional review boards. Second, participants in the massed therapy group may have lacked time to sufficiently practice homework assignments. Third, because participants were treatment seeking, the results are limited to military personnel seeking treatment for PTSD. Fourth, the dropout rate during treatment ranged from 12.1% (PCT) to 24.8% (spaced therapy), and only 59% of randomized participants completed the full study. Treatment effects likely would have been larger if a greater proportion of participants had completed the treatment portion of the study.
Conclusions
Among active duty military personnel with PTSD, massed prolonged exposure therapy (10 sessions delivered over 2 weeks) reduced PTSD symptom severity more than minimal contact control at 2-week follow-up and was noninferior to spaced prolonged exposure therapy (10 sessions delivered over 8 weeks), and there was no significant difference between spaced therapy and present-centered therapy. The reductions in PTSD symptom severity with all treatments were relatively modest, suggesting that further research is needed to determine the clinical importance of these findings.
Study Protocol and Statistical Analysis Plan
References
- 1.Hoge CW, Terhakopian A, Castro CA, Messer SC, Engel CC. Association of posttraumatic stress disorder with somatic symptoms, health care visits, and absenteeism among Iraq war veterans. Am J Psychiatry. 2007;164(1):150-153. [DOI] [PubMed] [Google Scholar]
- 2.Milliken CS, Auchterlonie JL, Hoge CW. Longitudinal assessment of mental health problems among active and reserve component soldiers returning from the Iraq war. JAMA. 2007;298(18):2141-2148. [DOI] [PubMed] [Google Scholar]
- 3.Gates MA, Holowka DW, Vasterling JJ, Keane TM, Marx BP, Rosen RC. Posttraumatic stress disorder in veterans and military personnel. Psychol Serv. 2012;9(4):361-382. [DOI] [PubMed] [Google Scholar]
- 4.Asnaani A, Reddy MK, Shea MT. The impact of PTSD symptoms on physical and mental health functioning in returning veterans. J Anxiety Disord. 2014;28(3):310-317. [DOI] [PubMed] [Google Scholar]
- 5.Kessler RC. Posttraumatic stress disorder: the burden to the individual and to society. J Clin Psychiatry. 2000;61(suppl 5):4-12. [PubMed] [Google Scholar]
- 6.Tanielian TL, Jaycox L. Invisible Wounds of War: Psychological and Cognitive Injuries, Their Consequences, and Services to Assist Recovery. Santa Monica, CA: RAND Corp; 2008. [Google Scholar]
- 7.Foa EB, Hembree EA, Cahill SP, et al. Randomized trial of prolonged exposure for posttraumatic stress disorder with and without cognitive restructuring. J Consult Clin Psychol. 2005;73(5):953-964. [DOI] [PubMed] [Google Scholar]
- 8.Schnurr PP, Friedman MJ, Engel CC, et al. Cognitive behavioral therapy for posttraumatic stress disorder in women. JAMA. 2007;297(8):820-830. [DOI] [PubMed] [Google Scholar]
- 9.Tuerk PW, Yoder M, Grubaugh A, Myrick H, Hamner M, Acierno R. Prolonged exposure therapy for combat-related posttraumatic stress disorder. J Anxiety Disord. 2011;25(3):397-403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Blount TH, Cigrang JA, Foa EB, Ford HL, Peterson AL. Intensive outpatient prolonged exposure for combat-related PTSD: a case study. Cogn Behav Pract. 2014;21(1):89-96. [Google Scholar]
- 11.Foa EB, Jameson JS, Turner RM, Payne LL. Massed vs. spaced exposure sessions in the treatment of agoraphobia. Behav Res Ther. 1980;18(4):333-338. [DOI] [PubMed] [Google Scholar]
- 12.Abramowitz JS, Foa EB, Franklin ME. Exposure and ritual prevention for obsessive-compulsive disorder: effects of intensive versus twice-weekly sessions. J Consult Clin Psychol. 2003;71(2):394-398. [DOI] [PubMed] [Google Scholar]
- 13.Deacon B, Abramowitz J. A pilot study of two-day cognitive-behavioral therapy for panic disorder. Behav Res Ther. 2006;44(6):807-817. [DOI] [PubMed] [Google Scholar]
- 14.Bohni MK, Spindler H, Arendt M, Hougaard E, Rosenberg NK. A randomized study of massed three-week cognitive behavioural therapy schedule for panic disorder. Acta Psychiatr Scand. 2009;120(3):187-195. [DOI] [PubMed] [Google Scholar]
- 15.Ehlers A, Hackmann A, Grey N, et al. A randomized controlled trial of 7-day intensive and standard weekly cognitive therapy for PTSD and emotion-focused supportive therapy. Am J Psychiatry. 2014;171(3):294-304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.American Psychiatric Association . Diagnostic and Statistical Manual of Mental Disorders. 4th ed, text revision. Washington, DC: American Psychiatric Association; 2000. [Google Scholar]
- 17.Foa EB, Riggs DS, Dancu CV, Rothbaum BO. Reliability and validity of a brief instrument for assessing post-traumatic stress disorder. J Trauma Stress. 1993;6(4):459-473. [Google Scholar]
- 18.Norman GR, Sloan JA, Wyrwich KW. Interpretation of changes in health-related quality of life. Med Care. 2003;41(5):582-592. [DOI] [PubMed] [Google Scholar]
- 19.Weathers FW, Litz BT, Herman DS, Huska JA, Keane TM. The PTSD Checklist (PCL): reliability, validity, and diagnostic utility. Paper presented at: 9th Annual Conference of the International Society for Traumatic Stress Studies; October 1993; San Antonio, TX. [Google Scholar]
- 20.Stefanovics EA, Rosenheck RA, Jones KM, Huang G, Krystal JH. Minimal clinically important differences (MCID) in assessing outcomes of post-traumatic stress disorder [published online June 21, 2017]. Psychiatr Q. 2017. doi: 10.1007/s11126-017-9522-y [DOI] [PubMed] [Google Scholar]
- 21.Selim AJ, Rogers W, Fleishman JA, et al. Updated U.S. population standard for the Veterans RAND 12-item Health Survey (VR-12). Qual Life Res. 2009;18(1):43-52. [DOI] [PubMed] [Google Scholar]
- 22.Foa EB, Hembree E, Rothbaum BO. Prolonged Exposure Therapy for PTSD: Therapist Guide. New York, NY: Oxford University Press; 2007. [Google Scholar]
- 23.Foa EB, Rothbaum BO, Riggs DS, Murdock TB. Treatment of posttraumatic stress disorder in rape victims. J Consult Clin Psychol. 1991;59(5):715-723. [DOI] [PubMed] [Google Scholar]
- 24.Julious SA. Sample sizes for clinical trials with normal data. Stat Med. 2004;23(12):1921-1986. [DOI] [PubMed] [Google Scholar]
- 25.Hedeker D, Gibbons RD, Waternaux C. Sample size estimation for longitudinal designs with attrition. J Educ Behav Stat. 1999;24(1):70-93. [Google Scholar]
- 26.Enders CK. Missing not at random models for latent growth curve analyses. Psychol Methods. 2011;16(1):1-16. [DOI] [PubMed] [Google Scholar]
- 27.Hedeker D, Gibbons R. Longitudinal Data Analysis. Hoboken, NJ: John Wiley & Sons; 2006. [Google Scholar]
- 28.Yekutieli D, Benjamini Y. The control of the false discovery rate in multiple testing under dependency. Ann Stat. 2001;29(4):1165-1188. [Google Scholar]
- 29.Bowalekar SK. Non-inferiority and equivalence trials. Perspect Clin Res. 2011;2(4):115-118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Feingold A. A regression framework for effect size assessments in longitudinal modeling of group differences. Rev Gen Psychol. 2013;17(1):111-121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Imel ZE, Laska K, Jakupcak M, Simpson TL. Meta-analysis of dropout in treatments for posttraumatic stress disorder. J Consult Clin Psychol. 2013;81(3):394-404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Foa EB, Dancu CV, Hembree EA, et al. A comparison of exposure therapy, stress inoculation training, and their combination for reducing posttraumatic stress disorder in female assault victims. J Consult Clin Psychol. 1999;67(2):194-200. [DOI] [PubMed] [Google Scholar]
- 33.Resick PA, Wachen JS, Mintz J, et al. ; STRONG STAR Consortium . A randomized clinical trial of group cognitive processing therapy compared with group present-centered therapy for PTSD among active duty military personnel. J Consult Clin Psychol. 2015;83(6):1058-1068. [DOI] [PubMed] [Google Scholar]
- 34.Resick PA, Wachen JS, Dondanville KA, et al. ; STRONG STAR Consortium . Effect of group vs individual cognitive processing therapy in active-duty military seeking treatment for posttraumatic stress disorder. JAMA Psychiatry. 2017;74(1):28-36. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Study Protocol and Statistical Analysis Plan