

Abstract
Background
Following the functional and physicochemical characterization of a proposed biosimilar, comparative clinical studies help to confirm biosimilarity by demonstrating similar safety and efficacy to the reference product in a sensitive patient population.
Patients and methods
LA-EP2006 is a proposed biosimilar that has been developed for pegfilgrastim, a long-acting form of granulocyte colony-stimulating factor for the prevention of neutropenia. The current analysis reports data pooled from two independent, multinational, prospective, randomized, controlled, double-blind phase III studies of similar design comparing the safety and efficacy of reference pegfilgrastim with LA-EP2006 in patients with breast cancer receiving myelotoxic (neo)adjuvant TAC (docetaxel, doxorubicin, and cyclophosphamide) chemotherapy and requiring granulocyte colony-stimulating factor.
Results
A total of 624 patients were randomized in the PROTECT-1 and PROTECT-2 studies (NCT01735175; NCT01516736) (LA-EP2006: n = 314; reference: n = 310). Baseline characteristics of patients were well balanced across treatment groups. The primary end point, mean duration of severe neutropenia in the first chemotherapy cycle was similar in both the LA-EP2006 and reference groups (1.05 ± 1.055 days versus 1.01 ± 0.958 days), with a treatment difference of − 0.04 days [95% confidence interval (CI): −0.19 to 0.11] that met the equivalence criteria (the 95% CI were within the defined margin of ±1 day). Secondary end points, such as the nadir of absolute neutrophil count and the incidence of febrile neutropenia, were also similar between LA-EP2006 and reference pegfilgrastim. The safety and tolerability profile of LA-EP2006 was similar to that observed with reference pegfilgrastim, and there were no reports of neutralizing antibodies.
Conclusions
This pooled analysis confirms, as a part of totality of evidence approach, that the proposed biosimilar pegfilgrastim LA-EP2006 has a comparable efficacy and safety profile to reference pegfilgrastim in patients with breast cancer receiving TAC chemotherapy.
Clinical trial numbers
NCT01735175 and NCT01516736.
Keywords: pegfilgrastim, granulocyte colony-stimulating factor, biosimilar, breast cancer, neutropenia
Key Message
PROTECT-1 and PROTECT-2 were clinical studies conducted to show similar safety and efficacy for the proposed biosimilar pegfilgrastim LA-EP2006, compared with reference pegfilgrastim. This pooled analysis confirms that LA-EP2006 has equivalent efficacy with no clinically meaning differences in safety to reference in patients with breast cancer receiving TAC chemotherapy.
Introduction
Biosimilars are biologics where the active substance is essentially the same biologic entity as the reference product and has no clinically meaningful differences in safety or efficacy. The development of biosimilar medicines involves a target-directed iterative stepwise process to ensure a product that is highly similar to the reference [1, 2]. Proof of biosimilarity is based on the totality of evidence including analytical, non-clinical and clinical data. Comparative efficacy and safety studies may comprise the final step to confirm biosimilarity and address any residual uncertainty, and should be carried out in the most sensitive population [3]. Once the totality of evidence has been established and confirmed in the most sensitive indication, biosimilars may be approved for, or extrapolated to, other indications of the reference product provided there is scientific justification [4, 5].
Recombinant human granulocyte colony-stimulating factor (G-CSF), filgrastim, and its long-acting pegylated form, pegfilgrastim, are widely used for the prevention of chemotherapy-induced neutropenia. Pegfilgrastim has the same active substance, mode of action and comparable efficacy and safety to filgrastim, but its longer serum half-life allows once-per-chemotherapy cycle administration, instead of the daily injection needed with filgrastim. This may offer improved convenience and compliance for patients receiving chemotherapy [6]. In clinical practice, the use of pegfilgrastim has been associated with reduced risk of febrile neutropenia (FN) and FN-related complications, including fewer hospitalizations, and enhanced chemotherapy dose intensity compared with short-acting G-CSFs [7, 8].
Although biosimilars of filgrastim have been licensed in Europe and approved for use in the United States, no pegfilgrastim biosimilar has yet been approved. Two phase III clinical trials (PROTECT-1 and PROTECT-2) of the proposed biosimilar pegfilgrastim LA-EP2006 have been conducted in patients with breast cancer in order to confirm equivalent efficacy and demonstrate no clinically meaningful differences in safety profile compared with reference pegfilgrastim (Neulasta®, Amgen Inc.) [9, 10]. We report a pooled analysis from these two studies in order to further assess the efficacy and safety of LA-EP2006 and reference pegfilgrastim. Separate trials are underway to compare pharmacokinetics and pharmacodynamics between LA-EP2006 and reference pegfilgrastim.
Methods
Study design
PROTECT-1 and PROTECT-2 were independent, multinational, prospective, randomized, double-blind phase III studies (clinicaltrials.gov: NCT01735175; NCT01516736) of similar design and included patients with breast cancer receiving myelotoxic (neo)adjuvant chemotherapy requiring G-CSF administration [9, 10]. These studies were conducted in 12 countries across North and Latin America, Europe and Asia and in accordance with the International Conference on Harmonization Guidelines for Good Clinical Practice, with applicable local regulations, and with the ethical principles of the Declaration of Helsinki. Both trials adhered to the rules of the CONSORT statement. Study protocols and all amendments were reviewed by Independent Ethics Committees for each participating site. All patients provided written informed consent.
Both studies included a screening period of up to 21 days, after which eligible patients were randomized 1 : 1 to either proposed biosimilar pegfilgrastim (LA-EP2006) or reference pegfilgrastim (Neulasta®, Amgen Inc.). Patients received TAC (docetaxel 75 mg/m2, doxorubicin 50 mg/m2, cyclophosphamide 500 mg/m2) chemotherapy administered intravenously on day 1 of each chemotherapy cycle every 3 weeks for up to 6 cycles. Pegfilgrastim (biosimilar or reference) 6 mg was administered by subcutaneous injection on day 2 of each chemotherapy cycle (at least 24 h after end of chemotherapy).
Patient population
The patient population has been reported previously [9, 10]. In brief, both studies enrolled adult women (aged ≥18 years) with histologically proved breast cancer who were chemotherapy-naïve and scheduled to receive up to six cycles of neoadjuvant or adjuvant treatment with TAC chemotherapy. Key inclusion criteria included Eastern Cooperative Oncology Group (ECOG) performance status ≤2 and adequate bone marrow function at day 1 of cycle 1 before chemotherapy [absolute neutrophil count (ANC) ≥1.5 × 109/l, platelet count ≥100 × 109/l, hemoglobin ≥10 g/dl).
End points
The primary efficacy end point in each study was the mean duration of severe (grade 4) neutropenia (DSN) during cycle 1 of chemotherapy, defined as the number of consecutive days with an ANC <0.5 × 109/l. Secondary efficacy assessments were depth of ANC nadir (lowest ANC) during cycle 1, time to ANC recovery (days from ANC nadir until ANC increased to ≥2 × 109/l) during cycle 1, incidence of FN [oral temperature of ≥38.3 °C with ANC <0.5 × 109/l or neutropenic sepsis (FN/NS)] by cycle and across all cycles, number of days of fever (oral temperature ≥38.3 °C) for each cycle, frequency of infections by cycle and across all cycles, and mortality due to infection.
Safety was assessed through the incidence, occurrence and severity of adverse events (AEs) during treatment, at follow-up 4 weeks after the last administration of pegfilgrastim (PROTECT-2 study) and at 6 months (PROTECT-1 study). Immunogenicity was assessed by a validated enzyme-linked immunosorbent assay for detection and characterization of binding anti-pegfilgrastim antibodies, and a validated cell-based neutralization antibody assay for the determination of potential neutralizing antibodies. Immunogenicity was assessed before the first administration of pegfilgrastim (LA-EP2006 or reference), on day 15 of cycle 6, and 4 weeks (PROTECT-2) and 6 months (PROTECT-1) after last administration.
Statistical analysis
Equivalence between biosimilar and reference pegfilgrastim were assessed in each study. Equivalence was assessed using two-sided 95% confidence intervals (CIs) for the difference in the mean DSN, with LA-EP2006 considered equivalent to reference pegfilgrastim if 95% CIs were within the pre-defined margin of ±1 day. A non-inferiority margin of 1 day for the mean DSN had been used previously in studies supporting the approval of pegfilgrastim in patients with breast cancer treated with myelosuppressive chemotherapy [11, 12] and an equivalence margin of ±1 day was agreed with regulatory authorities (US Food and Drug Administration [FDA] and European Medicines Agency [EMA]). Mean DSN was analyzed with an ANCOVA model using fixed and random terms: treatment, chemotherapy (adjuvant or neoadjuvant), region [America (both North and South), Europe and Asia], and baseline ANC count were fitted as fixed effects, and study (PROTECT-1 or PROTECT-2) as a random effect.
Results
A total of 624 patients were randomized and received ≥1 dose of pegfilgrastim (full analysis set: LA-EP2006: n = 314; reference: n = 310). Patient disposition has been reported for each of the PROTECT studies [9, 10].
Baseline characteristics were well balanced across treatment groups (Table 1). There were no relevant differences between treatment groups in the doses of chemotherapy during the first cycle and across all cycles. Mean (SD) relative dose intensity (RDI) of TAC chemotherapy was 0.99 (0.020) for LA-EP2006 and 0.99 (0.017) for reference pegfilgrastim in cycle 1, and 0.98 (0.050) with LA-EP2006 and 0.97 (0.061) for reference pegfilgrastim in cycle 6. Across all cycles, mean RDI was 0.99 (0.038) with LA-EP2006 and 0.98 (0.049) with reference pegfilgrastim.
Table 1.
Patient demographics and baseline characteristics (FAS)
| Parameter | LA-EP2006 (N=314) | Reference pegfilgrastim (N=310) | Total (N=624) |
|---|---|---|---|
| Age, years | |||
| n | 314 | 310 | 624 |
| Mean (SD) | 49.3 (10.02) | 49.8 (10.49) | 49.6 (10.25) |
| Median (range) | 50.0 (25–75) | 50.0 (26–76) | 50.0 (25–76) |
| BMI, kg/m2 | |||
| N | 313 | 309 | 622 |
| Mean (SD) | 27.1 (5.72) | 27.0 (5.38) | 27.0 (5.55) |
| Median (range) | 26.4 (14–44) | 26.2 (15–47) | 26.2 (14–47) |
| Race, n (%) | |||
| White | 219 (69.7) | 220 (71.0) | 439 (70.4) |
| Asian | 90 (28.7) | 84 (27.1) | 174 (27.9) |
| Black or African American | 1 (0.3) | 2 (0.6) | 3 (0.5) |
| Othera | 4 (1.3) | 4 (1.3) | 8 (1.3) |
| Ethnicity, n (%) | |||
| Not Hispanic or Latino | 293 (93.3) | 286 (92.3) | 579 (92.8) |
| Hispanic or Latino | 21 (6.7) | 24 (7.7) | 45 (7.2) |
| Time since initial diagnosis (months) | |||
| N | 308 | 298 | 606 |
| Median (range) | 1.33 (0.1–76.0) | 1.35 (0.2–11.2) | 1.35 (0.1–76.0) |
| Stage at initial diagnosis, n (%) | |||
| I | 11 (3.5) | 16 (5.2) | 27 (4.3) |
| II | 144 (45.9) | 134 (43.2) | 278 (44.6) |
| III | 159 (50.6) | 156 (50.3) | 315 (50.5) |
| IV | 0 | 4 (1.3) | 4 (0.6) |
| Any breast cancer surgical procedure, n (%) | 303 (96.5) | 298 (96.1) | 601 (96.3) |
| Any prior radiotherapy, n (%) | 9 (2.9) | 10 (3.2) | 19 (3.0) |
| ECOG coding at screening, n (%) | |||
| 0 | 245 (78.0) | 233 (75.2) | 478 (76.6) |
| 1 | 67 (21.3) | 77 (24.8) | 144 (23.1) |
| 2 | 2 (0.6) | 0 | 2 (0.3) |
Other race specified as Mestizo, Parda or Hispanic.
BMI, body mass index; ECOG, Eastern Cooperative Oncology Group; FAS, full analysis set; N, number of patients in a treatment group or analysis set; n, number of assessable patients; SD, standard deviation.
Efficacy
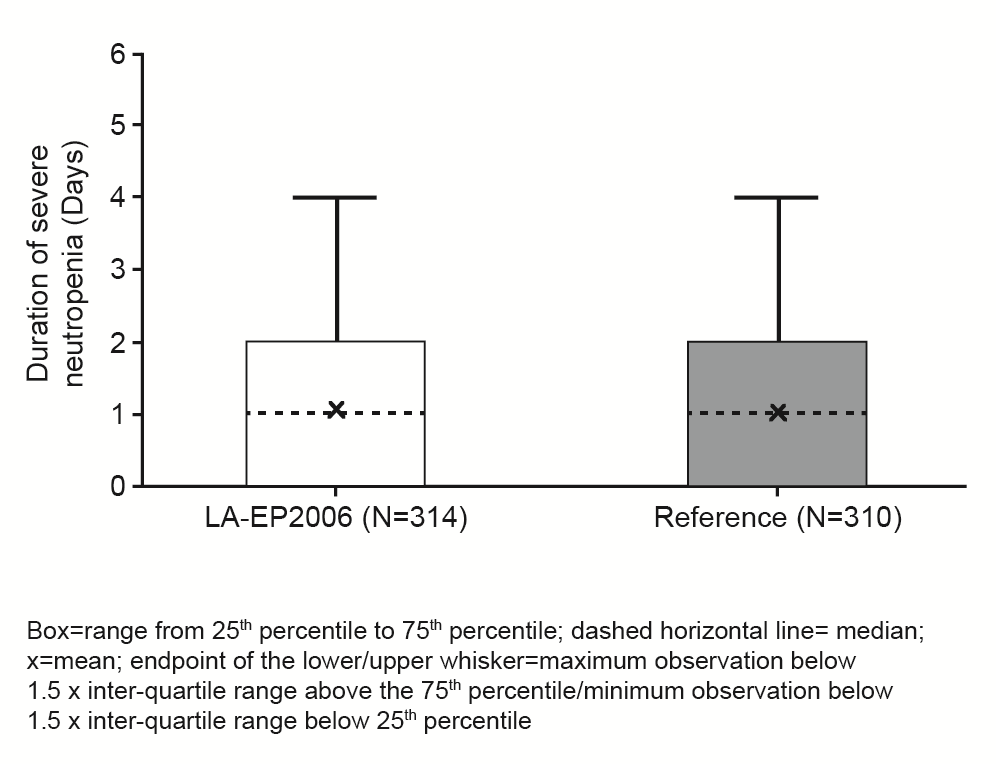
The primary end point, mean DSN was similar in both the LA-EP2006 and reference groups (1.05 ± 1.055 days versus 1.01 ± 0.958 days) (Table 2; supplementary Figure S1, available at Annals of Oncology online). The difference in DSN in cycle 1 was −0.04 days (95% CI: −0.19 to 0.11). LA-EP2006 met the equivalence criteria compared with the reference pegfilgrastim because the 95% CI was within the defined margin of ±1 day.
Table 2.
Efficacy parameters (FAS)
| LA-EP2006 (N=314) | Reference (N=310) | |
|---|---|---|
| Primary efficacy parameter | ||
| DSN in cycle 1, mean±SD (median) | 1.05±1.055 | 1.01±0.958 |
| (1.0) | (1.0) | |
| Secondary efficacy parameter | ||
| Depth of ANC nadir (×109/l) in cycle 1, mean±SD | 0.800±1.2436 | 0.687±0.9586 |
| Time to ANC recovery in cycle 1, mean±SD (median) | 1.84±1.01 | 1.88±1.04 |
| (2.0) | (2.0) | |
| Patients with ≥1 episode of FN/NS, n (%)a | ||
| Cycle 1 | 18 (5.7) | 26 (8.4) |
| All cycles | 25 (8.0) | 32 (10.3) |
| Patients with ≥1 episode of fever, n (%)a | ||
| Cycle 1 | 22 (7.0) | 31 (10.0) |
| All cycles | 58 (18.5) | 61 (19.7) |
| Patients with ≥1 infection, n (%)a | ||
| Cycle 1 | 17 (5.4) | 18 (5.8) |
| All cycles | 49 (15.6) | 56 (18.1) |
| Mortality due to infection, n (%) | 0 | 2 (0.6) |
All patients with FN/NS also experienced ≥1 fever episode.
Patients with >1 episode are counted only once.
ANC, absolute neutrophil count; ANC nadir, lowest ANC (109/l) in cycle 1; DSN, duration of severe neutropenia; FAS, full analysis set; FN/NS, febrile neutropenia/neutropenic sepsis; N, number of patients in a treatment group or analysis set; n, number of patients with at least one episode; SD, standard deviation; time to ANC recovery, time in days from ANC nadir until ANC had increased to ≥2 × 109/l.
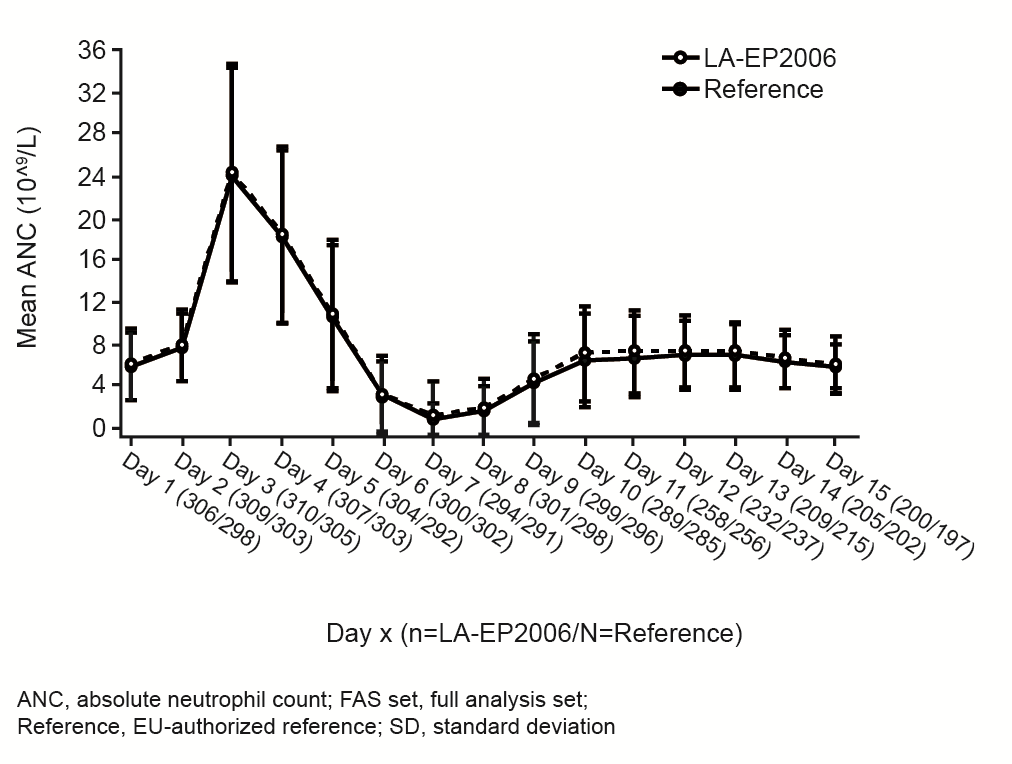
Secondary end points were similar between treatment groups (Table 2). The time course of the mean ANC count for LA-EP2006 was highly similar to that observed with reference pegfilgrastim (supplementary Figure S2, available at Annals of Oncology online). The mean ANC at nadir was 0.800 × 109/l with LA-EP2006 and 0.687 × 109/l with reference pegfilgrastim (Table 2), and the time for ANC to recover from the nadir to ≥2 × 109/l was 1.84 and 1.88 days, respectively. Incidence of FN/NS was low and similar between the treatment groups. Most patients experienced FN/NS in cycle 1, with a slightly higher incidence in the reference group (n = 26, 8.4%) than in the LA-EP2006 group (n = 18, 5.7%). Across all cycles, 25 patients (8.0%) in the LA-EP2006 group and 32 patients (10.3%) in the reference group experienced FN/NS.
Safety
The safety and tolerability profile for LA-EP2006 was similar to that observed with reference pegfilgrastim. A total of 92% and 89% of patients receiving LA-EP2006 or reference pegfilgrastim experienced ≥1 treatment-emergent (TE) AE during the treatment period (i.e. onset of AE was on or after the date of the first administration of chemotherapy and not later than 30 days after last pegfilgrastim administration). The type and the frequency of TEAEs were similar between LA-EP2006 and reference pegfilgrastim, with the most frequent TEAEs being chemotherapy-induced events (supplementary Table S1, available at Annals of Oncology online). Serious TEAEs occurred in 14.3% of LA-EP2006 patients and 17.1% of reference pegfilgrastim patients (supplementary Table S2, available at Annals of Oncology online).
A total of 71 (22.6%) patients in the LA-EP2006 group and 66 (21.3%) patients in the reference pegfilgrastim group had TEAEs with suspected relationship to pegfilgrastim (supplementary Table S2, available at Annals of Oncology online). The most frequent TEAEs with a suspected relationship to pegfilgrastim were musculoskeletal and connective tissue disorders (LA-EP2006: 10.2%; reference pegfilgrastim: 9.7%), of which bone pain was the most commonly reported (LA-EP2006: 4.5%; reference: 6.1%). Serious TEAEs with a suspected relationship to pegfilgrastim occurred with a low incidence in both treatment groups. Overall, FN was reported with similar frequencies in the two treatment groups (LA-EP2006: 8.0%; reference pegfilgrastim: 10.0%), but was considered to be related to pegfilgrastim more frequently in the LA-EP2006 group compared with the reference group [5 (1.6%) versus 0]. Overall, the number of patients with infections was low in each cycle, and there were no clinically meaningful differences between the treatment groups (Table 2).
A total of 11 patients died in the 2 studies (including the safety follow-up period); 4 patients in PROTECT-1 and 3 patients in PROTECT-2 in the LA-EP2006 group, and 2 patients in PROTECT-1 and 2 patients in PROTECT-2 in the reference pegfilgrastim group. None of the deaths were suspected to be pegfilgrastim related. Despite the numerical differences, analysis of the deaths did not reveal any pattern related to either product.
Local injection site reactions occurred rarely in either treatment group: three patients in the reference group and one patient in the LA-EP2006 group reported injection-site reactions recorded as non-serious TEAEs suspected to be related to study drug. No neutralizing or clinically relevant anti-drug antibodies were detected post-dose.
Discussion
This pooled analysis of two pivotal randomized phase III trials confirms the clinical equivalence of proposed biosimilar pegfilgrastim (LA-EP2006) with reference pegfilgrastim for the prevention of severe neutropenia in patients with breast cancer receiving myelotoxic chemotherapy.
TAC chemotherapy produces a prolonged and severe neutropenia [13] and increases the risk of FN in patients with breast cancer [14]. Primary prophylaxis with G-CSF is known to greatly reduce this risk of FN in these patients [14]. This population represents a sensitive and appropriate cohort for detecting potential differences between a proposed biosimilar and reference G-CSF product. Patients with breast cancer were used for pivotal registration trials for reference pegfilgrastim and other G-CSF products [11, 12, 15, 16], although a variety of myelosuppressive chemotherapy regimens were used in these studies.
Duration of severe neutropenia was used as the primary efficacy end point since it is a well-established end point to compare products of the G-CSF class. The continuous nature of this end point with frequent repeat sampling makes it more sensitive to detect potential differences than other categorical clinical end points such as FN or infections. It is also the time period at which patients may be at most risk of FN. There are limitations when comparing results from different studies, due to the potential influence of differing patient populations and chemotherapy regimens, etc. Nevertheless, the mean DSN with LA-EP2006 and reference pegfilgrastim in cycle 1 was consistent with that observed in previous studies of pegfilgrastim [11, 12, 15–19].
The safety and tolerability profile of LA-EP2006 was similar to that observed with reference pegfilgrastim and was generally consistent with the known safety profile of the G-CSF class. For example, TEAEs with a suspected relationship to pegfilgrastim occurred with similar incidences in both treatment groups (LA-EP2006: 22.6%; reference pegfilgrastim: 21.3%) and at an incidence (25.7%) comparable with that previously reported for pegfilgrastim 6 mg [15]. Reports of bone pain in the current analysis were lower than reported with pegfilgrastim in other studies [11, 12, 15, 17]. The incidence of bone pain greatly between pegfilgrastim studies, and this could reflect differences in patient populations, background therapies or in how bone pain was reported or defined. In contrast to several other pegfilgrastim studies [11, 12, 15, 17] a few deaths occurred in the PROTECT studies. However, there was no discernible pattern and the deaths were not considered related to either of the products under investigation.
In the current analysis, no clinically relevant binding or neutralizing anti-pegfilgrastim antibodies were detected, which is consistent with observations from other studies with pegfilgrastim [11, 12, 17, 19].
Patients receiving G-CSF for the prevention of chemotherapy-associated neutropenia are often undertreated [20, 21], with filgrastim being used for shorter durations or at lower doses than recommended [21–23]. The resulting inadequate prevention of FN could result in increased hospitalizations for FN [21] and delays in initiation of chemotherapy or reductions in dose intensity [9, 24, 25] that may adversely impact survival. There may be various reasons for the suboptimal use of filgrastim in clinical practice, including attempts to minimize costs or a lack of convenience resulting in poor adherence. The ability to administer pegfilgrastim once per cycle rather than once daily may be more convenient for patients and physicians. Moreover, the availability of biosimilar pegfilgrastim may increase competition and thereby help to decrease costs required for ensuring adequate prevention of chemotherapy-associated neutropenia. A cost-efficiency analysis showed that biosimilar filgrastim was more cost-efficient than the reference product, costing €1336.46 (14 days) compared with €1794.30 [26]. Analysis of prescription data from 8726 patients in Germany also showed a cost advantage of biosimilar G-CSF compared with reference medicines [27]. Evidence suggests that pegfilgrastim has potential for greater cost minimization compared with filgrastim, although these cost–benefits may be less pronounced in the EU compared with United States where the cost of treatment is generally higher [28].
In conclusion, this combined analysis confirms that the proposed biosimilar pegfilgrastim LA-EP2006 has comparable efficacy (duration of severe neutropenia) and safety to reference pegfilgrastim in breast cancer patients receiving TAC chemotherapy.
Supplementary Material
{kind=link}
{kind=link}
Acknowledgements
Editorial support was provided by Graham Allcock of Spirit Medical Communications Ltd, supported by Sandoz GmbH, Kundl, Austria. Final approval of the manuscript rested solely with the scientific authors.
Funding
This work was supported by Sandoz GmbH, Kundl, Austria. No grant number is applicable. Authors received no monetary compensation in return for their work on this manuscript.
Disclosure
KB has provided advisory or consulting services to Sandoz GmbH, Kundl, Austria. NH has provided advisory or consulting services to Amgen and Hexal AG. RN and AK are employees of Hexal AG (a Sandoz company), Holzkirchen, Germany, and YL is an employee of Sandoz Inc., Princeton, NJ, USA. All remaining authors have declared no conflicts of interest.
References
- 1. Bui LA, Hurst S, Finch GL. et al. Key considerations in the preclinical development of biosimilars. Drug Discov Today 2015; 20(Suppl 1): 3–15. [DOI] [PubMed] [Google Scholar]
- 2. Holzmann J, Balser S, Windisch J.. Totality of the evidence at work: the first U.S. biosimilar. Expert Opin Biol Ther 2016; 16(2): 137–142. [DOI] [PubMed] [Google Scholar]
- 3. Windisch J. Biosimilars versus original biologics. Similarities and differences from development to approval. Z Rheumatol 2015; 74(8): 672–681. [DOI] [PubMed] [Google Scholar]
- 4. European Medicines Agency. Guideline on Similar Biological Medicinal Products Containing Monoclonal Antibodies—Non-clinical and Clinical Issues. London, UK: Committee for Medicinal Products for Human Use; 2014. [Google Scholar]
- 5. Federal Drug Administration. Scientific considerations in demonstrating biosimilarity to a reference product: guidance for industry. April 2015; http://www.fda.gov/downloads/drugs/guidancecomplianceregulatoryinformation/guidances/ucm291128.pdf (1 July 2016, date last accessed).
- 6. Gabrilove JL. An analysis of current neutropenia therapies, including pegfilgrastim. Clin Cornerstone 2006; 8(Suppl 5): S19–S28. [DOI] [PubMed] [Google Scholar]
- 7. Mitchell S, Li X, Woods M. et al. Comparative effectiveness of granulocyte colony-stimulating factors to prevent febrile neutropenia and related complications in cancer patients in clinical practice: a systematic review. J Oncol Pharm Pract 2016; 22(5): 702–716. [DOI] [PubMed] [Google Scholar]
- 8. Kourlaba G, Dimopoulos MA, Pectasides D. et al. Comparison of filgrastim and pegfilgrastim to prevent neutropenia and maintain dose intensity of adjuvant chemotherapy in patients with breast cancer. Support Care Cancer 2015; 23(7): 2045–2051. [DOI] [PubMed] [Google Scholar]
- 9. Blackwell K, Donskih R, Jones CM. et al. A comparison of proposed biosimilar LA-EP2006 and reference pegfilgrastim for the prevention of neutropenia in patients with early-stage breast cancer receiving myelosuppressive adjuvant or neoadjuvant chemotherapy: Pegfilgrastim Randomized Oncology (Supportive Care) Trial to Evaluate Comparative Treatment (PROTECT-2), a phase III, randomized, double-blind trial. Oncologist 2016; 21(7): 789–794. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Harbeck N, Lipatov O, Frolova M. et al. Randomized, double-blind study comparing proposed biosimilar LA-EP2006 with reference pegfilgrastim in breast cancer. Future Oncol 2016; 12(11): 1359–1367. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Holmes FA, O'Shaughnessy JA, Vukelja S. et al. Blinded, randomized, multicenter study to evaluate single administration pegfilgrastim once per cycle versus daily filgrastim as an adjunct to chemotherapy in patients with high-risk stage II or stage III/IV breast cancer. J Clin Oncol 2002; 20: 727–731. [DOI] [PubMed] [Google Scholar]
- 12. Green MD, Koelbl H, Baselga J. et al. A randomized double-blind multicenter phase III study of fixed-dose single-administration pegfilgrastim versus daily filgrastim in patients receiving myelosuppressive chemotherapy. Ann Oncol 2003; 14: 29–35. [DOI] [PubMed] [Google Scholar]
- 13. Nabholtz JM, Mackey JR, Smylie M. et al. Phase II study of docetaxel, doxorubicin, and cyclophosphamide as first-line chemotherapy for metastatic breast cancer. J Clin Oncol 2001; 19: 314–321. [DOI] [PubMed] [Google Scholar]
- 14. Mackey JR, Pieńkowski T, Crown J. et al. ; Translational Research In Oncology (TRIO)/Breast Cancer International Research Group (BCIRG)-005 investigators. Long-term outcomes after adjuvant treatment of sequential versus combination docetaxel with doxorubicin and cyclophosphamide in node-positive breast cancer: BCIRG-005 randomized trial. Ann Oncol 2016; 27: 1041–1047. [DOI] [PubMed] [Google Scholar]
- 15. Bondarenko I, Gladkov OA, Elsaesser R. et al. Efficacy and safety of lipegfilgrastim versus pegfilgrastim: a randomized, multicenter, active-control phase 3 trial in patients with breast cancer receiving doxorubicin/docetaxel chemotherapy. BMC Cancer 2013; 13: 386.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Volovat C, Gladkov OA, Bondarenko IM. et al. Efficacy and safety of balugrastim compared with pegfilgrastim in patients with breast cancer receiving chemotherapy. Clin Breast Cancer 2014; 14: 101–108. [DOI] [PubMed] [Google Scholar]
- 17. Holmes FA, Jones SE, O’Shaughnessy J. et al. Comparable efficacy and safety profiles of once-per-cycle pegfilgrastim and daily injection filgrastim in chemotherapy-induced neutropenia: a multicenter dose-finding study in women with breast cancer. Ann Oncol 2002; 13: 903–909. [DOI] [PubMed] [Google Scholar]
- 18. Masuda N, Tokuda Y, Nakamura S. et al. Dose response of pegfilgrastim in Japanese breast cancer patients receiving six cycles of docetaxel, doxorubicin, and cyclophosphamide therapy: a randomized controlled trial. Support Care Cancer 2015; 23: 2891–2898. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Yang BB, Morrow PK, Wu X. et al. Comparison of pharmacokinetics and safety of pegfilgrastim administered by two delivery methods: on-body injector and manual injection with a prefilled syringe. Cancer Chemother Pharmacol 2015; 75(6): 1199–1206. [DOI] [PubMed] [Google Scholar]
- 20. Potosky AL, Malin JL, Kim B. et al. Use of colony-stimulating factors with chemotherapy: opportunities for cost savings and improved outcomes. J Natl Cancer Inst 2011; 103: 979–982. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Weycker D, Hackett J, Edelsberg JS. et al. Are shorter courses of filgrastim prophylaxis associated with increased risk of hospitalization? Ann Pharmacother 2006; 40: 402–407. [DOI] [PubMed] [Google Scholar]
- 22. Naeim A, Henk HJ, Becker L. et al. Pegfilgrastim prophylaxis is associated with a lower risk of hospitalization of cancer patients than filgrastim prophylaxis: a retrospective United States claims analysis of granulocyte colony-stimulating factors (G-CSF). BMC Cancer 2013; 13: 11.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Almenar Cubells D, Bosch Riog C, Jiminez Orozco E. et al. Effectiveness of daily versus non-daily granulocyte colony-stimulating factors in patients with solid tumours undergoing chemotherapy: a multivariate analysis of data from current practice. Eur J Cancer Care (Engl) 2013; 22: 400–412. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Aapro MS, Bohlius J, Cameron DA. et al. 2010 update of EORTC guidelines for the use of granulocyte-colony stimulating factor to reduce the incidence of chemotherapy-induced febrile neutropenia in adult patients with lymphoproliferative disorders and solid tumours. Eur J Cancer 2011; 47: 8–32. [DOI] [PubMed] [Google Scholar]
- 25. Lyman GH. Chemotherapy dose intensity and quality cancer care. Oncology (Williston Park) 2006; 20: 16–25. [PubMed] [Google Scholar]
- 26. Aapro M, Cornes P, Abraham I.. Comparative cost-efficiency across the European G5 countries of various regimens of filgrastim, biosimilar filgrastim, and pegfilgrastim to reduce the incidence of chemotherapy-induced febrile neutropenia. J Oncol Pharm Pract 2012; 18(2): 171–179. [DOI] [PubMed] [Google Scholar]
- 27. Hadji P, Kostev K, Schröder-Bernhardi D. et al. Cost comparison of outpatient treatment with granulocyte colony-stimulating factors (G-CSF) in Germany. Int J Clin Pharmacol Ther 2012; 50(4): 281–289. [DOI] [PubMed] [Google Scholar]
- 28. Hirsch BR, Lyman GH.. Pharmacoeconomics of the myeloid growth factors: a critical and systematic review. Pharmacoeconomics 2012; 30(6): 497–511. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.