

Abstract
We are now entering the very exciting era of treatment and management of diabetes mellitus (DM) with the emergence of new therapeutic agents, including sodium-glucose cotransporter 2 inhibitors (SGLT2i) and dipeptidyl peptidase-4 inhibitor (DPP-4i). From a cardiology and echocardiography perspective, the existence of diabetic cardiomyopathy has been proven through over four decades of discussion. DM is highly prevalent in patients with heart failure (HF). Independent associations are found after adjusting for hypertension (HTN) and coronary artery disease (CAD). In patients with both DM and HF, the prognosis is extremely dismal. In this review, the main focus is on both diabetic cardiomyopathy per se and its typical features (including myocardial additive insult related to DM), diagnosis, and management.
Keywords: Diabetes mellitus (DM), diabetic cardiomyopathy, echocardiography, myocardial strain, sodium-glucose cotransporter 2 inhibitors (SGLT2i)
Introduction
The concept of diabetic cardiomyopathy was first described in 1972 by Rubler et al. in their manuscript titled “New type of cardiomyopathy associated with diabetic glomerulosclerosis” (1). They found that 15% of postmortem cases with diabetic glomerulosclerosis had no hypertension (HTN) and no significant coronary artery disease (CAD) but left ventricular hypertrophy (LVH), cardiomegaly and congestive heart failure (HF). Their histopathologic study revealed diffuse fibrosis, myofibrillar hypertrophy, microvascular disease and deposition of acid mucopolysaccharide material. Their speculation on the pathophysiological mechanism remains valid in the current understanding: “Probably secondary to diabetic microangiopathy although the direct effects of the abnormal myocardial metabolism in diabetes mellitus (DM) could not be excluded.” Diabetic cardiomyopathy has subsequently been widely reported and used by epidemiologists and clinicians worldwide.
DM as an independent risk factor for HF
There has been a long debate whether DM causes cardiomyopathy or not (2), because some argue that CM in patients with DM could be due to confounders, such as CAD disease, concomitant HTN, and so on (Figure 1). Indeed, DM dramatically increases the risk of HF. Data from Framingham population demonstrated a 2- to 5-fold excess risk for developing new HF in individuals with DM (3). The risk is even higher (4- to 8-fold) in young patients. An almost linear increase in risk is observed: each 1% elevation in hemoglobin A1C (HbA1C) leads to an 8% increase in the frequency of HF. The independent association between DM and HTN is supported by several large sets of clinical data (Table 1).
Figure 1.
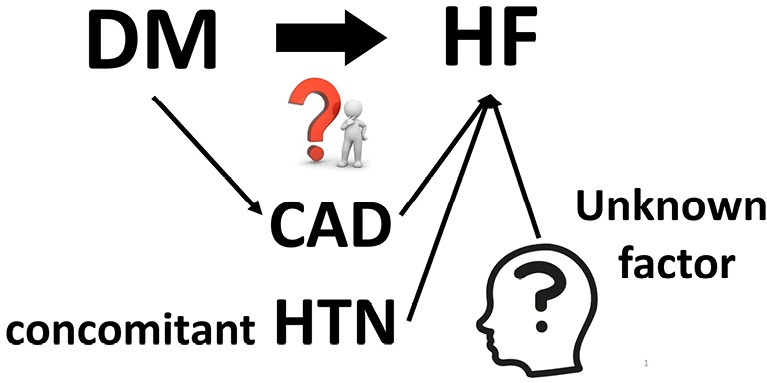
DM and HF. There has been a long period of discussion on the association between DM and HF, if it is an independent association or confounded by concomitant risk factors, like CAD, HTN or unknown factors. CAD, coronary artery diseases; DM, diabetes mellitus; HF, heart failure; HTN, hypertension
Table 1. Association between DM and HF.
| Study | Journal/year | Heart failure with DM |
|---|---|---|
| Framingham (4) | Am J Cardio 1974 | <65 years—HR =4 in men, 8 in women; overall—2.4 in men, 5.1 in women |
| CV Health study (5) | J Am Coll Cardiol 2000 | HR =1.74 (1.38–2.19) |
| UKPDS (6) | BMJ 2000 | HF risk related to HbA1c |
| Kaiser Permanente (7) | Diabetes Care 2001 | 45–54 years—33 cases per 1,000; 55–64 years—68 cases per 1,000; 65–74 years—135 cases per 1,000 |
| ALLHAT (8) | Circulation 2006 | RR =1.95 for HF hospitalization/death |
HF, heart failure; HR, hazard ratio; RR, risk ratio; DM, diabetes mellitus; HbA1c, hemoglobin A1C.
Effect of DM on HF prognosis
When a patient with DM develops HF, the prognosis generally remains dismal. Data were collected from the US Medicare which include >150,000 patients with DM and aged >65 years. Patients with DM and HF had a hazard ratio (HR) for mortality of >10 with very narrow confidence interval (CI) (HR =10.6; 95% CI: 10.4–10.9), compared with DM without HF (9). The finding is corroborated by several large clinical trials such as LIFE (HR for mortality was 5.98; 95% CI: 3.90–9.17; P<0.0001) and RENAAL (HR =3.99; 95% CI: 3.02–5.25; P<0.0001) (10).
Current understanding
Based on these data, ACCF/AHA Guidelines for HF determined diabetes as an independent risk factor for HF (11). From this revision of the Guidelines, they categorized HF into four stages (stages A to D). Stage A is at high risk for HF without structural changes or symptoms. They clearly mention that DM itself is a significant independent risk for HF. The definition of diabetic cardiomyopathy has been slightly modified from the initial definition by Rubler et al. “ventricular dysfunction that occurs independently of CAD and HTN” to “diabetes-associated structural and functional myocardial dysfunction not related to other confounding traditional factors such as CAD, HTN, congenital or valvular heart diseases” (12-14). In addition, diabetic cardiomyopathy is classified into two types: restrictive [similar to HF with preserved ejection fraction (EF) >50%] and dilated (HF with reduced EF <50%) (15).
The restrictive type is mainly characterized by coronary microvascular endothelial dysfunction and metabolic rearrangements (hyperglycemia, lipotoxicity, and obesity), whereas the dilated counterpart is characterized by cardiomyocyte cell death and autoimmune disorder [e.g., type 1 diabetes mellitus (T1DM)]. They also share common features, such as coronary microvascular rarefaction and advanced glycogen end product (AGE) deposition. Concerning further detailed mechanism, insulin resistance and hyperinsulinemia play a key role (16). They increase systemic metabolic disorders and activate the sympathetic nerve system (autonomic dysfunction); then activate renin-angiotensin-aldosterone system; prompt oxidative stress, mitochondrial dysfunction, and endoplasmic reticulum stress; and impair calcium homeostasis. These effects result in cardiac fibrosis, hypertrophy, cardiomyocyte death, dysfunction of the coronary microcirculation, and eventually HF. Furthermore, these pathophysiological changes in cardiomyocytes underlie the risk factors for insulin resistance and hyperinsulinemia, which can result in a potentially vicious cycle, which prompt the following question: does HF cause DM?
Does HF cause DM?
Data from the Bezafibrate Infarction Prevention trial, which included >2,600 patients who had myocardial infarction without diabetes at baseline, showed that those with New York Heart Association (NYHA) class III symptoms had a significant increase in subsequent DM with a 1.7-fold (95% CI: 1.1–2.6) increase, but those with NYHA class II did not (HR =1.0; 95% CI: 0.8–1.3) over the 7.7 years of follow-up (17). The main underlying mechanism is insulin resistance (18). A new HF medication, sacubitril/valsartan, has greater glycemic control than angiotensin converting enzyme inhibitor (19).
Who should be screened and how?
Thus far, the brief history of diabetic cardiomyopathy and HF risk and vicious cycle has been reviewed. The next logical questions are who to be screened and how. Our meta-analysis identified four key independent risk factors: history of CAD, age (every 5 years), poor glycemic control markers (i.e., insulin use, high fasting glucose, and HbA1c of >9.0%), and HTN (20). As routine clinical practice, the screening should comprise history (above four criteria) and physical examination (including blood pressure assessment), blood tests (for glycemic control), and electrocardiography (ECG) (for CAD and LVH).
The screening should include medical encounter for medical history (age, CAD, etc.), symptoms (dyspnea, etc.), and physical examination, including blood pressure measurement, followed by blood tests for glycemic control and ECG for CAD or LVH. As screening is mostly performed in asymptomatic subjects with risks (stage A HF), cardiac imaging plays an important role. The majority of data in the literature are from echocardiography, which will be discussed in the following section.
Echocardiographic assessment of diabetic cardiomyopathy
LVH and myocardial fibrosis (morphological alteration assessed by echocardiography): the main finding of diabetic cardiomyopathy was LVH in the initial autopsy study (1), where histopathologic study revealed diffuse fibrosis and myocyte hypertrophy (Figure 2). Using echocardiography, numerous studies, including population-based studies (21-28) (Table 2), confirmed LVH in a population with diabetes and in prediabetes stage, for example, impaired glucose tolerance (IGT) (21,22,25,27). In the Strong Heart Study population, Ilercil et al. identified independent associations of IGT with higher left ventricular (LV) relative wall thicknesses and LV mass/height2.7 (25). Collectively, DM, even from the prediabetes stage, is independently associated with LVH.
Figure 2.
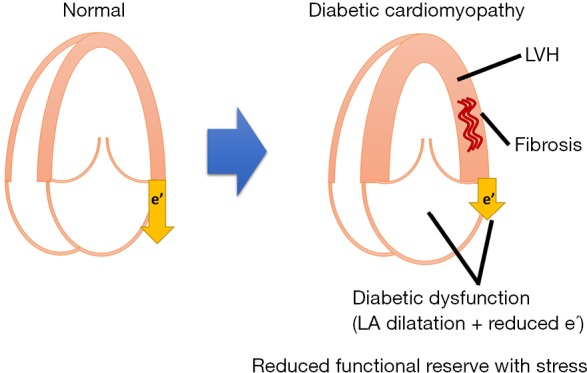
Schematic illustration of diabetic cardiomyopathy. LVH, left ventricular hypertrophy; LA, left atrial.
Table 2. Diabetes mellitus and left ventricular hypertrophy.
| Year | First author | Study cohort | DM or IGT | Main findings |
|---|---|---|---|---|
| 1991 | Galderisi (21) | FHS | DM or IGT | Increase in LVM in women |
| 1997 | Lee (22) | CV Health Study | DM or IGT | Increase in LVM in both sexes |
| 2000 | Devereux (23) | Strong Heart Study | DM | Increase in LVM |
| 2001 | Palmeri (24) | HyperGEN Study | DM + HTN | Increase in LVM and RWT |
| 2001 | Ilerci (25) | Strong Heart Study | IGT | Increase of LVM and RWT |
| 2001 | Bella (26) | Strong Heart Study | DM ± HTN | Progressive increase of LVM in both DM ± HTN |
| 2003 | Rutter (27) | FHS | DM or IGT | Progressive increase in LVM, RWT, and LA |
CV, cardiovascular; DM, diabetes mellitus; FHS, Framingham Heart Study; IGT, impaired glucose tolerance; HTN, hypertension; LA, left atrial; LVM, left ventricular mass; RWT, relative wall thickness.
The main underlying histopathologic alteration in diabetic cardiomyopathy is fibrosis (29). Integrated backscatter (IB) is a technique used to assess echocardiographic tissue characteristic using the reflectivity of tissue to ultrasound, developed in the 1980s (30,31). From the early 1990s, the IB has been performed in patients with diabetes (32,33) (Table 3). Their primary findings are greater IB (indicating greater fibrosis) and lower cyclic variation of IB in the diabetic myocardium.
Table 3. Diabetes mellitus and fibrosis.
| Year | First author | Journal | Main findings |
|---|---|---|---|
| 1992 | Perez (32) | J Am Coll Cardiol | Lower cyclic variation of IB in insulin dependent DM and further reduced in patients with insulin DM with neuropathy |
| 1995 | Di Bello (33) | J Am Coll Cardiol | Increased echodensity by IB in insulin DM |
| 2003 | Fang (34) | J Am Coll Cardiol | Greater calibrated IB in DM than in normal controls |
| 2008 | van Heerebeek (29) | Circulation | Determinants for diastolic stiffness are fibrosis, AGEs, and myocyte resting tension using biopsy specimen |
AGEs, advanced glycogen end products; IB, integrated backscatter; DM, diabetes mellitus.
Diastolic dysfunction: the primary and early functional consequence of these morphological alterations is LV diastolic dysfunction (16) (Table 4). Early reports showed lower transmitral E/A ratios among patients with DM (35-37), followed by lower mitral annular early diastolic velocity assessment (38), greater E/E' (41,43), and larger left atrial (LA) volume (46). Subclinical LV diastolic dysfunction is associated with poor diabetic control, advancing age, HTN, metformin treatment (39), and cardiac autonomic neuropathy (44). Diastolic dysfunction in diabetes indicates worse prognosis (42,43,46). E/E'sept of >15 in patients with DM is associated with subsequent HF and increased mortality independent of HTN, CAD, or other echocardiographic parameters (43).
Table 4. Diabetes mellitus and diastolic dysfunction.
| Year | First author | Journal | Main findings |
|---|---|---|---|
| 1988 | Zarich (35) | J Am Coll Cardiol | Lower E/A ratio and higher A-wave velocity in T1DM than control subjects |
| 1995 | Celentano (36) | Am J Cardio | Lower E/A ratios in patients with T2DM or IGT than in normoglycemic subjects |
| 2001 | Liu (37) | J Am Coll Cardiol | Progressive reduction of E/A ratio and prolongation of DT in DM ± HTN |
| 2002 | Hansen (38) | Diabetes | Lower e' in T1DM than in normal controls |
| 2005 | Fang (39) | Diabetologia | Subclinical LV diastolic dysfunction is associated with poor diabetic control, advancing age, hypertension, and metformin treatment; ACE inhibitor and insulin therapies appear to be protective |
| 2006 | Bajraktari (40) | Int J Cardio | Insulin resistance is associated with diastolic dysfunction |
| 2006 | Moir (41) | Heart | Higher E/E' in T2DM than in controls |
| 2009 | From (42) | Am J Cardio | DM of >4 years is correlated with significant LV diastolic dysfunction; LV diastolic dysfunction is predictive of all-cause mortality in patients with DM independent of HTN and CAD |
| 2010 | From (43) | J Am Coll Cardiol | E/E'sept of >15 in patients with DM is associated with the subsequent development of HF and increased mortality independent of HTN, CAD, or other echocardiographic parameters |
| 2010 | Sacre (44) | JACC Cardiovasc Imaging | Diastolic dysfunction in DM is associated with cardiac autonomic neuropathy assessed by MIBG |
| 2011 | Falcão-Pires (45) | Circulation | DM further worsens diastolic function in severe aortic stenosis, via greater fibrosis, AGE accumulation, and stiffened myocytes |
| 2013 | Poulsen (46) | J Am Coll Cardiol | Increased LAVI was an independent and incremental predictor of CV morbidity and mortality in patients with T2DM with no history of CVD |
AGE, advanced glycogen end product; CAD, coronary artery disease; CV, cardiovascular; CVD, cardiovascular disease; HTN, hypertension; LV, left ventricular; MIBG, iodine 123-metaiodobenzylguanidine; T1DM, type 1 diabetes mellitus; T2DM, type 2 diabetes mellitus; IGT, impaired glucose tolerance; DM, diabetes mellitus; HF, heart failure; ACE, angiotensin-converting enzyme; DT, deceleration time; LAVI, left atrial volume index.
Valvular heart diseases: there have been significant increases in the prevalence of DM and valvular heart diseases (47,48). DM accelerates progression of calcific aortic stenosis (49) and worsens LV diastolic function via altering myocardial structure and cardiomyocyte stiffness (45). A small study showed the possibility that DM may accelerate aortic stenosis progression with enhanced inflammation (50). In patients with mitral regurgitation (MR), prevalence of MR is as high as 32%, mainly due to both mitral valve and myocardial abnormalities (48). As a result, patients with even mild MR have a 3.3-fold increased risk of all-cause mortality, whereas those with moderate-to-severe MR have a 5.1-fold increased risk (48).
Myocardial reserve assessed by stress echocardiography
Pharmacological and exercise stress echocardiography have provided intriguing insights into diabetic cardiomyopathy (Table 5). Patients with DM have impaired longitudinal functional reserve in both systolic (51) and diastolic functions (34). Furthermore, LV circumferential contractility and longitudinal systolic function reserves are correlated with stroke index reserve during low-dose dobutamine stress (53). Exercise stress echocardiography confirmed diminished systolic and diastolic functional reserve in this population (54,55).
Table 5. Diabetes mellitus and functional reserve.
| Year | First author | Journal | Main findings |
|---|---|---|---|
| 2003 | Vinereanu (51) | Clin Sci (Lond) | T2DM has impaired functional reserve in s' during DSE |
| 2003 | Fang (52) | J Am Coll Cardiol | During DSE, e' in patients with DM was lower than controls at baseline, low, pre-peak, and peak dose |
| 2006 | Palmieri (53) | J Am Soc Echocardiogr | LV circumferential contractility and longitudinal systolic function reserves correlated with stroke index reserve during low-dose dobutamine stress |
| 2007 | Ha (54) | Heart | Exercise stress echocardiography demonstrated that both systolic and diastolic reserves in longitudinal function are reduced in DM, compared with age- and sex-matched controls |
| 2010 | Mizuno (55) | J Card Fail | Patients with DM have exercise-induced delayed onset of LV relaxation and impaired coronary microcirculatory function without coexistent heart disease |
| 2017 | Cortigiani (56) | J Am Soc Echocardiogr | Dual-imaging stress echocardiography dipyridamole stress echocardiography [conventional wall motion analysis and Doppler-derived coronary flow velocity reserve (CFVR) of the left anterior descending coronary artery] has independent prognostic value in patients with DM |
DM, diabetes mellitus; LV, left ventricular; T2DM, type 2 diabetes mellitus; DSE, dobutamine stress echocardiography.
Although the negative predictive value of exercise stress echocardiography for exclusion of underlying myocardial ischemia in type 2 diabetes mellitus (T2DM) is reduced compared with the nondiabetic population (57), recent data provided a favorable finding, where dual-imaging dipyridamole stress echocardiography [conventional wall motion analysis and Doppler-derived coronary flow velocity reserve (CFVR) of the left anterior descending coronary artery] has independent prognostic value in patients with DM (56). This result is in line with previous findings on reduced myocardial flow (38) and flow reserve (41) in this population. Among patients with diabetes, hypoglycemia can be fatal. As acute hypoglycemia decreases myocardial blood flow reserve in both healthy humans and patients with T1DM (58), this could be one of the underlying mechanisms.
Myocardial strain
Myocardial strain analysis brought further intriguing insights (Table 6). Others and we reported that patients with DM have impaired systolic and diastolic longitudinal strains irrespective of concomitant HTN in tissue Doppler-derived and speckle-tracking strain methods (41,52,61,62). This deteriorated longitudinal function has been demonstrated using more largely available technique, like tissue Doppler and atrioventricular plane displacement by M-mode (64). Studies using magnetic resonance imaging (MRI) tagging strain reported similar findings (59,60). Not only peak systolic circumferential and longitudinal strains and principal 3-D shortening strain were smaller in the T2DM group but also peak diastolic rate of relaxation of these strains were lower in patients with DM with normal EF (P<0.001 for each) (59). Furthermore, patients with DM have paradoxical increase in myocardial torsion (60). They had a higher resting HR (77.0±12.4 vs. 59.0±5.6 beats/min; P<0.01), higher maximal torsion by 23% (3.5±0.9 vs. 2.7±0.4 °/cm; P<0.01), and higher maximal systolic torsion rate by 25% (0.013±0.003 vs. 0.010±0.002 °/cm/s; P<0.01). Torsion did not significantly change with chronotropic stimulation by atropine injection (P=0.30).
Table 6. Diabetes mellitus and tissue Doppler/myocardial strain.
| Year | First author | Journal | Main findings |
|---|---|---|---|
| 2003 | Fang (34) | J Am Coll Cardiol | Both patients with DM only and DM + HTN showed significant decreases in peak strain as well as peak strain rate compared with controls |
| 2004 | Fonseca (59) | Am J Cardiol | MRI tagging strain data: peak systolic strains and diastolic rates of relaxation are lower in patients who have T2DM and normal LVEF |
| 2006 | Chung (60) | J Am Coll Cardiol | MRI tagging strain data showed that paradoxical increase in myocardial torsion (3.5±0.9 vs. 2.7±0.4 °/cm; P<0.01) and torsion rate (0.013±0.003 vs. 0.010±0.002 °/cm/s; P=0.01) in patients with T1DM |
| 2006 | Moir (41) | Heart | Impaired strain and strain rate confirmed in T2DM but not associated with abnormal transmural flow |
| 2009 | Ng (61) | Am J Cardiol | The LV longitudinal systolic and diastolic functions were impaired, but the circumferential and radial functions were preserved in patients with uncomplicated T2DM |
| 2016 | Yang (62) | Open Heart | Patients with DM had impaired GLS and diastolic function |
| 2016 | Leung (63) | Circ Cardiovasc Imaging | Reversibility in diabetic cardiomyopathy with intensive treatment including optimization of treatment for blood glucose, blood pressure, and cholesterol |
DM, diabetes mellitus; HTN, hypertension; MRI, magnetic resonance imaging; T1DM, type 1 diabetes mellitus; T2DM, type 2 diabetes mellitus; LV, left ventricular; GLS, global longitudinal strain; LVEF, left ventricular ejection fraction.
Recently, Leung et al. reported possible reversibility in systolic and diastolic functions among patients with DM treated intensively (63). Subjects with T2DM and poor glycemic control received optimization of treatment for blood glucose, blood pressure, and cholesterol to recommended targets for 12 months. The improvement in HbA1c, from 10.3%±2.4% to 8.3%±2.0%, was associated with significant relative improvement in global longitudinal strain (GLS) of 21% and septal e' of 24%. A progressively greater improvement was observed in GLS as patients achieved a lower final HbA1c. Patients achieving an HbA1c of <7.0% had the highest improvement, whereas patients whose HbA1c worsened experienced a decline in GLS. Patients who improved their HbA1c by ≥1.0% had a significantly higher relative improvement in e' than those who did not (32% vs. 8%; P=0.003). These encouraging results lead us to the final section on treatment options.
Treatment options
Glycemic control agents: although good glycemic control is the main goal in the management of DM, a meta-analysis demonstrated that intensive glycemic control does not prevent HF (65). Metformin has been previously contraindicated, but recent data showed beneficial protective effects of the drug (66,67). A meta-analysis demonstrated that metformin was associated with reduced mortality [adjusted risk ratio 0.80 (0.74–0.87); P<0.001] (68). No increased risks were observed in those with reduced left ventricular ejection fraction (LVEF) or chronic kidney disease (CKD). Of note, no increased risk of lactic acidosis was found. Insulin has neutral effect on CVD outcome (69). Peroxisome proliferator-activated receptor (PPAR)-γ agonists increase the cardiovascular (CV) risk (70-74). Among the newer generation agents, including dipeptidyl peptidase-4 inhibitor (DPP-4i), glucagon-like peptide-1 receptor agonist (GLP-1 RA), and sodium-glucose cotransporter 2 inhibitors (SGLT2i), to date, DPP-4 inhibitor has demonstrated CV safety only without clear CV benefit (75). CV benefit has been shown in some of SGLT2i, such as empagliflozin (76) and canagliflozin (77), and GLP-1 RA, such as liraglutide (78) and semaglutide (79). Results from ongoing clinical trials are also underway: CREDENCE (ClinicalTrials.gov identifier: NCT02065791) and DECLARE-TIMI58 (ClinicalTrials.gov identifier: NCT01730534).
Of note, several cardioprotective agents have demonstrated their effectiveness among patients with DM. The effectiveness of angiotensin-converting enzyme (ACE) inhibitor in a population with DM has been confirmed in a meta-analysis (80). A discrepancy has been found among beta-blockers. Favorable effect of carvedilol has been confirmed in this population (81), but metoprolol has a neutral effect so far (82). Accordingly, ACCF/AHA Guidelines on HF recommend ACE inhibitors and beta-blockers for patients with DM, even without HF symptoms (stage A) (11).
Conclusions
Currently, diabetic cardiomyopathy is recognized as a real disease entity and is not a myth anymore. The underlying pathophysiological mechanism includes insulin resistance and cascades of metabolic disorders and autonomic disturbances, which result in clinical phenotype of LVH, diastolic dysfunction, fibrosis, and limited cardiac functional reserve. Recent reports suggest novel links between DM and valvular heart diseases, where mild degree of valvular disease may be associated with adverse prognosis. Myocardial strain analysis also demonstrated subclinical systolic dysfunction on top of diastolic dysfunction and possible reversibility. Collectively, careful cardiac imaging assessments including advanced techniques are crucial in the clinical management of patients with DM. Novel therapeutic agents, such as SGLT2i and DPP4i, are expected to improve these functions as a part of mechanisms explaining favorable prognostic effect on this population.
Acknowledgements
K Negishi is supported by an award from the Select Foundation, which had no role in the preparation of this manuscript.
Footnotes
Conflicts of Interest: The author has no conflicts of interest to declare.
References
- 1.Rubler S, Dlugash J, Yuceoglu YZ, et al. New type of cardiomyopathy associated with diabetic glomerulosclerosis. Am J Cardiol 1972;30:595-602. 10.1016/0002-9149(72)90595-4 [DOI] [PubMed] [Google Scholar]
- 2.Ernande L, Derumeaux G. Diabetic cardiomyopathy: myth or reality? Arch Cardiovasc Dis 2012;105:218-25. 10.1016/j.acvd.2011.11.007 [DOI] [PubMed] [Google Scholar]
- 3.Kannel WB, McGee DL. Diabetes and cardiovascular disease. The Framingham study. JAMA 1979;241:2035-8. 10.1001/jama.1979.03290450033020 [DOI] [PubMed] [Google Scholar]
- 4.Kannel WB, Hjortland M, Castelli WP. Role of diabetes in congestive heart failure: the Framingham study. Am J Cardiol 1974;34:29-34. 10.1016/0002-9149(74)90089-7 [DOI] [PubMed] [Google Scholar]
- 5.Gottdiener JS, Arnold AM, Aurigemma GP, et al. Predictors of congestive heart failure in the elderly: the Cardiovascular Health Study. J Am Coll Cardiol 2000;35:1628-37. 10.1016/S0735-1097(00)00582-9 [DOI] [PubMed] [Google Scholar]
- 6.Stratton IM, Adler AI, Neil HA, et al. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. BMJ 2000;321:405-12. 10.1136/bmj.321.7258.405 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Nichols GA, Hillier TA, Erbey JR, et al. Congestive heart failure in type 2 diabetes: prevalence, incidence, and risk factors. Diabetes Care 2001;24:1614-9. 10.2337/diacare.24.9.1614 [DOI] [PubMed] [Google Scholar]
- 8.Davis BR, Piller LB, Cutler JA, et al. Role of diuretics in the prevention of heart failure: the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial. Circulation 2006;113:2201-10. 10.1161/CIRCULATIONAHA.105.544031 [DOI] [PubMed] [Google Scholar]
- 9.Bertoni AG, Hundley WG, Massing MW, et al. Heart failure prevalence, incidence, and mortality in the elderly with diabetes. Diabetes Care 2004;27:699-703. 10.2337/diacare.27.3.699 [DOI] [PubMed] [Google Scholar]
- 10.Carr AA, Kowey PR, Devereux RB, et al. Hospitalizations for new heart failure among subjects with diabetes mellitus in the RENAAL and LIFE studies. Am J Cardiol 2005;96:1530-6. 10.1016/j.amjcard.2005.07.061 [DOI] [PubMed] [Google Scholar]
- 11.Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2013;62:e147-239. 10.1016/j.jacc.2013.05.019 [DOI] [PubMed] [Google Scholar]
- 12.Liu Q, Wang S, Cai L. Diabetic cardiomyopathy and its mechanisms: Role of oxidative stress and damage. J Diabetes Investig 2014;5:623-34. 10.1111/jdi.12250 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Boudina S, Abel ED. Diabetic cardiomyopathy revisited. Circulation 2007;115:3213-23. 10.1161/CIRCULATIONAHA.106.679597 [DOI] [PubMed] [Google Scholar]
- 14.Miki T, Yuda S, Kouzu H, et al. Diabetic cardiomyopathy: pathophysiology and clinical features. Heart Fail Rev 2013;18:149-66. 10.1007/s10741-012-9313-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Seferović PM, Paulus WJ. Clinical diabetic cardiomyopathy: a two-faced disease with restrictive and dilated phenotypes. Eur Heart J 2015;36:1718-27, 1727a-c. [DOI] [PubMed]
- 16.Jia G, DeMarco VG, Sowers JR. Insulin resistance and hyperinsulinaemia in diabetic cardiomyopathy. Nat Rev Endocrinol 2016;12:144-53. 10.1038/nrendo.2015.216 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Tenenbaum A, Motro M, Fisman EZ, et al. Functional class in patients with heart failure is associated with the development of diabetes. Am J Med 2003;114:271-5. 10.1016/S0002-9343(02)01530-9 [DOI] [PubMed] [Google Scholar]
- 18.Witteles RM, Tang WH, Jamali AH, et al. Insulin resistance in idiopathic dilated cardiomyopathy: a possible etiologic link. J Am Coll Cardiol 2004;44:78-81. 10.1016/j.jacc.2004.03.037 [DOI] [PubMed] [Google Scholar]
- 19.Seferovic JP, Claggett B, Seidelmann SB, et al. Effect of sacubitril/valsartan versus enalapril on glycaemic control in patients with heart failure and diabetes: a post-hoc analysis from the PARADIGM-HF trial. Lancet Diabetes Endocrinol 2017;5:333-40. 10.1016/S2213-8587(17)30087-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Wang Y, Negishi T, Negishi K, et al. Prediction of heart failure in patients with type 2 diabetes mellitus- a systematic review and meta-analysis. Diabetes Res Clin Pract 2015;108:55-66. 10.1016/j.diabres.2015.01.011 [DOI] [PubMed] [Google Scholar]
- 21.Galderisi M, Anderson KM, Wilson PW, et al. Echocardiographic evidence for the existence of a distinct diabetic cardiomyopathy (the Framingham Heart Study). Am J Cardiol 1991;68:85-9. 10.1016/0002-9149(91)90716-X [DOI] [PubMed] [Google Scholar]
- 22.Lee M, Gardin JM, Lynch JC, et al. Diabetes mellitus and echocardiographic left ventricular function in free-living elderly men and women: The Cardiovascular Health Study. Am Heart J 1997;133:36-43. 10.1016/S0002-8703(97)70245-X [DOI] [PubMed] [Google Scholar]
- 23.Devereux RB, Roman MJ, Paranicas M, et al. Impact of diabetes on cardiac structure and function: the strong heart study. Circulation 2000;101:2271-6. 10.1161/01.CIR.101.19.2271 [DOI] [PubMed] [Google Scholar]
- 24.Palmieri V, Bella JN, Arnett DK, et al. Effect of type 2 diabetes mellitus on left ventricular geometry and systolic function in hypertensive subjects: Hypertension Genetic Epidemiology Network (HyperGEN) study. Circulation 2001;103:102-7. 10.1161/01.CIR.103.1.102 [DOI] [PubMed] [Google Scholar]
- 25.Ilercil A, Devereux RB, Roman MJ, et al. Relationship of impaired glucose tolerance to left ventricular structure and function: The Strong Heart Study. Am Heart J 2001;141:992-8. 10.1067/mhj.2001.115302 [DOI] [PubMed] [Google Scholar]
- 26.Bella JN, Devereux RB, Roman MJ, et al. Separate and joint effects of systemic hypertension and diabetes mellitus on left ventricular structure and function in American Indians (the Strong Heart Study). Am J Cardiol 2001;87:1260-5. 10.1016/S0002-9149(01)01516-8 [DOI] [PubMed] [Google Scholar]
- 27.Rutter MK, Parise H, Benjamin EJ, et al. Impact of glucose intolerance and insulin resistance on cardiac structure and function: sex-related differences in the Framingham Heart Study. Circulation 2003;107:448-54. 10.1161/01.CIR.0000045671.62860.98 [DOI] [PubMed] [Google Scholar]
- 28.Galderisi M. Diastolic dysfunction and diabetic cardiomyopathy: evaluation by Doppler echocardiography. J Am Coll Cardiol 2006;48:1548-51. 10.1016/j.jacc.2006.07.033 [DOI] [PubMed] [Google Scholar]
- 29.van Heerebeek L, Hamdani N, Handoko ML, et al. Diastolic stiffness of the failing diabetic heart: importance of fibrosis, advanced glycation end products, and myocyte resting tension. Circulation 2008;117:43-51. 10.1161/CIRCULATIONAHA.107.728550 [DOI] [PubMed] [Google Scholar]
- 30.Mimbs JW, O'Donnell M, Bauwens D, et al. The dependence of ultrasonic attenuation and backscatter on collagen content in dog and rabbit hearts. Circ Res 1980;47:49-58. 10.1161/01.RES.47.1.49 [DOI] [PubMed] [Google Scholar]
- 31.Shapiro LM, Moore RB, Logan-Sinclair RB, et al. Relation of regional echo amplitude to left ventricular function and the electrocardiogram in left ventricular hypertrophy. Br Heart J 1984;52:99-105. 10.1136/hrt.52.1.99 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Pérez JE, McGill JB, Santiago JV, et al. Abnormal myocardial acoustic properties in diabetic patients and their correlation with the severity of disease. J Am Coll Cardiol 1992;19:1154-62. 10.1016/0735-1097(92)90316-F [DOI] [PubMed] [Google Scholar]
- 33.Di Bello V, Talarico L, Picano E, et al. Increased echodensity of myocardial wall in the diabetic heart: an ultrasound tissue characterization study. J Am Coll Cardiol 1995;25:1408-15. 10.1016/0735-1097(95)00026-Z [DOI] [PubMed] [Google Scholar]
- 34.Fang ZY, Yuda S, Anderson V, et al. Echocardiographic detection of early diabetic myocardial disease. J Am Coll Cardiol 2003;41:611-7. 10.1016/S0735-1097(02)02869-3 [DOI] [PubMed] [Google Scholar]
- 35.Zarich SW, Arbuckle BE, Cohen LR, et al. Diastolic abnormalities in young asymptomatic diabetic patients assessed by pulsed Doppler echocardiography. J Am Coll Cardiol 1988;12:114-20. 10.1016/0735-1097(88)90364-6 [DOI] [PubMed] [Google Scholar]
- 36.Celentano A, Vaccaro O, Tammaro P, et al. Early abnormalities of cardiac function in non-insulin-dependent diabetes mellitus and impaired glucose tolerance. Am J Cardiol 1995;76:1173-6. 10.1016/S0002-9149(99)80330-0 [DOI] [PubMed] [Google Scholar]
- 37.Liu JE, Palmieri V, Roman MJ, et al. The impact of diabetes on left ventricular filling pattern in normotensive and hypertensive adults: the Strong Heart Study. J Am Coll Cardiol 2001;37:1943-9. 10.1016/S0735-1097(01)01230-X [DOI] [PubMed] [Google Scholar]
- 38.Hansen A, Johansson BL, Wahren J, et al. C-peptide exerts beneficial effects on myocardial blood flow and function in patients with type 1 diabetes. Diabetes 2002;51:3077-82. 10.2337/diabetes.51.10.3077 [DOI] [PubMed] [Google Scholar]
- 39.Fang ZY, Schull-Meade R, Downey M, et al. Determinants of subclinical diabetic heart disease. Diabetologia 2005;48:394-402. 10.1007/s00125-004-1632-z [DOI] [PubMed] [Google Scholar]
- 40.Bajraktari G, Koltai MS, Ademaj F, et al. Relationship between insulin resistance and left ventricular diastolic dysfunction in patients with impaired glucose tolerance and type 2 diabetes. Int J Cardiol 2006;110:206-11. 10.1016/j.ijcard.2005.08.033 [DOI] [PubMed] [Google Scholar]
- 41.Moir S, Hanekom L, Fang ZY, et al. Relationship between myocardial perfusion and dysfunction in diabetic cardiomyopathy: a study of quantitative contrast echocardiography and strain rate imaging. Heart 2006;92:1414-9. 10.1136/hrt.2005.079350 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.From AM, Scott CG, Chen HH. Changes in diastolic dysfunction in diabetes mellitus over time. Am J Cardiol 2009;103:1463-6. 10.1016/j.amjcard.2009.01.358 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.From AM, Scott CG, Chen HH. The development of heart failure in patients with diabetes mellitus and pre-clinical diastolic dysfunction a population-based study. J Am Coll Cardiol 2010;55:300-5. 10.1016/j.jacc.2009.12.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Sacre JW, Franjic B, Jellis CL, et al. Association of cardiac autonomic neuropathy with subclinical myocardial dysfunction in type 2 diabetes. JACC Cardiovasc Imaging 2010;3:1207-15. 10.1016/j.jcmg.2010.09.014 [DOI] [PubMed] [Google Scholar]
- 45.Falcão-Pires I, Hamdani N, Borbély A, et al. Diabetes mellitus worsens diastolic left ventricular dysfunction in aortic stenosis through altered myocardial structure and cardiomyocyte stiffness. Circulation 2011;124:1151-9. 10.1161/CIRCULATIONAHA.111.025270 [DOI] [PubMed] [Google Scholar]
- 46.Poulsen MK, Dahl JS, Henriksen JE, et al. Left atrial volume index: relation to long-term clinical outcome in type 2 diabetes. J Am Coll Cardiol 2013;62:2416-21. 10.1016/j.jacc.2013.08.1622 [DOI] [PubMed] [Google Scholar]
- 47.Movahed MR, Hashemzadeh M, Jamal MM. Significant increase in the prevalence of non-rheumatic aortic valve disease in patients with type 2 diabetes mellitus. Exp Clin Endocrinol Diabetes 2007;115:105-7. 10.1055/s-2007-949656 [DOI] [PubMed] [Google Scholar]
- 48.Rossi A, Zoppini G, Benfari G, et al. Mitral Regurgitation and Increased Risk of All-Cause and Cardiovascular Mortality in Patients with Type 2 Diabetes. Am J Med 2017;130:70-6.e1. 10.1016/j.amjmed.2016.07.016 [DOI] [PubMed] [Google Scholar]
- 49.Kamalesh M, Ng C, El Masry H, et al. Does diabetes accelerate progression of calcific aortic stenosis? Eur J Echocardiogr 2009;10:723-5. 10.1093/ejechocard/jep048 [DOI] [PubMed] [Google Scholar]
- 50.Natorska J, Wypasek E, Grudzien G, et al. Does diabetes accelerate the progression of aortic stenosis through enhanced inflammatory response within aortic valves? Inflammation 2012;35:834-40. 10.1007/s10753-011-9384-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Vinereanu D, Nicolaides E, Tweddel AC, et al. Subclinical left ventricular dysfunction in asymptomatic patients with Type II diabetes mellitus, related to serum lipids and glycated haemoglobin. Clin Sci (Lond) 2003;105:591-9. 10.1042/CS20030168 [DOI] [PubMed] [Google Scholar]
- 52.Fang ZY, Najos-Valencia O, Leano R, et al. Patients with early diabetic heart disease demonstrate a normal myocardial response to dobutamine. J Am Coll Cardiol 2003;42:446-53. 10.1016/S0735-1097(03)00654-5 [DOI] [PubMed] [Google Scholar]
- 53.Palmieri V, Capaldo B, Russo C, et al. Left ventricular chamber and myocardial systolic function reserve in patients with type 1 diabetes mellitus: insight from traditional and Doppler tissue imaging echocardiography. J Am Soc Echocardiogr 2006;19:848-56. 10.1016/j.echo.2006.02.011 [DOI] [PubMed] [Google Scholar]
- 54.Ha JW, Lee HC, Kang ES, et al. Abnormal left ventricular longitudinal functional reserve in patients with diabetes mellitus: implication for detecting subclinical myocardial dysfunction using exercise tissue Doppler echocardiography. Heart 2007;93:1571-6. 10.1136/hrt.2006.101667 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Mizuno R, Fujimoto S, Saito Y, et al. Exercise-induced delayed onset of left ventricular early relaxation in association with coronary microcirculatory dysfunction in patients with diabetes mellitus. J Card Fail 2010;16:211-7. 10.1016/j.cardfail.2009.10.024 [DOI] [PubMed] [Google Scholar]
- 56.Cortigiani L, Gherardi S, Faggioni M, et al. Dual-Imaging Stress Echocardiography for Prognostic Assessment of High-Risk Asymptomatic Patients with Diabetes Mellitus. J Am Soc Echocardiogr 2017;30:149-58. 10.1016/j.echo.2016.10.003 [DOI] [PubMed] [Google Scholar]
- 57.Cortigiani L, Bigi R, Sicari R, et al. Prognostic value of pharmacological stress echocardiography in diabetic and nondiabetic patients with known or suspected coronary artery disease. J Am Coll Cardiol 2006;47:605-10. 10.1016/j.jacc.2005.09.035 [DOI] [PubMed] [Google Scholar]
- 58.Rana O, Byrne CD, Kerr D, et al. Acute hypoglycemia decreases myocardial blood flow reserve in patients with type 1 diabetes mellitus and in healthy humans. Circulation 2011;124:1548-56. 10.1161/CIRCULATIONAHA.110.992297 [DOI] [PubMed] [Google Scholar]
- 59.Fonseca CG, Dissanayake AM, Doughty RN, et al. Three-dimensional assessment of left ventricular systolic strain in patients with type 2 diabetes mellitus, diastolic dysfunction, and normal ejection fraction. Am J Cardiol 2004;94:1391-5. 10.1016/j.amjcard.2004.07.143 [DOI] [PubMed] [Google Scholar]
- 60.Chung J, Abraszewski P, Yu X, et al. Paradoxical increase in ventricular torsion and systolic torsion rate in type I diabetic patients under tight glycemic control. J Am Coll Cardiol 2006;47:384-90. 10.1016/j.jacc.2005.08.061 [DOI] [PubMed] [Google Scholar]
- 61.Ng AC, Delgado V, Bertini M, et al. Findings from left ventricular strain and strain rate imaging in asymptomatic patients with type 2 diabetes mellitus. Am J Cardiol 2009;104:1398-401. 10.1016/j.amjcard.2009.06.063 [DOI] [PubMed] [Google Scholar]
- 62.Yang H, Wang Y, Negishi K, et al. Pathophysiological effects of different risk factors for heart failure. Open Heart 2016;3:e000339. 10.1136/openhrt-2015-000339 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Leung M, Wong VW, Hudson M, et al. Impact of Improved Glycemic Control on Cardiac Function in Type 2 Diabetes Mellitus. Circ Cardiovasc Imaging 2016;9:e003643. 10.1161/CIRCIMAGING.115.003643 [DOI] [PubMed] [Google Scholar]
- 64.Ballo P, Cameli M, Mondillo S, et al. Impact of diabetes and hypertension on left ventricular longitudinal systolic function. Diabetes Res Clin Pract 2010;90:209-15. 10.1016/j.diabres.2010.08.004 [DOI] [PubMed] [Google Scholar]
- 65.Castagno D, Baird-Gunning J, Jhund PS, et al. Intensive glycemic control has no impact on the risk of heart failure in type 2 diabetic patients: evidence from a 37,229 patient meta-analysis. Am Heart J 2011;162:938-48.e2. 10.1016/j.ahj.2011.07.030 [DOI] [PubMed] [Google Scholar]
- 66.Masoudi FA, Inzucchi SE, Wang Y, et al. Thiazolidinediones, metformin, and outcomes in older patients with diabetes and heart failure: an observational study. Circulation 2005;111:583-90. 10.1161/01.CIR.0000154542.13412.B1 [DOI] [PubMed] [Google Scholar]
- 67.Aguilar D, Chan W, Bozkurt B, et al. Metformin use and mortality in ambulatory patients with diabetes and heart failure. Circ Heart Fail 2011;4:53-8. 10.1161/CIRCHEARTFAILURE.110.952556 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Eurich DT, Weir DL, Majumdar SR, et al. Comparative safety and effectiveness of metformin in patients with diabetes mellitus and heart failure: systematic review of observational studies involving 34,000 patients. Circ Heart Fail 2013;6:395-402. 10.1161/CIRCHEARTFAILURE.112.000162 [DOI] [PubMed] [Google Scholar]
- 69.ORIGIN Trial Investigators , Gerstein HC, Bosch J, et al. Basal insulin and cardiovascular and other outcomes in dysglycemia. N Engl J Med 2012;367:319-28. 10.1056/NEJMoa1203858 [DOI] [PubMed] [Google Scholar]
- 70.Nissen SE, Wolski K. Effect of rosiglitazone on the risk of myocardial infarction and death from cardiovascular causes. N Engl J Med 2007;356:2457-71. 10.1056/NEJMoa072761 [DOI] [PubMed] [Google Scholar]
- 71.Mahaffey KW, Hafley G, Dickerson S, et al. Results of a reevaluation of cardiovascular outcomes in the RECORD trial. Am Heart J 2013;166:240-9.e1. 10.1016/j.ahj.2013.05.004 [DOI] [PubMed] [Google Scholar]
- 72.Dormandy JA, Charbonnel B, Eckland DJ, et al. Secondary prevention of macrovascular events in patients with type 2 diabetes in the PROactive Study (PROspective pioglitAzone Clinical Trial In macroVascular Events): a randomised controlled trial. Lancet 2005;366:1279-89. 10.1016/S0140-6736(05)67528-9 [DOI] [PubMed] [Google Scholar]
- 73.Kernan WN, Viscoli CM, Furie KL, et al. Pioglitazone after Ischemic Stroke or Transient Ischemic Attack. N Engl J Med 2016;374:1321-31. 10.1056/NEJMoa1506930 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Lincoff AM, Tardif JC, Schwartz GG, et al. Effect of aleglitazar on cardiovascular outcomes after acute coronary syndrome in patients with type 2 diabetes mellitus: the AleCardio randomized clinical trial. JAMA 2014;311:1515-25. 10.1001/jama.2014.3321 [DOI] [PubMed] [Google Scholar]
- 75.Monami M, Dicembrini I, Mannucci E. Dipeptidyl peptidase-4 inhibitors and heart failure: a meta-analysis of randomized clinical trials. Nutr Metab Cardiovasc Dis 2014;24:689-97. 10.1016/j.numecd.2014.01.017 [DOI] [PubMed] [Google Scholar]
- 76.Zinman B, Wanner C, Lachin JM, et al. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N Engl J Med 2015;373:2117-28. 10.1056/NEJMoa1504720 [DOI] [PubMed] [Google Scholar]
- 77.Neal B, Perkovic V, Mahaffey KW, et al. Canagliflozin and Cardiovascular and Renal Events in Type 2 Diabetes. N Engl J Med 2017;377:644-57. 10.1056/NEJMoa1611925 [DOI] [PubMed] [Google Scholar]
- 78.Marso SP, Daniels GH, Brown-Frandsen K, et al. Liraglutide and Cardiovascular Outcomes in Type 2 Diabetes. N Engl J Med 2016;375:311-22. 10.1056/NEJMoa1603827 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Marso SP, Bain SC, Consoli A, et al. Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N Engl J Med 2016;375:1834-44. 10.1056/NEJMoa1607141 [DOI] [PubMed] [Google Scholar]
- 80.Shekelle PG, Rich MW, Morton SC, et al. Efficacy of angiotensin-converting enzyme inhibitors and beta-blockers in the management of left ventricular systolic dysfunction according to race, gender, and diabetic status: a meta-analysis of major clinical trials. J Am Coll Cardiol 2003;41:1529-38. 10.1016/S0735-1097(03)00262-6 [DOI] [PubMed] [Google Scholar]
- 81.Wedel H, Demets D, Deedwania P, et al. Challenges of subgroup analyses in multinational clinical trials: experiences from the MERIT-HF trial. Am Heart J 2001;142:502-11. 10.1067/mhj.2001.117600 [DOI] [PubMed] [Google Scholar]
- 82.Effect of metoprolol CR/XL in chronic heart failure: Metoprolol CR/XL Randomised Intervention Trial in Congestive Heart Failure (MERIT-HF). Lancet 1999;353:2001-7. 10.1016/S0140-6736(99)04440-2 [DOI] [PubMed] [Google Scholar]