

Abstract
Background
We aimed to investigate in patients with type 2 diabetes whether aortic stiffness is: (i) associated with glycaemic control, (ii) associated with adverse outcomes and (iii) can be reversed on treatment with RAAS inhibition.
Methods
Patients with type 2 diabetes (N = 94) and low vascular risk underwent assessment of cardiovascular risk and CMR assessment of ascending aortic distensibility (AAD), descending aortic distensibility (DAD) and aortic pulse wave velocity (PWV). Of these patients a subgroup with recent onset microalbuminuria (N = 25) were treated with renin–angiotensin–aldosterone system (RAAS) inhibition and imaging repeated after 1 year. All 94 patients were followed up for 2.4 years for major adverse cardiovascular disease (CVD) events including myocardial infarction detected on late gadolinium enhancement CMR.
Results
Ascending aortic distensibility, DAD and PWV all had a significant association with age and 24 h systolic blood pressure but only AAD had a significant association with glycaemic control, measured as HbA1c (Beta − 0.016, P = 0.04). The association between HbA1c and AAD persisted even after correction for age and hypertension. CVD events occurred in 19/94 patients. AAD, but not DAD or PWV, was associated with CVD events (hazard ratio 0.49, 95% confidence interval 0.25–0.95, P = 0.01). On treatment with RAAS inhibition, AAD, but not DAD or PWV, showed significant improvement from 1.51 ± 1.15 to 1.97 ± 1.07 10−3 mmHg−1, P = 0.007.
Conclusions
Ascending aortic distensibility measured by CMR is independently associated with poor glycaemic control and adverse cardiovascular events. Furthermore it may be reversible on treatment with RAAS inhibition. AAD is a promising marker of cardiovascular risk in asymptomatic patients with type 2 diabetes and has potential use as a surrogate cardiovascular endpoint in studies of novel hypoglycaemic agents.
Clinical trials registration https://clinicaltrials.gov/ct2/show/NCT01970319
Keywords: Cardiovascular magnetic resonance, Aortic distensibility, Pulse wave velocity, Cardiovascular risk, Renin–angiotensin–aldosterone
Introduction
With aging there is progressive stiffening of the aorta that appears to be accelerated by the presence of additional risk factors such as hypertension and diabetes [1]. Aortic stiffness can be assessed by cardiovascular magnetic resonance (CMR) either directly as aortic distensibility (AD) the relative change in aortic cross sectional area divide by pulse pressure; or indirectly as pulse wave velocity (PWV) the propagation speed of the velocity wave between two aortic locations. PWV is proportional to the square root AD by the Bramwell-Hill equation [2]. These techniques do not expose the patient to ionising radiation or contrast agent and can image three dimensional aortic characteristics at any point along the vessel [3].
Increased aortic stiffness can be detected in patients with type 2 diabetes with and without established cardiovascular disease by CMR [4–6] and applanation tonometry [7–10]. Although CMR measures of aortic stiffness have been shown to predict vascular morbidity [11, 12] studies specific to the diabetic population have not yet been conducted.
Patients with diabetes and microalbuminuria have even further elevated cardiovascular risk [13, 14]. Data from clinical trials suggests that the use of renin–angiotensin–aldosterone system (RAAS) inhibition in this patient group may reduce this risk [15, 16]. It has been shown that AD and PWV measured by CMR can be improved by RAAS inhibition in other high risk disease cohorts [17, 18] but this principle is not yet been tested in diabetes.
We aimed to investigate in patients with type 2 diabetes whether aortic stiffness is: (i) associated with glycaemic control, (ii) associated with adverse outcomes and (iii) can be reversed on treatment with RAAS inhibition. We also aimed to compare three CMR measures of aortic stiffness including ascending aortic distensibility (AAD), descending aortic distensibility (DAD) and aortic pulse wave velocity (PWV).
Methods
We measured aortic stiffness by CMR in 94 asymptomatic patients with type 2 diabetes from a cohort of 100 patients with type 2 diabetes studied to investigate the relationship between microalbuminuria, cardiac remodelling and fibrosis (Fig. 1) [19, 20]. Patients were recruited from 30 primary care health centres in the local area between August 2013 and March 2015 [20]. Exclusion criteria for all subjects were known cardiac disease, kidney disease (eGFR < 30 ml/min/1.73 m2), uncontrolled hypertension, treatment with insulin or angiotensin converting enzyme (ACE) inhibitor/angiotensin receptor blocker (ARB). All patients underwent 24 h blood pressure (BP) monitoring with a Welch-Allyn 6100 ambulatory blood pressure monitor. All HbA1c measurements since diagnosis were recorded from review of records.
Fig. 1.
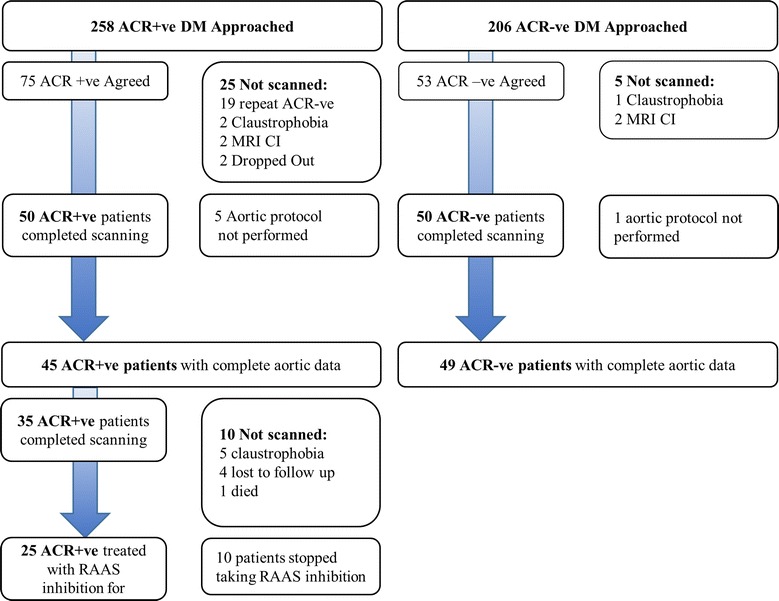
Flow chart of patient recruitment
We specifically recruited patients with persistent microalbuminuria (N = 45) who were due to be started on an ACE inhibitor by their primary care team following the baseline investigations [21]. ACE inhibitors were uptitrated to maximum tolerated dose and those who could not tolerate an ACE inhibitor because of cough were changed to an ARB. All testing was repeated after 1 year treatment with RAAS inhibition. In addition 20 age and sex matched healthy controls underwent identical CMR studies.
The study was approved by the National Research Ethics Service (13/YH/0098) and conducted in accordance with the declaration of Helsinki. All subjects gave informed written consent.
CMR protocol
Patients and controls underwent CMR using an identical protocol on a dedicated cardiovascular 3 Tesla Philips Achieva system equipped with a 32 channel coil and MultiTransmit® technology.
For aortic distensibility, brachial artery blood pressure was recorded by Dinamap (Critikon, Tampa, USA) immediately prior to high temporal resolution multi-phase SSFP cine imaging (retrospective gating, slice thickness 10 mm, acquired spatial resolution 1.2 × 1.2 mm, acquired temporal resolution 50 phases, repetition time 2.6 ms, echo time 1.3 ms, breath-held, acquired transverse to the ascending and descending thoracic aorta at the level of the pulmonary artery bifurcation) (Fig. 2) [4]. Aortic PWV was assessed using identical geometric planning with retrospectively gated, through-plane, phase-contrast velocity encoded images (single slice, 10 mm thick, acquired spatial resolution 2.9 × 2.9 mm, acquired temporal resolution 50 phases, repetition time 4.7 ms, echo time 2.8 ms, typical FOV 320, and VENC 200 cm/s, breath-held).
Fig. 2.
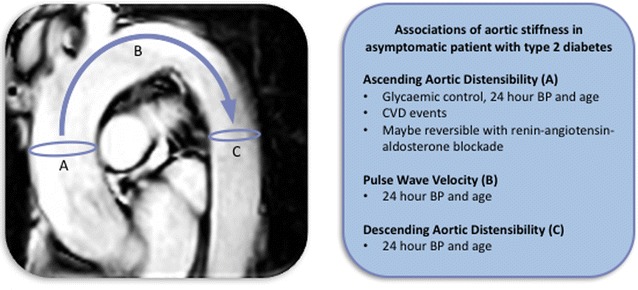
Associations of three measures of aortic stiffness in asymptomatic patients with type 2 diabetes
Late gadolinium enhancement (LGE) imaging of the heart was carried out more than 6 min after contrast injection (0.15 mmol/kg Gadovist, Bayer Pharma) using inversion recovery-prepared T1-weighted echo. The optimal inversion time to null signal from normal myocardium was determined using a Look-Locker approach (acquired spatial resolution 1.54 × 1.76 mm, TR 3.5 ms, TE 2.0 ms, flip angle 25°, breath-held) performed in 10–12 short axis slices with further slices acquired in the vertical and horizontal long axis orientations, phase-swapped or imaged in systole, if indicated based on LGE imaging obtained or wall-motion abnormality.
CMR interpretation
Cardiovascular magnetic resonance data were assessed quantitatively using commercially available software (CVI42, Circle Cardiovascular Imaging Inc. Calgary, Canada) blinded to glycaemic status. To derive the aortic distensibility of the ascending and descending thoracic aorta, cross sectional measurements were made by manual planimetry of the endovascular-blood pool interface for each phase to determine the maximal and minimal aortic dimensions. Aortic distensibility (mmHg−1) was calculated using the equation:
Aortic PWV (m/s) was calculated by dividing the distance separating two locations and the transit time needed to cover this distance [22]. Analysis was performed using a validated software (PMI v0.4, https://github.com/plaresmedima/PMI-0.4-Runtime-CMRLeeds) based on IDL 6.4 (ITT Visual Information Systems, Boulder, USA) [23]. The distance between the ascending and descending aorta was measured manually from the sagittal/oblique cines of the aortic arch. Transit time was calculated using the foot–foot delay method from velocity encoded images of the ascending and descending aorta, manually contoured to derive velocity–time curves [24].
The presence of silent MI was identified by two physicians experienced (5 and 15 years) in CMR interpretation based upon typical subendocardial distribution of LGE present.
Laboratory methods
Cholesterol, hsCRP and microalbumin were measured on Siemens Advia (Siemens Healthcare Diagnostics, Camberley, UK) with typical coefficient of variability (CV) 0.94, 3.7 and 2.2%, respectively. HbA1c was measured on Tosoh G8 (Tosoh Bioscience, Tessenderlo, Belgium) with typical CV 1.4%. Serum aldosterone was measured in the SAS Steroid Centre (Leeds Teaching Hospitals) with an in-house radio-immunoassay with typical CV 11% at 218 pmol/L.
Follow up
Patients were followed up by review of electronic and clinical records for CVD events including cardiovascular death, myocardial infarction (either silent detected on LGE CMR or clinically recognised during the follow up period), stroke, heart failure or arrhythmia.
Statistical analysis
Statistical analysis was performed using IBM SPSS® Statistics 22.0 (IBM Corp., Armonk, NY). Continuous variables were expressed as mean ± SD. Categorical variables were expressed as N (%). Logistic regression was performed to identify clinical and aortic parameters associated with CVD events over follow up. Univariable linear regression was performed to identify associations between clinical parameters and AAD, DAD and PWV. Only factors with a significant association on univariable regression (P < 0.05) were included in multivariable linear regression. In those who underwent treatment with RAAS inhibition paired t tests were used to compare parameters before and after treatment. When normally distributed, data are presented as mean ± SD. P < 0.05 was considered statistically significant.
Results
Ninety-four patients had a CMR protocol that included aortic imaging and were included in this study. Patients had a mean age of 61 ± 11 years (range 32–86), Table 1. 81% of participants were male with mean duration of diabetes of 5 ± 5 years and HbA1c of 62 ± 16 mmol/mol. The majority were on metformin therapy (88%) with 34% receiving, a sulphonylurea 34, 10% a gliptin and only 4% took another hypoglycaemic agent (exanatide, pioglitazone, dapagliflozin and repaglinide, in one patient each). On 24 h ambulatory monitoring, blood pressure was well controlled at 131 ± 15/72 ± 9 mmHg. Only 13% of patients were taking an antihypertensive which included a calcium channel blocker 11%, a diuretic 4% and a beta blocker 3%. Twenty age and sex matched healthy controls were recruited with 7 (70%) male, mean age 56 ± 11, clinic blood pressure 127 ± 10/77 ± 9 mmHg and HbA1c of 38 ± 3 mmol/mol.
Table 1.
Baseline Characteristics presented as mean ± standard deviation for continuous or N (%) for categorical data
| Diabetes mellitus | Control | P value | |
|---|---|---|---|
| N | 94 | 20 | |
| Age (years) | 60.8 ± 11.1 | 57.2 ± 11.6 | 0.72 |
| Male gender, n (%) | 76 (81) | 14 (70) | 0.34 |
| Body mass index, kg/m2 | 28.7 ± 4.3 | – | – |
| Duration of diabetes, years | 5.1 ± 4.5 | – | – |
| HbA1c, mmol/mol | 61.6 ± 15.6 | 37.1 ± 4.6 | < 0.0001 |
| Median HbA1c since diagnosis, mmol/mol | 63.8 ± 15.2 | – | – |
| Maximum HbA1c since diagnosis, mmol/mol | 85.0 ± 24.6 | – | – |
| Microalbuminuria, n (%) | 45 (48) | – | – |
| Systolic BP, mmHga | 131.1 ± 15.2 | 127.8 ± 15.5 | 0.93 |
| Diastolic BP, mmHga | 72.3 ± 9.0 | 76.9 ± 10.3 | 0.05 |
| Total cholesterol, mmol/L | 4.3 ± 1.1 | 5.2 ± 0.9 | 0.003 |
| Smoking | 15 (16) | 0 | – |
| Metformin | 83 (88) | 0 | – |
| Sulphonylurea | 32 (34) | 0 | – |
| Gliptin | 10 (11) | 0 | – |
| Other hypoglycaemic | 4 (4) | 0 | – |
| Insulin | 0 | 0 | – |
| ACE inhibitor | 0 | 0 | – |
| Beta blocker | 3 (3) | 0 | – |
| Calcium channel blocker | 10 (11) | 1 (5) | 0.44 |
| Diuretic | 4 (4) | 0 | – |
| Statin | 66 (70) | 3 (15) | < 0.0001 |
| Aspirin | 16 (17) | 2 (10) | 0.43 |
| Serum aldosterone, pmol/L | 306.3 ± 18.8 | – | – |
| High sensitivity C reactive protein, mg/L | 3.5 ± 5.5 | – | – |
| Ascending aortic distensibility, 10−3 mmHg−1 | 1.81 ± 1.16 | 2.78 ± 1.67 | 0.002 |
| Descending aortic distensibility, 10−3 mmHg−1 | 2.11 ± 1.05 | 3.47 ± 1.54 | 0.0002 |
| Pulse wave velocity, m/s | 8.00 ± 2.87 | 7.58 ± 2.11 | 0.74 |
ACE angiotensin converting enzyme, CVD cardiovascular disease
a24 h blood pressure in patients with diabetes mellitus, clinic blood pressure in controls
Baseline AAD was 1.81 ± 1.16 10−3 mmHg−1, DAD was 2.11 ± 1.05 10−3 mmHg−1 and PWV was 8.00 ± 2.87 m/s. In healthy controls AAD was 2.78 ± 1.67 10−3 mmHg−1, DAD was 3.47 ± 1.54 10−3 mmHg−1 and PWV was 7.58 ± 2.11 m/s. AAD and DAD were significantly lower in patients with diabetes than matched controls (P = 0.002 and 0.0002 respectively). The difference in PWV was not significant (P = 0.74).
Association between demographic and risk factors and aortic parameters
Ascending aortic distensibility had significant associations with age (Beta − 0.063, P < 0.0001), current HbA1c (Beta − 0.016, P = 0.04), maximum HbA1c since diagnosis (Beta − 0.011, P = 0.02), sulphonylurea use (Beta − 0.57, P = 0.02) and 24 h systolic blood pressure (Beta − 0.026, P = 0.001), Table 2. On multivariable linear regression associations with age, current HbA1c and 24 h systolic BP remained significant: Age (Beta − 0.068, P < 0.0001), current HbA1c (Beta − 0.017, P = 0.007) and 24 h systolic BP (Beta − 0.014, P = 0.03). In this regression model maximum HbA1c was of borderline significance (Beta − 0.0077, P = 0.05) but sulphonylurea use was no longer significant (Beta − 0.12, P = 0.53).
Table 2.
Linear regression of association between aortic stiffness and clinical factors with significant associations in italic
| AAD | DAD | PWV | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Beta | 95% CI | P value | Beta | 95% CI | P value | Beta | 95% CI | P value | |
| Age | − 0.063 | − 0.080; − 0.046 | < 0.0001 | − 0.052 | − 0.068; 0.036 | < 0.0001 | 0.11 | 0.064; 0.16 | < 0.0001 |
| Male gender | 0.13 | − 0.47; 0.73 | 0.69 | − 0.18 | − 0.73; 0.36 | 0.50 | 0.11 | − 1.39; 1.61 | 0.88 |
| Body mass index | 0.0042 | − 0.051; 0.060 | 0.88 | − 0.030 | − 0.080; 0.020 | 0.24 | − 0.30 | − 0.17; 0.11 | 0.67 |
| Duration of diabetes | − 0.037 | − 0.090; 0.016 | 0.17 | − 0.040 | − 0.090; 0.0050 | 0.08 | 0.087 | − 0.044; 0.22 | 0.19 |
| HbA1c | − 0.016 | − 0.031; − 0.00073 | 0.04 | − 0.00037 | − 0.014; 0.013 | 0.96 | 0.027 | − 0.010; 0.065 | 0.15 |
| Median HbA1c since diagnosis | − 0.013 | − 0.029; 0.0026 | 0.10 | 0.00084 | − 0.013; 0.015 | 0.91 | 0.019 | − 0.020; 0.058 | 0.33 |
| Maximum HbA1c since diagnosis | − 0.011 | − 0.020; − 0.0014 | 0.02 | − 0.0035 | − 0.012; 0.0050 | 0.42 | 0.0083 | − 0.016; 0.032 | 0.50 |
| Microalbuminuria | − 0.21 | − 0.69; 0.26 | 0.37 | − 0.21 | − 0.64; 0.22 | 0.34 | 0.89 | − 0.28; 2.06 | 0.13 |
| 24 h systolic BP | − 0.026 | − 0.040; − 0.011 | 0.001 | − 0.020 | − 0.034; − 0.0067 | 0.004 | 0.040 | 0.0014; 0.078 | 0.04 |
| 24 h diastolic BP | − 0.0058 | − 0.033; 0.021 | 0.67 | − 0.0027 | − 0.027; − 0.022 | 0.83 | − 0.0015 | − 0.068; 0.065 | 0.97 |
| Total cholesterol | 0.15 | − 0.062; 0.36 | 0.16 | 0.056 | − 0.14; 0.25 | 0.57 | − 0.44 | − 0.97; 0.081 | 0.10 |
| Smoking | 0.11 | − 0.54; 0.76 | 0.74 | 0.098 | − 0.49; 0.69 | 0.74 | − 0.59 | − 2.20; 1.02 | 0.47 |
| Metformin | 0.27 | − 0.47; 1.01 | 0.47 | 0.35 | − 0.31; 1.02 | 0.30 | 0.32 | − 2.16; 1.51 | 0.73 |
| Sulphonylurea | − 0.57 | − 1.06; − 0.08 | 0.02 | 0.34 | − 0.79; 0.11 | 0.14 | 1.17 | − 0.056; 2.39 | 0.06 |
| Gliptin | − 0.31 | − 1.08; 0.46 | 0.43 | 0.14 | − 0.57; 0.83 | 0.70 | 0.73 | − 1.18; 2.64 | 0.45 |
| Statin | − 0.048 | − 0.57; 0.47 | 0.86 | − 0.13 | − 0.60; 0.35 | 0.60 | 0.38 | − 0.91; 1.67 | 0.56 |
| Aspirin | − 0.61 | − 1.23; 0.012 | 0.06 | − 0.51 | − 1.08; − 0.51 | 0.07 | 1.10 | − 0.46; 2.66 | 0.16 |
Significant associations in italics
Abbreviations as in Table 1
DAD had significant associations with age (Beta − 0.052, P < 0.0001) and 24 h systolic BP (Beta − 0.020, P = 0.004) but no indices related to diabetes. PWV had significant associations with age (Beta 0.11, P < 0.0001) and 24 h systolic BP (Beta 0.040, P = 0.04) but no indices related to diabetes.
Cardiovascular disease events
Patients were followed up for 882 ± 146 days. 19 patients (20%) had a CVD event including silent MI on baseline scan 15 (16%), stroke 3 (3%), cardiovascular death 2 (2%), ST elevation MI 2 (2%), silent MI on follow up scan 1 (1%), percutaneous coronary intervention 2 (2%), heart failure 1 (1%) and arrhythmia 1 (1%). 9/19 subjects with CVD events were asymptomatic and were only detected on CMR. 1 patient died from non-cardiovascular causes (malignancy).
The differences in aortic stiffness between those with silent MI on baseline scan (N = 15) and without silent MI did not reach statistical significance (AAD 1.33 ± 0.89 vs 1.90 ± 1.19 10−3 mmHg−1, P = 0.0.8; DAD 1.76 ± 1.13 vs 2.18 ± 1.03 10−3 mmHg−1 P = 0.12; PWV 8.31 ± 2.14 vs 7.94 ± 3.00 m/s).
On logistic regression of the aortic parameters only AAD had a significant association with CVD events; hazard ratio (HR) 0.49, 95% confidence interval (CI) 0.25–0.95, P = 0.01, Table 3. The associations of DAD and PWV with CVD events were not significant (P = 0.19 and 0.45 respectively). Smoking was the only individual risk factor to have a trend to association with CVD events (HR 3.38, 95% CI 1.03–11.15, P = 0.05).
Table 3.
Logistic regression of the association between aortic stiffness and clinical factors with CVD events
| Hazard ratio | 95% CI | P value | |
|---|---|---|---|
| AAD | 0.49 | (0.25; 0.95) | 0.01 |
| DAD | 0.70 | (0.41; 1.20) | 0.19 |
| PWV | 1.07 | (0.90; 1.26) | 0.45 |
| Age | 1.05 | (1.00; 1.10) | 0.07 |
| Gender | 0.19 | (0.02; 1.52) | 0.12 |
| Body mass index | 0.97 | (0.86; 1.09) | 0.62 |
| Duration of diabetes | 0.99 | (0.88; 1.10) | 0.80 |
| HbA1c | 0.98 | (0.95; 1.02) | 0.35 |
| Median HbA1c since diagnosis | 1.01 | (0.97; 1.04) | 0.75 |
| Maximum HbA1c since diagnosis | 1.00 | (0.97; 1.02) | 0.74 |
| Microalbuminuria | 2.19 | (0.77; 6.16) | 0.13 |
| 24 h systolic BP | 1.02 | (0.99; 1.06) | 0.18 |
| 24 h diastolic BP | 1.01 | (0.95; 1.06) | 0.80 |
| Total cholesterol | 0.89 | (0.56; 1.43) | 0.64 |
| Smoking | 3.38 | (1.03; 11.15) | 0.05 |
| Serum aldosterone | 1.00 | (0.99; 1.00) | 0.33 |
| High sensitivity C reactive protein | 0.99 | (0.90; 1.09) | 0.87 |
Significant associations in italics
CI confidence interval, AAD ascending aorta distensibility, DAD descending aorta distensibility, PWV pulse wave velocity, CVD cardiovascular disease
Response of aortic stiffness to RAAS inhibition
25 patients with persistent microalbuminuria were treated with RAAS inhibition and had a repeat CMR 365 ± 38 days after the initial scan. Prescribed RAAS inhibition included ramipril 19, losartan 3, perindopril 1, candesartan 1, irbesartan 1 equivalent to a dose of ramipril 4.9 ± 3.1 mg. RAAS inhibition was associated with a non-significant decrease in blood pressure of 5 ± 16 mmHg in systolic and 3 ± 8 mmHg in diastolic blood pressures. Over follow up there was no significant change in weight (86.2 ± 11.1 to 86.7 ± 11.5 kg, P = 0.51) or HbA1c (60.1 ± 17.7 to 61.8 ± 14.7 mmol/mol, P = 0.57). Treatment with RAAS inhibition was associated with a significant increase in AAD of 0.47 ± 1.04 10−3 mmHg−1 but no significant change in DAD or PWV (P = 0.92 and 0.42 respectively). After treatment with RAAS inhibition AAD was increased but was still significantly lower than in healthy controls (1.97 ± 1.07 10−3 mmHg−1 vs 2.78 ± 1.67 10−3 mmHg−1, P = 0.04) (Table 4).
Table 4.
Baseline characteristics and change in AAD, DAD and PWV after 1 year treatment with RAAS inhibition in 25 subjects
| Baseline | Follow up | P value | |
|---|---|---|---|
| Age | 64.2 ± 11.8 | ||
| Male gender, N (%) | 22 (88%) | ||
| Body mass index, kg/m2 | 29.1 ± 3.4 | ||
| Duration of diabetes, years | 5.2 ± 4.5 | ||
| HbA1c, % | 7.6 ± 1.5 | ||
| HbA1c, mmol/mol | 60.1 ± 17.7 | ||
| Median HbA1c since diagnosis, mmol/mol | 63.4 ± 17.6 | ||
| Maximum HbA1c since diagnosis, mmol/mol | 86.6 ± 25.6 | ||
| 24 h systolic BP, mmHg | 136.7 ± 19.3 | 131.6 ± 20.9 | 0.12 |
| 24 h diastolic BP, mmHg | 72.9 ± 10.1 | 70.7 ± 11.1 | 0.07 |
| Total cholesterol, mmol/L | 4.1 ± 1.0 | ||
| Smoking, N (%) | 4 (16%) | ||
| Serum aldosterone, pmol/L | 337.0 ± 190.8 | 238.8 ± 138.2 | 0.11 |
| AAD (10−3 mmHg−1) | 1.51 ± 1.15 | 1.97 ± 1.07 | 0.007 |
| DAD (10−3 mmHg−1) | 1.98 ± 1.29 | 1.96 ± 1.10 | 0.92 |
| PWV (m/s) | 8.95 ± 2.60 | 8.33 ± 3.58 | 0.42 |
Significant associations in italics
Abbreviations as in Table 1
Discussion
We have demonstrated increased aortic stiffness by CMR in asymptomatic patients with type 2 diabetes compared to healthy controls. We have also shown that AAD, DAD and PWV are significantly influenced by age and 24 h systolic BP. However only AAD had an association with HbA1c, which remained significant after correction for age and BP. AAD had a significant association with CVD events over 2.4 years follow up. Furthermore, no other traditional cardiovascular risk factors or marker of glycaemic control had an association with CVD events. Finally, we have shown with RAAS inhibition that AAD improves towards that of healthy controls.
The findings that AAD is associated with glycaemic control, adverse CVD events and that it is improved on treatment suggest that AAD has a potential role as an imaging marker of cardiovascular risk in asymptomatic patients with type 2 diabetes, although the cost and availability of CMR may be prohibitive for routine clinical use.
AAD and glycaemia
In the present study AAD was the only parameter of aortic stiffness to have a significant association with glycaemic control, independent of blood pressure. Previous studies have shown an association between dysglycaemia and PWV [25, 26] but previous CMR studies showing that diabetes is associated with decreased AAD were either not powered to show an association with glycaemic control [4, 5, 27] or data on glycaemic agents and glycaemic control were not reported [6]. The association of AAD with sulphonylurea therapy is potentially interesting as it may implicate hypoglycaemia in the observed changes in AAD. However, this relationship was not significant after correction for HbA1c suggesting it is merely a marker of worse glycaemic control. Taken together, glycaemic control appears to influence AAD and hence glucose levels may play a direct role in stiffening of the aorta. Preliminary data suggests that aortic stiffness may be reduced by the sodium-glucose co-transporter-2 inhibitor dapagliflozin [28] and larger studies are required to confirm whether this is mediated by glucose lowering or other mechanisms.
AAD and CVD events
In the present study decreasing AAD appeared to be a marker of cardiovascular disease events, independently of conventional risk factors. The association between AAD and outcome in patients with diabetes are in agreement with previous studies demonstrating the prognostic importance of AAD measured by CMR in asymptomatic cohorts of patients of varied cardiovascular risk (including a minority with diabetes). AAD was measured in 3675 subjects from the Multi-Ethnic Study of Atherosclerosis study who were followed up for 8.5 years [11]. In this period decreased AAD was associated with increased all-cause mortality and CVD events (myocardial infarction, stroke, cardiac arrest and cardiovascular death). This risk was independent of conventional risk factors. In the Dallas Heart Study, both AAD and PWV were measured using CMR in 2122 participants free from cardiovascular disease [12]. After correction for traditional risk factors AAD and PWV had weak associations with nonfatal cardiac events and nonfatal extra-cardiac events but not cardiovascular death.
The prognostic importance of aortic PWV has been extensively studied by applanation tonometry with clear evidence of an incremental benefit over traditional risk factors for the prediction of cardiovascular events [29]. This technique has been used specifically in patients with diabetes and has shown that PWV is increased in diabetes independently of BP and associated with increased mortality [30]. PWV was not associated with CVD events in the present study and may reflect measurement of flow in a shorter section of aorta (arch only in our study compared with carotid to distal abdominal aorta by tonometry) or significantly worse temporal resolution than with tonometry.
Reversing AAD
A subgroup of 25 patients in the present study were treated with RAAS inhibition for newly diagnosed microalbuminuria. In these patients RAAS inhibition was associated with a significant increase in AAD (but not DAD or PWV). It is well recognised that patients with albuminuria have markedly elevated cardiovascular risk [13, 14] which may in part be reduced by RAAS inhibition [15, 16]. Although only an observational finding we believe that ours is the first study to show that aortic stiffness associated with diabetes can be reduced by medical intervention. A previous randomised study has shown that RAAS modulation with spironolactone can decrease aortic stiffness in patients with chronic kidney disease [17]. Our findings suggest the same might be true in diabetes although larger randomised trials are needed to establish whether decreasing aortic stiffness by RAAS inhibition leads to improved outcomes.
Recent trials of hypoglycaemic agents in type 2 diabetes have included patients with established CVD [31] or at risk of CVD [32] and have shown that it is possible to improve CVD outcomes in these patient groups. AAD measured by CMR has the potential to be used as a surrogate endpoint in future studies of hypoglycaemic agents to identify those with increased CVD risk who are most likely to demonstrate mortality benefit. Furthermore AAD could easily be added to a scan protocol including comprehensive assessment of cardiac structure function and tissue characteristics.
Limitations
This was an observational non-randomised study and the interventional component needs to be repeated in a larger randomised study, although it can be argued that this is a strength as patient selection was limited and they were studied under real life, and not randomised controlled trial, conditions. 9/19 patients with CVD events were asymptomatic with MI being detected on LGE CMR. However in patients with diabetes the mortality associated with unrecognised MI is significant and is comparable to those with clinically recognised MI [33, 34]. The temporal resolution of the CMR PWV was at least 10 times lower than that achieved by tonometry and the lack of association between PWV and glycaemia or CVD events may reflect a limitation of the technique used. There was a male preponderance in this cohort reflecting the different cut-offs for ACR, which may have influenced our findings. The blood pressure measurement for AD calculation was performed peripherally which due to the pressure amplification phenomenon could lead to overestimation of stiffness, although the identical protocol was used for all subjects therefore minimising bias.
Conclusions
Ascending aortic distensibility measured by CMR is independently associated with poor glycaemic control and adverse cardiovascular events. Furthermore, it appears to be reversible on treatment with RAAS inhibition. AAD is a promising marker of cardiovascular risk in asymptomatic patients with type 2 diabetes and has potential use as a surrogate cardiovascular endpoint in studies of novel hypoglycaemic agents.
Authors’ contributions
Study design PPS, RA, KKW, MTK, JHB, JPG, SP; patient scanning PS, BE, AKM, PG, TAM, LED; scan analysis BE, RK, PS; statistical analysis PS; initial drafting of manuscript, PS, BE, RK. All authors read and approved the final manuscript.
Acknowledgements
This work would not have been possible without the assistance of the team of research nurses led by Petra Bijsterveld and radiographers including Gavin Bainbridge, Stephen Mhiribii, Margaret Saysell and Caroline Richmond.
Competing interests
KKW and MTK have received research funding from Medtronic UK. Other authors have no disclosures.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Consent for publication
All authors consent to publication of this manuscript.
Ethics approval and consent to participate
The study was approved by the National Research Ethics Service (13/YH/0098) and conducted in accordance with the declaration of Helsinki. All subjects gave informed written consent.
Funding
This work was supported by British Heart Foundation fellowships FS/12/88/29901 to PPS and FS/1062/28409 to SP, National Institute for Health Research (NIHR) clinical lectureship to PS and the NIHR Leeds Clinical Research Facility. The views expressed are those of the authors and not necessarily those of the NHS, NIHR or the Department of Health.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Abbreviations
- AAD
ascending aortic distensibility
- ACE
angiotensin converting enzyme
- ARB
angiotensin receptor blocker
- BP
blood pressure
- CMR
cardiovascular magnetic resonance
- CV
coefficient of variability
- CVD
cardiovascular disease
- DAD
descending aortic distensibility
- LGE
late gadolinium enhancement
- PWV
pulse wave velocity
- RAAS
renin–angiotensin–aldosterone system
Contributor Information
Peter P. Swoboda, Phone: +441133925909, Email: p.swoboda@leeds.ac.uk
Bara Erhayiem, Email: b.erhayiem@leeds.ac.uk.
Rachel Kan, Email: um11rleh@leeds.ac.uk.
Adam K. McDiarmid, Email: a.k.mcdiarmid@leeds.ac.uk
Pankaj Garg, Email: p.garg@leeds.ac.uk.
Tarique A. Musa, Email: t.a.musa@leeds.ac.uk
Laura E. Dobson, Email: l.dobson@leeds.ac.uk
Klaus K. Witte, Email: k.k.witte@leeds.ac.uk
Mark T. Kearney, Email: m.t.kearney@leeds.ac.uk
Julian H. Barth, Email: Julian.barth@nhs.net
Ramzi Ajjan, Email: r.ajjan@leeds.ac.uk.
John P. Greenwood, Email: j.greenwood@leeds.ac.uk
Sven Plein, Email: s.plein@leeds.ac.uk.
References
- 1.Cavalcante JL, Lima JA, Redheuil A, Al-Mallah MH. Aortic stiffness: current understanding and future directions. J Am Coll Cardiol. 2011;57(14):1511–1522. doi: 10.1016/j.jacc.2010.12.017. [DOI] [PubMed] [Google Scholar]
- 2.Laurent S, Cockcroft J, Van Bortel L, Boutouyrie P, Giannattasio C, Hayoz D, Pannier B, Vlachopoulos C, Wilkinson I, Struijker-Boudier H, et al. Expert consensus document on arterial stiffness: methodological issues and clinical applications. Eur Heart J. 2006;27(21):2588–2605. doi: 10.1093/eurheartj/ehl254. [DOI] [PubMed] [Google Scholar]
- 3.Whitlock MC, Hundley WG. Noninvasive imaging of flow and vascular function in disease of the aorta. JACC Cardiovasc Imaging. 2015;8(9):1094–1106. doi: 10.1016/j.jcmg.2015.08.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Lee JM, Shirodaria C, Jackson CE, Robson MD, Antoniades C, Francis JM, Wiesmann F, Channon KM, Neubauer S, Choudhury RP. Multi-modal magnetic resonance imaging quantifies atherosclerosis and vascular dysfunction in patients with type 2 diabetes mellitus. Diabetes Vasc Dis Res. 2007;4(1):44–48. doi: 10.3132/dvdr.2007.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.van der Meer RW, Diamant M, Westenberg JJ, Doornbos J, Bax JJ, de Roos A, Lamb HJ. Magnetic resonance assessment of aortic pulse wave velocity, aortic distensibility, and cardiac function in uncomplicated type 2 diabetes mellitus. J Cardiovasc Magn Reson. 2007;9(4):645–651. doi: 10.1080/10976640601093703. [DOI] [PubMed] [Google Scholar]
- 6.Stacey RB, Bertoni AG, Eng J, Bluemke DA, Hundley WG, Herrington D. Modification of the effect of glycemic status on aortic distensibility by age in the multi-ethnic study of atherosclerosis. Hypertension. 2010;55(1):26–32. doi: 10.1161/HYPERTENSIONAHA.109.134031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Webb DR, Khunti K, Silverman R, Gray LJ, Srinivasan B, Lacy PS, Williams B, Davies MJ. Impact of metabolic indices on central artery stiffness: independent association of insulin resistance and glucose with aortic pulse wave velocity. Diabetologia. 2010;53(6):1190–1198. doi: 10.1007/s00125-010-1689-9. [DOI] [PubMed] [Google Scholar]
- 8.Cardoso CR, Ferreira MT, Leite NC, Salles GF. Prognostic impact of aortic stiffness in high-risk type 2 diabetic patients: the Rio de Janeiro Type 2 Diabetes Cohort Study. Diabetes Care. 2013;36(11):3772–3778. doi: 10.2337/dc13-0506. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Chen Q, Chiheb S, Fysekidis M, Jaber Y, Brahimi M, Nguyen MT, Millasseau S, Cosson E, Valensi P. Arterial stiffness is elevated in normotensive type 2 diabetic patients with peripheral neuropathy. Nutr Metab Cardiovasc Dis. 2015;25(11):1041–1049. doi: 10.1016/j.numecd.2015.08.001. [DOI] [PubMed] [Google Scholar]
- 10.Ferreira MT, Leite NC, Cardoso CR, Salles GF. Correlates of aortic stiffness progression in patients with type 2 diabetes: importance of glycemic control: the Rio de Janeiro type 2 diabetes cohort study. Diabetes Care. 2015;38(5):897–904. doi: 10.2337/dc14-2791. [DOI] [PubMed] [Google Scholar]
- 11.Redheuil A, Wu CO, Kachenoura N, Ohyama Y, Yan RT, Bertoni AG, Hundley GW, Duprez DA, Jacobs DR, Jr, Daniels LB, et al. Proximal aortic distensibility is an independent predictor of all-cause mortality and incident CV events: the MESA study. J Am Coll Cardiol. 2014;64(24):2619–2629. doi: 10.1016/j.jacc.2014.09.060. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Maroules CD, Khera A, Ayers C, Goel A, Peshock RM, Abbara S, King KS. Cardiovascular outcome associations among cardiovascular magnetic resonance measures of arterial stiffness: the Dallas heart study. J Cardiovasc Magn Reson. 2014;16:33. doi: 10.1186/1532-429X-16-33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Gerstein HC, Mann JF, Yi Q, Zinman B, Dinneen SF, Hoogwerf B, Halle JP, Young J, Rashkow A, Joyce C, et al. Albuminuria and risk of cardiovascular events, death, and heart failure in diabetic and nondiabetic individuals. JAMA. 2001;286(4):421–426. doi: 10.1001/jama.286.4.421. [DOI] [PubMed] [Google Scholar]
- 14.Schiffrin EL, Lipman ML, Mann JF. Chronic kidney disease: effects on the cardiovascular system. Circulation. 2007;116(1):85–97. doi: 10.1161/CIRCULATIONAHA.106.678342. [DOI] [PubMed] [Google Scholar]
- 15.de Zeeuw D, Remuzzi G, Parving HH, Keane WF, Zhang Z, Shahinfar S, Snapinn S, Cooper ME, Mitch WE, Brenner BM. Albuminuria, a therapeutic target for cardiovascular protection in type 2 diabetic patients with nephropathy. Circulation. 2004;110(8):921–927. doi: 10.1161/01.CIR.0000139860.33974.28. [DOI] [PubMed] [Google Scholar]
- 16.Cheng J, Zhang W, Zhang X, Han F, Li X, He X, Li Q, Chen J. Effect of angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers on all-cause mortality, cardiovascular deaths, and cardiovascular events in patients with diabetes mellitus: a meta-analysis. JAMA Intern Med. 2014;174(5):773–785. doi: 10.1001/jamainternmed.2014.348. [DOI] [PubMed] [Google Scholar]
- 17.Edwards NC, Steeds RP, Stewart PM, Ferro CJ, Townend JN. Effect of spironolactone on left ventricular mass and aortic stiffness in early-stage chronic kidney disease: a randomized controlled trial. J Am Coll Cardiol. 2009;54(6):505–512. doi: 10.1016/j.jacc.2009.03.066. [DOI] [PubMed] [Google Scholar]
- 18.Ripley DP, Negrou K, Oliver JJ, Worthy G, Struthers AD, Plein S, Greenwood JP. Aortic remodelling following the treatment and regression of hypertensive left ventricular hypertrophy: a cardiovascular magnetic resonance study. Clin Exp Hypertens. 2015;37(4):308–316. doi: 10.3109/10641963.2014.960974. [DOI] [PubMed] [Google Scholar]
- 19.Swoboda PP, McDiarmid AK, Erhayiem B, Haaf P, Kidambi A, Fent GJ, Dobson LE, Musa TA, Garg P, Law GR, et al. A novel and practical screening tool for the detection of silent myocardial infarction in patients with type 2 diabetes. J Clin Endocrinol Metab. 2016;101(9):3316–3323. doi: 10.1210/jc.2016-1318. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Swoboda PP, McDiarmid AK, Erhayiem B, Ripley DP, Dobson LE, Garg P, Musa TA, Witte KK, Kearney MT, Barth JH, et al. Diabetes mellitus, microalbuminuria, and subclinical cardiac disease: identification and monitoring of individuals at risk of heart failure. J Am Heart Assoc. 2017;6(7):e005539. doi: 10.1161/JAHA.117.005539. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Sibal L, Home PD. Management of type 2 diabetes: nICE guidelines. Clin Med. 2009;9(4):353–357. doi: 10.7861/clinmedicine.9-4-353. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Oliver JJ, Webb DJ. Noninvasive assessment of arterial stiffness and risk of atherosclerotic events. Arterioscler Thromb Vasc Biol. 2003;23(4):554–566. doi: 10.1161/01.ATV.0000060460.52916.D6. [DOI] [PubMed] [Google Scholar]
- 23.Huber A, Sourbron S, Klauss V, Schaefer J, Bauner KU, Schweyer M, Reiser M, Rummeny E, Rieber J. Magnetic resonance perfusion of the myocardium: semiquantitative and quantitative evaluation in comparison with coronary angiography and fractional flow reserve. Investig Radiol. 2012;47(6):332–338. doi: 10.1097/RLI.0b013e31824f54cb. [DOI] [PubMed] [Google Scholar]
- 24.Ibrahim ESH, Johnson KR, Miller AB, Shaffer JM, White RD. Measuring aortic pulse wave velocity using high-field cardiovascular magnetic resonance: comparison of techniques. J Cardiovasc Magn Reson. 2010;12:26. doi: 10.1186/1532-429X-12-26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Kozakova M, Morizzo C, Fraser AG, Palombo C. Impact of glycemic control on aortic stiffness, left ventricular mass and diastolic longitudinal function in type 2 diabetes mellitus. Cardiovasc Diabetol. 2017;16(1):78. doi: 10.1186/s12933-017-0557-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Homsi R, Sprinkart AM, Gieseke J, Meier-Schroers M, Yuecel S, Fischer S, Nadal J, Dabir D, Luetkens JA, Kuetting DL, et al. Cardiac magnetic resonance based evaluation of aortic stiffness and epicardial fat volume in patients with hypertension, diabetes mellitus, and myocardial infarction. Acta Radiol. 2018;59(1):65–71. doi: 10.1177/0284185117706201. [DOI] [PubMed] [Google Scholar]
- 27.Khan JN, Wilmot EG, Leggate M, Singh A, Yates T, Nimmo M, Khunti K, Horsfield MA, Biglands J, Clarysse P, et al. Subclinical diastolic dysfunction in young adults with type 2 diabetes mellitus: a multiparametric contrast-enhanced cardiovascular magnetic resonance pilot study assessing potential mechanisms. Eur Heart J Cardiovasc Imaging. 2014;15(11):1263–1269. doi: 10.1093/ehjci/jeu121. [DOI] [PubMed] [Google Scholar]
- 28.Solini A, Giannini L, Seghieri M, Vitolo E, Taddei S, Ghiadoni L, Bruno RM. Dapagliflozin acutely improves endothelial dysfunction, reduces aortic stiffness and renal resistive index in type 2 diabetic patients: a pilot study. Cardiovasc Diabetol. 2017;16(1):138. doi: 10.1186/s12933-017-0621-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Vlachopoulos C, Aznaouridis K, Stefanadis C. Prediction of cardiovascular events and all-cause mortality with arterial stiffness: a systematic review and meta-analysis. J Am Coll Cardiol. 2010;55(13):1318–1327. doi: 10.1016/j.jacc.2009.10.061. [DOI] [PubMed] [Google Scholar]
- 30.Cruickshank K, Riste L, Anderson SG, Wright JS, Dunn G, Gosling RG. Aortic pulse-wave velocity and its relationship to mortality in diabetes and glucose intolerance: an integrated index of vascular function? Circulation. 2002;106(16):2085–2090. doi: 10.1161/01.CIR.0000033824.02722.F7. [DOI] [PubMed] [Google Scholar]
- 31.Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, Hantel S, Mattheus M, Devins T, Johansen OE, Woerle HJ, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med. 2015;373(22):2117–2128. doi: 10.1056/NEJMoa1504720. [DOI] [PubMed] [Google Scholar]
- 32.Marso SP, Daniels GH, Brown-Frandsen K, Kristensen P, Mann JF, Nauck MA, Nissen SE, Pocock S, Poulter NR, Ravn LS, et al. Liraglutide and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2016;375(4):311–322. doi: 10.1056/NEJMoa1603827. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Kwong RY, Chan AK, Brown KA, Chan CW, Reynolds HG, Tsang S, Davis RB. Impact of unrecognized myocardial scar detected by cardiac magnetic resonance imaging on event-free survival in patients presenting with signs or symptoms of coronary artery disease. Circulation. 2006;113(23):2733–2743. doi: 10.1161/CIRCULATIONAHA.105.570648. [DOI] [PubMed] [Google Scholar]
- 34.Schelbert EB, Cao JJ, Sigurdsson S, Aspelund T, Kellman P, Aletras AH, Dyke CK, Thorgeirsson G, Eiriksdottir G, Launer LJ, et al. Prevalence and prognosis of unrecognized myocardial infarction determined by cardiac magnetic resonance in older adults. JAMA. 2012;308(9):890–896. doi: 10.1001/2012.jama.11089. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.