

Abstract
Rationale
The relationship of functional parameters such as lung mechanics, chest kinematics, metabolism and peripheral and respiratory muscle function with the level of exercise tolerance remains a controversial subject. While it has been previously shown that pulmonary rehabilitation is capable of improving exercise tolerance in patients afflicted by COPD, as expressed by values of 6-minute walking test (6MWT), the degree of contribution to this change by each of the aforementioned parameters remains unclear.
Aims
To investigate the correlation between changes in exercise capacity and other functional markers following pulmonary rehabilitation in COPD and to determine which parameters are more closely related to improvements of exercise tolerance.
Materials and methods
Three hundred and twenty-seven patients with COPD (with average, 95% CI for forced expiratory volume in the first second [FEV1]: 45% [25%–83%] predicted, age: 64 [48–80] years, and BMI: 27 [13.5–40.4] kg/m2) participated in this study. Thirty percent of the patients had pulmonary hypertension as comorbidity. Patients underwent a pulmonary rehabilitation program with 20–30 minutes sessions two to three times per day for 4 weeks. The program was composed of chest wall-stretching, controlled breathing exercises, and a personalized training schedule for cycling and treadmill use. Measurements of 6MWT, lung function, chest wall expansion, grip strength, maximal inspiratory pressure, and breath holding time were taken. The Body mass index, airflow Obstruction, Dyspnea and Exercise capacity (BODE-index), body mass index [BMI], FEV1, 6MWT, modified Medical Research Dyspnea Scale score, and an alternative scale score (for BMI, FEV1, 6MWT, and COPD Assessment Test) were calculated.
Results
Rehabilitation resulted in a generalized improvement in 6MWT among patients (average: 360 [95% CI: 178–543 m] vs average: 420 [95% CI: 238–601 m], p<0.05). Improvements in exercise tolerance were found to be most closely associated with changes in composite BODE-index (R2=−0.6), Alternative Scale (R2=−0.56), dyspnea score (modified Medical Research Dyspnea Scale R2=−0.54), and health status (COPD Assessment Test R2=−0.4, p<0.05). In addition, improvements in exercise tolerance were found to moderately correlate with improvements in inspiratory vital capacity (IVC, R2=0.34, p<0.05). Post-rehabilitation changes in IVC displayed a connection with grip strength (R2=0.6) and chest expansion (R2=0.48).
Conclusion
Enhancements in exercise tolerance had correlation with changes in IVC, BODE-index, and the new Alternative Scale. However, comprehensive assessment needs to include considerations of chest kinematics and peripheral and respiratory muscle function as well.
Keywords: exercise tolerance, lung mechanics, respiratory and peripheral muscle function, breath holding time, health status
Introduction
The conservation of effective lung mechanics is closely associated with the proper function of the two phases of respiration. In inspiration, the diaphragmatic contraction and the action of external intercostal muscles lead to an increase in the vertical and horizontal diameters of the chest, respectively.1 However, as observed in the pathologic lung mechanics of COPD patients, the appropriate operation of these muscular mechanisms can be compromised as a result of dynamic hyperinflation. This is attributed to the higher values of end-expiratory and end-inspiratory lung volumes. This dysfunction contributes to the limitation of the exercise capacity in COPD.1
The malfunction of lung mechanics is further compounded by respiratory muscle weakness as seen in patients with severe stage COPD and COPD-associated weight loss.2 This respiratory muscle weakness can be directly correlated to increased breathlessness and reduced exercise tolerance.2 The strength and force of the respiratory muscles can be improved by specific strength and endurance respiratory muscle training as components of pulmonary rehabilitation.2
General health status can be evaluated by COPD Assessment Test (CAT), which is related to the global health status of the patients (coughing, quantity of sputum, ability to do physical work, and energy level).3 The modified Medical Research Council (mMRC) dyspnea score shows the manifestation of dyspnea during different levels of effort.4 The Body mass index, airflow Obstruction, Dyspnea and Exercise capacity (BODE-index) characterizes the severity of COPD in a complex way (based on body mass index [BMI], forced expiratory volume in the first second [FEV1], mMRC, and 6-minute walking distance [6MWD]).5
Pulmonary rehabilitation is one of the main contributors to improve exercise tolerance in COPD. We sought to discover the strength of correlation between improvements of exercise tolerance and enhancements in lung mechanics, chest kinematics, metabolism, peripheral and respiratory muscle function.
Materials and methods
Three hundred twenty-seven patients with COPD (FEV1: 45%±19% predicted, age: 64±8 years, BMI: 27±7 kg/m2) participated in this study conducted by the National Koranyi Institute for Pulmonology (Table 1). Thirty percent of the observed patients also suffered from pulmonary hypertension (PH). Written informed consent was obtained from all of the patients who participated in the study (Department of Pulmonary Rehabilitation). The study protocol was approved by the Ethical Committee of the National Koranyi Institute for Pulmonology with the registration number 25/2017.
Table 1.
Patients’ demographic, lung function, comorbidity, and smoking habit characteristics
| Characteristics, N=327 | |
|---|---|
| Age (years) | 64±8 |
| Male/female | 181/146 |
| BMI (kg/m2) | 27±7 |
| FEV1 (% predicted) | 45±19 |
| Hypertension | 257 (79%) |
| Diabetes | 85 (26%) |
| Pulmonary hypertension | 104 (32%) |
| Quitting of smoking | 245 (75%) |
Note: Data presented as mean ± SD, n/n, and n (%).
Abbreviations: BMI, body mass index; FEV1, forced expiratory volume in the first second.
Patients underwent a complex pulmonary rehabilitation program comprising chest wall-stretching, physiotherapy, controlled breathing techniques, and a personalized exercise schedule two to three times per day consisting of 20–30 minutes of cycling and treadmill for 4 weeks. The personalized exercises were adjusted according to patients’ BORG scoring (dyspnea and leg fatigue) and the individual patient requirements, with changes in duration and intensity being made with the intent of maintaining a BORG scale of 7 as stated in international guidelines.6 The protocol was defined considering the stage of COPD, the actual status of the heart and other comorbidities, blood gas value, and history of exacerbations.6
Training exercises performed by our patients were at a high intensity and were either continuous or with intervals. While controversy exists regarding the effectiveness of different modalities of supervised exercise training, such as continuous (C), interval (I), and self-paced (S) programs, a previous study conducted by our research group has given credence only to the use of continuous and interval forms of supervised training schedules.7 In this previous study, patients in group C exercised at 80% of pretraining peak work rate in an incremental cycle ergometer test. In group I, training consisted of 30 minutes of cycling, 2 minutes at 90%, followed by 1 minute at 50% peak work rate, bracketed by 7.5 minutes at 50% peak work rate.7 A similar protocol was used in our current work. Patients with PH were referred to the interval training group.
Breathing exercises were performed in an open-air corridor to take advantage of the special microclimate of the hospital. The patients were taught controlled breathing and stretching techniques and performed muscle strengthening exercises followed by chest and spine mobilization.6,8
The parameters evaluated were the 6-minute walking test (6MWT), lung function, chest wall expansion (CWE), grip strength, maximal inspiratory pressure (MIP), and breath-holding time (BHT). Health status and dyspnea were measured by CAT, mMRC, BODE-index, and the new Alternative Scale.3,4,9–11,19
In summary, our rehabilitation program contained a combination of both endurance and strength components, with resistance training being conducted in the mornings and aerobic training performed on either bicycle or treadmill in a personalized format that took into account patient health status and the related comorbidities.
It should be noted that the intensity and complexity of this program were greater than that of most commonly used rehabilitation protocols, which on average consist of a similar subset of exercises once per day for three times a week. However, it should also be stated that, despite its higher intensity, the 4-week duration of our rehabilitation protocol is less than that of similar programs.
Measurements
Measurements of the following parameters were recorded before, during, and after rehabilitation.
Pulmonary function
According to American Thoracic Society/European Respiratory Society guidelines, all patients underwent post-bronchodilator pulmonary function testing (Vmax 229 and Autobox 6200; Sensormedics, Yorba Linda, CA, USA) including spirometry measurements.12 COPD patients inhaled 400 μg of salbutamol 20 minutes before testing. We measured dynamic spirometry values, FEV1, forced vital capacity (FVC), airway obstruction (FEV1/FVC), and resting slow vital capacity (VC), which represent a reference point of chest hyperinflation.
Six-minute walking test
The 6MWT was measured in the corridor of our department. Before, during, and after the test, oxygen saturation and heart rate were measured and a modified Borg scale was evaluated as per the international guideline. Patients were instructed to walk as fast as possible.13,14
Chest wall expansion
CWE was measured as the difference in chest circumferences between deep inspiration and expiration at the level of xiphoid process.8,15 Measurements were repeated three times and the average of the three obtained values was calculated.
Maximal inspiratory pressure
To evaluate MIP, we used a special digital instrument referred to as the Power Breathe K1 (POWERbreathe International Limited, Southam, UK). Measurements were made in relation to the patient’s height, weight, age, and gender, with the intent of calculating the degree of diaphragmatic force during inspiration. Results were classified as “very poor,” “poor,” “average,” “fair,” “good,” and “very good.” Patients were asked to inhale suddenly with maximal force after a maximal exhalation.16 Measurements were repeated three times and the average of the three obtained values was calculated.
Breath-holding time
Respiratory peripheral neural afferents which are activated by breath-holding and dyspnea perception may interact with the neural circuit responsible for processing of motor output. Following maximal inspiration, the subjects were asked to hold their breath for as long as possible, while keeping their nose and mouth shut and refraining from further inhalation.17,18
Grip strength measurement
Kern handgrip dynamometer (2016 Kern and Sohn GmbH, Balingen, Germany) was used to identify the peripheral muscle force.19,20 Measurements were repeated three times and the average of the three obtained values was calculated.
Health status questionnaire and dyspnea score
Health status was evaluated using the CAT marker test,3,8 and dyspnea was screened using mMRC scoring.4,10 The tests were conducted both before and after rehabilitation.
Bode-index
BODE-index was calculated based on BMI, FEV1, 6MWD, and mMRC.10
Alternative Scale
A new Alternative Scale was developed by our group. Similar to the BODE-index, the new Alternative Scale was based on BMI, FEV1, and 6MWD. In our new Alternative Scale, however, the mMRC scoring utilized by the BODE-index was replaced by the CAT-questionnaire (CAT 0–10= mMRC 1 score, 11–20= mMRC 2 scores, 21–30= mMRC 3 scores, 31–40= mMRC 4 scores).11
Statistical analysis
Patient characteristics, lung function, resting and exercise functional variables were compared by a paired t-test, a nonparametric sign test, and a Wilcoxon signed-rank test. Significance was accepted at p<0.05 level. The distribution around the mean was expressed as ±SD in tables. Scatterplot distribution was observed in figures. Distributions were tested for normality by the Kolmogorov–Smirnov test. Pearson correlation coefficient was calculated between the change in functional parameters and the health status markers.
Results
Rehabilitation resulted in improvements of the 6MWD (360±93 vs 420±92 m, p<0.05), as shown in Figure 1. Exercise tolerance had stronger correlation with changes in the composite, dyspnea, and health status scores (BODE-index R2=−0.6, Alternative Scale R2=−0.56, mMRC R2=−0.54, CAT-questionnaire R2=−0.4; p<0.05), as compared to alterations in other functional parameters (Table 2).
Figure 1.
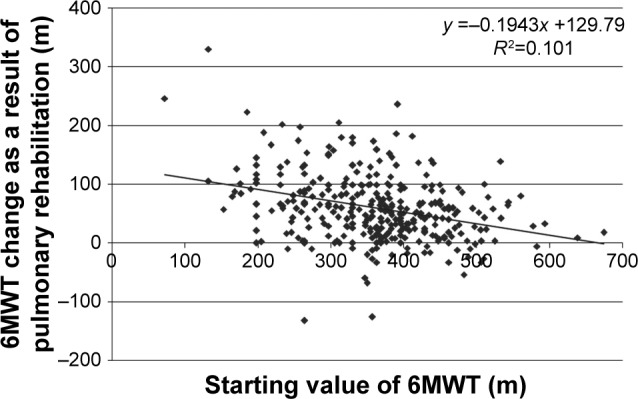
Scatterplot of 6-minutes walking test (6MWD in m) between values at the start of rehabilitation and the change as an effect of rehabilitation.
Abbreviation: 6MWD, 6-minute walking distance.
Table 2.
Correlation between 6MWD and other functional markers
| Demographic and functional parameters | 6MWD |
|---|---|
| BODE-index | −0.6 |
| Alternative Scale | −0.56 |
| mMRC | −0.54 |
| CAT | −0.4 |
| IVC (L) | 0.34 |
| IVC% | 0.27 |
| Breath holding time | 0.24 |
| FEV1 | 0.22 |
| FVC | 0.22 |
| Grip strength | 0.2 |
| Chest wall expansion | 0.2 |
| Age | −0.18 |
| FEV1/FVC | 0.16 |
| BMI | 0.12 |
Abbreviations: 6MWD, 6-minute walking distance; BMI, body mass index; BODE-index, Body mass index, airflow Obstruction, Dyspnea and Exercise capacity; CAT, COPD Assessment Test; FEV1, forced expiratory volume in the first second; FVC, forced vital capacity; IVC, inspiratory vital capacity; mMRC, modified Medical Research Dyspnea Scale.
However, analysis of lung mechanics revealed that higher inspiratory vital capacity (IVC) (L) with R2=0.48 and grip strength (R2=0.35) were correlated with improved chest kinematics (CWE), a lower degree of dynamic hyperinflation, and increased exercise tolerance. In addition, further interactions between IVC and other functional parameters were observed. Strong correlations between hand grip strength (R2=0.6) and IVC (L) were found and, in turn, moderate correlation was noted between BHT and hand grip strength (R2=0.35), as shown in Table 3. IVC% correlated with both BODE-index (R2=−0.53) and the newly created Alternative Scale (R2=−0.5), as shown in Table 3. Furthermore, the degree of airway obstruction, as expressed by FEV1 values, was found to be directly related to the degree of hyperinflation, which exists in a relation of inverse proportionality to IVC% (R2=0.67). Thus, we believe that IVC represents one of the most important factors in predicting exercise intolerance, and it should be noted that, improved IVC dynamics were observed as a result of pulmonary rehabilitation (Figure 2).
Table 3.
Correlation between IVC (L) and other functional markers
| Demographic and functional parameters | IVC (L) |
|---|---|
| Gender | −0.6 |
| Grip strength | 0.6 |
| IVC% | 0.57 |
| FVC | 0.51 |
| Chest wall expansion | 0.48 |
| BODE-index | −0.39 |
| Stage of COPD | −0.36 |
| FEV1 | 0.35 |
| Breath holding time | 0.35 |
| 6MWD | 0.34 |
| Alternative Scale | −0.34 |
| mMRC | −0.26 |
| CAT | −0.16 |
| BMI | 0.05 |
Abbreviations: 6MWD, 6-minute walking distance; BMI, body mass index; BODE-index, Body mass index, airflow Obstruction, Dyspnea and Exercise capacity; CAT, COPD Assessment Test; FEV1, forced expiratory volume in the first second; FVC, forced vital capacity; IVC, inspiratory vital capacity; mMRC, modified Medical Research Dyspnea Scale.
Figure 2.
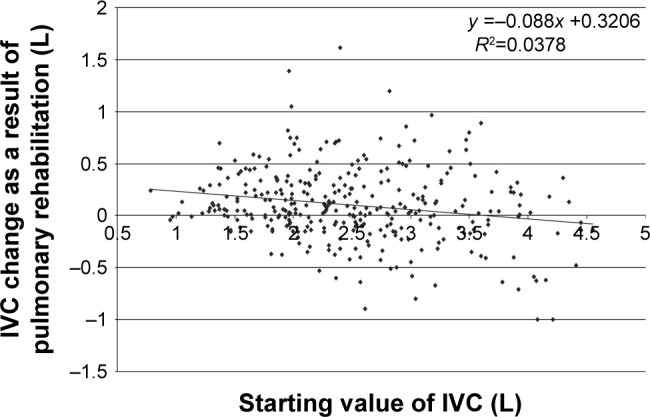
Scatterplot of inspiratory vital capacity (IVC) between the values at the start of rehabilitation and the change as an effect of rehabilitation.
Finally, a number of secondary, but notable, observations were made in the duration of our study. The FVC was found to be correlated with both the BODE-index (R2=−0.51) and the Alternative Scale (R2=−0.5) equally. FEV1 also displayed a strong influence in the composite scores as a part of the BODE-index (R2=−0.72) and in the Alternative Scale (R2=−0.7).
Discussion
We conducted clinical research about the relationship between functional and health status markers and the effectiveness of pulmonary rehabilitation in increasing exercise tolerance. Pulmonary rehabilitation resulted in an improvement of 6MWT. Correlations were found between improvement in 6MWD and the BODE-index, the Alternative Scale, and the mMRC. IVC was determined to be an important factor in predicting exercise intolerance. Post-rehabilitation changes to IVC were related to grip strength and chest expansion.
For the analysis of the role of respiratory muscles, Aliverti et al conducted a clinical study describing the actions of human respiratory muscles in healthy patients during quiet breathing and gradually increasing workload.23 They found that the pressure of diaphragm increased 2-fold, the velocity of shortening changed 6.5-fold, and the workload of diaphragm became 13-fold greater during exercise.21–23 The diaphragm acted as a flow generator. Throughout our study, we observed an increase in MIP. We believe that changes in MIP are a result of rehabilitation procedures that lead to strengthening of the diaphragmatic muscle. We strongly support that this enhancement of respiratory muscle is one of the major elements in the reduction of exercise intolerance that our rehabilitation program was able to produce. Thus, the recorded MIP, which is associated with the function of inspiratory muscles, can improve as a result of respiratory rehabilitation.
The chest wall kinematics of patients afflicted by ankylosing spondylitis were examined by Romagnoli et al in 2004.24 In this study, it was hypothesized that ankylosing spondylitis results in limitations of chest movement. The stiffening of the respiratory apparatus resulted in the need for greater integration of the abdominal and diaphragmatic musculatures in respiration. A similar stiffening of the chest was noted in patients included in our study, followed by a similar shift in emphasis of related musculature during respiration. It has been deduced that the mechanical changes accompanying chest stiffness play a significant role in COPD symptomatology and deterioration of lung mechanics and exercise capacity.
The deficiencies in neuromuscular strength and chest wall mechanics, which accompany COPD, were investigated in a clinical study conducted by Alter et al in 2017.25 Evidence of neuromuscular uncoupling was observed where the increased respiratory drive in patients with inappropriately high CO2, such as COPD patients, was unable to elicit a sufficiently high increase in respiratory muscle strength. This was later found to exist in relation to respiratory muscle insufficiency secondary to dynamic hyperinflation of the chest. The expansion of the chest cavity seen in dynamic hyperinflation was shown to result in respiratory muscle overstretch, compromising the ability of respiratory muscles to enhance their output in correct proportion to the increased neurologic signals.25 The consequence of these pathologic changes was neuromuscular weakness. Ultimately, this manifested clinically as dyspnea, poor exercise capacity, and decreased quality of life, cementing the importance of neuromuscular weakness to decreased exercise tolerance.25
In addition, there is increasing evidence that acute dynamic increases in lung hyperinflation, under conditions of worsening expiratory flow limitation and increased ventilator demand, can severely stress cardiopulmonary reserves, particularly in patients with more advanced disease in COPD.26 Our understanding of the physiologic mechanisms of dynamic lung hyperinflation during both physical activity and exacerbations in COPD continues to grow, together with an appreciation of its serious negative mechanical and sensory consequences.27 Dynamic hyperinflation can develop in COPD parallel with expiratory flow limitation. Inspiration begins before expiration ends, end-expiratory lung volume increases, inspiratory reserve volume decreases, and exercise intolerance appears.26–31
Overall, lung hyperinflation is a staple of expiratory flow limitation in patients with COPD and contributes importantly to dyspnea and activity limitation.22,23 Beyond respiratory muscle weakness induced by overstretch, lung hyperinflation can contribute to insufficiency of the respiratory apparatus through alterations in the anatomic position of the ribs and the diaphragm, leading to shortening of the diaphragmatic fibers. It is not surprising, therefore, that lung hyperinflation has become an important therapeutic target in symptomatic COPD patients.26 Through observation of our rehabilitation program, we have come to support that inspiratory muscle training plays an important role in correcting these problems and in improving exercise capacity.28,29
Physical activity, peripheral and respiratory muscle strength are reduced in patients with PH. In a clinical study, respiratory muscle strength and its relationship with spirometry parameters, exercise capacity, physical activity level, quality of life, and pulmonary hemodynamics were investigated in patients with PH.32 MIP and maximal expiratory pressure values of the patients with PH were significantly lower than those of age- and gender-matched healthy controls.32 The relationship between maximum inspiratory pressure, exercise capacity, and physical activity level showed that a decrease in exercise capacity or physical activity level may be a predictor for decreased MIP.32 On the basis of this observation, we also found reduced MIP and 6MWD in 30% of our COPD patients in this study who also suffered from PH.
There was a question about whether patients with COPD are capable of obtaining a physiologic training effect, as manifested by a reduction in blood lactate and ventilation at a given level of exercise.33 There was another question whether training work rate determines the size of the training effect. Most COPD subjects studied had increased blood lactate at low work rates. Many of these patients were able to achieve a physiologic training effect.33,34 Though total work was the same, training at a high work rate was more effective than training at a low work rate. The lower ventilation requirement to perform exercise was in proportion to the lower lactate level. These findings provide a physiologic rationale for exercise training of patients with COPD.33
In our study, physiotherapy was performed using the Manual Diaphragm Release Technique. This choice of technique was based on a clinical study published by Rocha et al35 in which 20 patients afflicted with COPD were treated by use of this method. The authors hypothesized that the release technique can improve the movement of diaphragm, exercise capacity, and maximal respiratory pressure.35 The treatments resulted in significant improvements in diaphragmatic mobility as analyzed by ultrasonography, in exercise capacity as measured by 6MWT and maximal respiratory pressure, and in abdominal and chest wall kinematics as measured by optoelectronic plethysmography.35 The results shown by use of the Manual Diaphragm Release Technique in this study mirror our own. This outcome lends credence to the inclusion of this technique in future rehabilitation protocols.
In one of our earlier studies, we observed that preoperative pulmonary rehabilitation consisting of controlled breathing techniques, stretching, and resistance training as well as personalized training every day for 2–3 weeks improved exercise capacity, chest expansion, the quality of life, and lung mechanics significantly in patients with COPD.36 We used the same protocol in this study as well.
In our study, exercise capacity as measured by 6MWT correlated to BODE-index, Alternative Scale, mMRC, and CAT, reflecting the fact that improved exercise tolerance attracts higher health status. However, several research groups dealing with the same subject were capable of using different parameters to achieve a similar measurement of exercise tolerance and its effects. In an earlier clinical study conducted by Gosselink et al,37 41 consecutive severe COPD patients participated in a pulmonary rehabilitation program. Patients displayed a poor 6MWT and maximal oxygen uptake (VO2max) and reduced respiratory and peripheral muscle force.38 Significant correlations were found with VO2max and transfer factor for carbon monoxide (TlCO), FEV1, quadriceps force (QF), hand grip strength, and body weight.37 Walking distance significantly correlated with QF, hand grip strength, maximal inspiratory pressure (Plmax), and TlCO. In stepwise multiple regression analysis, the variables that significantly contributed to 6MWD were QF and Plmax. The variables that significantly contributed to VO2max were TlCO, QF, and FEV1.37 The methodology of aforementioned study as contrasted by our own acts as a statement that multiple methods still exist to quantify the nature of exercise tolerance and that many more variables remain to be evaluated in future studies before a definite algorithm is to be found.
Finally, the following limitations to our study are to be noted. The population observed encompassed only patients suffering with COPD. In future works, patients affected by additional afflictions such as with interstitial lung disease and pulmonary arterial hypertension are to be included. Also, while psychological elements of chronic respiratory disorders were not taken into account in our current work, previous studies such as the one conducted by Sandoz et al38 have shown these to be important elements of chronic respiratory pathology. We hope to use scales such as the St George’s Respiratory Questionnaire and the Hospital Anxiety and Depression Scale to measure and include such factors in future assessments. It should also be stated that our rehabilitation program spanned a period of 4 weeks, a duration shorter than that of other rehabilitation protocols; however, we wish to note that the total amount of work performed by our patients remained consistent with that of traditionally longer programs.
In summary, our study showed that pulmonary rehabilitation was effective in terms of improvement of exercise tolerance and functional parameters. We would like to underline that the 6MWD was found to be correlated to changes in the BODE-index, Alternative Scale, and mMRC. Correlation was also found between improvements in IVC and gender, grip strength, and chest expansion. On the basis of our data, it should be noted that accurate prediction for the improvement of exercise tolerance requires consideration of a wider variety of different markers than what is currently used.
Acknowledgments
The authors would like to thank George Agathou for English language copy editing.
Footnotes
Disclosure
The authors report no conflicts of interest in this work.
References
- 1.Chaitow L, Breadly D, Gilbert C, Ley R. Multidisciplinary Approaches to Breathing Pattern Disorders. Amsterdam: Elsevier B.V.; 2013. The structure and function of breathing; pp. 1–41. [Google Scholar]
- 2.Ambrosino N, Simonds A. The clinical management in extremely severe COPD. Respir Med. 2007;101(8):1613–1624. doi: 10.1016/j.rmed.2007.02.011. [DOI] [PubMed] [Google Scholar]
- 3.Jones PW, Tabberer M, Chen WH. Creating scenarios of the impact of COPD and their relationship to COPD Assessment Test (CAT™) scores. BMC Pulm Med. 2011;11:42. doi: 10.1186/1471-2466-11-42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Launois C, Barbe C, Bertin E, et al. The modified Medical Research Council scale for the assessment of dyspnea in daily living in obesity: a pilot study. BMC Pulm Med. 2012;12:61. doi: 10.1186/1471-2466-12-61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Funk GC, Kirchheiner K, Burghuber OC, Hartl S. BODE index versus GOLD classification for explaining anxious and depressive symptoms in patients with COPD – a cross-sectional study. Respir Res. 2009;10:1. doi: 10.1186/1465-9921-10-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Rochester CL, Vogiatzis I, Holland AE, et al. ATS/ERS Task Force on Policy in Pulmonary Rehabilitation An official American Thoracic Society/European Respiratory Society Policy Statement: enhancing implementation, use, and delivery of pulmonary rehabilitation. Am J Respir Crit Care Med. 2015;192(11):1373–1386. doi: 10.1164/rccm.201510-1966ST. [DOI] [PubMed] [Google Scholar]
- 7.Varga J, Porszasz J, Boda K, Casaburi R, Somfay A. Supervised high intensity continuous and interval training vs. self-paced training in COPD. Respir Med. 2007;101(11):2297–2304. doi: 10.1016/j.rmed.2007.06.017. [DOI] [PubMed] [Google Scholar]
- 8.de Sá RB, Pessoa MF, Cavalcanti AGL, Campos SL, Amorim C, Dornelas de Andrade A. Immediate effects of respiratory muscle stretching on chest wall kinematics and electromyography in COPD patients. Respir Physiol Neurobiol. 2017;242:1–7. doi: 10.1016/j.resp.2017.03.002. [DOI] [PubMed] [Google Scholar]
- 9.Jones PW, Agusti AG. Outcomes and markers in the assessment of chronic obstructive pulmonary disease. Eur Respir J. 2006;27(4):822–832. doi: 10.1183/09031936.06.00145104. [DOI] [PubMed] [Google Scholar]
- 10.Cote CG, Celli BR. Pulmonary rehabilitation and the BODE index in COPD. Eur Respir J. 2005;26(4):630–636. doi: 10.1183/09031936.05.00045505. [DOI] [PubMed] [Google Scholar]
- 11.Kerti M, Balogh ZS, Halasz A, Kelemen K, Varga J. COPD Assessment for Symptoms and Functional Condition in Pulmonary Rehabilitation. Amsterdam: ERS Annual Congress; 2015. p. 2218. [Google Scholar]
- 12.Quanjer PH, Tammeling GJ, Cotes JE, Pedersen OF, Peslin R, Yernault JC. Lung volumes and forced ventilatory flows. Report working party standardization of lung function tests, European community for steel and coal. Official statement of the European Respiratory Society. Eur Respir J. 1993;16:5–40. [PubMed] [Google Scholar]
- 13.Balke B. A simple field test for the assessment of physical fitness Rep 63-6. Rep Civ Aeromed Res Inst US. 1963:1–8. [PubMed] [Google Scholar]
- 14.Holland AE, Spruit MA, Troosters T, et al. An official European Respiratory Society/American Thoracic Society technical standard: field walking tests in chronic respiratory disease. Eur Respir J. 2014;44(6):1428–1446. doi: 10.1183/09031936.00150314. [DOI] [PubMed] [Google Scholar]
- 15.Debouche S, Pitance L, Robert A, Liistro G, Reychler G. Reliability and reproducibility of chest wall expansion measurement in young healthy adults. J Manipulative Physiol Ther. 2016;39(6):443–449. doi: 10.1016/j.jmpt.2016.05.004. [DOI] [PubMed] [Google Scholar]
- 16.Neumeister W, Rasche K, Maas P, Monnerjahn C, Singh B, Schultze-Werninghaus G. Reproduzierbarkeit der EDV-gestützte Mund Okklusion Druckmessungen [Reproducibility of computer-assisted mouth occlusion pressure measurements] Med Klin (Munich) 1996;91(Suppl 2):73–75. German. [PubMed] [Google Scholar]
- 17.Mirsky IA, Lipman E, Grinker RR. Breath holding time in anxiety states. Fed Proc. 1946;5(1 Pt 2):74. [PubMed] [Google Scholar]
- 18.Shingai K, Kanezaki M. Effect of dyspnea induced by breath-holding on maximal muscular strength of patients with COPD. J Phys Ther Sci. 2014;26(2):255–258. doi: 10.1589/jpts.26.255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.An KN, Chao NY, Askew LJ. Hand strength measurement instruments. Arch Phys Med Rehabil. 1980;61(8):366–368. [PubMed] [Google Scholar]
- 20.Jeong M, Kang HK, Song P, et al. Hand grip strength in patients with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2017;12:2385–2390. doi: 10.2147/COPD.S140915. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Aliverti A, Cala SJ, Duranti R, et al. Human respiratory muscle actions and control during exercise. J Appl Physiol (1985) 1997;83(4):1256–1269. doi: 10.1152/jappl.1997.83.4.1256. [DOI] [PubMed] [Google Scholar]
- 22.Kenyon CM, Cala SJ, Yan S, et al. Rib cage mechanics during quiet breathing and exercise in humans. J Appl Physiol (1985) 1997;83(4):1242–1255. doi: 10.1152/jappl.1997.83.4.1242. [DOI] [PubMed] [Google Scholar]
- 23.Aliverti A, Ghidoli G, Dellacà RL, Pedotti A, Macklem PT. Chest wall kinematic determinants of diaphragm length by optoelectronicplethysmography and ultrasonography. J Appl Physiol (1985) 2003;94(2):621–630. doi: 10.1152/japplphysiol.00329.2002. [DOI] [PubMed] [Google Scholar]
- 24.Romagnoli I, Gigliotti F, Galarducci A, et al. Chest wall kinematics and respiratory muscle action in ankylosing spondylitis patients. Eur Respir J. 2004;24(3):453–460. doi: 10.1183/09031936.04.00123903. [DOI] [PubMed] [Google Scholar]
- 25.Alter A, Aboussouan LS, Mireles-Cabodevila E. Neuromuscular weakness in chronicobstructive pulmonary disease: chest wall, diaphragm, and peripheral muscle contributions. Curr Opin Pulm Med. 2017;23(2):129–138. doi: 10.1097/MCP.0000000000000360. [DOI] [PubMed] [Google Scholar]
- 26.O’Donnel DE, Revill SM, Webb KA. Dynamic hyperinflation and exercise intolerance in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2001;164(5):770–777. doi: 10.1164/ajrccm.164.5.2012122. [DOI] [PubMed] [Google Scholar]
- 27.O’Donnell DE, Webb KA. Breathlessness in patients with severe chronic airflow limitation; physiological correlates. Chest. 1992;102(3):824–831. doi: 10.1378/chest.102.3.824. [DOI] [PubMed] [Google Scholar]
- 28.Petrovic M, Reiter M, Zipko H, Pohl W, Wanke T. Effects of inspiratory muscle training on dynamic hyperinflation in patients with COPD. Int J Chron Obstruct Pulmon Dis. 2012;7:797–805. doi: 10.2147/COPD.S23784. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Beckerman M, Magadle R, Weiner M, Weiner P. The effects of 1 year of specific inspiratory muscle training in patients with COPD. Chest. 2005;128(5):3177–3182. doi: 10.1378/chest.128.5.3177. [DOI] [PubMed] [Google Scholar]
- 30.Albuquerque AL, Quaranta M, Chakrabarti B, Aliverti A, Calverley PM. Exercise performance and differences in physiological response to pulmonary rehabilitation in severe chronic obstructive pulmonary disease with hyperinflation. J Bras Pneumol. 2016;42(2):121–129. doi: 10.1590/S1806-37562015000000078. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.O’Donnell DE, Laveneziana P. The clinical importance of dynamic lung hyperinflation in COPD. COPD. 2006;3(4):219–232. doi: 10.1080/15412550600977478. [DOI] [PubMed] [Google Scholar]
- 32.Aslan GK, Akinci B, Yeldan I, Okumus G. Respiratory muscle strength in patients with pulmonary hypertension: the relationship with exercise capacity, physical activity level, and quality of life. Clin Respir J. 2016 Nov 17; doi: 10.1111/crj.12582. Epub. [DOI] [PubMed] [Google Scholar]
- 33.Varga J. Mechanisms to dyspnoea and dynamic hyperinflation related exercise intolerance in COPD. Act Physiol Hung. 2015;102(2):163–175. doi: 10.1556/036.102.2015.2.7. [DOI] [PubMed] [Google Scholar]
- 34.Casaburi R, Patessio A, Ioli F, Zanaboni S, Donner CF, Wasserman K. Reductions in exercise lactic acidosis and ventilation as a result of exercise training in patients with obstructive lung disease. Am Rev Respir Dis. 1991;143(1):9–18. doi: 10.1164/ajrccm/143.1.9. [DOI] [PubMed] [Google Scholar]
- 35.Rocha T, Souza H, Brandão DC, et al. The manual diaphragm release technique improves diaphragmatic mobility, inspiratory capacity and exercise capacity in people with chronic obstructive pulmonary disease: a randomised trial. J Physiother. 2015;61(4):182–189. doi: 10.1016/j.jphys.2015.08.009. [DOI] [PubMed] [Google Scholar]
- 36.Vagvolgyi A, Rozgonyi Z, Kerti M, Vadasz P, Varga J. Effectiveness of perioperative pulmonary rehabilitation in thoracic surgery. J Thorac Dis. 2017;9(6):1584–1591. doi: 10.21037/jtd.2017.05.49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Gosselink R, Troosters T, Decramer M. Peripheral muscle weakness contributes to exercise limitation in COPD. Am J Respir Crit Care Med. 1996;153(3):976–980. doi: 10.1164/ajrccm.153.3.8630582. [DOI] [PubMed] [Google Scholar]
- 38.Sandoz JS, Roberts MM, Cho JG, Wheatley JR. Magnitude of exercise capacity and quality of life improvement following repeat pulmonary rehabilitation in patients with COPD. Int J Chron Obstruct Pulmon Dis. 2017;12:1085–1091. doi: 10.2147/COPD.S131778. [DOI] [PMC free article] [PubMed] [Google Scholar]