

Inflammatory bowel disease (IBD) may be associated with a number of extra-intestinal complications, including, rarely, myocarditis. Diagnosis of this can be difficult however, but we highlight the utility of cardiovascular magnetic resonance (CMR) in this patient group.
Two hospitalised patients with IBD [one with an exacerbation of ulcerative colitis (UC), and one on a tapering schedule of steroid treatment for Crohn’s disease (CD)] had crushing chest pain, a troponin rise and normal coronary arteries on angiography. Both patients underwent CMR at 1.5 T, including dark-blood T2-weighted, late gadolinium enhancement (LGE) imaging, and native T1-mapping (Figure 1). The left ventricular ejection fraction was 55% in the patient with UC and 30% in the patient with CD. In both cases, global myocardial oedema was not apparent on conventional dark-blood T2-weighted imaging, with a myocardial-to-skeletal muscle T2 signal intensity ratio of <1.9.
Figure 1.
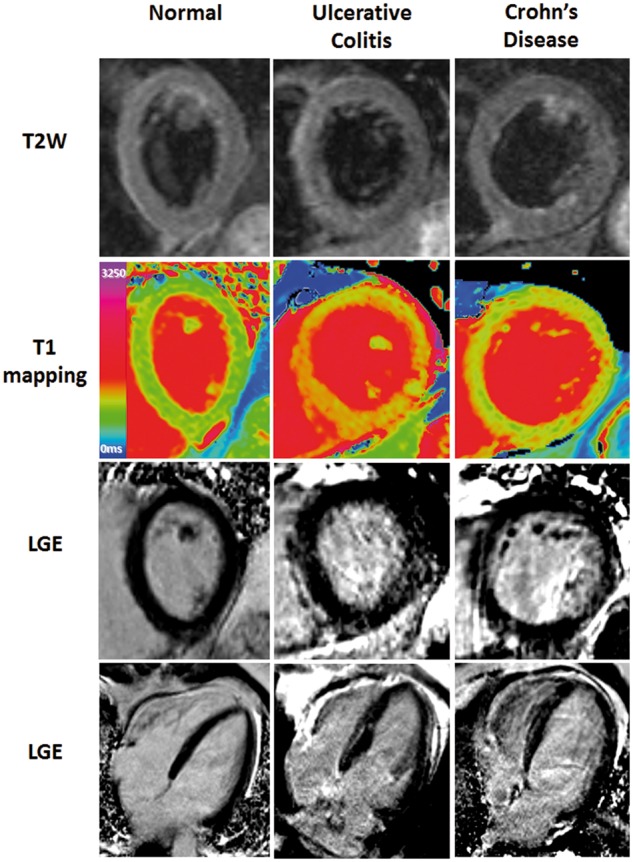
Multi-parametric CMR (1.5 T) in a normal control, a patient with UC and a patient with CD.
LGE showed small areas of mid-wall enhancement in the septum and patchy enhancement in the basal inferolateral wall. However, native T1-mapping revealed a larger extent of myocardial involvement, with marked elevated global myocardial T1 values in both cases (UC: 1166 ± 77 ms; CD: 1047 ± 99 ms; normal ShMOLLI myocardial T1 = 962 ± 25 ms). This was consistent with (although not specific for) acute myocardial oedema (T1 > 990 ms).
Both cases demonstrate the importance of recognising that myocarditis can accompany active IBD. CMR can be used to confirm this diagnosis within the clinical context, using novel mapping techniques to reveal global myocardial oedema, which may be missed by conventional T2-weighted imaging if the degree of inflammation is subtle, or if skeletal muscle is also inflamed as part of a systemic response. A correct diagnosis of myocarditis may then be managed appropriately, avoiding treatment for acute coronary syndrome with antiplatelet agents and anticoagulation, which may exacerbate intestinal bleeding in active IBD.
Conflict of interest: S.K.P. has patent authorship rights for U.S. patent 9285446 B2. Systems and methods for shortened look locker inversion recovery (Sh-MOLLI) cardiac gated mapping of T1. Granted March 15, 2016. All rights transferred to Siemens Medical. Other authors have no conflicts of interests to declare.
Funding
S.K.P., S.G.M., and V.M.F. are funded in part by the National Institute for Health Research (NIHR) Oxford Biomedical Research Centre at The Oxford University Hospitals NHS Foundation Trust and the University of Oxford.