

Abstract
Researchers examined whether a parent-implemented language intervention improved problem behaviors one year after intervention. Ninety seven children with language delays (mean age at 12 month follow-up = 48.22 months) were randomized to receive Enhanced Milieu Teaching (EMT) language intervention or business as usual treatment. Twelve months after the intervention ended, children in the EMT intervention condition displayed lower rates of parent-reported externalizing, internalizing, and total problem behaviors. A mediation analysis revealed that the relation between EMT and problem behaviors was partially mediated by child rate of communication for both internalizing and total problem behaviors. A developmental framework is proposed to explain the impact of EMT on problem behaviors, and future lines of research are discussed.
Keywords: problem behaviors, language, early intervention
Toddlers and preschool-aged children with language delays frequently exhibit elevated rates of problem behaviors when compared to same-age peers with typically developing language (e.g., Benasich, Curtiss, & Tallal, 1993; Qi & Kaiser, 2004) In a large birth cohort, Horwitz et al. (2003) found that 21.3 percent of parents of language-delayed children over 30 months of age were worried about their child’s behavior, and that 23.2 percent of these children fell in the 90th percentile or above on the externalizing scale of the Infant Toddler Social Emotional Assessment. More recent meta-analyses of the relation between language and problem behaviors have found that 81% of school-age children with an emotional-behavioral disorder had below-average language skills (Hollo, Wehby, & Oliver, 2014) and that there is a stable, negative correlation between language skills and problem behaviors, both concurrently and predictively (Chow, 2016). Although there is evidence of a high degree of comorbidity between language delays and problem behaviors, few studies have examined the impact of language interventions on children’s problem behavior. Presumably, early language interventions could simultaneously improve language skills while reducing children’s behavioral difficulties. The current study investigated the effects of a parent-implemented intervention, Enhanced Milieu Teaching (EMT), on problem behaviors in toddlers and preschoolers with receptive and expressive language delays.
Language Delays in Early Childhood
The trajectory of early language delays varies from child to child. While there is evidence that the effects of these delays are persistent, there is also considerable variability across children and over time (Preston et al., 2010). Some young children with early language delays, particularly children with expressive only delays, go on to “recover” and no longer meet diagnostic criteria for a language delay (Zambrana, Pons, Eadie, & Ystrom, 2014). However, even these children who no longer meet clinical criteria for a language delay consistently score lower on standardized language tests than their typically developing peers (see Rescorla (2011) for a full review). Early language delays have been associated with neurological differences in language processing (Preston et al., 2010) and difficulties in reading comprehension (Rescorla, 2002, 2005), as well as gaps in academic performance that can persist into young adulthood (Rescorla, 2005).
While many clinicians adopt a “wait and see approach” (Paul, 1996) to conserve resources for children with established persistent language impairment, this approach may result in lasting academic and social deficits for children with early language delays. Longitudinal data suggest that leaving early language delays untreated can have lasting effects on children’s academic skills (Catts, Fey, Tomblin, & Zhang, 2002), as well as on their social emotional development (Benasich et al., 1993).
Problem Behaviors in Early Childhood
Researchers frequently divide problem behaviors in childhood into two categories: internalizing problems and externalizing problems (Achenbach, 1978). Internalizing behaviors include symptoms of anxiety and depression, as well as disordered emotion or mood (Kovacs & Devlin, 1998). In childhood, these disorders include symptoms such as acting fearful, sad, withdrawn, or panicked (Achenbach & Rescorla, 2001). Estimates of the prevalence of anxiety disorders during the preschool period vary widely, but have been reported to range from 1.8% to 15.4% (Egger & Angold, 2006). Once established, internalizing problems may be persistent across development (Briggs-Gowan, Carter, Skuban, & Horwitz, 2001; Mesman & Koot, 2001). Furthermore, internalizing disorders can have debilitating effects on children’s functioning across developmental domains and may affect child participation in family life and school or daycare (Luby, Belden, Pautsch, Si, & Spitznagel, 2009).
Externalizing behaviors, on the other hand, include hyperactive, disruptive, and aggressive behaviors (Hinshaw, 1987). Estimates of the prevalence of externalizing disorders in the preschool period range between 9.0% and 14.9% (Egger & Angold, 2006). As with internalizing disorders, early externalizing behaviors are frequently persistent. Briggs-Gowan et al. (2001) found that for externalizing problems, 49.9% of 1–3 year olds with scores above the 90th percentile persisted in meeting this criteria one year later. Early externalizing problems have been associated with poor literacy development (Allan, Joye, & Lonigan, 2013) and academic performance (Masten et al., 2005) over time. Thus, the presence of externalizing behaviors may prevent children from fully benefitting from early learning opportunities and have a cascading effect on both social and academic behavior. These behaviors present significant challenges to parents and families (Neece, Green, & Baker, 2012), and the need for interventions that can be applied early in life is evident based on these findings. Comorbidity is common between internalizing and externalizing behaviors, with specific rates varying widely between studies and between specific disorders (Angold & Egger, 2007).
There are a number of proposed causes for both internalizing and externalizing behaviors, including genetics, neurobiological differences, information processing differences, and attachment styles (see Hayden and Mash (2014) for a comprehensive review). One proposed developmental mechanism that is related to both internalizing and externalizing problems is emotion regulation. This decades-old construct has numerous empirical studies, chapters, and books dedicated to it (notably Gross (2014)). While many definitions have been created for emotion regulation,, Thompson (1994) defined emotion regulation as the processes, both internal and external, used to monitor, evaluate, and modulate emotional reactions in order to facilitate accomplishment of one’s goals. Emotion regulation skills are related to both internalizing and externalizing behaviors (Cole, Zahn-Waxler, Fox, Usher, & Welsh, 1996; Halligan et al., 2013). In order to categorize the many behaviors that children and adults may engage in to regulate their emotions, Gross (1998) developed the Process Model of Emotion Regulation (PMER) that posits that an individual can modify his or her emotional state at several time points in the course of an emotional experience. Emotion regulation strategies can be applied before an emotion is experienced, which Gross defines as antecedent focused. Alternatively, strategies can be applied after the emotion is experienced, which Gross refers to as response-focused. Antecedent-focused emotion regulation strategies include selecting and modifying the environmental situation (i.e., choosing an activity or modifying the activity by requesting caregiver support), changing ones attentional focus (i.e., distracting oneself during a stressful task by focusing on something else), and changing ones cognitive appraisal of a given situation. Response-focused strategies seek to modify an emotional response once it has already occurred. The PMER model provides an excellent framework for classifying the many behaviors that children may engage in in order to regulate their emotions (López-Pérez, Gummerum, Wilson, & Dellaria, 2016).
Children begin to develop emotion regulation abilities early in life in the context of parent-child interactions (Kopp, 1989). Initially, children rely on their parents or caregivers to use emotion regulation strategies to regulate their emotions. Later, children begin to use emotion regulation strategies to independently modulate their own emotions(Spinrad, Stifter, Donelan‐McCall, & Turner, 2004). While the ability to use emotion regulation strategies to regulate one’s own emotional state, or self-regulation, is an important developmental achievement (Garber & Dodge, 1991), toddlers and young children frequently continue to engage in mutual-regulation with their caregivers, by actively enlisting the caregiver’s support to regulate their emotional state (Tronick, 1989). For instance, a child may request emotional support from an adult when completing a difficult puzzle.
Gratz and Roemer (2004) proposed an expanded definition of emotion regulation that incorporates emotional awareness and understanding, citing Lane and Schwartz’s (1987) developmental model of emotion awareness and its impact on internalizing and externalizing behaviors. Emotion awareness is the ability to identify that one is experiencing an emotion and to classify that emotion. While there has been very little work on the development of emotion awareness as it relates to behavior difficulties in toddlers and preschoolers, emotion awareness and understanding have been linked to problem behaviors in older children (Trentacosta & Fine, 2010).
In addition to the roles played by children’s emotion awareness and their self- and mutual-regulation of emotions, the quality of parent-child interactions in toddlers and preschoolers has been shown to affect children’s problem behaviors (Harrist & Waugh, 2002). The quality of parent child interaction can be characterized by the degree to which a parent and child share affect, respond to each other’s emotions and actions, and share the same focus during play (Deater-Deckard & O’Connor, 2000). This parent-child synchrony has been linked to children’s externalizing and internalizing behaviors (Harrist & Waugh, 2002), child compliance with adult directions (Rocissano, Slade, & Lynch, 1987), and children’s use of emotion regulation strategies (Raver, 1996). In sum, children’s internalizing and externalizing behaviors are influenced by a complex set of factors, including the quality of the parent-child relationship, the development of emotion awareness, and the instruction and use of self- and mutual-regulation strategies to modulate emotions.
Relation Between Problem Behaviors and Language Ability
Children with language delays may be at elevated risk for problem behaviors. Caulfield, Fischel, DeBaryshe, and Whitehurst (1989) found that toddlers with expressive language delays were rated as more shy and fearful in new situations as compared to their typically developing peers. Likewise, Irwin, Carter, and Briggs-Gowan (2002) found that parents of late-talking toddlers rated their children as more shy and withdrawn than parents of typically developing toddlers did, and that observers rated these late-talking toddlers as more withdrawn, depressed, and sober during parent-child interactions. Paul and James (1990) found that parents of late talkers rated their children as having higher levels of conduct, attention, and mood difficulties than parents of typically developing toddlers. Prior, Bavin, Cini, Eadie, and Reilly (2011) reported that preschoolers with language impairments were rated higher on a scale of conduct problems by their parents than their typically developing peers. A similar relation between language delays and internalizing behaviors has been indicated for older children as well, using both teacher ratings (Hart, Fujiki, Brinton, & Hart, 2004) and observation of children’s behaviors on the playground (Fujiki, Brinton, Isaacson, & Summers, 2001), suggesting a persistent link between language skills and problem behaviors (Chow, 2016). While studies have shown a relation between language skills and both internalizing and externalizing behaviors, many studies have found that internalizing problems are more common in children with language delays than are externalizing problems (e.g., Irwin et al., 2002), suggesting a differentiated impact of language skills on internalizing behaviors.
One proposed mechanism for the association between language skills and problem behaviors is the essential role that language plays in the social interactions that foster parent-child synchrony and emotion regulation development in children (Cole, Armstrong, & Pemberton, 2010). This relation between language and emotion regulation can be seen in studies of emotion awareness, mutual-regulation, and self-regulation. Children learn about emotion awareness and regulation through interactions with their caregivers, and much of this instruction occurs through linguistic social interactions (Kopp, 1989; Stansbury & Zimmermann, 1999). For instance, increased parental labeling of emotions predicts child labeling and understanding of emotions (Cervantes & Callanan, 1998). In regards to emotion regulation strategies, Stansbury and Zimmermann (1999) found that parents of children with language delays used a smaller range of emotion regulation strategies with their children, suggesting that language delays can disrupt the socialization of emotion regulation abilities. Likewise, Prizant and Meyer (1993) suggest that children with language delays have fewer social interactions with their caregivers, and so have fewer opportunities to engage in mutual-regulation of emotions, which may limit the emotion regulation strategies that children can then learn to apply themselves for the purposes of self-regulation.
In Gross’s (1998) process model of emotion regulation, language abilities may impact a child’s ability to use any of the five regulatory mechanisms that Gross identifies: selecting the situation, modifying the situation, changing attentional focus, changing cognition, or modifying an emotional reaction. Indeed, there is evidence that children with language delays are less able to distract themselves during difficult tasks (changing attentional focus) (Stansbury & Zimmermann, 1999) and less likely to seek maternal support (modifying the situation) (Roben, Cole, & Armstrong, 2013). Additionally, Sala, Pons, and Molina (2014) found that children with better verbal abilities were more likely to use cognitive reappraisal as an emotion regulation strategy. It is also possible that young children use language to select a situation by verbally requesting or stating their preference for a certain activity or toy. While there is very little research exploring how language impacts each of the five emotional regulation processes outlined by Gross, we posit that children’s language abilities may play a crucial role in implementing these strategies both independently and in the context of the parent-child relationship.
Interventions for Language Delays and for Problem Behaviors in Early Childhood
Over the past several decades, numerous parent-implemented language interventions have been proposed and studied. In a meta-analysis of 18 studies, Roberts and Kaiser (2011) found that parent-implemented language interventions significantly improve both expressive and receptive language skills in children with language impairment. These interventions sought to modify parental behavior in a number of ways in order to enhance children’s language-learning. These modifications included altering the quantity of adult linguistic input, providing specific language models, increasing parental responsiveness to child communication, and following the child’s lead during parent-child interactions. The outcomes of these studies focused on changes in parental behaviors and child language outcomes. Few studies included measures of behavioral and social outcomes.
While there is a lack of evidence about the effect of parent-led language interventions on children’s problem behaviors, conceptually, most parent-implemented language interventions share common features with interventions targeting social development and behavior in young children. For instance, studies have investigated the efficacy of Parent Child Interaction Therapy (PCIT) on child problem behaviors (Eyberg & Robinson, 1982). PCIT was originally designed for the treatment of disruptive behavior in preschoolers and features a Child Directed Interaction (CDI) component, as well as a Parent Directed Interaction (PDI) component. The CDI component focuses on improving parent-child synchrony by teaching parents to create positive, child-focused, and contingent interactions with their children. Recent modifications to PCIT have incorporated additional components to address the development of emotion understanding and emotion regulation skills in children to reduce depressive symptoms (Lenze, Pautsch, & Luby, 2011).
Both parent-implemented language interventions and parent-implemented problem behavior interventions target building positive, contingent interactions between the parent and child in order to increase parent-child synchrony. Because of the similarities in intervention approaches, it is possible that language interventions may impact children’s problem behaviors in much the same way that parent-implemented problem behavior interventions do. It is also possible that enhancing children’s language abilities through parent-child interactions may provide children with the necessary language abilities to implement both mutual and self-regulation skills and in turn to reduce problem behaviors.
Proposed model of the effects of Enhanced Milieu Teaching (EMT) on problem behaviors
The current study investigated the effect of a parent-implemented language intervention, Enhanced Milieu Teaching (EMT), on the problem behaviors of toddlers and preschool-aged children with language delays. Enhanced Milieu Teaching involves teaching parents to use a set of language facilitation strategies, including noticing and responding to child communication, modeling language and expanding child utterances, and using specific language prompts in response to child requests. Because this intervention teaches parents to respond contingently to their children’s interests in any given situation, specific vocabulary items were not targeted. Instead, parents provided children with linguistic models to express their children’s interests, actions, or emotional states in the moment. While the main goals in EMT are promoting the use of language facilitation behaviors by parents, we posit that this intervention also impacts children’s problem behaviors both directly and indirectly. The proposed direct effects of EMT on children’s problem behaviors include: 1) altering the parent-child relationship quality by increasing dyadic synchrony, 2) increasing parent responsiveness to child emotional states, and 3) teaching parents to model and reinforce the use of language-mediated emotion regulation strategies. The proposed indirect effect of EMT on problem behaviors is through the development of richer vocabulary and language skills for children to use while employing self- and mutual emotion regulation strategies.
One key component of increasing parental responsiveness to child communication is teaching parents to “follow their child’s lead” in play. Rather than directing play and conversation themselves, parents are instructed to watch and imitate their child’s play actions, to join and expand their children’s play schemes, and to talk about their children’s focus of interest. These components of EMT strongly resemble the Child Directed Interaction component of PCIT, in which parents are coached to attentively listen to their child and to respond at their child’s level with enthusiasm and warmth, among other strategies (Eyberg & Robinson, 1982). Brinkmeyer and Eyberg (2003) suggest that enhancing parent-child synchrony by encouraging non-directive play and increased parental responsiveness may create a more secure attachment relationship, leading to increased emotion regulation skills. In this way, EMT may improve the quality of the parent-child relationship and thereby reduce child problem behaviors.
During the EMT intervention, parents are also taught to model language that reflects their child’s interests and what their child intends to communicate. For instance, if a child points to a car, the parent is taught to respond to the child’s communicative intent (sharing attention to the car or requesting the car) by saying “car.” Modeling language based on the child’s communicative intent can also include labeling emotional states, such as saying “mad” or “I’m scared.” Providing these labels for children’s emotional experiences increases children’s emotion awareness, as outlined above, and is consistent with other intervention strategies for internalizing disorders in young children, such as the Emotional Development Module from Lenze, Patusch, and Luby’s modification of PCIT (2011). In EMT, parents are also instructed to provide labels for other behaviors that may serve to regulate emotions, such as help-seeking. By encouraging parents to model these linguistically-based emotion regulation strategies, EMT increases the number of regulation strategies that children are exposed to. After being taught to respond to child nonverbal requests by providing models of effective language, including regulation strategies, parents are then taught several language prompting strategies in order to encourage children to use these models to make requests. Because these strategies require the child to respond verbally before the child’s request is met, these strategies reinforce the use of language as a regulating strategy. This reinforcement may encourage children to increase their independent use of communication as an emotion regulation strategy in order to have more of their emotional and substantive needs met. Thus, EMT may improve both the parent’s and the child’s ability to engage in mutually regulating behaviors within the context of the parent-child relationship.
Finally, EMT may indirectly affect problem behaviors by improving child language skills (Roberts & Kaiser, 2015). These enhanced language skills may allow children to more fully describe their emotions and desires (Harris, 1996) and to communicate with their parents more effectively, behaviors that may regulate children’s behavior by modifying the situational context in Gross’s PMER framework. As language skills are related to emotion regulation abilities (Roben et al., 2013), improving children’s language abilities may allow them to employ a wider number of regulating strategies. Thus, EMT may have a direct impact on children’s behavior through changes in the parent-child relationship, the socialization of emotion regulating strategies, and parental responsiveness to child emotional states, and an indirect impact through improvement in children’s linguistic abilities that allow parents and children to implement these strategies. Because the development of communication skills supports the development and use of self-regulation and mutual regulation skills, it may be that language skills mediate the relation between EMT and problem behaviors.
The Current Study
The current study was a secondary analysis of data from a randomized clinical trial examining the effects of parent-implemented Enhanced Milieu Teaching on the language outcomes of toddlers with language delays (Roberts & Kaiser, 2015). The primary analysis of the randomized controlled trial showed that EMT significantly increased children’s receptive and expressive language abilities immediately after the intervention. The current study was designed to examine the effects of EMT on children’s problem behaviors and to determine the extent to which this relation was driven by changes in child language.
Mediation analyses require that the independent variable, EMT, be a significant predictor of the mediator variable, language. Immediately after intervention, EMT significantly improved receptive language scores on the Preschool Language Scales (PLS-3), the Peabody Picture Vocabulary Test (PPVT-IV), and the number of different words (NDW) children used in a parent-child play sample (Roberts & Kaiser, 2015). At the 12 month follow-up, however, there was no significant effect of EMT on these language measures. EMT did significantly increase children’s rate of communication at 12 month follow-up. These findings suggest that EMT may function as what Gottlieb termed a facilitative intervention for children’s language abilities (Gottlieb, 1976), by accelerating the trajectory of language development for a period of time. As argued by Olswang and Bain (1991) and Robertson and Weismer (1999), facilitative interventions may improve developmental domains that are not directly targeted in the intervention but that rely on the skills developed during the intervention. The fact that EMT significantly increased child rate of communication 12 months after intervention suggests that EMT’s long-term impact on child language is an increase in child communicativeness. This increase may allow children to more frequently employ verbal self- and mutual regulation strategies to modulate their emotions and behaviors, which may in turn decrease problem behaviors. Accordingly, we used children’s rate of communication as the language variable in all analyses, and tested whether rate of communication mediated the relationship between EMT and children’s problem behaviors.
The following research questions guided this study:
What is the impact of parent-implemented EMT on children’s problem behaviors, and which specific type of problem behaviors (internalizing, externalizing, or total problem behaviors) does EMT most impact?
Do child language skills (rate of communication) mediate the relation between EMT and child problem behaviors?
Based on literature showing a consistent relation between language and internalizing behavior, and the important role that language plays in the acquisition and use of emotion regulation strategies, we believed that EMT would have the greatest impact on internalizing behaviors, and that this association will be mediated by child rate of communication.
METHODS
Trial Design
A randomized controlled trial (NCT01975922) was conducted in Nashville, Tennessee to investigate the efficacy of parent-implemented Enhanced Milieu Teaching (EMT; (Kaiser, 1993)) to improve receptive and expressive language abilities in toddlers with language delays. Ninety-seven children (mean age 30.5 months at baseline; 45 children in the intervention condition, 52 children in the control condition; 81% male) meeting criteria for language delays and their parents were randomized to the intervention condition or the business as usual control condition. Participants were recruited continuously between October 2009 and October 2013. The high percentage of male participants is reflective of a greater prevalence of language delays in males than in females and is in keeping with previous work with toddlers with delayed language development in this age range (Rescorla & Alley, 2001). After baseline data were collected for all participants, those in the intervention condition received a three-month intervention that was carried out over 28 sessions in the clinic and the home. Parents were taught six language facilitation strategies, including responding contingently to children’s communicative acts, matching their communicative turns to the child’s (as opposed to the parent having many more conversational turns than the child), expanding child utterances by adding one to two words, and two language elicitation strategies: time delays and prompting (see Roberts and Kaiser (2015) for details about the intervention). Control participants did not receive treatment, but were referred to the Tennessee Early Intervention System. This study is a registered clinical trial and post-intervention main results have been published in Roberts and Kaiser (2015). All participants were tested before the intervention (baseline), 3 months (immediately after intervention), 9 months (6 month follow-up), and 15 months (12 month follow-up) after entry into the study. In order to determine the long-term impact of EMT on problem behaviors, the primary outcome measures for this study were 12 month follow-up data. Children in both treatment and control groups could participate in early interventions provided in the community; however, fewer than 25% of children in either group received services. On average, children in the treatment group received 14 hours more intervention than children in the control group over the course of the study.
Participants
Participants were recruited from local pediatricians’ offices, through advertisements in the Nashville Parent, and by referrals from the Tennessee Early Intervention System. Children were eligible for the study if their receptive and/or expressive scores on the Bayley Scales of Infant Development, Third Edition (Bayley, 2005) were at least 1.33 SD below the normative mean (a scaled score of ≤ 6), they were between 24 and 42 months of age, and their parent consented to participation in the study. Exclusion criteria included intellectual disabilities (BSDI-3 cognitive score of less than 80), autism diagnosis, significant motor impairment, and hearing loss of > 40 dB.
Measures
Problem Behaviors
Children’s problem behaviors were measured using the total problems, externalizing, and internalizing composite scores from the Child Behavioral Checklist 1.5 – 5 (Achenbach & Rescorla, 2001). The CBCL is a widely-used parent report measure of child problem behaviors. The authors report test-retest reliability of .90 for the total problems composite score, .87 for the externalizing composite score, and .90 for the internalizing composite score. Caregivers completed the CBCL at each assessment time point. In all analyses, CBCL raw scores were used in place of standardized scores. We chose this strategy for several reasons. To control for pre-intervention differences in child problem behaviors, baseline CBCL scores were included in all models as a covariate, in effect creating a change score between baseline and 12 month follow-up. Utilizing raw scores while controlling for baseline scores represents true changes in child problem behaviors, whereas using scaled scores would represent changes in rank-order of child problem behaviors as compared to a normative sample. Additionally, the language variables derived from parent-child interactions are not age-normed, and so age was included as a covariate in all models. If CBCL scaled scores were used in place of raw scores, the child age covariate would “re-norm” the scaled scores, potentially altering the variance in CBCL scores. To account for inherent differences in rates of problem behaviors between boys and girls that are controlled for in CBCL standard scores, gender was also included as a covariate in all models. Items on the CBCL were analyzed to assess whether any items assessed language abilities. Only two items, “doesn’t answer when people talk to him/her” in the Internalizing Composite scale, and “speech problems” in the Total Problem Behaviors scale directly assessed language abilities. As only two of the 99 items in the CBCL 1.5–5 included definitions that might measure language instead of problem behaviors in children with language delays, these two items were retained in analyses.
Rate of Communication
At baseline and at 12 month follow-up, children’s rate of communication was calculated as the number of utterances spoken by the child during two play-based observational samples in which children interacted with their caregivers in a clinic setting, totaling 20 minutes of observation at each time point. The interactions were video recorded by a research assistant; no other research personnel were present. In the first sample, children played with their caregivers for 10 minutes using a set of standardized toys, such as toy dinosaurs, toy pots and pans, blocks, and a pop-up toy. In the second sample, children engaged in a pretend picnic with their caregivers for 10 minutes using a second set of standardized materials, including toys such as a play picnic basket, a play grill with food, a set of plastic bugs, and a beach ball. In both contexts, caregivers were instructed to play as they normally would with their children. All interactions were video recorded and transcribed by trained coders blind to the experimental conditions
Analysis Plan
Because our research questions involved testing both direct and mediated effects, a statistical approach that allowed for flexible estimation of both of these types of parameters was needed. We chose to use structural equation modeling (SEM) to construct a series of models to answer each research question. SEM uses full-information maximum likelihood (FML) estimation to determine parameter estimates. SEM allows the researcher to flexibly specify relations between endogenous and exogenous variables, allowing for the re-creation of typical multiple regression models, as well as more complex relations between variables.
Modeling of Main Effects
For each type of problem behavior (internalizing, externalizing, and total problem behaviors), a series of five SEM models was constructed (described in detail below). The first model in each series allowed us to address our first research question by modeling the direct effect of EMT on each type of problem behavior. These models included effect size estimates, allowing us to compare the magnitude of the impact of EMT on each problem behavior to address our second research question.
Modeling of Mediation Effect
In order to construct a mediation model, we employed SEM to estimate the indirect path or the product of the path from EMT to child rate of communication and the path from rate of communication to child problem behavior by creating an algebraic calculation of the a and b paths shown in Figure 1. As previously discussed, rate of communication was chosen as the language variable in these analyses, as this is the only language measure that EMT significantly improved at the 12 month follow-up. This SEM-based method constructs a confidence interval for this parameter directly, as opposed to simply inferring it’s significance as in Baron and Kenny’s causal steps approach (1986). This estimation method also does not assume a normal sampling distribution of the indirect effect as in the Sobel method (Sobel, 1982), which is not always the case, especially for small samples (Bollen & Stine, 1990). Models 4 and 5 in each series test the mediation hypothesis and contain all three mediation variables and the indirect path.
Figure 1.
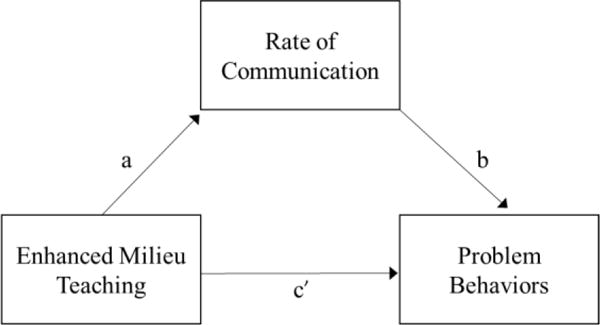
A simple mediation model.
Model Summaries
For each type of problem behavior, five structural equation models were created to create Baron and Kenny’s (1986) causal steps to mediation. In all models, baseline problem behavior scores, baseline rate of communication, the child’s age at follow-up, and the child’s gender were entered as covariates, as shown in Figure 2. The models for each problem behavior variable were constructed to demonstrate:
The effect of EMT on child problem behaviors, without current rate of communication (c path).
The effect of EMT on child rate of communication, without current problem behaviors (a path)
The effect of child rate of communication on child problem behaviors, without including intervention status (b path)
The full mediation model, with the indirect c′ path freely estimated (EMT → child rate of communication → problem behaviors, test of partial mediation).
The full mediation model, with the indirect c′ path constrained to zero. (EMT → child rate of communication → problem behaviors, test of full mediation).
Figure 2.
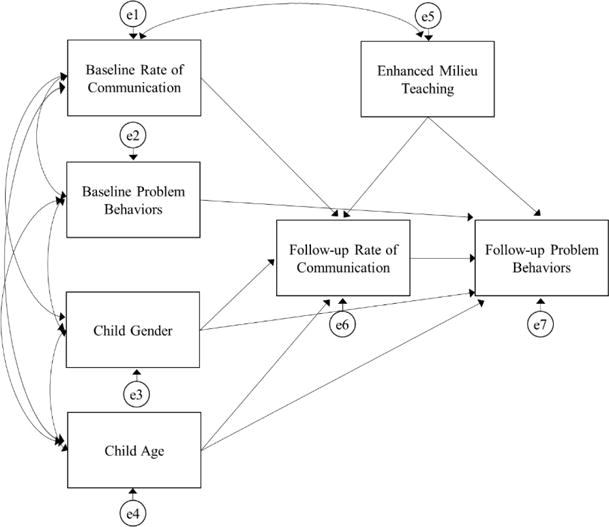
Model 4 – Full mediation model with c′ path freely estimated.
RESULTS
Participant characteristics are given in Table 1. We first looked for differences in the covariates between the EMT group and the control group. Child age, child gender, and baseline internalizing scores did not differ significantly between groups. The two groups did differ significantly on baseline rate of communication, (mean of control group = 61.54 utterances, mean of intervention group = 86.09 utterances, p = .048). Because of this significant difference, all models that include EMT include a non-causal covariance path between baseline rate of communication and EMT status.
Table 1.
Summary of Participant Characteristics
| Intervention | Control | |||
|---|---|---|---|---|
|
| ||||
| Variable | N | Mean (SD) or % | N | Mean (SD) or % |
|
| ||||
| N | 45 | 52 | ||
| Household Income (U.S. dollars) | 44 | $71135.27 (35,105.49) | 48 | $57,171.65 (51,525.85) |
| Maternal Education | 45 | 52 | ||
| Without HS Diploma | 0 | 4 | ||
| HS Graduate without college education | 9 | 10 | ||
| Some college education or 2 year degree | 29 | 31 | ||
| Degree from 4-year college or more | 62 | 50 | ||
| Not reported | 0 | 6 | ||
| Race | 45 | 52 | ||
| African American | 18 | 19 | ||
| White | 78 | 79 | ||
| Other | 4 | 2 | ||
| Male | 45 | 82 | 52 | 81 |
| Mixed Receptive Expressive Language Delay | 45 | 87 | 52 | 80 |
| Expressive – Only Language Delay | 45 | 13 | 52 | 20 |
| Age at 12 month follow-up (months) | 42 | 47.93 (5.2) | 38 | 48.54 (5.76) |
| Baseline Scores | ||||
| Total Problem Behaviors Raw Score | 45 | 29.29 (20.11) | 48 | 30.21 (18.09) |
| Externalizing Problems Raw Score | 45 | 11.04 (8.22) | 48 | 11.67 (8.23) |
| Internalizing Problem Behaviors Raw Score | 45 | 6.64 (5.94) | 48 | 6.79 (4.77) |
| Total Problem Behaviors Standard Score | 45 | 47.87 (9.90) | 48 | 48.50 (9.77) |
| Externalizing Problems Standard Score | 45 | 47.47 (10.53) | 48 | 48.27 (10.28) |
| Internalizing Problems Standard Score | 45 | 46.71 (9.25) | 48 | 47.27 (9.12) |
| Internalizing Behavior in Clinical Range | 45 | 7 | 48 | 8 |
| Externalizing Behavior in Clinical Range | 45 | 9 | 48 | 13 |
| Communication Rate | 45 | 86.09 (62.54) | 50 | 61.54 (55.91) |
| 12 Month Follow-up Scores | ||||
| Total Problem Behaviors Score | 38 | 19.66 (15.10) | 37 | 27.65 (15.53) |
| Externalizing Problems Score | 38 | 6.95 (6.10) | 37 | 9.92 (6.83) |
| Internalizing Problem Behaviors Score | 38 | 4.63 (4.82) | 37 | 6.95 (4.82) |
| Total Problem Behaviors Standard Score | 38 | 42.26 (9.25) | 37 | 47.19 (9.10) |
| Externalizing Problems Standard Score | 38 | 41.68 (9.09) | 37 | 46.03 (9.32) |
| Internalizing Problems Standard Score | 38 | 41.87 (10.68) | 37 | 47.46 (9.56) |
| Internalizing Behavior in Clinical Range | 38 | 3 | 37 | 3 |
| Externalizing Behavior in Clinical Range | 38 | 3 | 37 | 5 |
| Communication Rate | 42 | 205 (60.39) | 38 | 157.58 (62.78) |
The effect of EMT on children’s problem behaviors
We first asked whether EMT was associated with the number of parent-reported problem behaviors exhibited one year after the intervention was delivered. Parameter estimates and confidence intervals are given in Table 2 for total problem behaviors, externalizing behaviors, and internalizing behaviors. After controlling for baseline problem behaviors, age at follow-up, baseline rate of communication, and gender, children in the EMT group had significantly fewer parent-reported total problem behaviors (−6.589, 95% CI [−11.804, −1.385]), externalizing behaviors (−2.231, 95% CI [−4.355, −0.108]), and internalizing behaviors (−2.091, 95% CI [−3.791,−0.391]).
Table 2.
Parameter Estimates for the effect of Enhanced Milieu Teaching on Problem Behaviors
| Model Parameters
|
||||
|---|---|---|---|---|
| Parameter | Est. (SE) | CI | Standardized Est. | Cohen’s d |
| EMT → Total Problem Behaviors | −6.589 (2.626) | [−11.804, −1.385] | −0.210 | −0.434 |
| EMT → Externalizing | −2.231 (1.067) | [−4.355, −0.108] | −0.169 | −0.346 |
| EMT → Internalizing | −2.091 (0.857) | [−3.791, −0.391] | −0.213 | −0.440 |
Note. EMT = Enhanced Milieu Teaching.
In order to address our second research question, effect sizes were calculated for the effect of EMT on each type of problem behavior, given in Table 2. The three effect sizes were similar (total problem behavior, d = −0.434; externalizing behavior, d = −0.346; internalizing behavior, d = −0.440). Using Cohen’s effect size interpretations, these three estimates are small to medium effects (Cohen, 1992).
The role of rate of communication as a mediator in the relation between EMT and problem behaviors
Model 4 from each series included all mediation variables and addressed the extent to which child rate of communication mediated the association between EMT and child problem behaviors. These models also included a term for the indirect path, or the product of the path from EMT to child rate of communication and the path from rate of communication to child problem behavior (a*b in Figure 1).
Parameter estimates and confidence intervals for all models for total problem behaviors are given in Table 3. Within Model 4, the paths from EMT to rate of communication, and from rate of communication to total problem behaviors remained significant, while the path from EMT to total problem behaviors was weakened compared to Model 2 (−4.218, 95% CI [−9.778, 1.345]). Because this confidence interval crossed zero, this path was no longer statistically significant. The estimated magnitude and confidence interval for the indirect path in this model of −1.887 (95% CI [−5.166, −0.720]) indicates that there is a significant mediation effect of rate of communication. Enhanced Milieu Teaching increased child rate of communication, which in turn decreased total problem behaviors in children.
Table 3.
Parameter Estimates and Confidence Intervals from the Five Structural Models for Total Problem Behaviors
| Parameters
|
|||||
|---|---|---|---|---|---|
| EMT → Language | Language → Tot. Prob. | EMT → Tot. Prob. | Indirect Path | ||
| Model 1 | Est. (SE) | 40.228 (12.702) | |||
| CI | [15.546, 64.911] | ||||
|
| |||||
| Model 2 | Est. (SE) | −.061 (.021) | |||
| CI | [−0.102, −0.020] | ||||
|
| |||||
| Model 3 | Est. (SE) | −6.589 (2.626) | |||
| CI | [−11.804, −1.385] | ||||
|
| |||||
| Model 4 | Est. (SE) | 40.228 (12.548) | −0.047 (0.023) | −4.218 (2.799) | −1.887 |
| CI | [15.546, 64.491] | [−.092, −.007] | [−9.778, 1.345] | [−4.529, −0.076] | |
|
| |||||
| Model 5 | Est. (SE) | 40.229 (12.565) | −.0610 (.021) | 0† | −2.507 |
| CI | [15.547, 64.911] | [−0.102, −0.020] | – | [−5.166, −0.720] | |
Model path was constrained to be 0.
Note. EMT = Enhanced Milieu Teaching. Tot. Prob. = Total Problem Behaviors.
In Model 5 for total problem behaviors, the path from EMT to child total problem behavior was constrained to a value of zero. This constraint forces the effect of EMT on total problem behaviors to be entirely explained by the indirect path through the effect of EMT on rate of communication. Fit values and χ2 difference test results are given in Table 4.
Table 4.
Comparative Fit Indices for Models 4 and 5 for Total Problem Behaviors
| Fit indices
|
||||||
|---|---|---|---|---|---|---|
| Model | Fit Value | χ2 | DF | Δ χ2 | Δ DF | p |
| 5. Full Model, with c′ constrained to 0 | 3999.472 | 3.967 | 6 | – | – | – |
| 4. Full Model, with c′ freely estimated | 3997.243 | 1.737 | 5 | 2.229 | 1 | 0.135 |
The SEM models were used to simultaneously estimate all required regression parameters, which gave greater precision and accounted for the relationships between all parameters. Unlike factor analysis, growth curve modeling, or many other SEM techniques that summarize a large amount of data with relatively few parameters, these mediation analyses estimated almost as many regressions and correlations as there were correlations in the data. As such, all of the models provide excellent fit by traditional fit statistics (e.g., RMSEA, CFI, TLI) because these fit statistics all compare a candidate model to a fully saturated model that includes all possible means, variances and covariances. This saturated model and our mediation models were very similar, thus, all fit statistics were very good (e.g., RMSEA = 0, all CFI = 1). In the current analyses, we relied on likelihood ratio tests to compare the relative differences between models rather than focus on the excellent fit of all candidate models.
The difference in fit between Model 4 and Model 5 was not significant (p = .135), indicating that the two models fit the data equally well. To determine whether rate of communication fully or partially mediated the relation between EMT and total problem behaviors, the change in the path between EMT and total problem behaviors between Model 3 and Model 4 (c and c′) was analyzed. The reduction in magnitude of this path was not large enough to indicate full mediation, and instead supported the conclusion that rate of communication only partially mediated the relation between EMT and total problem behaviors.
Parameter estimates and confidence intervals for all models for internalizing behaviors are given in Table 5. Similar to the pattern observed in total problem behaviors, within Model 4, the paths from EMT to rate of communication, and from rate of communication to internalizing behaviors remained significant, while the path from EMT to internalizing behaviors was weakened compared to Model 2 (−1.297, 95% CI [−3.117, 0.523]). The estimated magnitude and confidence interval for the indirect path in this model of −0.623 (95% CI [−1.491, −0.027]) indicated that there was a significant mediation effect of rate of communication.
Table 5.
Parameter Estimates and Confidence Intervals from the Five Structural Models for Internalizing Behaviors
| Parameters
|
|||||
|---|---|---|---|---|---|
| EMT →Language | Language → Internalizing | EMT → Internalizing | Indirect Path | ||
| Model 1 | Est. (SE) | 40.228 (12.604) | |||
| CI | [15.546,64.910] | ||||
|
| |||||
| Model 2 | Est. (SE) | −.020 (.0069) | |||
| CI | [−.033, −.007] | ||||
|
| |||||
| Model 3 | Est. (SE) | −2.091 (0.857) | |||
| CI | [−3.791, −0.391] | ||||
|
| |||||
| Model 4 | Est. (SE) | 40.228 (12.552) | −.015 (.0075) | −1.297 (0.915) | −0.623 |
| CI | [15.542, 64.918] | [−.030,−.001] | [−3.117, 0.523] | [−1.491, −0.027] | |
|
| |||||
| Model 5 | Est. (SE) | 40.228 (12.636) | −0.020 | 0† | −0.801 |
| CI | [15.544, 64.504] | [−0.033, −0.007] | – | [−1.690, −0.253] | |
Model path was constrained to be 0.
Note. EMT = Enhanced Milieu Teaching.
In Model 5, the path from EMT to child internalizing problems was again constrained to a value of zero. Fit values and χ2 difference test results are given in Table 6. The difference in fit between Model 4 and Model 5 was not significant (p = .160), indicating that the two models fit the data equally well. The change in the path between EMT and internalizing behaviors between Model 3 and Model 4 was not large enough to indicate full mediation, but again supported the conclusion that rate of communication only partially mediated the relation between EMT and internalizing behaviors.
Table 6.
Comparative Fit Indices for Models 4 and 5 for Internalizing Behaviors
| Fit indices
|
||||||
|---|---|---|---|---|---|---|
| Model | Fit Value | χ2 | DF | Δ χ2 | Δ DF | p |
| 5. Full Model, with c′ constrained to 0 | 3594.94 | 4.277 | 6 | – | – | – |
| 4. Full Model, with c′ freely estimated | 3592.97 | 2.301 | 5 | 1.977 | 1 | 0.160 |
Parameter estimates and confidence intervals for all models for externalizing behaviors are given in Table 7. Unlike for the models for total problem behaviors and internalizing behaviors, the path from rate of communication to externalizing behaviors did not remain significant in Model 4; however, the effect was in the same direction as for total problem and internalizing behaviors. Similar to the other models, the path from EMT to externalizing behaviors was weakened in Model 4 compared to Model 2 (−1.899, 95% CI [−4.216, 0.420]). The estimated magnitude and confidence interval for the indirect path in this model of −0.264, 95% CI [−1.183, 0.484]) indicated that there was not a significant mediation effect of rate of communication. While the paths in Model 4, apart from the path from EMT to rate of communication, were not significant, they were in the same direction as the estimates for total problem and internalizing behaviors.
Table 7.
Parameter Estimates from the Five Structural Models for Externalizing Behavior
| Parameters
|
|||||
|---|---|---|---|---|---|
| EMT →Language | Language → Externalizing | EMT → Externalizing | Indirect Path | ||
| Model 1 | Est. (SE) | 40.228 (12.562) | |||
| CI | [15.991, 64.910] | ||||
|
| |||||
| Model 2 | Est. (SE) | −0.013 (.009) | |||
| CI | [−0.030, 0.004] | ||||
|
| |||||
| Model 3 | Est. (SE) | −2.231 (1.067) | |||
| CI | [−4.355, −0.108] | ||||
|
| |||||
| Model 4 | Est. (SE) | 40.228 (12.540) | −0.007 (.009) | −1.899 (1.164) | −0.264 |
| CI | [15.546, 64.913] | [−0.023, 0.010] | −4.216, 0.420] | [−1.183, 0.484] | |
|
| |||||
| Model 5 | Est. (SE) | 40.228 (12.587) | −0.013 (0.009) | 0† | −0.514 |
| CI | [15.958, 64.910] | [−0.030, 0.004] | – | [−1.453, 0.182] | |
Model path was constrained to be 0.
Note. EMT = Enhanced Milieu Teaching.
DISCUSSION
The results from this study indicate that Enhanced Milieu Teaching, a parent-led language intervention, significantly reduced problem behaviors 12 months after the intervention in children with language delays. Although the intervention focused on increasing parent behaviors that facilitate language learning, the intervention also reduced problem behaviors in young children after the end of the intervention. This effect was consistent across internalizing behavior, externalizing behavior, and total problem behaviors. Because of the elevated level of problem behaviors in children with language delays, this finding is clinically meaningful. The fact that a single three-month intervention was able to affect multiple developmental domains suggests that EMT not only improves the language-learning environment in the home but also the general dyadic parent-child synchrony. The impact of this language intervention on problem behaviors also has important implications for policy, as applying only one intervention that is able to alter multiple developmental domains is desirable not only for reducing the cost of services, but more importantly for reducing demands on the family’s time and reducing the burden of implementing multiple interventions.
The changes in child problem behaviors due to EMT resulted in moderate effect sizes (see Table 2). For total problem behavior scores, EMT resulted in a reduction of approximately 6.5 raw points. Each item on the CBCL is rated as “not true,” “sometimes true,” or “often true,” meaning that a reduction in a raw score of six points may equate to a complete reduction in three symptoms, partial reduction in six symptoms, or some combination thereof. For the internalizing and externalizing scales, EMT resulted in a reduction of approximately two raw points. Average baseline internalizing and externalizing raw scores were 6.55 and 10.76, respectively, and did not differ significantly across groups. Thus, a 2 point change represents a 30.5% reduction in internalizing symptoms and an 18.6% reduction in externalizing symptoms.
We believe that EMT may have impacted problem behaviors through several mechanisms involving both the caregiver’s and child’s behavior. When considering parents’ behavior, EMT’s focus on encouraging parents to follow their children’s lead during play and to focus on their children’s interests may improve the general quality of the parent-child relationship by increasing parent-child synchrony and promoting more secure attachment. Additionally, parents are taught to model language based on their child’s communicative intent. In some situations, these models may serve as language-mediated emotion regulation strategies, such as labeling emotions or requesting help. When considering children’s behavior, EMT may have indirect effects on problem behaviors via its impact on children’s linguistic abilities. By improving children’s language and rate of communication, EMT may allow children to employ language to engage in both mutual and self-regulation strategies with greater frequency than the control group. This interpretation is supported by the significant mediation effect found for total problem behaviors and internalizing behaviors.
While EMT did significantly decrease externalizing behaviors in children, the indirect path through children’s rate of communication in the mediation model for externalizing behaviors was not significant. This difference in the effects of intervention on externalizing behavior as compared to total problem and internalizing behavior may be due to a number of reasons. While the coefficients in the externalizing behaviors model did not reach significance, all coefficients were in the same direction as in the other mediation models, suggesting that with a larger sample size, we may have found a significant relation. Additionally, when considering parents’ modeling of language-mediated emotion regulation strategies, it is possible that certain strategies differentially impacted internalizing behaviors over externalizing behaviors, and that parents naturally modeled these strategies with more frequency. For instance, labeling of emotions has been shown to impact internalizing behaviors, such as depression (Lenze et al., 2011), while other strategies, such as self-distraction, have been shown to impact externalizing behaviors.
In this sample, it is important to note that most children had subclinical levels of problem behaviors at baseline (internalizing T-score M = 46.75, externalizing T-scored M = 47.08, total problem behaviors T-score M = 47.7). In thinking about applying EMT as a clinical intervention for children with concomitant language delays and problem behaviors that are in the clinical range, it will be important for future researchers to investigate the impact of EMT on children who present with more severe problem behaviors. For instance, future studies may recruit participants from pediatric mental health agencies and select children with co-occurring language delays and clinically-significant problem behaviors.
Limitations and Future Directions
One limitation of the current findings is that we relied on parent report of children’s problem behaviors. Because discrepancies frequently exist between different informants’ ratings of children’s behavior (Achenbach, McConaughy, & Howell, 1987), future research should incorporate multiple sources of information on children’s problem behaviors, including both parent report and direct observation of children’s problem behaviors in naturalistic settings. Most children in the current study did not attend preschool and so it was not possible to include teacher reports of children’s problem behaviors. Parents trained in EMT may have changed their perceptions of child behavior as potentially communicative, consistent with the approach of noticing and responding to child communication and behavior taught in the intervention. It is also possible that at the beginning of the study, parents rated their children higher on internalizing behaviors because they interpreted their children’s lack of verbal communication as a sign of shyness, instead of rating true internalizing behaviors. While this is possible, many items on the CBCL internalizing domain have little to do with communication (i.e., “Looks unhappy without good reason,” “Nervous, highstrung, or tense”). We also removed one item, “Doesn’t answer when people talk to him/her” because of its reliance on language, and the pattern of significance for the coefficients in the final model for internalizing behaviors was unchanged. Nevertheless, future studies should incorporate multiple assessment methods for problem behaviors.
Another limitation of the study is that parents’ behaviors, such as responsiveness to distress and emotion-regulation strategies, were not coded specifically, limiting our ability to investigate the impact of EMT on these other behaviors. Likewise, children’s use of emotion regulation strategies was not coded. Children’s communication was observed in the clinic for the current study and was not analyzed in the home, an environment where problem behaviors are more likely to occur. Further, it is possible that language may influence internalizing and externalizing behaviors through different mechanisms. Future research into the effect of EMT on problem behaviors should include coding parent-child interactions in the home and examining how parent’s and children’s use of self- and mutual regulation strategies may differentially affect internalizing and externalizing behaviors. Examining the use of specific emotion regulation strategies may facilitate our understanding of how specific intervention strategies impact both t language skills and problem behaviors in children with language delays. Another consideration to make in interpreting the results of the current analysis is that 81% of the children in this study were male. While this is reflective of the general rate of language delays in children at this age (Rescorla & Alley, 2001), it is possible that the relation between language and problem behaviors may function differently in boys than in girls, and that EMT’s impact on these behaviors may vary by gender. However, the limited number of girls in the present study makes any statistical analysis of gender differences not feasible.
CONCLUSIONS
The outcomes of this study indicated that EMT was effective in reducing problem behaviors in children with language delays one year after intervention. This finding is important because of the need for early interventions that address language delays and other developmental concerns, such as problem behaviors, that often co-occur in this population of children. It is encouraging that a three month intervention resulted in changes in child problem behaviors 12 months after the intervention, suggesting enduring benefits of this intervention approach. Future research should focus on determining which specific EMT strategies are most effective in reducing child problem behaviors in order to maximize the efficacy of this intervention for this population.
Table 8.
Comparative Fit Indices for Models 4 and 5 for Externalizing Behaviors
| Fit indices
|
||||||
|---|---|---|---|---|---|---|
| Model | Fit Value | χ2 | DF | Δ χ2 | Δ DF | p |
| 5. Full Model, with c′ constrained to 0 | 3713.897 | 3.747 | 6 | – | – | – |
| 4. Full Model, with c′ freely estimated | 3711.297 | 1.147 | 5 | 2.600 | 1 | 0.107 |
Acknowledgments
The authors would like to thank the team at Vanderbilt University for implementing the study, as well as participating families for their time and commitment.
This research was supported by grant R324A090181 from the Institute of Education Sciences and by UL1 TR000445 from the National Center for Advancing Translational Sciences, NIH.
Contributor Information
Philip R. Curtis, Roxelyn and Richard Pepper Department of Communication Sciences and Disorders, Northwestern University, Evanston, IL
Megan Y. Roberts, Roxelyn and Richard Pepper Department of Communication Sciences and Disorders, Northwestern University, Evanston, IL.
Ryne Estabrook, Department of Medical Social Sciences, Feinberg School of Medicine, Northwestern University, Chicago, IL.
Ann P. Kaiser, Department of Special Education, Peabody College, Vanderbilt University, Nashville, TN
References
- Achenbach TM. The Child Behavior Profile: I. Boys aged 6–11. Journal of Consulting and Clinical Psychology. 1978;46(3):478–488. doi: 10.1037/0022-006X.46.3.478. [DOI] [PubMed] [Google Scholar]
- Achenbach TM, McConaughy SH, Howell CT. Child/adolescent behavioral and emotional problems: implications of cross-informant correlations for situational specificity. Psychological Bulletin. 1987;101(2):213–232. doi: 10.1037/0033-2909.101.2.213. [DOI] [PubMed] [Google Scholar]
- Achenbach TM, Rescorla LA. Manual for the ASEBA school-age forms & profiles: an integrated system of multi-informant assessment. Burlington, VT: University of Vermont; 2001. [Google Scholar]
- Allan NP, Joye SW, Lonigan CJ. Does gender moderate the relations netween externalizing behavior and key emergent literacy abilities? Evidence from a longitudinal study. Journal of Attention Disorders. 2013 doi: 10.1177/1087054713512522. [DOI] [PubMed] [Google Scholar]
- Angold A, Egger HL. Preschool psychopathology: lessons for the lifespan. J Child Psychol Psychiatry. 2007;48(10):961–966. doi: 10.1111/j.1469-7610.2007.01832.x. [DOI] [PubMed] [Google Scholar]
- Baron RM, Kenny DA. The moderator–mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology. 1986;51(6):1173–1182. doi: 10.1037/0022-3514.51.6.1173. [DOI] [PubMed] [Google Scholar]
- Bayley N. Bayley Scales of Infant Development III. San Antonio, TX: Psychological Corporation; 2005. [Google Scholar]
- Benasich AA, Curtiss S, Tallal P. Language, learning, and behavioral disturbances in childhood: A longitudinal perspective. Journal of the American Academy of Child & Adolescent Psychiatry. 1993;32(3):585–594. doi: 10.1097/00004583-199305000-00015. [DOI] [PubMed] [Google Scholar]
- Bollen KA, Stine R. Direct and indirect effects: Classical and bootstrap estimates of variability. Sociological Methodology. 1990;20(1):115–140. doi: 10.2307/271084. [DOI] [Google Scholar]
- Briggs-Gowan MJ, Carter AS, Skuban EM, Horwitz SM. Prevalence of social-emotional and behavioral problems in a community sample of 1-and 2-year-old children. Journal of the American Academy of Child & Adolescent Psychiatry. 2001;40(7):811–819. doi: 10.1097/00004583-200107000-00016. [DOI] [PubMed] [Google Scholar]
- Brinkmeyer MY, Eyberg SM. Parent-child interaction therapy for oppositional children. In: Kazdin AE, Weisz JR, editors. Evidence-based psychotherapies for children and adolescents. New York, NY: Guilford Press; 2003. pp. 204–223. [Google Scholar]
- Catts HW, Fey ME, Tomblin JB, Zhang X. A longitudinal investigation of reading outcomes in children with language impairments. Journal of Speech, Language, and Hearing Research. 2002;45(6):1142–1157. doi: 10.1044/1092-4388(2002/093). [DOI] [PubMed] [Google Scholar]
- Caulfield MB, Fischel JE, DeBaryshe BD, Whitehurst GJ. Behavioral correlates of developmental expressive language disorder. Journal of Abnormal Child Psychology. 1989;17(2):187–201. doi: 10.1007/BF00913793. [DOI] [PubMed] [Google Scholar]
- Cervantes CA, Callanan MA. Labels and explanations in mother–child emotion talk: Age and gender differentiation. Developmental psychology. 1998;34(1):88–98. doi: 10.1037/0012-1649.34.1.88. [DOI] [PubMed] [Google Scholar]
- Chow JC. The Concurrent and Predictive Association between Language and Behavior: A Systematic Review and Meta-Analysis. Manuscript submitted for publication 2016 [Google Scholar]
- Cohen J. A power primer. Psychological Bulletin. 1992;112(1):155–159. doi: 10.1037/0033-2909.112.1.155. [DOI] [PubMed] [Google Scholar]
- Cole PM, Armstrong LM, Pemberton CK. The role of language in the development of emotion regulation. In: Calkins SD, Bell MA, editors. Child development at the intersection of emotion and cognition. Washington, DC: American Psychological Association; 2010. [Google Scholar]
- Cole PM, Zahn-Waxler C, Fox NA, Usher BA, Welsh JD. Individual differences in emotion regulation and behavior problems in preschool children. Journal of Abnormal Psychology. 1996;105(4):518. [PubMed] [Google Scholar]
- Deater-Deckard K, O’Connor TG. Parent–child mutuality in early childhood: Two behavioral genetic studies. Developmental psychology. 2000;36(5):561. doi: 10.1037/0012-1649.36.5.561. [DOI] [PubMed] [Google Scholar]
- Egger HL, Angold A. Common emotional and behavioral disorders in preschool children: presentation, nosology, and epidemiology. Journal of Child Psychology and Psychiatry. 2006;47(3–4):313–337. doi: 10.1111/j.1469-7610.2006.01618.x. [DOI] [PubMed] [Google Scholar]
- Eyberg SM, Robinson EA. Parent‐child interaction training: Effects on family functioning. Journal of Clinical Child & Adolescent Psychology. 1982;11(2):130–137. doi: 10.1080/15374418209533076. [DOI] [Google Scholar]
- Fujiki M, Brinton B, Isaacson T, Summers C. Social behaviors of children sith language impairment on the playground: A pilot study. Language, Speech, and Hearing Services in Schools. 2001;32(2):101–113. doi: 10.1044/0161-1461(2001/008). [DOI] [PubMed] [Google Scholar]
- Garber J, Dodge KA, editors. The development of emotion regulation and dysregulation. New York, NY: Cambridge University Press; 1991. [Google Scholar]
- Gottlieb G. The roles of experience in the development of behavior and the nervous system. Neural and behavioral specificity. 1976;3:25–54. [Google Scholar]
- Gratz KL, Roemer L. Multidimensional assessment of emotion regulation and dysregulation: Development, factor structure, and initial validation of the difficulties in emotion regulation scale. Journal of psychopathology and behavioral assessment. 2004;26(1):41–54. doi: 10.1023/B:JOBA.0000007455.08539.94. [DOI] [Google Scholar]
- Gross JJ. The emerging field of emotion regulation: an integrative review. Review of general psychology. 1998;2(3):271. doi: 10.1037/1089-2680.2.3.271. [DOI] [Google Scholar]
- Gross JJ, editor. Handbook of emotion regulation. 2. New York, NY: Guilford publications; 2014. [Google Scholar]
- Halligan SL, Cooper PJ, Fearon P, Wheeler SL, Crosby M, Murray L. The longitudinal development of emotion regulation capacities in children at risk for externalizing disorders. Development and psychopathology. 2013;25(02):391–406. doi: 10.1017/S0954579412001137. [DOI] [PubMed] [Google Scholar]
- Harris P. Desires, beliefs, and language. In: Carruthers P, Smith PK, editors. Theories of theories of mind. Cambridge, England: Cambridge University Press; 1996. pp. 344–354. [Google Scholar]
- Harrist AW, Waugh RM. Dyadic synchrony: Its structure and function in children’s development. Developmental Review. 2002;22(4):555–592. [Google Scholar]
- Hart KI, Fujiki M, Brinton B, Hart CH. The relationship between social behavior and severity of language impairment. Journal of Speech, Language, and Hearing Research. 2004;47(3):647–662. doi: 10.1044/1092-4388(2004/050). [DOI] [PubMed] [Google Scholar]
- Hayden EP, Mash EJ. Child Psychopathology: A Developmental-Systems Perspective. In: Mash EJ, Barkley RA, editors. Child Psychopathology. 3. New York, NY: The Guilford Press; 2014. pp. 3–74. [Google Scholar]
- Hinshaw SP. On the distinction between attentional deficits/hyperactivity and conduct problems/aggression in child psychopathology. Psychological Bulletin. 1987;101(3):443–463. doi: 10.1037/0033-2909.101.3.443. [DOI] [PubMed] [Google Scholar]
- Hollo A, Wehby JH, Oliver RM. Unidentified language deficits in children with emotional and behavioral disorders: A meta-analysis. Exceptional Children. 2014;80(2):169–186. doi: 10.1177/001440291408000203. [DOI] [Google Scholar]
- Horwitz SM, Irwin JR, Briggs-Gowan MJ, Heenan JMB, Mendoza J, Carter AS. Language delay in a community cohort of young children. Journal of the American Academy of Child & Adolescent Psychiatry. 2003;42(8):932–940. doi: 10.1097/01.CHI.0000046889.27264.5E. [DOI] [PubMed] [Google Scholar]
- Irwin JR, Carter AS, Briggs-Gowan MJ. The social-emotional development of “late-talking” toddlers. Journal of the American Academy of Child & Adolescent Psychiatry. 2002;41(11):1324–1332. doi: 10.1097/00004583-200211000-00014. [DOI] [PubMed] [Google Scholar]
- Kaiser AP. Parent-implemented language intervention: An environmental system perspective. In: Kaiser AP, Gray DB, editors. Enhancing children’s communication: Research foundations for intervention. Baltimore, MD: P.H. Brookes; 1993. pp. 63–84. [Google Scholar]
- Kopp CB. Regulation of distress and negative emotions: A developmental view. Developmental Psychology. 1989;25(3):343–354. doi: 10.1037/0012-1649.25.3.343. [DOI] [Google Scholar]
- Kovacs M, Devlin B. Internalizing disorders in childhood. Journal of Child Psychology and Psychiatry. 1998;39(01):47–63. [PubMed] [Google Scholar]
- Lane RD, Schwartz GE. Levels of emotional awareness: A cognitive-developmental theory and its application to psychopathology. The American Journal of Psychiatry. 1987;144(2):133–143. doi: 10.1176/ajp.144.2.133. [DOI] [PubMed] [Google Scholar]
- Lenze SN, Pautsch J, Luby J. Parent–child interaction therapy emotion development: A novel treatment for depression in preschool children. Depression and Anxiety. 2011;28(2):153–159. doi: 10.1002/da.20770. [DOI] [PMC free article] [PubMed] [Google Scholar]
- López-Pérez B, Gummerum M, Wilson E, Dellaria G. Studying Children’s Intrapersonal Emotion Regulation Strategies from the Process Model of Emotion Regulation. The Journal of Genetic Psychology. 2016:1–16. doi: 10.1080/00221325.2016.1230085. [DOI] [PubMed] [Google Scholar]
- Luby J, Belden AC, Pautsch J, Si X, Spitznagel E. The clinical significance of preschool depression: impairment in functioning and clinical markers of the disorder. Journal of Affective Disorders. 2009;112(1–3):111–119. doi: 10.1016/j.jad.2008.03.026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Masten AS, Roisman GI, Long JD, Burt KB, Obradović J, Riley JR, Tellegen A. Developmental cascades: linking academic achievement and externalizing and internalizing symptoms over 20 years. Developmental Psychology. 2005;41(5):733–746. doi: 10.1037/0012-1649.41.5.733. [DOI] [PubMed] [Google Scholar]
- Mesman J, Koot HM. Early preschool predictors of preadolescent internalizing and externalizing DSM-IV diagnoses. Journal of the American Academy of Child & Adolescent Psychiatry. 2001;40(9):1029–1036. doi: 10.1097/00004583-200109000-00011. [DOI] [PubMed] [Google Scholar]
- Neece CL, Green SA, Baker BL. Parenting stress and child behavior problems: a transactional relationship across time. Am J Intellect Dev Disabil. 2012;117(1):48–66. doi: 10.1352/1944-7558-117.1.48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Olswang LB, Bain BA. Intervention issues for toddlers with specific language impairments. Topics in Language Disorders. 1991;11(4):69–86. [Google Scholar]
- Paul R. Clinical implications of the natural history of slow expressive language development. American Journal of Speech-Language Pathology. 1996;5:5–30. [Google Scholar]
- Paul R, James DF. Language delay and parental perceptions. Journal of the American Academy of Child & Adolescent Psychiatry. 1990;29(4):669–670. doi: 10.1097/00004583-199007000-00030. [DOI] [PubMed] [Google Scholar]
- Preston JL, Frost SJ, Mencl WE, Fulbright RK, Landi N, Grigorenko E, Pugh KR. Early and late talkers: school-age language, literacy and neurolinguistic differences. Brain. 2010;133(8):2185–2195. doi: 10.1093/brain/awq163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Prior M, Bavin E, Cini E, Eadie P, Reilly S. Relationships between language impairment, temperament, behavioural adjustment and maternal factors in a community sample of preschool children. International Journal of Language & Communication Disorders. 2011;46(4):489–494. doi: 10.1111/j.1460-6984.2011.00003.x. [DOI] [PubMed] [Google Scholar]
- Prizant BM, Meyer EC. Socioemotional aspects of language and social-communication disorders in young children and their families. American Journal of Speech-Language Pathology. 1993;2(3):56–71. [Google Scholar]
- Qi CH, Kaiser AP. Problem Behaviors of Low-Income Children With Language Delays: An Observation Study. Journal of Speech, Language, and Hearing Research. 2004;47(3):595–609. doi: 10.1044/1092-4388(2004/046). [DOI] [PubMed] [Google Scholar]
- Raver CC. Relations between social contingency in mother-child interaction and 2-year-olds’ social competence. Developmental Psychology. 1996;32(5):850. [Google Scholar]
- Rescorla L. Language and reading outcomes to age 9 in late-talking toddlers. Journal of Speech, Language, and Hearing Research. 2002;45(2):360–371. doi: 10.1044/1092-4388(2002/028). [DOI] [PubMed] [Google Scholar]
- Rescorla L. Age 13 language and reading outcomes in late-talking toddlers. Journal of Speech, Language, and Hearing Research. 2005;48(2):459–472. doi: 10.1044/1092-4388(2005/031). [DOI] [PubMed] [Google Scholar]
- Rescorla L. Late talkers: do good predictors of outcome exist? Developmental Disabilities Research Reviews. 2011;17(2):141–150. doi: 10.1002/ddrr.1108. [DOI] [PubMed] [Google Scholar]
- Rescorla L, Alley A. Validation of the Language Delopment Survey (LDS): A parent report tool for identifying language delay in toddlers. Journal of Speech, Language, and Hearing Research. 2001;44(2):434–445. doi: 10.1044/1092-4388(2001/035). [DOI] [PubMed] [Google Scholar]
- Roben CK, Cole PM, Armstrong LM. Longitudinal relations among language skills, anger expression, and regulatory strategies in early childhood. Child Development. 2013;84(3):891–905. doi: 10.1111/cdev.12027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roberts MY, Kaiser AP. The effectiveness of parent-implemented language interventions: A meta-analysis. American Journal of Speech-Language Pathology. 2011;20(3):180–199. doi: 10.1044/1058-0360(2011/10-0055). [DOI] [PubMed] [Google Scholar]
- Roberts MY, Kaiser AP. Early intervention for toddlers with language delays: A randomized controlled trial. Pediatrics. 2015;135(4):686–693. doi: 10.1542/peds.2014-2134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Robertson SB, Weismer SE. Effects of treatment on linguistic and social skills in toddlers with delayed language development. Journal of Speech, Language, and Hearing Research. 1999;42(5):1234–1248. doi: 10.1044/jslhr.4205.1234. [DOI] [PubMed] [Google Scholar]
- Rocissano L, Slade A, Lynch V. Dyadic synchrony and toddler compliance. Developmental Psychology. 1987;23(5):698. [Google Scholar]
- Sala MN, Pons F, Molina P. Emotion regulation strategies in preschool children. British Journal of Developmental Psychology. 2014;32(4):440–453. doi: 10.1111/bjdp.12055. [DOI] [PubMed] [Google Scholar]
- Sobel ME. Asymptotic confidence intervals for indirect effects in structural equation models. Sociological Methodology. 1982;13(1982):290–312. doi: 10.2307/270723. [DOI] [Google Scholar]
- Spinrad TL, Stifter CA, Donelan‐McCall N, Turner L. Mothers’ Regulation Strategies in Response to Toddlers’ Affect: Links to Later Emotion Self‐Regulation. Social Development. 2004;13(1):40–55. [Google Scholar]
- Stansbury K, Zimmermann LK. Relations among child language skills, maternal socialization of emotion regulation, and child behavior problems. Child Psychiatry and Human Development. 1999;30(2):121–142. doi: 10.1023/A:1021954402840. [DOI] [PubMed] [Google Scholar]
- Thompson RA. Emotion regulation: A theme in search of definition. Monographs of the society for research in child development. 1994;59(2–3):25–52. [PubMed] [Google Scholar]
- Trentacosta CJ, Fine SE. Emotion knowledge, social competence, and behavior problems in childhood and adolescence: A meta‐analytic review. Social Development. 2010;19(1):1–29. doi: 10.1111/j.1467-9507.2009.00543.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tronick EZ. Emotions and emotional communication in infants. American Psychologist. 1989;44(2):112–119. doi: 10.1037/0003-066X.44.2.112. [DOI] [PubMed] [Google Scholar]
- Zambrana IM, Pons F, Eadie P, Ystrom E. Trajectories of language delay from age 3 to 5: persistence, recovery and late onset. International Journal of Language & Communication Disorders. 2014;49(3):304–316. doi: 10.1111/1460-6984.12073. [DOI] [PubMed] [Google Scholar]