

Background
Creation of pneumoperitoneum is the first step in laparoscopy and is often done blindly using a Veress needle. Although generally safe, this technique may be associated with life threatening complications such as injury to bowel and intra-abdominal vessels, especially in obese patients.1–3 We describe a simple technique of ultrasound guided visual insertion of a Veress needle.
Technique
The stomach is decompressed by an orogastric tube. The ultrasonography probe is tilted, rotated or both to improve visualisation of the three layers of the abdominal wall (Fig 1). With an oblique orientation on the abdominal wall, the muscle planes are identified and the Veress needle is inserted. (We use Palmer’s point for insertion [Fig 2].) The progression of the needle is assessed by ultrasonography (Fig 3). Once the tip is in the peritoneal cavity, insufflation is begun and can be visualised as a hypoechoic shadow around the tip of the Veress needle.
Figure 1.

The layers of the abdominal wall are well visualised even in morbid obese patients using real time ultrasonography
Figure 2.
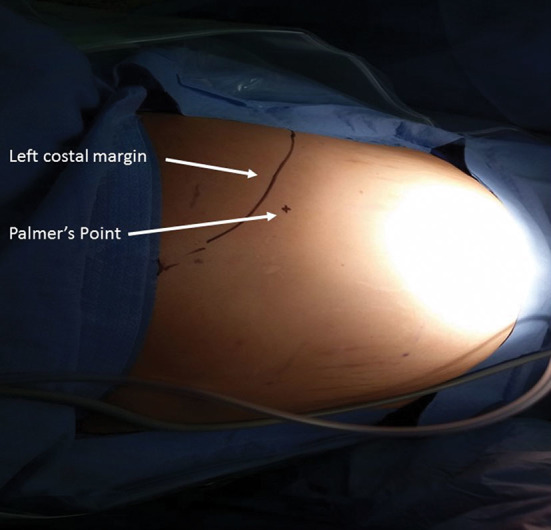
Palmer’s point is our preferred site for Veress needle insertion, lying two fingerbreadths below the left subcostal margin in the midclavicular line
Figure 3.

The path of the Veress needle (arrow) is visualised using real time ultrasonography
Discussion
We have standardised this technique in 53 patients who underwent weight loss surgery without any complications. Use of this method eliminates the blind steps of Veress needle insertion (two blind entries and one blind gas insufflation).4 This technique holds promise for decreasing the risks and improving the safety of trocar insertion without requiring costly optical devices.
References
- 1.Azevedo JL, Azevedo OC, Miyahira SA et al. Injuries caused by Veress needle insertion for creation of pneumoperitoneum: a systematic literature review. Surg Endosc 2009; : 1,428–1,432. [DOI] [PubMed] [Google Scholar]
- 2.Abbassi-Ghadi N, Skull A. Trocar injury of abdominal wall vessels: a simple method to stop the haemorrhage. Ann R Coll Surg Engl 2011; : 552. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Schäfer M, Lauper M, Krähenbühl L. Trocar and Veress needle injuries during laparoscopy. Surg Endosc 2001; : 275–280. [DOI] [PubMed] [Google Scholar]
- 4.Jiang X, Anderson C, Schnatz PF. The safety of direct trocar versus Veress needle for laparoscopic entry: a meta-analysis of randomized clinical trials. J Laparoendosc Adv Surg Tech A 2012; : 362–370. [DOI] [PubMed] [Google Scholar]