

Abstract
Rationale:
Surgical site infection (SSI) following spine surgeries involving internal fixation often require removing the instrument; however, this can cause spinal instability. Previous reports have demonstrated the usefulness of vacuum sealing drainage (VSD) therapy, but the cases require wound opening, aseptic condition to replace the VSD device, and a secondary operation to close the wound. Thus, to improve the VSD treatment and develop a maneuverable procedure, make sense in spine surgery.
Patients concerns:
A 59-year-old male patient with a T12 vertebral fracture was affected by SSIs after spinal osteotomy with internal fixation.
Diagnoses:
The patient complained of wound exudation and had a fever 3 weeks after posterior spinal surgery. Initial serum investigations showed elevated white blood cell count and bacterial cultures of wound exudate were positive for Enterococcus faecalis. Therefore, SSI is confirmed.
Interventions:
The infection was not controlled after 2 debridements, so the patient was treated with VSD treatment. The VSD foam dressings containing a drainage tube were placed into the wound from the exudation site of the wound until they contacted the internal fixation devices. After covering external fixation devices, continuous drainage was performed for 24 h. The VSD device was replaced every 4 to 5 days until the wound effusion stopped. All of the operations were performed at the bedside without complex manipulation or secondary closure under harsh aseptic condition.
Outcomes:
Wound exudation decreased remarkably and the infection was controlled 2 weeks after the application of VSD treatment. After 5 weeks, inflammatory indicators all decreased to normal levels and the exudate of the wound had stopped. The VSD treatment was then terminated and the drainage site of the wound was sutured. After 7 weeks, complete wound healing was achieved and no infection recurred during the 6-month follow-up.
Lessons:
VSD could be a reliable treatment for SSIs that require preservation of internal fixation. Complete opening of the wound during the VSD treatment and secondary wound closure surgery were avoided.
Keywords: posterior spine surgery, spinal internal fixation, surgical site infection, vacuum sealing drainage
1. Introduction
Surgical site infection (SSI) in posterior spine surgery with internal fixation remains a challenge for clinical surgeons. Previous studies have shown that bacteria involved in these infections form biofilms that adhere to internal fixation devices and that these films are resistant to antimicrobial agents.[1,2] To treat such infections, surgical removal of internal fixation is sometimes required, although the loss of fixation can promote spinal instability.[3–5] Therefore, strategies to control infection while retaining internal fixation are needed. Vacuum sealing drainage (VSD) is an efficient drainage system to achieve secure and rapid wound healing of traumatic soft wounds and chronic infections.[6] A previous study demonstrated the usefulness of VSD therapy,[7] but these cases required wound opening during the VSD treatment and the VSD applications were done under aseptic condition in the operation theater, which increased patient discomfort, limited patient activity, and required advanced medical facilities. Moreover, these patients require a second surgery to close the wound. Thus, improvement of the VSD treatment and development of a maneuverable procedure would make sense to reduce patient discomfort, lower the expense, and improve clinical application. Here, we report a case of SSI of posterior spine surgery with internal fixation wherein VSD was successfully used to promote wound healing with all medical practices performed at the bedside.
2. Case report
Written informed consent was obtained from the patient for publication of the article.
This case was a 59-year-old, previously healthy male who suffered from intractable back pain arising from a T12 traumatic vertebral fracture (Fig. 1). The back pain did not improve after 3 months of bed rest, and thus a posterior pedicle subtraction osteotomy (PSO) combined with pedicle screw fixation (UPASS, Titanium, WeiGao Orthopaedic Devices Company, Weihai City, China) was performed (Fig. 2). The patient received 3 intravenous perioperative antibiotics (cefuroxime), 1 dose 30 min preoperatively, and 2 additional doses at 8 and 16 h postoperatively and recovered well during the early postoperative period. The patient was discharged 1 week after the operation. Two weeks after discharge, the patient complained of wound exudation (Fig. 3) and had a fever (37.8°C). Initial serum investigations showed elevated white blood cell count (WBC) of 10,040/mm3 (normal range 3500–9500/mm3), hypersensitive C-reactive protein (hs-CRP) levels of 11.30 mg/L (normal range 0–3.00 mg/L), and erythrocyte sedimentation rate (ESR) of 42 mm/h (normal range 0–15 mm/h). Bacterial cultures of wound exudate were positive for Enterococcus faecalis and a drug sensitivity test was performed. After 4 days of intravenous treatment with the selected antibiotics (vancomycin and ceftazidime), infection symptoms did not improve, so wound debridement was performed. The necrotic tissue and bone grafts were removed and a pulse lavage system (WJ-06, Beijing WANJIE Medical Device Co., Ltd, Beijing City, China) was used during the debridements. The internal fixation was not found loosening or ruptured and no local antibiotics were used when the wound was closed. After 2 debridement surgeries, the infection remained uncontrolled and the patient presented with high fever and recurrent wound exudation (Fig. 4). One suture around the exudation site was then removed and appropriately sized VSD foam dressings containing a drainage tube were placed into the wound such that they contacted the internal fixation devices (Fig. 5). The foam contacted the internal fixation and assisted in facilitating drainage of the exudate. After a semipermeable membrane (Smith & Nephew, Hull, United Kingdom) was used to seal the wound, the drainage tube was connected to a negative pressure source with regular replacement of VSD every 4 to 5 days. Meanwhile, the patient received systemic antibiotic therapy.
Figure 1.
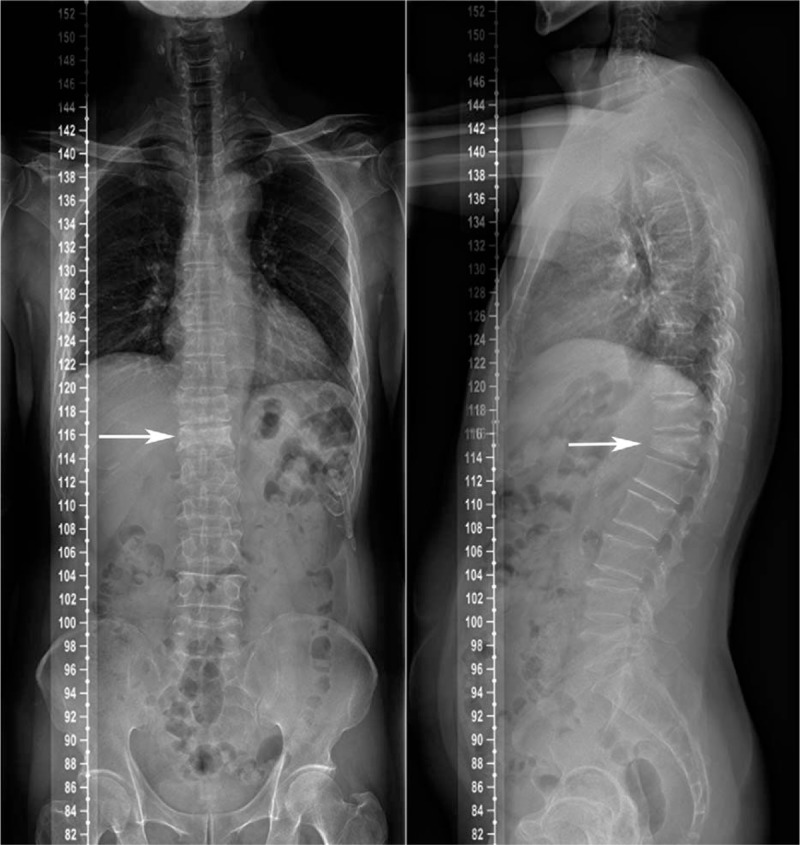
Preoperative posteroanterior and lateral radiographs of the patient's spine showing a vertebral compression fracture of T12.
Figure 2.

Postoperative posteroanterior and lateral radiographs of the patient's spine.
Figure 3.

Wound exudation occurred 3 weeks after surgery.
Figure 4.

Wound exudation recurred after 2 debridement surgeries. Drainage gauze was inserted into the wound from the ostium.
Figure 5.

Wound covered with VSD. The image in the bottom right corner shows the VSD foam dressings containing the drainage tube. VSD = vacuum sealing drainage.
Two weeks after initiating the VSD treatment the patient's body temperature returned to normal and the wound exudation was remarkably decreased. After 5 weeks, the hs-CRP, WBC, and ESR all returned to normal levels and the exudate of the wound had stopped. The VSD treatment was then stopped and the drainage site of the wound was sutured at the bedside. After 7 weeks, complete wound healing was achieved, and no infection recurred during the 6-month follow-up (Fig. 6).
Figure 6.

The wound was completely healed.
3. Discussion
Posterior spinal surgery is associated with higher infection rates compared with anterior spinal surgery,[8] and often requires use of spine instrumentation to stabilize the operative segments. For SSI after posterior spine surgery, the stabilization devices are often removed to facilitate infection control, but removal of these devices increases the risk of spinal instability. In the case described here, after undergoing PSO the patient developed SSI. Two debridements were performed, but the infection symptoms persisted. As mentioned above, removal of spinal stabilization devices would increase the risk of spinal instability and neurological risks. Strict bed rest for 2 to 3 months would be required to decrease these risks, but would also significantly decrease the patient's quality of life. As an alternative, VSD was used for this case with remarkable therapeutic efficacy.
VSD is a negative-pressure technique that drains seepage, pus, and necrotic tissues[9] to reduce opportunities for bacterial growth at the wound site. More importantly, VSD can eliminate wound lacuna, which contains pus and necrotic tissues that can hinder the anti-infective function of paraspinal muscle and granulation tissues.[10] By eliminating wound lacuna using negative pressure, the muscle and granulation tissue would have closer contact with the internal fixation device surfaces to exert antimicrobial effects. Due to retention of the internal fixation, the patient is not strictly confined to bed, but instead may move around the negative pressure source under brace protection. Another advantage of VSD treatment in this case is that all of the operations after the debridement were performed at the bedside without complex manipulation and secondary closure surgery under harsh aseptic condition was not needed, so the treatment is available for primary medical organizations and has a lower cost. The main focus of the procedure is that VSD foam dressings were placed into the wound deeply enough so that they could contacted the internal fixation devices. Otherwise, the drainage would be insufficient and soft tissue could hinder the drainage of VSD. Here, the internal fixation acts as a draining device in the wound and can help to achieve adequate drainage.
Staphylococcus aureus is the most common bacteria causing SSI after internal fixation,[11] but E faecalis have also been identified as common causative pathogens in SSI after internal fixation.[12] Many studies have shown that VSD can help infectious wounds heal regardless of the bacterial species.[7,13] This is an indication that removal of necrotic tissues and eliminating the wound lacuna are quite important to prevent infections.
This patient did undergo 2 debridements, which improved the infection symptoms soon after the operation, but wound exudation recurred later. This outcome demonstrated that debridement alone cannot completely eliminate bacteria and suggests that the patient might have recovered sooner if VSD had been applied before the second debridement. The bone grafts were removed in the first debridement surgery, but there were still some small sequestra that blocked the drainage tube in the early stage of VSD treatment. Therefore, it is important to eliminate as many as possible. Lack of a bone graft may cause spine fusion difficulties, so the patient was required to strictly wear a brace for 3 months. There were no signs of loosening or breakage of internal fixation during follow-up.
4. Conclusions
Although this strategy should be applied to a larger number of patients, the findings described here indicate that VSD is a possible treatment option for SSI after posterior spine surgery, especially for those patients requiring retention of internal fixation. In this case, we improved the VSD treatment in SSI with internal fixation. Because the infectious wound was not opened during VSD treatment, all operations were performed at the bedside and secondary closure surgery was avoided, which reduced patient discomfort, lowered costs, and improved general clinical application.
Footnotes
Abbreviations: ESR = erythrocyte sedimentation rate, hs-CRP = hypersensitive C-reactive protein, PSO = pedicle subtraction osteotomy, SSI = surgical site infection, VSD = vacuum sealing drainage, WBC = white blood cell count.
The authors have no funding and conflicts of interest to disclose.
References
- [1].Costerton JW, Stewart PS, Greenberg EP. Bacterial biofilms: a common cause of persistent infections. Science 1999;284:1318–22. [DOI] [PubMed] [Google Scholar]
- [2].Halliman DG, Ahearn DG. Relative susceptibilities to vancomycin and quinupristin-dalfopristin of adhered and planktonic vancomycin-resistant and vancomycin-susceptible coagulase-negative staphylococci. Curr Microbiol 2004;48:214–8. [DOI] [PubMed] [Google Scholar]
- [3].Rasouli MR, Viola J, Maltenfort MG, et al. Hardware removal due to infection after open reduction and internal fixation: trends and predictors. Arch Bone Joint Surg 2015;3:184–92. [PMC free article] [PubMed] [Google Scholar]
- [4].Picada R, Winter RB, Lonstein JE, et al. Postoperative deep wound infection in adults after posterior lumbosacral spine fusion with instrumentation: incidence and management. J Spinal Disord 2000;13:42–5. [DOI] [PubMed] [Google Scholar]
- [5].Cahill PJ, Warnick DE, Lee MJ, et al. Infection after spinal fusion for pediatric spinal deformity: thirty years of experience at a single institution. Spine 2010;35:1211–7. [DOI] [PubMed] [Google Scholar]
- [6].Argenta LC, Morykwas MJ. Vacuum-assisted closure: a new method for wound control and treatment: clinical experience. Ann Plast Surg 1997;38:563–76. [PubMed] [Google Scholar]
- [7].Kale M, Padalkar P, Mehta V. Vacuum-assisted closure in patients with post-operative infections after instrumented spine surgery: a series of 12 cases. J Orthop Case Rep 2017;7:95–100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Wimmer C, Gluch H, Franzreb M, et al. Predisposing factors for infection in spine surgery: a survey of 850 spinal procedures. J Spinal Disord 1998;11:124–8. [PubMed] [Google Scholar]
- [9].Chen B, Hao F, Yang Y, et al. Prophylactic vacuum sealing drainage (VSD) in the prevention of postoperative surgical site infections in pediatric patients with contaminated laparotomy incisions. Medicine 2017;96:e6511. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Dumanian GA, Ondra SL, Liu J, et al. Muscle flap salvage of spine wounds with soft tissue defects or infection. Spine 2003;28:1203–11. [DOI] [PubMed] [Google Scholar]
- [11].Shah MQ, Zardad MS, Khan A, et al. Surgical site infection in orthopaedic implants and its common bacteria with their sensitivities to antibiotics, in open reduction internal fixation. J Ayub Med Coll Abbottabad 2017;29:50–3. [PubMed] [Google Scholar]
- [12].Suzuki T, Morgan SJ, Smith WR, et al. Postoperative surgical site infection following acetabular fracture fixation. Injury 2010;41:396–9. [DOI] [PubMed] [Google Scholar]
- [13].Wang J, Zhang H, Wang S. Application of vacuum sealing drainage in the treatment of internal fixation instrument exposure after early postoperative infection. Minerva Chir 2015;70:17–22. [PubMed] [Google Scholar]