

Abstract
Human epidermal growth factor receptor 2 (HER-2) has an important clinical role in various cancers. However, the prognostic impact of HER-2 in gastric cancer (GC) is controversial. RAB1A is an important small molecule in the mechanistic target of rapamycin signalling pathway, which is one of the downstream signalling pathways of the epidermal growth factor receptor family. In recent years, the aberrant expression of RAB1A has been reported in a number of tumours, but its regulation in GC has not been extensively examined. Therefore, the present study investigated the expression pattern and prognostic significance of HER-2 and RAB1A in gastric adenocarcinoma (CAG). A comprehensive analysis was performed to examine the expression level of HER-2 and RAB1A in 280 cases of paired paraffin-embedded GAC tissues and an additional 120 archived GAC tissue samples. HER-2 and RAB1A protein expression was assessed by immunohistochemistry and cases with a 2+ score for HER-2 expression levels were subjected to fluorescence in situ hybridization to determine the HER-2 amplification status. Furthermore, HER-2 and RAB1A mRNA expression was quantified by reverse transcription-quantitative polymerase chain reaction. The comparison of continuous data between two groups was performed using a paired-samples t-test. Clinical correlations were determined using Pearson's Chi-square and Fisher's exact tests. Kaplan-Meier survival curves were used to estimate overall survival (OS). Cox proportional hazards models were used to determine associations between HER-2 and RAB1A expression and outcomes. Regression analyses were performed to detect the correlation between the mRNA levels of HER-2 and RAB1A in GAC tissues. It was observed that RAB1A was significantly overexpressed in GAC tissues compared with normal tissues (P<0.001). Approximately 12.86% of the 280 GAC patients had HER-2 amplification. Additionally, RAB1A expression was significantly associated with a short OS (P<0.001) but there were no significant differences in survival between the HER-2 high-expression group and the HER-2 low-expression group. Additionally, the co-expression of HER-2 and RAB1A indicated poorer OS than the overexpression of each protein (P=0.001), and the two factors were significantly positively correlated in GAC (P=0.012). These findings may be used to further explore the molecular mechanisms and regulatory associations among signalling pathways in GC.
Keywords: human epidermal growth factor receptor 2, RAB1A, gastric cancer, prognostic factors
Introduction
Being one of the most common malignancies, gastric cancer (GC) has a high incidence and mortality worldwide (1). The most common histological subtype of GC is gastric adenocarcinoma (GAC). Despite great advancements in the diagnosis and therapy of GC in the past decades, the overall survival (OS) rate of patients with this disease is still poor. According to a survey, the 5-year survival rate of GC patients is very poor, with a rate of no more than 35% (2,3). In recent years, numerous studies on molecular targeted therapy and associated molecular pathways involved in the gastric carcinogenesis have shed light on the pathogenesis of GC and enabled the improvement of GC patient prognosis (4). Consequently, detailed and systematic analysis of the biomarkers involved in GC is important for the development of biomarker-driven targeted treatment. Our study has emerged from this perspective.
Human epidermal growth factor receptor 2 (HER-2/ERBB2/neu), a member of the epidermal growth factor receptor family of receptor tyrosine kinases, is known as one of the most important biomarkers in breast cancer (5). For patients undergoing targeted therapy, HER-2 expression is used as a biomarker for identifying subgroups that are likely to achieve a survival benefit from trastuzumab therapy (6). Unfortunately, trastuzumab resistance is universally observed in both breast cancer and GC. Moreover, the expression pattern and prognostic significance of HER-2 in GC remain controversial. The rate of HER-2 overexpression varies across the literature, ranging from 4.4 to 53.4%, with a mean of 17.9% (7). Consequently, increasing studies have focused on the molecular mechanisms underlying advanced trastuzumab resistance in GC patients. Although many studies have reported that activated HER-2 signalling can enhance the capability of cancer cells to migrate and colonize distant sites by phosphorylating pivotal downstream small molecules and signalling pathway effectors (8,9), the definitive relationship between HER-2 and the mTOR signalling pathway has not yet been reported. Here, for the first time, we have demonstrated the expression pattern and clinical significance of the HER-2 signalling pathway downstream small molecule RAB1A.
The RAB1A protein is a small GTP-binding protein that is involved in membrane vesicular transport between the Golgi complex and the endoplasmic reticulum (10). Previous studies have reported that RAB1A is dysregulated in cancers such as tongue cancer (11) and that it is indicative of unfavourable survival in patients. In recent years, studies have demonstrated that RAB1A is a mTORC1 activator in colorectal cancer (12) and a deregulator of the phosphoinositide 3-kinase/protein kinase B/mammalian target of rapamycin complex 1 (PI3K/AKT/mTORC1) pathway in breast cancer (13). Meanwhile, another study indicated that RAB1A interacts with other factors to regulate the initiation of autophagy (14). These findings indicate that RAB1A plays an important role in tumour initiation and progression and is involve in the pathogenesis of cancer. Thus, in the present study, we aimed to examine the expression pattern of RAB1A and its clinical significance and association with HER-2 expression in GC.
To date, little is known regarding the relation between HER-2 and RAB1A expression and its prognostic significance in human GC. Therefore, the aim of this study was to investigate HER-2 and RAB1A expression in GC patient samples and to determine the prognostic significance of and the correlation between the two biomarkers, which may shed light on the mechanisms associated with HER-2 resistance during targeted therapy.
Materials and methods
Patients and clinicopathological information
In this study, we included a total of 280 formalin-fixed paraffin-embedded primary GC specimens and paired noncancerous tissues from patients diagnosed with primary GAC in Nanfang Hospital between 2006 and 2009. In addition, we included 120 cases of GAC tissues preserved in −80°C ultra-low temperature refrigerator in Nanfang Hospital between 2015 and 2016. All included patients underwent radical operation for GC and had no history of chemotherapy or radiotherapy before surgery. The cases were diagnosed by two pathologists at the Department of Pathology, Nanfang Hospital, Southern Medical University (Guangzhou, China). Information on clinicopathological variables including age, sex, Lauren type, lymph node invasion status, tumour size, recurrence, tumour, node and metastasis (TNM) stage and other factors was collected by reviewing electronic records at Nanfang Hospital. The study was approved by the Ethics Committee of Southern Medical University with informed consent from patients.
Immunohistochemistry (IHC) and evaluation of immunohistochemical staining
To evaluate HER-2 and RAB1A expression, we obtained 3–4 micrometre-thick serial sections from the archived paraffin blocks. Immunohistochemical staining for HER-2 was performed using the HercepTest™ kit (Dako Denmark A/S, Glostrup, Denmark) according to manufacturer's protocols. For RAB1A immunohistochemical staining, dewaxing and blocking nonspecific binding was performed as previously described (15). We used monoclonal antibodies against RAB1A (1:200 dilution; Santa Cruz Biotechnology, Inc., Dallas, TX, USA) as the primary antibody. Following signal development, the specimens were washed, dehydrated in alcohol and mounted with coverslips. RAB1A expression was graded as high expression or low expression according to the cytoplasmic staining intensity and average percentage of positively stained area at ×10 magnification. HER-2 immunohistochemical scoring was performed as follows: No staining or membrane staining in less than 10% of invasive tumour cells, IHC score, 0; weak membrane staining in 10% or more in invasive tumour cells, IHC score, 2+; and moderate to strong complete or basolateral membrane staining in 10% or more of invasive tumour cells, IHC score, 3+. In this study, an IHC score of 3+ for HER-2 was considered positive amplification, and IHC scores of 0 and 1+ for HER-2 were considered negative amplification according previous literature reports (16). For specimens with an IHC score of 2+, we performed fluorescence in situ hybridization (FISH) assay to verify the HER-2 amplification status.
FISH
GC specimens with IHC score of 2+ for HER-2 were further subjected to FISH assay. FISH was performed using a AmoyDx HER-2/neu DNA probe kit (ADx-FHE01; Xiamen, China) according to the manufacturer's protocols. Briefly, neutral formalin fixed and paraffin-embedded sections (3–4 µm-thick) were placed on adherent slides and then baked in an oven overnight at 56°C. After deparaffinization and dehydration at room temperature, the slides were incubated with a pretreatment solution (with sodium thiocyanate) and a protease solution for 15 min and subsequently dehydrated with 70, 85, and 100% alcohol for 5 min each before being air dried. The probe mixture was denatured at 80°C for 5 min, added to each slide and sealed under a small glass cover slip before overnight hybridization at 42°C. Excess probe was washed away using 0.4X sodium saline citrate (SSC)/0.3% Nonidet (NP40) and 2X SSC buffer. After hybridization, nuclei were counterstained with 4′,6-diamidino-2-phenylindole (DAPI). Slides were analysed for hybridization signals on a cell-by-cell basis using a multifiltered fluorescence microscope (Olympus BX51; Olympus Corporation, Tokyo, Japan) and Imstar FISH assay controller software 2.1 vision according to standard procedures. The data were expressed as the ratio of HER-2/neu signal (red) to centromere 17 signal (green), and the scores were evaluated as follows: An expected ratio of 1–1.8, no gene amplification (negative), a ratio of >2.2 or HER-2 signal cluster, HER-2/neu gene amplification (positive), and a ratio of 1.8–2.2, equivocal cases. The presence of polysomy 17 was also recorded in the cells using four spec green signals as moderate polysomy and >4 spec green signals as high polysomy.
RNA extraction and reverse transcription-quantitative polymerase chain reaction (RT-qPCR)
Total RNA was isolated using TRIzol reagent (Invitrogen; Thermo Fisher Scientific, Inc., Waltham, MA, USA). To quantify mRNA expression levels in tissues, the Advantage RT-for-PCR kit (Clontech Laboratories, Inc., Mountainview, CA, USA) was used to synthesize cDNA. SYBR-Green PCR master mix (Applied Biosystems; Thermo Fisher Scientific, Inc., Waltham, MA, USA) was then used for qPCR amplification, followed by detection with an ABI PRISM 7,900 Sequence Detector and analysis with the ABI SDS 2.3 software (Applied Biosystems; Thermo Fisher Scientific, Inc.). GAPDH was used as a reference gene. The PCR primer sequences were as follows: RAB1A forward, 5′-CAGCAGGCCAGGAAAGATT-3′ and reverse, 5′-GGTCAGATCACATTTGTTCCCTA-3′; HER-2 forward, 5′-TGTGACTGCCTGTCCCTACAA-3′ and reverse, 5′-CCAGACCATAGCACACTCGG-3′; and GAPDH forward, 5′-CTCCTCCTGTTCGACAGTCAGC-3′ and reverse, 5′-CCCAATACGACCAAATCCGTT-3′; relative Rab1A and HER-2 expression levels (defined as fold change) were expressed as 2−ΔCT (ΔCT = CTRAB1A - CTGAPDH) and 2−ΔCT (ΔCT = CTHER-2 - CTGAPDH) and then normalized to the relative expression levels detected in control samples. Each sample was tested in triplicate.
Statistical analysis
Statistical analyses were performed using SPSS (version 20.0; SPSS, Inc., Chicago, IL, USA) or GraphPad Prism 5.0 (GraphPad Software, Inc., La Jolla, CA, USA). Categorical data were analysed using Chi-square statistics. Quantitative analysis of the GAC group and the paired adjacent normal gastric tissue group was performed using a paired-samples t-test and was presented as the mean ± standard deviation. The Kaplan-Meier method was used for survival analysis, and comparisons between different subgroups were performed using the log-rank test. Multivariate analysis was carried out by using the Cox proportional hazards model with adjustment for covariates to identify meaningful prognostic indicators that are independently associated with survival. Spearman correlation coefficient analysis was used to detect associations between variables. All statistics were two-sided, and P-values <0.05 were considered to be significant.
Results
RAB1A up-regulation and HER-2 amplification were observed in GAC tissues
To evaluate the protein expression of RAB1A and HER-2 in GAC patients and to analyse the associated clinicopathological characteristics, we detected the localization and expression of HER-2 and RAB1A proteins by IHC and evaluated the relationship of these proteins with clinicopathological features of patients. In total, 280 GAC patients were enrolled in the present study. As shown in Fig. 1, compared to that in adjacent noncancerous tissues, RAB1A was overexpressed in GAC tissues (P<0.001). RAB1A expression was strong in the cytoplasm of tumour cells in most cases and weak in paired normal gastric epithelial cells (Fig. 2). Regarding HER-2 expression, 192 of 280 cases (68.57%) scored 0; 40 cases (14.29%) scored 1+; 19 cases (6.76%) scored 2+; and 29 cases (10.36%) scored 3+. According to previous studies (16), samples with an IHC score of 0 or 1+ did not have HER-2 amplification, whereas samples with an IHC score of 3+ did. For samples with an IHC score of 2+, we used FISH assay to validate the HER-2 amplification status (Fig. 2I-L). Among the 19 tumours with an IHC score of 2+ for HER-2, only 7 showed amplification by FISH assay (36.84%). Overall, 36 cases (12.86%) of positive HER-2 amplification was observed. The relationship between RAB1A and HER-2 expression/amplification level and clinicopathological parameters is summarized in Table I. High RAB1A expression was significantly associated with tumour size (P<0.001), lymph node invasion (P<0.001), recurrence (P<0.001) and TNM stage (P<0.001) and World Health Organisation (WHO) Classification (P=0.040). However, no correlation was observed with age, sex, WHO Classification, Lauren type or Helicobacter pylori infection status. HER-2 positive amplification was closely associated with Lauren type (P<0.001), tumour size (P<0.001) and lymph node invasion. However, no difference was observed regarding the amplification status stratified by age, sex, H. pylori infection status, WHO Classification, recurrence or TNM stage.
Figure 1.
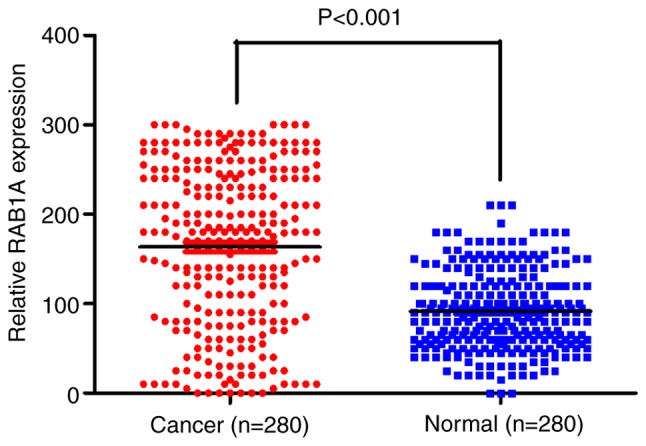
RAB1A protein is overexpressed in GAC tissues as shown by mmunohistochemistry. RAB1A levels in GAC tissues (n=280) and adjacent normal tissues. RAB1A expression was significantly higher in GAC tissues than in adjacent normal tissues (n=280) (P<0.001). CAG, gastric adenocarcinoma.
Figure 2.

Variable expression of RAB1A and HER-2 in human GAC tissue samples. The variable expression of RAB1A and HER-2 in human GAC tissue samples was assayed by (A-H) IHC and (I-L) FISH. (A) Negative membrane staining for HER-2 in GAC epithelium (0+). (B) Weak membrane staining in >10% tumour cells (1+). (C) Moderate complete membrane staining in >10% tumour cells (2+). (D) Strong complete membrane staining in >10% tumour cells (3+). (E) Cytoplasmic staining for RAB1A in normal gastric epithelium (negative). (F) Cytoplasmic staining for RAB1A in tumour cells (weakly positive). (G) Cytoplasmic staining for RAB1A in tumour cells (moderately positive). (H) Cytoplasmic staining for RAB1A in tumour cells (strongly positive). (I and J) FISH assay representing negative HER-2 amplification. (K and L) FISH assay representing positive HER-2 amplification (magnification, ×100). HER-2, human epidermal growth factor receptor 2; CAG, gastric adenocarcinoma; IHC, immunohistochemistry; FISH, fluorescence in situ hybridization.
Table I.
Correlation between clinicopathological parameters and RAB1A expression levels/human epidermal growth factor receptor 2 amplification in 280 patients with gastric cancer.
| HER-2 amplification | RAB1A expression | ||||||
|---|---|---|---|---|---|---|---|
| Clinicopathologic characteristics | n | Positive | Negative | P-value | Positive | Negative | P-value |
| Age (years) | 0.580 | 0.157 | |||||
| ≥60 | 191 | 26 (72.2) | 165 (67.6) | 124 (65.3) | 67 (74.4) | ||
| <60 | 89 | 10 (27.8) | 79 (32.4) | 66 (34.7) | 23 (25.6) | ||
| Sex | 0.290 | 0.329 | |||||
| Female | 108 | 11 (30.6) | 97 (39.8) | 77 (40.5) | 31 (34.4) | ||
| Male | 172 | 25 (69.4) | 147 (60.2) | 113 (59.5) | 59 (65.6) | ||
| Lauren | <0.001a | 0.157 | |||||
| Intestinal | 90 | 27 (75.0) | 63 (25.8) | 60 (31.6) | 30 (33.3) | ||
| Diffuse | 114 | 6 (16.7) | 108 (44.3) | 72 (37.9) | 42 (46.7) | ||
| Mixed | 76 | 3 (8.3) | 73 (29.9) | 58 (30.5) | 18 (20.0) | ||
| Tumor size (cm) | <0.001a | <0.001a | |||||
| ≥5 | 93 | 25 (69.4) | 68 (27.9) | 75 (39.5) | 18 (20.0) | ||
| <5 | 187 | 11 (30.6) | 176 (72.1) | 115 (60.5) | 72 (80.0) | ||
| Lymph node invasion | <0.001a | <0.001a | |||||
| Positive | 81 | 19 (52.8) | 62 (25.4) | 69 (36.3) | 12 (13.3) | ||
| Negative | 199 | 17 (47.2) | 182 (74.6) | 121 (63.7) | 78 (86.7) | ||
| TNM stage | 0.066 | <0.001a | |||||
| I–II | 171 | 27 (75.0) | 144 (59.0) | 137 (72.1) | 34 (37.8) | ||
| III–IV | 109 | 9 (25.0) | 100 (41.0) | 53 (27.9) | 56 (62.2) | ||
| WHO Classification | 0.265 | 0.040a | |||||
| High | 39 | 8 (22.2) | 31 (12.7) | 24 (12.6) | 15 (16.7) | ||
| Medium | 152 | 19 (52.8) | 133 (54.5) | 113 (59.5) | 39 (43.3) | ||
| Low | 89 | 9 (25.0) | 80 (32.8) | 53 (27.9) | 36 (40.0) | ||
| Recurrence | <0.216 | <0.001a | |||||
| Yes | 70 | 12 (33.3) | 58 (23.8) | 60 (31.6) | 10 (11.1) | ||
| No | 210 | 24 (66.7) | 186 (76.2) | 130 (68.4) | 80 (88.9) | ||
| Helicobacter pylori infection | 0.742 | 0.556 | |||||
| Yes | 231 | 29 (80.6) | 202 (82.8) | 155 (81.6) | 76 (84.4) | ||
| No | 49 | 7 (19.4) | 42 (17.2) | 35 (18.4) | 14 (15.6) | ||
P<0.05, Chi-square test and Fisher's exact test. HER-2, human epidermal growth factor receptor 2; TNM, tumour, node and metastasis; WHO, World Health Organisation.
Association of RAB1A but not HER-2 with adverse prognosis in GAC patients
To evaluate the clinical significance of RAB1A and HER-2 overexpression/amplification, we performed survival analyses in these 280 patients. The median level of RAB1A expression was used as a cutoff to divide the 280 patients into two groups. Patients who expressed RAB1A at levels higher than the cutoff value were assigned to the high-expression group, while patients with expression lower than the cutoff value were assigned to the low-expression group. Kaplan-Meier analysis demonstrated that patients with high expression of RAB1A had worse OS than did patients with low expression of RAB1A (P<0.001). However, the Kaplan-Meier curves did not reveal any difference in survival between patients with or without HER-2. Meanwhile, we analysed the co-expression of HER-2 and RAB1A; Kaplan-Meier analysis demonstrated that GAC patients co-expressing both HER-2 and RAB1A had a significantly poorer OS than did GAC patients expressing either HER-2 or RAB1A (P=0.001) (Fig. 3). To evaluate whether RAB1A expression with or without HER-2 amplification is an independent prognostic factor for GAC, we performed univariate and multivariate analyses. Univariate analysis demonstrated that Lauren type (P<0.001), lymph node invasion (P<0.001), recurrence (P<0.001), RAB1A overexpression (P=0.002), WHO Classification (P=0.001), HER-2 amplification (P<0.001) and co-expression of both RAB1A and HER-2 (P<0.001) were significantly associated with OS of GC patients (Table II). However, multivariate analysis using the Cox proportional hazards model for all variables that were significant in univariate analyses showed that only the co-expression of RAB1A and HER-2 was an independent prognostic factor for GAC patients (Table II).
Figure 3.

Kaplan-Meier curves representing OS in GAC patients with RAB1A and HER-2. (A) Kaplan-Meier curves representing OS in GAC patients according to RAB1A expression; the OS duration was shorter in patients with high RAB1A levels than in patients with low RAB1A levels (P<0.001). (B) Kaplan-Meier curves representing OS in GAC patients according to the HER-2 amplification status; the OS duration was not significantly different between the HER-2-positive and HER-2-negative groups (P=0.069). (C) Kaplan-Meier survival curves based on HER-2 amplification and RAB1A expression level. Patients with positive HER-2 amplification and RAB1A expression had a significantly poorer survival than did patients without (P=0.001). OS, overall survival; CAG, gastric adenocarcinoma; HER-2, human epidermal growth factor receptor 2.
Table II.
Univariate and multivariate analyses of various potential prognostic factors in 280 patients with gastric cancer.
| Univariate analysis | Multivariate analysis | |||
|---|---|---|---|---|
| Factor | HR (95% CI) | P-value | HR (95% CI) | P-value |
| Age | 1.152 (0.732–1.811) | 0.541 | – | – |
| Sex | 1.096 (0.730–1.645) | 0.659 | – | – |
| Tumor size | 1.214 (0.800–1.843) | 0.361 | – | – |
| TNM stage | 0.991 (0.663–1.482) | 0.966 | – | – |
| Helicobacter pylori infection | 1.162 (0.681–1.983) | 0.582 | – | – |
| Lauren type | 0.505 (0.383–0.667) | <0.001a | 0.679 (0.445–1.036) | 0.072 |
| Lymph node invasion | 3.184 (2.141–4.736) | <0.001a | 0.743 (0.422–1.307) | 0.302 |
| RAB1A overexpression | 1.938 (1.277–2.943) | 0.002a | 0.932 (0.619–1.442) | 0.669 |
| Recurrence | 2.567 (1.715–3.841) | <0.001a | 0.787 (0.425–1.454) | 0.444 |
| HER-2 amplification | 9.241 (5.973–14.296) | <0.001a | 1.291 (1.081–2.365) | 0.253 |
| WHO classification | 1.687 (1.261–2.258) | 0.001a | 1.400 (0.813–2.413) | 0.225 |
| RAB1A/HER-2 co-expression | 9.241 (5.973–14.296) | <0.001a | 6.662 (3.448–12.871) | <0.001a |
P<0.05. HR, hazard ratio; CI, confidence interval; WHO, World Health Organisation; TNM, tumor, node, metastasis; HER-2, human epidermal growth factor receptor 2.
Positive correlation of RAB1A expression with HER-2 amplification in GAC patients
To confirm whether there was correlation between HER-2 amplification and RAB1A expression in GAC tissues, we analysed the IHC data for RAB1A and HER-2 combined with HER-2 FISH results (Fig. 2). As described in Table III, 47.84% (111/232) of patients with an IHC score of 0 or 1+ had weak staining for RAB1A, and 75.00% (27/36) of patients with an IHC score of 3+ for HER-2 or HER-2 amplification had strong staining for RAB1A. Thus, HER-2 amplification was found to be significantly positively associated with RAB1A expression in GAC tissues (P=0.036). Furthermore, we compared RAB1A and HER-2 mRNA expression in 120 GAC tissues by RT-PCR. The correlation coefficient was 0.053 (P=0.012), and the scatter diagram is shown in Fig. 4. The results of statistical analysis indicated a significant correlation between RAB1A and HER-2 in GAC.
Table III.
Correlation between RAB1A overexpression and HER-2 amplification.
| HER-2 | ||||
|---|---|---|---|---|
| FISH (N) IHC 0+/1+ | FISH (N) IHC 2+ | FISH (A) IHC 3+ | P-value | |
| RAB1A | ||||
| Low expression (n=125) | 111 | 5 | 9 | 0.036a |
| High expression (n=155) | 121 | 7 | 27 | |
| Total | ||||
| 280 | 232 | 12 | 36 | |
P<0.05, Chi-square test. HER-2, human epidermal growth factor receptor 2; FISH, fluorescence in situ hybridization; IHC, immunohistochemistry; N, no amplification; A, amplification.
Figure 4.
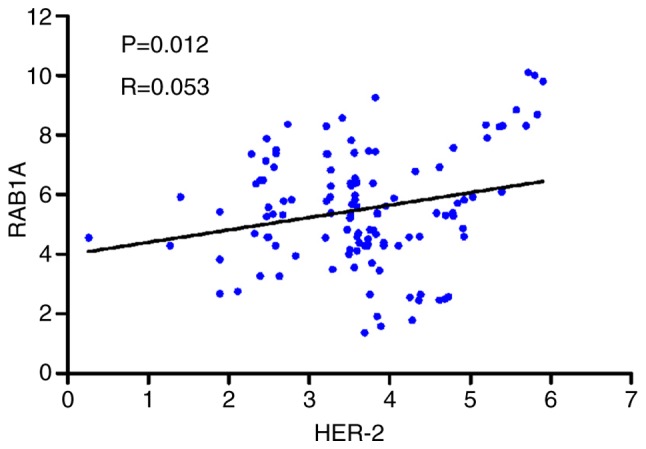
Regression analyses. Regression analyses were performed between HER-2 and RAB1A mRNA expression in GAC tissues, indicating a correlation between relative HER-2 and RAB1A mRNA levels (P=0.012, R=0.053). HER-2, human epidermal growth factor receptor 2; CAG, gastric adenocarcinoma.
Discussion
GC is an important health problem worldwide, and despite the development of various diagnostic and treatment strategies, the morbidity associated with this disease remains high. Traditional methods of diagnostic and treatment strategies are limited in GCs. In recent years, molecular classification based on the HER-2 status and targeted therapies have been introduced for GC because of potential therapeutic implications. However, given that the rate of clustering of positive cells in tissue biopsies is low or at least 10% of positive neoplastic cells in surgical resection specimens are needed for these type of therapies (17), immunohistochemical scoring for HER-2 may not have adequate sensitivity. Thus, further classifications based on molecular alterations are urgently required. Based on this perspective, we conducted this study to evaluate the expression pattern of and correlation between RAB1A and HER-2 and their clinical significance in GAC patients. Previous studies have demonstrated that the HER-2 protein/gene is overexpressed/amplified in various human cancers, including ovarian cancer (18), prostate cancer (19), GC (20), lung cancer (21) and bladder cancer (22) and that HER-2 is an important biomarker for therapeutic assessment for the use of trastuzumab treatment in breast cancer and GC patients. In our study, 12.86% of the patients had HER-2 amplification, but we could not identify any association between HER-2 amplification and adverse prognosis in GAC patients. The reason that HER-2 is not associated with survival might be that the small sample size in our research. According to the literatures, HER-2 overexpression are associated with poor prognosis in GC patients in large-scale population study (23,24). HER-2 amplification was closely associated with Lauren type, tumour size, lymph node invasion and the co-expression of RAB1A and HER-2 indicated worse survival than did the expression of RAB1A and HER-2 alone. Moreover, the co-expression of RAB1A and HER-2 was identified as a prognostic factor in GAC patients. Our results were partially consistent with those of other studies involving GC patients. Variations in the rate of HER-2-positivity and other related factors are reflective of heterogeneous testing modalities and other variables. However, because GC phenotyping is heterogenous and because histopathologic and molecular characteristics in patients can lead to inconsistencies in therapeutic effects, our findings would aid in the identification of molecular signatures for HER-2-associated GAC.
Previous reports have demonstrated that RAB1A regulates the sorting of early endocytic vesicles from the endoplasmic reticulum to the Golgi complex (25) and have implicated RAB1A in Parkinson's disease (26). Additionally, RAB1A has been shown to combine with some small molecules or complexes to regulate cellular ageing and autophagy (27,28). In recent years, evidence on the role of RAB1A in tumours has begun to emerge. RAB1A overexpression has been reported in human tongue cancer (11) and lung cancer (29). In our previous study, RAB1A was identified as an oncogene in colorectal and liver cancer. The overexpression of RAB1A was significantly associated with poor prognosis in colorectal and liver cancer patients. Moreover, RAB1A gene amplification was shown to promote oncogenic transformation and malignant growth by hyperactivating mTORC1 signalling. In the present study, we detected the expression status and analysed the clinical significance of RAB1A and HER-2. RAB1A was found to be overexpressed in GAC tissues, and the high expression of RAB1A was associated with lymph node invasion, TNM stage, tumour size, recurrence and WHO Classification consistent with the role of RAB1A in inducing migration, invasion and metastasis in cancer cells as shown in our earlier study. These results further confirmed the significance of RAB1A in cancer pathogenesis and provided new perspectives for molecular therapy for GC.
The PI3K/Akt/mTOR pathway is one of the main downstream signalling pathways of HER-2. When HER-2 is activated by various factors, it mediates signal transduction through heterodimerization and autophosphorylation of its tyrosine kinases, leading to subsequent activation of downstream pathways, including the PI3K/Akt/mTOR and Ras/Raf/mitogen-activated protein kinase (MAPK) pathways (30). Previous studies in breast cancer have demonstrated that the PI3K/AKT/mTORC1 pathway is activated after adjuvant endocrine therapy (31). These findings prompted us to investigate whether RAB1A is involved in cancer pathogenesis because RAB1A is a direct activator of the mTORC1 pathway and because mTORC1 is a downstream signalling molecule of HER-2. Based on this hypothesis, we analysed RAB1A protein expression and HER-2 amplification in 280 GAC specimens and observed a significant positive correlation between these two factors. Additionally, we compared the mRNA expression of RAB1A and HER-2 in 120 GAC specimens and observed a significant positive correlation between the two biomarkers. Therefore, RAB1A is likely involved in downstream signalling pathways of HER-2 in GAC. Moreover, we confirmed that both HER-2 and RAB1A were overexpressed in GAC patients. Furthermore, the co-expression of HER-2 and RAB1A were found to predict adverse prognosis and could thus be used as an independent prognostic indicator. Moreover, both RAB1A and HER-2 were associated with lymph node invasion and recurrence. In future studies, we intend to detect the expression pattern of mTORC1 and its pivotal downstream molecules, such as 4EBP1 and p70S6K. Also, we intend to verify prognostic value of HER-2 and it's clinical significance in large-scale of GAC patients. Further studies regarding HER-2 and its associated molecular pathways may reveal potential targets for therapeutic intervention, especially for HER-2-targeted therapy-resistant cancers.
In conclusion, for the first time, we assessed the expression levels of RAB1A in GAC tissues and showed that RAB1A expression was significantly higher in GAC tissues than in normal tissues. Overexpression of RAB1A was closely associated with the degree of tumour invasion and metastasis as well as poor prognosis. Meanwhile, the pattern of HER-2 expression observed in our study was similar to that in other studies, and HER-2 overexpression/amplification was not correlated with poor prognosis in GAC patients. Furthermore, the expression of RAB1A was positively correlated with HER-2 amplification, and the co-expression of RAB1A and HER-2 indicated poor OS, suggesting that the two factors likely play a synergistic role in tumour progression, metastasis and angiogenesis. Our results indicate that multiple signalling pathways might determine the prognosis of cancer patients, and these pathways may be potential targets for combined therapeutic intervention, especially in HER-2-targeted therapy-resistant GC patients.
Glossary
Abbreviations
- HER-2
human epidermal growth factor receptor 2
- GC
gastric cancer
- IHC
immunohistochemistry
- FISH
fluorescence in situ hybridization
- OS
overall survival
References
- 1.Global Burden of Disease Cancer Collaboration. Fitzmaurice C, Dicker D, Pain A, Hamavid H, Moradi-Lakeh M, MacIntyre MF, Allen C, Hansen G, Woodbrook R, et al. The global burden of cancer 2013. JAMA Oncol. 2015;1:505–527. doi: 10.1001/jamaoncol.2015.0735. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Chon SH, Berlth F, Plum PS, Herbold T, Alakus H, Kleinert R, Moenig SP, Bruns CJ, Hoelscher AH, Meyer HJ. Gastric cancer treatment in the world: Germany. Transl Gastroenterol Hepatol. 2017;2:53. doi: 10.21037/tgh.2017.05.07. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Song Z, Wu Y, Yang J, Yang D, Fang X. Progress in the treatment of advanced gastric cancer. Tumour Biol. 2017;39:1010428317714626. doi: 10.1177/1010428317714626. [DOI] [PubMed] [Google Scholar]
- 4.Jou E, Rajdev L. Current and emerging therapies in unresectable and recurrent gastric cancer. World J Gastroenterol. 2016;22:4812–4823. doi: 10.3748/wjg.v22.i20.4812. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Tong ZJ, Shi NY, Zhang ZJ, Yuan XD, Hong XM. Expression and prognostic value of HER-2/neu in primary breast cancer with sentinel lymph node metastasis. Biosci Rep. 2017;37(pii):BSR20170121. doi: 10.1042/BSR20170121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Gajria D, Chandarlapaty S. HER2-amplified breast cancer: Mechanisms of trastuzumab resistance and novel targeted therapies. Expert Rev Anticancer Ther. 2011;11:263–275. doi: 10.1586/era.10.226. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Abrahao-Machado LF, Scapulatempo-Neto C. HER2 testing in gastric cancer: An update. World J Gastroenterol. 2016;22:4619–4625. doi: 10.3748/wjg.v22.i19.4619. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Hashimoto K, Tsuda H, Koizumi F, Shimizu C, Yonemori K, Ando M, Kodaira M, Yunokawa M, Fujiwara Y, Tamura K. Activated PI3K/AKT and MAPK pathways are potential good prognostic markers in node-positive, triple-negative breast cancer. Ann Oncol. 2014;25:1973–1979. doi: 10.1093/annonc/mdu247. [DOI] [PubMed] [Google Scholar]
- 9.Shan X, Wen W, Zhu D, Yan T, Cheng W, Huang Z, Zhang L, Zhang H, Wang T, Zhu W, et al. miR 1296-5p inhibits the migration and invasion of gastric cancer cells by repressing ERBB2 expression. PLoS One. 2017;12:e0170298. doi: 10.1371/journal.pone.0170298. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Mukhopadhyay A, Nieves E, Che FY, Wang J, Jin L, Murray JW, Gordon K, Angeletti RH, Wolkoff AW. Proteomic analysis of endocytic vesicles: Rab1a regulates motility of early endocytic vesicles. J Cell Sci. 2011;124:765–775. doi: 10.1242/jcs.079020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Shimada K, Uzawa K, Kato M, Endo Y, Shiiba M, Bukawa H, Yokoe H, Seki N, Tanzawa H. Aberrant expression of RAB1A in human tongue cancer. Br J Cancer. 2005;92:1915–1921. doi: 10.1038/sj.bjc.6602594. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Thomas JD, Zhang YJ, Wei YH, Cho JH, Morris LE, Wang HY, Zheng XF. Rab1A is an mTORC1 activator and a colorectal oncogene. Cancer Cell. 2014;26:754–769. doi: 10.1016/j.ccell.2014.09.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Davis NM, Sokolosky M, Stadelman K, Abrams SL, Libra M, Candido S, Nicoletti F, Polesel J, Maestro R, D'Assoro A, et al. Deregulation of the EGFR/PI3K/PTEN/Akt/mTORC1 pathway in breast cancer: Possibilities for therapeutic intervention. Oncotarget. 2014;5:4603–4650. doi: 10.18632/oncotarget.2209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Webster CP, Smith EF, Bauer CS, Moller A, Hautbergue GM, Ferraiuolo L, Myszczynska MA, Higginbottom A, Walsh MJ, Whitworth AJ, et al. The C9orf72 protein interacts with Rab1a and the ULK1 complex to regulate initiation of autophagy. EMBO J. 2016;35:1656–1676. doi: 10.15252/embj.201694401. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Xu BH, Li XX, Yang Y, Zhang MY, Rao HL, Wang HY, Zheng XF. Aberrant amino acid signaling promotes growth and metastasis of hepatocellular carcinomas through Rab1A dependent activation of mTORC1 by Rab1A. Oncotarget. 2015;6:20813–20828. doi: 10.18632/oncotarget.5175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Hofmann M, Stoss O, Shi D, Büttner R, van de Vijver M, Kim W, Ochiai A, Rüschoff J, Henkel T. Assessment of a HER2 scoring system for gastric cancer: Results from a validation study. Histopathology. 2008;52:797–805. doi: 10.1111/j.1365-2559.2008.03028.x. [DOI] [PubMed] [Google Scholar]
- 17.Van Cutsem E, Sagaert X, Topal B, Haustermans K, Prenen H. Gastric cancer. Lancet. 2016;388:2654–2664. doi: 10.1016/S0140-6736(16)30354-3. [DOI] [PubMed] [Google Scholar]
- 18.Ouyang W, Xu L, Huang Z, Guo J, Cai J, Gao X, Wang Z. Role of HER family members in predicting prognoses in epithelial ovarian cancer: A meta-analysis. Tumori. 2015;101:595–602. doi: 10.5301/tj.5000343. [DOI] [PubMed] [Google Scholar]
- 19.Murray NP, Reyes E, Fuentealba C, Jacob O, Orellana N. Possible role of HER-2 in the progression of prostate cancer from primary tumor to androgen independence. Asian Pac J Cancer Prev. 2015;16:6615–6619. doi: 10.7314/APJCP.2015.16.15.6615. [DOI] [PubMed] [Google Scholar]
- 20.Lordick F, Al-Batran SE, Dietel M, Gaiser T, Hofheinz RD, Kirchner T, Kreipe HH, Lorenzen S, Möhler M, Quaas A, et al. HER2 testing in gastric cancer: Results of a German expert meeting. J Cancer Res Clin Oncol. 2017;143:835–841. doi: 10.1007/s00432-017-2374-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Kim EK, Kim KA, Lee CY, Shim HS. The frequency and clinical impact of HER2 alterations in lung adenocarcinoma. PLoS One. 2017;12:e0171280. doi: 10.1371/journal.pone.0171280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Cormio L, Sanguedolce F, Cormio A, Massenio P, Pedicillo MC, Cagiano S, Calò G, Pagliarulo V, Carrieri G, Bufo P. Human epidermal growth factor receptor 2 expression is more important than Bacillus Calmette Guerin treatment in predicting the outcome of T1G3 bladder cancer. Oncotarget. 2017;8:25433–25441. doi: 10.18632/oncotarget.15989. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Kurokawa Y, Matsuura N, Kimura Y, Adachi S, Fujita J, Imamura H, Kobayashi K, Yokoyama Y, Shaker MN, Takiguchi S, et al. Multicenter large-scale study of prognostic impact of HER2 expression in patients with resectable gastric cancer. Gastric Cancer. 2015;18:691–697. doi: 10.1007/s10120-014-0430-7. [DOI] [PubMed] [Google Scholar]
- 24.Lei YY, Huang JY, Zhao QR, Jiang N, Xu HM, Wang ZN, Li HQ, Zhang SB, Sun Z. The clinicopathological parameters and prognostic significance of HER2 expression in gastric cancer patients: A meta-analysis of literature. World J Surg Oncol. 2017;15:68. doi: 10.1186/s12957-017-1132-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Hutagalung AH, Novick PJ. Role of Rab GTPases in membrane traffic and cell physiology. Physiol Rev. 2011;91:119–149. doi: 10.1152/physrev.00059.2009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Winslow AR, Chen CW, Corrochano S, Acevedo-Arozena A, Gordon DE, Peden AA, Lichtenberg M, Menzies FM, Ravikumar B, Imarisio S, et al. α-synuclein impairs macroautophagy: Implications for Parkinson's disease. J Cell Biol. 2010;190:1023–1037. doi: 10.1083/jcb.201003122. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Liu X, Fu B, Chen D, Hong Q, Cui J, Li J, Bai X, Chen X. miR-184 and miR-150 promote renal glomerular mesangial cell aging by targeting Rab1a and Rab31. Exp Cell Res. 2015;336:192–203. doi: 10.1016/j.yexcr.2015.07.006. [DOI] [PubMed] [Google Scholar]
- 28.Ramírez-Peinado S, Ignashkova TI, van Raam BJ, Baumann J, Sennott EL, Gendarme M, Lindemann RK, Starnbach MN, Reiling JH. TRAPPC13 modulates autophagy and the response to Golgi stress. J Cell Sci. 2017;130:2251–2265. doi: 10.1242/jcs.199521. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Wang X, Liu F, Qin X, Huang T, Huang B, Zhang Y, Jiang B. Expression of Rab1A is upregulated in human lung cancer and associated with tumor size and T stage. Aging (Albany NY) 2016;8:2790–2798. doi: 10.18632/aging.101087. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Wilks ST. Potential of overcoming resistance to HER2-targeted therapies through the PI3K/Akt/mTOR pathway. Breast. 2015;24:548–555. doi: 10.1016/j.breast.2015.06.002. [DOI] [PubMed] [Google Scholar]
- 31.Beelen K, Hoefnagel LD, Opdam M, Wesseling J, Sanders J, Vincent AD, van Diest PJ, Linn SC. PI3K/AKT/mTOR pathway activation in primary and corresponding metastatic breast tumors after adjuvant endocrine therapy. Int J Cancer. 2014;135:1257–1263. doi: 10.1002/ijc.28769. [DOI] [PMC free article] [PubMed] [Google Scholar]