

Abstract
Over the past four decades, psychiatric social workers have been conducting group interventions for persons with substance use disorders at NIMHANS. In this article, the authors highlight the brief history of group therapy, differences between group therapy and group work, and purpose and indicators of group therapy. This article sheds light on practical aspects of conducting group interventions for persons with substance use disorders and skills required by the group therapist for conducting the same andbenefits of attending group interventions. Research studies carried out at NIMHANS on group intervention for persons with substance use disorders, assessing group processes, dynamics and outcome of group interventions have been highlighted as well.
Keywords: Group work, Group therapy, substance use, alcohol
Perhaps the most important forces in each person's field are other persons
– Kurt Lewin
INTRODUCTION
Social work treatment is an integral component in the treatment of persons with substance use disorders. Social workers play a prominent role in any given substance abuse treatment centre, along with other multidisciplinary team members.
Group therapy is a form of treatment in which emotionally disturbed persons are placed in a group, guided by one or more therapists for the purpose of helping individuals to bring a change in them. It helps individuals to enhance their social functioning through purposeful group experiences and to cope more effectively with their personal, group or community problems.
Brief History of Group Therapy
Joseph Hersey Pratt is known as father of Group therapy. In 1905, he began his work with a group of eight patients with pulmonary tuberculosis in Greater Boston. He was holding general-care instruction classes for recently discharged tuberculosis patients, for whom no place could be found in the sanatoria. He noticed the impact of this experience on their emotional states and allowed them to discuss their common problems. Pratt reported very positive results from this new type of treatment[1]. This is known to be the first formally organized therapeutic group in literature.
In 1936, application of group therapy was practiced among prison inmates and discharged patients in psychiatric hospitals. This was pioneered by Paul Schilder and Louis Wender[2]. Later, it was extended to persons with neurosis, alcohol dependence and disturbed children. During World War II, group therapy was applied to emotionally disturbed war victims.
Social Group Work Vs Group Therapy
Though group work and group therapy are used interchangeably, there is a difference between both the terms. Group work as a primary method of social work is practiced with normal human beings and persons with minor adjustment problems in non-clinical settings. Group work is considered when primary level of prevention is needed and not as a form of treatment. The group worker acts as an enabler; s/he enables the group members to plan, organize and execute the programme activities. Group work activities help its members for their personal growth and development. Social Group Work is practiced by a trained social work professional who has had adequate field work supervision.
Group therapy is considered one of the promising psychosocial treatment modalities which is practiced in clinical settings for persons with emotional problems or mental health issues by qualified mental health professionals such as psychiatrists, clinical psychologists, psychiatric nurses, psychiatric social workers and occupational therapists specialized in mental health. The group therapist is as active participant of the group and helps its members to understand their individual problems as well as interpersonal problems. Group discussion is focused on the current problems in relation to oneself and others. Group therapy aims to bring about reduction in symptoms such as negative symptoms, poor motivation, as well as improvement in social functioning, better adjustment and improved interpersonal relationship skills.
Assumptions
There are certain universal assumptions that underlie group therapy interventions. These include the following:
Group Experience is Universal
Group Therapy is used to bring about changes in attitude and behaviour
Groups produce change which is more permanent
Groups act as instruments for helping others
Through Groups, people can grow together
It is easy to change people in groups than at the individual level
Purpose of Group Therapy
Group therapies can serve a variety of functions. They can be:
Corrective
Developmental
Educative
Preventive
Recreational
Therapeutic
Contra-indications for Group therapy
While a majority of persons seeking treatment for addictive disorders could benefit from group interventions, the following members may not be suitable for group therapy:
Persons with acute psychotic symptoms
Those with active suicidal thoughts
Organic disorders
Physically unhealthy individuals
Persons with significant Cognitive decline/deficits
Persons with severe Personality disorders
Poorly motivated persons
Group Formation
Certain broad principles underlying group interventions are presented below.
Selection of Individuals: Selection of individuals for group therapy should be based on similarity of the problems.
Number of members: Group therapy may be practised with more than two members and less than 15. Optimum number for group therapy is 8-12 members.
Seating arrangements: There should be enough chairs to accommodate the group members. Particular member chair should be left vacant if he/she is absent. Therapist and patients must have similar chairs.
Frequency of group session: Group Therapy can be conducted once in a week or 3-4 times a day depends upon the needs of the group members and clinical settings. Groups that are conducted on a daily basis may be of 45 minutes duration; group duration may be up to 90 minutes if it is once in a week.
Time Period: Length of the group therapy may be extended for a maximum of 25 sessions or for a maximum period of six months.
Age range: Age range of the group members can be relatively similar; ranging from 25 years to 55 years. There should not be too much age disparity.
Phases of Group Development
In closed groups, the following phases are described:
Forming
Norming
Storming
Performing
Adjourning
Forming
Members became oriented toward each other, work on being accepted, and learn more about the group. This stage is marked by a period of uncertainty in which members try to determine their places in the group and learn the groups' rules and procedures.
Storming
Conflicts begin to arise as member resist the influence of the group and rebel against accomplishing their tasks. Members confront their various differences, and the management of conflict often becomes the focus of attention.
Norming
The group establishes cohesiveness and commitment. In the process, the members discover new ways to work together. Norms are also set for appropriate behaviour.
Performing
The group works as a unit to achieve group goals. Members develop proficiency in achieving goals and become more flexible in their patterns of working together.
Adjourning
The group disbands. The feelings that members experience are similar to “Separation Stage”.
Practical aspects of conducting groups
It is important that members of the group follow some ground rules with respect to group therapy participation.
For the members
Members must be informed about the purpose of group: Purpose is to meet together to discuss their problems.
Discipline: Regularity, Punctuality, Confidentiality. Members should agree to attend the group regularly as per schedule. Group members are advised that issues deliberated in the group not to be discussed after the group session or outside of the group.
For the therapist
There must be two therapists. Participant recordings can be done interchangeably for each session by the therapists.
The Group therapist should have individual session with each member before the therapy starts.
The therapist should be aware of his/her own feelings towards the members of the group (the therapist's experience with other groups such as students, colleagues etc., may affect the interaction with the group).
Therapist role
In a therapist facilitated group interventions, various attributes of the therapist have been described;
Directive approach: S/he has to enable the members to participate in the group intervention process.
Extensional: When a particular aspect comes up, the therapist has to extend the discussion if it is beneficial.
Interpretive: The therapist must be able to provide insight that the members of the group have improved. At the same time, premature interpretation must be avoided
Therapist needs to function as an Enabler and Leader
Therapist has a responsibility to share knowledge/information
Helping to form, develop, participate in order to achieve its objectives
Ability to listen to members' view
Efficient in handling agency schedule
Types of Group
Groups may be Closed or Open Groups depending on whether the same group members continue in a session, or whether any member can join into the group. In addition, groups may be defined as homogenous (members with similar characteristics) or heterogeneous (variable characteristics).
Guidelines for Conducting Group Therapy[3]
Certain broad principles underlie the conduct of group therapy. These include:
Planned Group Formation
Specific Objectives
Purposeful Worker - Group Relationship
Continuous Individualization
Guided group Interaction
Democratic Group self-determination
Flexible Functional Organization
Progressive Programme Experiences
Resource Utilization
Evaluation
Skills required for the Group Therapist[4]
Every group therapist must have the skills to work as a part of clinical setting. She/he must know the hospital needs and must possess a growing awareness of oneself as well as the group. The group therapist skills are most evident while actively engaged in a helping capacity with the group. The basic therapy skills required are summarised below:
-
Skill in establishing purposeful relationships
- The group therapist must be skilful in gaining the acceptance of the group and in relating to the group on a positive professional basis.
- The group therapist must be skilful in helping individuals in the group to accept one another and to join with the group in common pursuits.
-
Skill in analysing the group situation
- The group therapist must be skilful in judging the developmental level of the group to determine what the level is, what the group needs, and how quickly the group can be expected to move. This calls for skills in direct observation of groups as a basis for analysis and judgement.
- The group therapist must be skilful in helping the group to express ideas, work out objectives, clarify immediate goals, and see both its potentialities and limitations as a group.
-
Skills in participating with the group
- The group therapist must be skilful in determining, interpreting, assuming, and modifying his/her own role with the group.
- The group therapist must be skilful in helping group members to participate, to locate leadership among themselves, and to take responsibility for their own activities.
-
Skill in dealing with group feeling
- The group therapist must be skilful in controlling his/her own feelings about the group and must study each new situation with a high degree of objectivity.
- The group therapist must be skilful in helping the groups to release their own feelings, both positive and negative. The therapist must be skilful in helping groups to analyse situations as a part of the working – through of group or intergroup conflicts.
-
Skills in programme development
- The group therapist must be skilful in guiding group thinking so that interests and needs will be revealed and understood.
- The group therapist must be skilful in helping groups to develop programmes which they want as a means through which their needs may be met.
-
Skill in using agency and community resources
- The group therapist must be skilful in locating and then acquainting the group with various helpful resources which can be utilized by them for programme purposes.
- The group therapist must be skilful in helping certain individual members to make use of specialised services by means of referral when they have needs, which cannot be met within the group.
-
Skill in Evaluation
- The group therapist must have skill in recording the development processes that are going on while working with the group.
- The group therapist must be skilful in using group therapy records and in helping the group to review its experiences as a means of improvement.
Group Process/Group Dynamics
In the beginning, members may be dependent on therapist as an authoritative figure. They associate the therapist with magical powers and the ability to solve all their problems.
Various processes occur as the group sessions progress. These include:
Cohesiveness: It is a key element of success to the group. There has to be feeling of identification with the group, feeling of belongingness, willingness to sacrifice personal wishes. Members keep a focus on the main goal, which is to help each other to solve their problem and have warm feelings for each other. The group should not hinder the individual functioning outside. The group should become an end in itself. This means that members should not feel that all the needs are met within group.
Content of the discussion: It is concerned with the current interpersonal problems of daily life and not on the past. It is focused on the current interaction between the members and the therapist; ‘go- round’ technique is used to make everyone express as a particular matter/technique.
Modelling: Patient identifies with therapist and uses the therapist as a role model for more effective functioning. Negative transference of the members is revealed through anger and negative response. Therapist in response has to be kind and calm. This will in turn be an example to the participants to be calm and serene in similar situations. Retaliation is not good. Other members express the feeling of acceptance. They realise that they alone don't have the problems, but others also have similar problems. (universalization). There would be group pressure to alter the individual's behaviour.
Cliques: Therapist must be aware of formation of group cliques
Group bond: An important factor in group process is group bond. It represents the feelings of cohesion that makes for a group. Group bond is exclusively defined as “sense of belonging”. It can be measure a group's effectiveness. However, group bond can also be destructive. Its strength might have been produced by threat or by serious dependence of the members on each other. Group bond, therefore, may be a powerful aspect of the group process in either a constructive or destructive sense.
Other Group dynamics to be considered: Sometimes an individual is in an even less favourable position than isolation. He is rejected by the group and exposed to open hostility. Again, one must search for the reasons before trying to change them
Therapeutic Factors in Group
A variety of therapeutic factors have been described in group therapy processes. These include universality, altruism, cohesion, catharsis, imparting information, imitation and modelling, instilling hope, developing social skills, learning interpersonal skills and support[5,6]. The most favourable factor perceived by persons with SUD in group intervention is catharsis, followed by group cohesiveness and interpersonal learning. Patients who received group intervention for 15 sessions or more had a significantly more favourable outcome rate than those who received other modes of treatment, in terms of lesser relapse rate[7]. Apparently because of therapeutic techniques used in the group such as feedback, reward, accepting them as they are, joining, membership, confidentiality, support, and identification of their needs and problems has the capacity to bond patients in overall treatment process[8].
Assessing Group dynamics and Outcome of Group therapy
There are a few tools available for analysing the group therapy process, group dynamics and interaction among group members. Understanding behaviour of the individual in group therapy is essential. Some of the commonly used scales include the Group Climate Questionnaire, Group Cohesiveness Scale and Group Work Engagement Measure, the Therapeutic Factors Scale, Group Session Rating Scale, Individual Group Member Interpersonal Process Scale, Interpersonal Relation Checklist, Group Emotionality Rating System, The Hill Interaction Matrix, Member – Leader scoring system, The Hostility/Support Scale and SYMLOG, which is a measurement method for assessing norms, roles and others dimensions of a group as a whole[9,10,11,12,13,14,15,16,17].
Research on Group Therapy at NIMHANS
Process of Group therapy
Advice giving, insight giving, support giving, self-revealing, symptom reporting, abreaction, imparting information were frequently observed group process in a group therapy for persons with alcohol dependence syndrome at NIMHANS, Bengaluru[18]
Effectiveness of Group therapy
Group therapy for persons with substance use disorder was significantly effective in reducing number days and quantity of substance use, lesser number of days of family role dysfunction, financial problems, routine family activities, occupational dysfunction. Medium to large effect size was seen in improving all the domains of quality of life, coping behaviour, self-efficacy[19].
Self-Help Group (Alcohol Anonymous) Vs Group Therapy
Therapeutic elements such as remaining abstinent, empathy, advice, using anti-craving medicines were found more useful in De-addiction treatment group whereas in Alcoholic anonymous group acceptance, self-confidence, spirituality, technique like ‘remain sober today’ were more useful. Patients attending Alcoholic anonymous group had longer periods of abstinence and lesser number of relapses due to euphoric mood and external factors than the alcohol dependents attended Group therapy at the De-addiction Centre, NIMHANS. AA group members were more satisfied with their life in terms of neighbourhood and community and financial well-being [20]. These groups however are not strictly comparable, because addiction inpatient facilities get a heterogeneous group of patients at different stages of motivation, whereas people likely to be regular at AA meetings usually represent a group committed to change. Self-Help group may be used as a viable option for effective after care intervention for persons with substance use disorder who are discharged from the addiction treatment centres.
Glimpses of Group Interventions at Centre for Addiction Medicine
Group interventions for substance use disorder at NIMHANS started in 1986. First, it was started for outpatients, later it was extended to in-patients as well at psychiatry ward. The aim of group intervention was to encourage the group members to open and share their experiences with other members and to learn skills to prevent relapse and maintain abstinence. Presently, in-patient setting runs three group interventions in different languages English, Kannada and Tamil in parallel. Sometimes, depending upon the number of patients, group interventions would be conducted in Telugu and Hindi as well.
Kind and Form of group
Group is an open one. Members can join and leave the group according to their admission and discharge timings. Groups are educative in nature. Their opportunity to learn (gain knowledge) is more as compared to their opportunity to express[21].
Group structure
Often, groups are homogenous; each group contains 8-16 members (often-speaking same language) each session lasts for a duration of 45 minutes to an hour.
Group format
In a week, four group sessions were conducted in a week by two psychiatric social workers and a M. Phil Psychiatric Social Work trainees posted in the centre would observe and on few occasions they conducts some group sessions. A group session on recreational activities would be conducted as well once in a week by psychiatric social workers and occupational therapist.
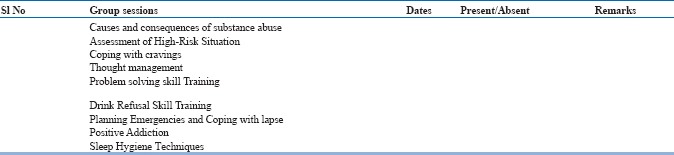
A 12 cycle of sessions on group intervention focuses on
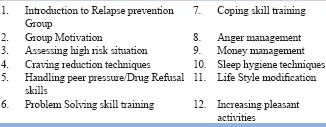
Family Support Group
Apart from the group intervention for persons with substance use disorders, Group sessions were also conducted for their family members once in a week since 2006. The focus is to allow them to ventilate their feelings emotions. In addition, psychiatric social workers educate them about to realize their roles and involvement in recovery process. Family support group would be in multi-lingual as the people from varied culture seek treatment at centre for addiction medicine.
Group Intervention for women
Group intervention for women with substance use disorders commenced in the year 2016, after initiation of separate services for women. Presently, four to eight women used to attend the relapse prevention group interventions. Owing to culture sensitivity and varying treatment needs for women with substance use disorder, a separate relapse prevention group has been initiated. Women recovery group had favourably more reductions in average substance using days, and more satisfaction than mixed gender group intervention. A women-focused same-gender group intervention may enhance longer-term clinical outcomes among women with substance use disorders[22]. Affiliative statements such as supportive, shared experiences, and strategy statements were more in women-focused group intervention than in mixed gender group intervention[23]. Women felt more safe, greater acceptance of different aspects of their self, having their needs met, developing familiarity and confidence, empathy, morality, group cohesion and perceived increased support in women-focused group intervention on gender-relevant topics played an important role in supporting their recovery[24,25]. Women focused groups shown improved treatment satisfaction than mixed gender group treatment. However, both the groups did not differ significantly in terms of reduction in mean number of substance use days [26,27]. This research finding needs to be interpreted with caution. The fact that there is no difference in reduction in number of substance using days does not warrant that women can be placed in mixed gender group intervention.
Out-Patient Recovery Support Group intervention
Recovery support group for recovering persons with substance use disorder have been in place since 2010. It occurs three days in a week during out-patient consultation. Persons who have maintained abstinence for a period of one year have been felicitated during the recovery support group intervention. In NIMHANS, Dr Murthy felt there is a need for such support group for recovering persons and this provides an opportunity for those not treated in an in-patient setting. Recovery support group is usually facilitated by a person who has recovered from substance use disorder and enabled by psychiatric social workers. Recovery support group enables people who abuse substances to witness the recovery of others. It provides useful information to clients regarding new and alternate ways to recovery. Felicitation of recovery provides positive peer reinforcement for recovering persons for sustenance.
CONCLUSION
It was observed that patients who are actively involved and participated in the group intervention are far better in terms of less relapse rate than those who are merely involved in pharmacological and individual intervention. Group intervention and pharmacological intervention are natural allies for the treatment of SUD. One reason why group intervention is effective in treatment of SUD is that people often are more likely to remain abstinent and committed to recovery when treatment is provided in groups and the changes through the group are relatively stable[28].
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
APPENDIX- I: GROUP THERAPY- RECORD SHEET
Name:
Medium of Intervention: Kannada/English/Tamil/others
D.O.A:
P/No:
Duration:
D.O.D:
Signature of the Group Therapist:
APPENDIX 2: SOCIOGRAM AND GROUP THERAPY RECORD
Socio- gram: (diagrammatic representation of group interactions)
Issues brought up for the discussion by the members:
___________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Suggestions given in the group:
_______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Satisfaction in the group:
--------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------
Poor
Good
Very Good
Excellent
Group Processes Observed:

Outcome of the Group Session:

Summary of the Group Process:
(The salient features, the phases and the direction in which the group progressed)
Signature of the Therapist
REFERENCES
- 1.Editorial. Joseph Pratt: The Pioneer. New Engl J Medicine. 1955;253:203–204. [Google Scholar]
- 2.Pinney EL., Jr Paul Schilder and group psychotherapy: the development of psychoanalytic group psychotherapy. Psychiatr Q. 1978 Summer;50(2):133–43. doi: 10.1007/BF01064813. [DOI] [PubMed] [Google Scholar]
- 3.Trecker, Harleigh Bradley. Social group work: principles and practices. New York: Woman's Press; 1948. [Google Scholar]
- 4.Trecker, Harliegh Bradley. Rev. and enl. New York: Whiteside; 1955. Social group work: principles and practices. [Google Scholar]
- 5.Yalom I.D. The theory and practice of group psychotherapy. 3rd ed. New York, NY: Basic Books; 1985. [Google Scholar]
- 6.Brown S, Yalom ID. Interactional group therapy with alcoholics. Journal of Studies on Alcohol. 1977;38(3):426–456. doi: 10.15288/jsa.1977.38.426. [DOI] [PubMed] [Google Scholar]
- 7.Sanaa, et al. Therapeutic Factors in Group Psychotherapy: A Study of Egyptian Drug Addicts. Journal of Groups in Addiction and Recovery. 2010;5:194–213. [Google Scholar]
- 8.Treatment Improvement Protocol (TIP) Series, No. 41. Center for Substance Abuse Treatment. Rockville (MD): Substance Abuse and Mental Health Services Administration (US); 2005. [Google Scholar]
- 9.Corey Marianne Schneider, Corey Gerald, Cindy . 9th edition. New Delhi: Cengage learning India Private Limited; 2014. Group Work Process and Practice. [Google Scholar]
- 10.Garvin Charles D, Gutierrez Lorraine M, et al. India edition. Jaipur: Rawat Publications; 2004. Handbook of Social Work with Groups. [Google Scholar]
- 11.Edwards Suzette Glasner. 1st Edition. Oakland: The Guilford Press; 2010. The Addiction Recovery Skills Workbook. [Google Scholar]
- 12.Hepworth Dean H, Rooney Ronald H, et al. India edition. New Delhi: C engage learning India Private Limited; 2010. Theory and Skills in Social Work. [Google Scholar]
- 13.Nick Kansa. Process and Outcome in Therapy Groups for Substance Abusers. International Journal of Group Psychotherapy. 1999;49(2) [Google Scholar]
- 14.Palmer Sharon Duca. 1st Edition. Oakville: Apple Academic Press Inc; 2011. Social Work in Mental Health and Substance Abuse. [Google Scholar]
- 15.Paylor Ian, Meashan Fiona, et al. Social Work and Drug Use. 1st India (reprint) edition. Jaipur: Rawat Publications; 2013. [Google Scholar]
- 16.Segal Elizabeth A, Gerdes Karen E, et al. 1st India (reprint) edition. New Delhi: Cengage learning India Private Limited; 2010. Professional Social Work. [Google Scholar]
- 17.Sheafor Bradford W, Horejsi Charles J. 9th edition. New Delhi: PHI Learning Pvt Limited; 2011. Techniques and Guidelines for Social Work Practice. [Google Scholar]
- 18.Bhatti R. S. Paper presented at the International Consultation on Christian Response to Alcohol and Drug Addiction, held at ECC. Bangalore, India: 1982. Family Therapy in Alcoholism; pp. 22–27. on November. [Google Scholar]
- 19.Bala Shanthi Nikketha, Muralidhar D, Benegal V. PhD Thesis, Department of Psychiatric Social work. Bengaluru: NIMHANS; 2009. Effectiveness of Group Work Intervention for persons with substance use disorder. [Google Scholar]
- 20.Sujit, Bhatti RS. M.Phil Thesis. Department of Psychiatric social Work. NIMHANS; 2000. Effectiveness of Self-help group for persons with alcohol dependence. [Google Scholar]
- 21.Sinu E, Ushakiran, Bala SN. Social Group work practice in De-addiction centre: An Experience Sharing. Journal of School Social Work. 2005;2(1):30–32. [Google Scholar]
- 22.Greenfield SF, Trucco EM, McHugh RK, Lincoln M, Gallop RJ. The Women's Recovery Group Study: a Stage I trial of women-focused group therapy for substance use disorders versus mixed-gender group drug counseling. Drug Alcohol Depend. 2007 Sep 6;90(1):39–47. doi: 10.1016/j.drugalcdep.2007.02.009. Epub 2007 Apr 18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Sugarman DE, et al. Measuring affiliation in group therapy for substance use disorders in the Women's Recovery Group study: Does it matter whether the group is all-women or mixed-gender? Am J Addict. 2016 Oct;25(7):573–80. doi: 10.1111/ajad.12443. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Greenfield SF, et al. Group Process in the single-gender Women's Recovery Group compared with mixed-gender Group Drug Counseling. J Groups Addict Recover. 2013;8(4) doi: 10.1080/1556035X.2013.836867. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Greenfield SF, et al. A qualitative analysis of women's experiences in single-gender versus mixed-gender substance abuse group therapy. Subst Use Misuse. 2013 Jun;48(9):750–60. doi: 10.3109/10826084.2013.787100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Greenfield SF, et al. Implementing substance abuse group therapy clinical trials in real-world settings: challenges and strategies for participant recruitment and therapist training in the Women's Recovery Group Study. Am J Addict. 2014 May-Jun;23(3):197–204. doi: 10.1111/j.1521-0391.2014.12099.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Greenfield SF, et al. Group therapy for women with substance use disorders: results from the Women's Recovery Group Study. Drug Alcohol Depend. 2014 Sep 1;142:245–53. doi: 10.1016/j.drugalcdep.2014.06.035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Zastrow Charles H. Indian edition. New Delhi: Cengage learning India Private Limited; 2009. Social Work with Groups. [Google Scholar]