

Abstract
The expanding use of digital technology in mental health has widened the scope of emerging addiction interventions. This review focus on the use of technological advances in the field of addiction and mental health. We discuss about how these advances has been implemented in addiction treatment and research. Further, we also mention about the utilisation of these services in India.
Keywords: Digital intervention, Addiction, eHealth
INTRODUCTION
Internet based technologies now provide the capacity to merge the efficacy of evidence based treatments with the advantages of wide reaching interventions1. It allows interactive responses and also face-to-face interactions. In substance use disorders (SUD) management, providing tailored support is often said to play a crucial role2 and technological innovations appear to have an ability to provide such type of interventions3. Also, the motivation of SUD patients fluctuates, which results in difficulty in the initiation of treatment and associated high level of drop out if these patients are not provided timely interventions3,4,5,6.
Around 28% of population in India is actively using the internet with per annum growth of 9% of urban users and 26% of rural India7. The rural growth is estimated to grow 3 times every year. With this drastic growth in the number of internet users, it is the right time to start making use of technology and internet in substance use management services. The use of technology may help us reaching these services to remote rural populations, who might have been deprived of these services, in the absence of technological ventures.
In this article, we aim to summarize the evidence on the use of digital technology, including mobile applications in the treatment and prevention of substance use disorders. We also discuss the Indian perspectives regarding use of digital technology. Further, we discuss how such technological advances could help in overcoming the barriers to improve access to substance use care [Figure 1].
Figure 1.

Image from Raney et al. (2017)8
This figure illustrates the multiple domains across which digital technology in mental health can be used.
Patient facing technology
In the present era, digital technology use involves the use of smartphone applications and emails9,10. Earlier, the use of technology in mental health research involved devices such as alarm watches and beepers to remind about any paper based assessments. This approach was called as the Experience sampling method (ESM) or ecological momentary assessment (EMA)11,12. This type of data collection helped in generating insight about changes in the outcome measures with the daily life activities, parameters which were inaccessible with other research methodologies. Initially, descriptive studies comparing different psychiatric disorders were reported. Later, the focus shifted towards more hypothesis driven studies exploring the nature of specific disorders. Although the initial studies varied in the intensity and duration of these mobile devices used, they demonstrated the uniqueness and utility of this research methodology in mental health research. However, the use of labour intensive paper based methods for collecting outcome related data, limited the utility of EMA. For example, the participants were many a time facing the difficulty in mentioning the accurate timings when the daily reports were completed13. Later, technological advances increased the availability of programmable electronic devices such as smartphones and palmtop computers. These devices made the data collection more feasible and decreased the bias associated with paper based research. For example, the data entry time points were having date and time stamps, which increased the reliability of the EMA.
The research concentrating on the use of technology in addiction research has focused on the relationship between cue exposure and craving for the actual substance use. The advances in technology have also made it possible to provide therapeutic interventions at the time when it is needed. A recently FDA approved app named ‘RESET’, in a 12-week multicentric clinical trial of 507 patients, has shown a significant increase in abstinence rates in substance use disorder patients14. These types of applications include not only providing therapeutic interventions but also measuring the follow-up.
Multiple modalities have been tried in mental health in which patients are directly involved. For the purpose of addiction related research, patients facing technological modalities are directed towards a set of psychosocial interventions, personalised for changing participants' drug-use behaviour. The major motives of these interventions are participants' insight facilitation, motivation, craving management, developing coping strategies and preventing relapses.
Internet based interventions are divided into four categories: i) web-based interventions, ii) online counselling and therapy, iii) artificial intelligence and virtual reality therapeutic software, and iv) other online activities15.
1. Web-based self-help interventions:
These are self-guided programmes providing either basic information and intervention or information only. These type of programmes are executed through a structured website, where the clients can explore the information provided at their own pace. These types of interventions can be subdivided into four types based on how required information is communicated.
A. Information and education based intervention
These type of programmes are structured to enable clients to access the information regarding the specific problem area such as symptoms of specific disorders, diagnostic criteria, causes and treatment strategies15. The aim of such interventions is to provide an easily understandable piece of basic information about addiction and related disorders. These also provide links to other websites with helpful information. These types of interventions do not have an objective of providing therapy, however sometimes they may contain information related to therapy such as method of applying breathing control technique16.
B. Self-guided web based therapeutic interventions
These types of interventions move one step ahead of providing only specific information. They provide a therapeutic feedback in addition to the personalised information provided. In this, initially an elaborate assessment about the particular behaviour would be conducted. Depending on this, a tailored feedback would be provided about the nature of behaviour. Further, this may take ahead to the ways on how the behaviour can be modified. The feedback varies from display of large text or graphics over the screen or an automated sms/email.
Figure 2.
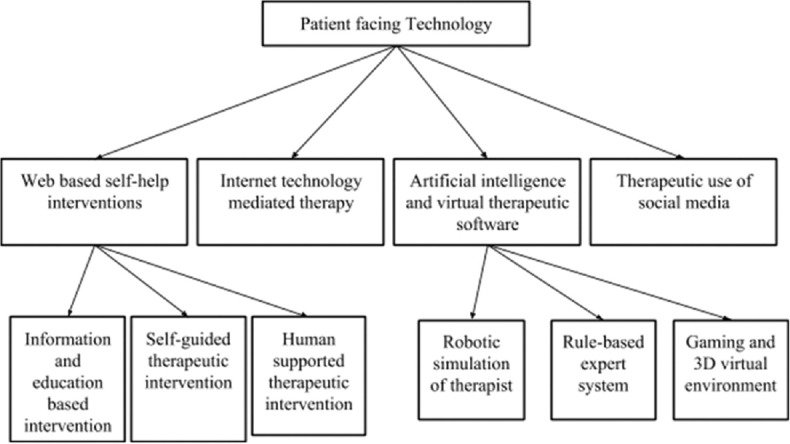
Based on Barak et al. (2009)15. Tree chart of the classification of patient facing technology
One example of this type of intervention is the Down Your Drink website (https://www.downyourdrink.org.uk/17 targeting reduction in alcohol consumption. In this, first the amount and pattern of drinking along with the stage of motivation to decrease or quit alcohol is assessed. This is followed by a personalised feedback on alcohol consumption and the harm associated with it. Later, by adopting a strategy of cognitive behaviour therapy, an interactive therapy is delivered targeting to reduce the alcohol consumption (eg: strategies such as asking of advantages and disadvantages of alcohol consumption, deciding the quit date).
C. Human-supported therapeutic web based intervention
Like the self-guided approaches, this type of intervention also aims for changing behaviour through a designed content. Furthermore, this intervention has an added human contact for providing support, contact or feedback. This is either provided by health/mental health professionals or sometimes by peer supporters. The human support provided in this type of intervention is generally one-to-one by e-mail, instant message or webcam. The variability in this type of interventions is in amount/quantity, frequency, and immediacy of the response, and of human contact. The human contact may vary from couple of minutes to several hours18,19. The frequency also may vary from one to several times a day to once off over the entire intervention. The responses also vary from the immediate ones provided through chat or webcam, or delayed responses through emails.
D. Therapeutic Education System
This is a Web-based psychosocial skills training intervention for individuals with substance use disorders based on the validated community reinforcement approach to behavior change. It has different interactive multimedia modules, starting with basic cognitive behavioural skills (e.g. refusal skills for risk behavior, managing harmful thoughts). Other modules teach skills to improve psychosocial functions (e.g. family and social relations, managing negative moods). The therapeutic education system is self-directed, includes functionality to build individualized treatment plans, assesses a patient's understanding of material, and adjusts the pace and level of repetition of material to promote skills mastery20.
2. Internet technology mediated therapy (Online counseling)
In this method, an individual or a group communicate with the therapist through an online platform. In its inception in mid-1990s, there was a strong resistance to this method of communication for therapy. The subsequent increase in the utility and success stories suggested that this opposition was based on myths, without any basis in reality21. This type of therapy has an advantage of surpassing the distance barrier. The clients can contact a counselor from any distance and at any time, at their convenience. This also shares the advantage of changing the regular office based approach. Clients can get in touch with their therapist from their home or any other locations of their choice. Also, in this modality, writing shares an equal role with the face - to - face interaction.
There are certain disadvantages to this method of counselling. First, the therapist always needs to make sure that the client fits this type of counselling. The clients with extreme pathology and poor digital literacy are not fit for this type of counselling. Second, as most part of therapy is through writing, the nonverbal communication cues such as gestures, body language and voice are missed. Third, clients may find difficult to express their feelings, which is an automatic process in face-to-face relationships. Fourth, the distance barrier makes it difficult to make emergency provisions. Finally, there are many ethical and legal issues related with the online therapy. For these reasons, ethical guidelines are set by many professional associations such as International Society for Mental Health Online.
There are many studies conducted evaluating online therapies in addiction. One of the studies by Woodruff et al.22, has shown its effectiveness in smoking cessation. These types of interventions have also been shown to be beneficial in the after care of clients receiving group therapy23,24,25.
3. Internet operated therapeutic software
These types of intervention are delivered through sophisticated therapeutic software having advanced capacities such as artificial intelligence. They can be broadly divided into 3 types.
Robotic simulation of therapist
These are the type of software where simulations are built in order to provide a dialog-based therapy with patients. These interventions are programmed to detect certain pattern match, conversation rules and simple vocabulary. Previously, the main communication of such software was through text in and text out. The recent development in such software is the use of artificial intelligence. One of these, the Artificial Linguistic Computer Entity programme (A.L.I.C.E.; see http://www.alicebot.org), is built to recognise particular voices and can provide a voice communication rather than the text26. New developments have also shown these applications to have a capacity to detect emotional needs of the users and creating a perception of care and empathy27,28, further improving the compliance29.
Rule-based expert system
These types of systems are used for assessment and treatment selection followed by progress monitoring. A background algorithm would be prepared following certain rules streamlining the process. One of the example for such system used in the addiction treatment is the ‘Drinker's Check-Up’. This system is built to detect level of risk due to alcohol consumption and readiness to change30. With the advent of smartphones, there are many software that are easily accessible, having the basic capacity to calculate commonly used scoring systems such as AUDIT. Such software have shown promising results in terms of promoting behavioural changes31.
Games and virtual 3D systems
Research with the use of virtual “avatars” for treating problems with substance use is increasing. One of the popular example is the use of Second Life (http:/secondlife.com). The programmes are designed so that the person participating is represented by a virtual avatar who could interact in the virtual world which has a background of discussion forums, blogs, news resources, shopping, information exchange, and more. One of the other example for treating substance use is an application named “MindCotine”. In this, a cue exposure therapy is provided through the virtual avatar and the participants are taught how to deal with the craving for smoking, thus preventing relapse.
Another perspective is the use of therapeutic computer or smartphone based games to train the impaired neurocognitive circuits in substance users. The aim of these training games is to repeatedly stimulate certain neuronal circuits by using neuropsychology task principles. For example, there are computer tasks designed to train disinhibition and attention bias in alcohol users. We at our Centre have designed a smartphone game to train inhibitory control in heavy drinkers and alcohol dependent patients. We found the improvement in the neuronal markers of inhibition with short term training using this mobile game. Further, longer trainings with such type of games may help us in developing add-on therapies for treating addiction disorders.
4. Therapeutic use of Social Media
Another type of technology based intervention in substance use disorders involves the use of social media such as personal blogs or twitter or participation in support groups via chat, audio, or webcam communication channels.
A. Building primary care providers (PCP) capacity (Tele-ECHO) Substance use Disorder, in spite of being a public health problem, has a > 80% treatment gap in developing countries like India (mhGAP WHO). Mental Health Gap action programme (mhGAP) of the WHO has recommended adequate and appropriate training of human resources for substance use and other mental health disorders, to make the standard intervention available at community level. Intervention in SUDs relies heavily on health professionals than on technology or equipment. It is also challenging to get the right professionals with the right skills in the right place, providing the best treatment. Studies from across the globe have pointed out that outcomes are better with early identification and intervention as well as when intervention is provided at the community.
Current technology offers an alternative approach in the context of limited human resources in health care and provides a means to reach evidence-based substance use treatment services to unreached populations. Tele-ECHO (Extension of Community Healthcare Outcome)8, a tele-health technology, has the ability to bridge the gap between a tertiary academic medical centre and a community health centre or general health practitioner. Virtual Knowledge Network NIMHANS, in collaboration with Project ECHO (Extension of Health Care Outcomes) has been using the HUB and SPOKEs knowledge-sharing networks in the area of Addiction and Mental health since the last three years. VKN NIMHANS ECHO, led by expert teams of NIMHANS uses multipoint video conferencing to conduct virtual sessions with community non-specialist doctors and other primary health providers. The focus of this weekly session/clinic is on “patient centric learning to understand the complexities”, “following best-practices like algorithms, guidelines along with clinical wisdom for knowledge diffusion”, “using technology to leverage scarce resources” and “web based monitoring for the outcomes”. During this weekly NIMHANS ECHO clinic, the primary healthcare providers like medical officers, counsellor etc., will be present clinical cases and seek clarification regarding standard management from our multidisciplinary team as well as peers who have logged in simultaneously. This guided practice of case management strengthens the confidence and enhances the skills of the practitioner. Patients also get the best treatment in their own community without travelling to a distant, speciality centre situated in big cities32.
The above model was implemented to train health professionals of Bihar for treating alcohol dependence32. Medical officers along with lay counsellors from 12 districts (total 27) of Bihar underwent training for the management of alcohol use disorders at NIMHANS and later joined sessions every 2nd and 4th Wednesday for two hours to discuss the cases from their districts with NIMHANS multidisciplinary experts. Of the 28 doctors and counsellors who attended the onsite training programme, 18 regularly attended the online component and provided feedback at three months. Significant improvements were reported in knowledge, and competence to assess and treat alcohol use disorders. The relative contribution of the online tele-mentoring and handholding component in these improvements was perceived by the participants as 72%. Over three months, 2143 cases were screened across all the centres, of whom 709 (33%) had an AUDIT score greater than 16, indicating harmful use or dependence. The follow up rate was noted to be 49.1%. Only 76 (3%) cases required referral to specialists33.
A similar model of tele-mentoring has been recently conducted for tobacco cessation for the counsellors working at District tobacco cessation centres in the state of Karnataka. The counselors from 16 districts would join virtually (secured multipoint video conference) through their personal smartphones app/laptops on every 2nd and 4th Friday 11:00am to 1:00pm to the Tobacco Cessation Centre of NIMHANS (Hub). They would present the case summaries and ask the NIMHANS experts about the specific management. The NIMHANS expert Hub is advising them about “best practices” to be implemented in specific cases. This is being followed by a didactic lecture as well as sharing of information. After each session, the NIMHANS team sent the recommendation to be implemented for each patient. The number of patients seen by these counselors over the time has doubled. In the beginning of the programme, 401 patients were seen by these counselors and this steadily increased to 769 for these districts by the end of the programme. Similarly, >70% increase in the confidence level of theses counsellors was noted in managing tobacco dependence and they were working like local experts in their community.
This model of tele-mentoring has now been upgraded and also used in the management of all the addictive disorders34.
The PCP joined the fortnightly NIMHANS ECHO sessions from their workplace via internet enabled devices (smartphone app or laptop) and discussed the cases.
B. Virtual Visit/Telepsychiatry
One of the major challenges in addiction mental health treatment is the logistic difficulty to access treatment services. Telepsychiatry is a form of video conferencing by which a specialist at a remote site directly evaluates patients at an originating site. This treatment domain in psychiatry has been present for a decade and also plays a major role by leveraging technology. This method basically uses teleconferencing technology to evaluate patients, establish the doctor patient relationship, as well as facilitate documentation8.
Figure 3.

Hub and Spokes model
Telepsychiatry is either real-time live interaction (synchronous) or as a store forward approach (asynchronous). It helps both the physician and the patients. The capacity of this service to overcome geographical barriers to access services, is a major advantage. This facility has the ability to reach the remotest areas where health care is sparse. Other than this, it saves a lot of money and time spent in traveling and accessing specialist doctors in person. It may not be useful in generating human resources; however, it can be counterproductive sometimes as it may be an extra burden considering the sparse resources and time of the available psychiatrist.
Studies which looked at the feasibility of this methods have shown impressive results35. Also, the outcomes of this approach are comparable with other technological interventions and face to face consultations36,37,38. Studies in Opioid dependence patients on medication assisted treatments have reported that there is no significant difference in the outcomes of patients treated with face to face consultations and through telepsychiatry, implying its potential role in the development of treatment services39. In India, asynchronous telepsychiatry had been seen as a feasible option40. Even though there has been expertise developed as well as research conducted in telepsychiatry in the area of general psychiatry, its applicability in addiction mental health has not been studied. Currently, there is growing interest in increasing the telepsychiatry services in India, but many facets need to be explored41,42.
CONCLUSION
Digital intervention in addiction has arrived and is going to increase further. From the use of simple smartphones to digital sensors and even to machine learning that predicts responses and helps the person choose an intervention, the choices will increase with time. The FDA approval of reSET for prevention of long term relapse is one example. Smartphones, owing to their many data sensors, large screens, and various communication modalities, have emerged as frontrunners in digital intervention.
The ultimate goal of digital technology should be enhancing the engagement between patient and clinician to facilitate the recovery by strengthening the connectedness. There are potential hindrances such as digital trust and transparency, cost and accessibility, interoperability and handling big data to produce best practices, that need to be addressed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Shahab L, McEwen A. Addiction. 11. Vol. 104. Abingdon, England: 2009. Online support for smoking cessation: a systematic review of the literature; pp. 1792–804. Available from: http://www.ncbi.nlm.nih.gov/pubmed/19832783 . [DOI] [PubMed] [Google Scholar]
- 2.Durvasula R, Miller TR. Substance Abuse Treatment in Persons with HIV/AIDS: Challenges in Managing Triple Diagnosis. Behavioral Medicine. 2014;40(2):43–52. doi: 10.1080/08964289.2013.866540. Available from: http://www.tandfonline.com/doi/abs/10.1080/08964289.2013.866540 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.VanDeMark NR, Burrell NR, Lamendola WF, Hoich CA, Berg NP, Medina E. An exploratory study of engagement in a technology-supported substance abuse intervention. Substance abuse treatment, prevention, and policy. 2010;5:10. doi: 10.1186/1747-597X-5-10. Available from: http://www.ncbi.nlm.nih.gov/pubmed/20529338 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Mentha H. Motivational Dialogue: Preparing Addiction Professionals for Motivational Interviewing Practice. Drug and Alcohol Review. 2008;27(5) Available from: http://doi.wiley.com/10.1080/09595230802089958 . [Google Scholar]
- 5.Prochaska JO, Velicer WF, Rossi JS, Goldstein MG, Marcus BH, Rakowski W, et al. Stages of change and decisional balance for 12 problem behaviors. Health Psychology. 1994;13(1) doi: 10.1037//0278-6133.13.1.39. Available from: http://doi.apa.org/getdoi.cfm?doi=10.1037/0278-6133.13.1.39 . [DOI] [PubMed] [Google Scholar]
- 6.Prochaska JO, DiClemente CC, Norcross JC. In search of how people change: Applications to addictive behaviors. American Psychologist. 1992;47(9) doi: 10.1037//0003-066x.47.9.1102. Available from: http://doi.apa.org/getdoi.cfm?doi=10.1037/0003-066X.47.9.1102 . [DOI] [PubMed] [Google Scholar]
- 7.TRAI. India: Telecom Regulatory Authority of India; 2017. The Indian Telecom Services Performance Indicators. [Google Scholar]
- 8.Raney L, Bergman D, Torous J, Hasselberg M. Digitally Driven Integrated Primary Care and Behavioral Health: How Technology Can Expand Access to Effective Treatment. Curr Psychiatry reports. 2017;19(11):86. doi: 10.1007/s11920-017-0838-y. Available from: http://www.ncbi.nlm.nih.gov/pubmed/28965319 . [DOI] [PubMed] [Google Scholar]
- 9.Swendsen J. Contributions of mobile technologies to addiction research. Dialog- Clin Neurosci. 2016;18(2):213–21. doi: 10.31887/DCNS.2016.18.2/jswendsen. Available from: http://www.ncbi.nlm.nih.gov/pubmed/27489461 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Muench F. The Promises and Pitfalls of Digital Technology in Its Application to Alcohol Treatment. Alcohol Res Curr Rev. 2014;36(1):131–42. Available from: http://www.ncbi.nlm.nih.gov/pubmed/26259008 . [PMC free article] [PubMed] [Google Scholar]
- 11.Csikszentmihalyi M, Larson R. Validity and reliability of the Experience-Sampling Method. The Journal of nervous and mental disease. 1987;175(9):526–36. doi: 10.1097/00005053-198709000-00004. Available from: http://www.ncbi.nlm.nih.gov/pubmed/3655778 . [DOI] [PubMed] [Google Scholar]
- 12.Robbins ML, Kubiak T. In: The Handbook of Behavioral Medicine. John Wiley and Sons, Ltd; 2014. Ecological Momentary Assessment in Behavioral Medicine; pp. 429–46. Available from: http://doi.wiley.com/10.1002/9781118453940.ch20 . [Google Scholar]
- 13.Stone AA, Shiffman S, Schwartz JE, Broderick JE, Hufford MR. Patient compliance with paper and electronic diaries. Controlled clinical trials. 2003;24(2):182–99. doi: 10.1016/s0197-2456(02)00320-3. Available from: http://www.ncbi.nlm.nih.gov/pubmed/12689739 . [DOI] [PubMed] [Google Scholar]
- 14.Campbell ANC, Nunes EV, Matthews AG, Stitzer M, Miele GM, Polsky D, et al. Internet-delivered treatment for substance abuse: a multisite randomized controlled trial. The American journal of psychiatry. 2014;171(6):683–90. doi: 10.1176/appi.ajp.2014.13081055. Available from: http://www.ncbi.nlm.nih.gov/pubmed/24700332 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Barak A, Klein B, Proudfoot JG. Defining internet-supported therapeutic interventions. Ann Behav Med Publ Soc Behav Med. 2009;38(1):4–17. doi: 10.1007/s12160-009-9130-7. Available from: http://www.ncbi.nlm.nih.gov/pubmed/19787305 . [DOI] [PubMed] [Google Scholar]
- 16.Griffiths M. Online therapy for addictive behaviors. Cyberpsychology and Behav Impact Internet, Multimed Virtual Real Behav Soc. 2005. Available from: http://www.ncbi.nlm.nih.gov/pubmed/16332166 . [DOI] [PubMed]
- 17.Linke S, Brown A, Wallace P. Down your drink: a web-based intervention for people with excessive alcohol consumption. Alcohol Alcohol. 2004;39(1):29–32. doi: 10.1093/alcalc/agh004. Available from: http://www.ncbi.nlm.nih.gov/pubmed/14691071 . [DOI] [PubMed] [Google Scholar]
- 18.Clarke G, Eubanks D, Reid E, Kelleher C, O’Connor E, DeBar LL, et al. Overcoming Depression on the Internet (ODIN) (2): a randomized trial of a self-help depression skills program with reminders. J Med Internet Res. 2005;7(2):e16. doi: 10.2196/jmir.7.2.e16. Available from: http://www.ncbi.nlm.nih.gov/pubmed/15998607 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Klein B, Richards JC, Austin DW. Efficacy of internet therapy for panic disorder. J Behav Ther Exp Psychiatry. 2006;37(3):213–38. doi: 10.1016/j.jbtep.2005.07.001. Available from: http://www.ncbi.nlm.nih.gov/pubmed/16126161 . [DOI] [PubMed] [Google Scholar]
- 20.Marsch LA. Leveraging Technology to Enhance Addiction Treatment and Recovery. Journal of Addictive Diseases. 2012;31(3):313–8. doi: 10.1080/10550887.2012.694606. Available from: http://www.tandfonline.com/doi/abs/10.1080/10550887.2012.694606 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Fenichel M, Suler J, Barak A, Zelvin E, Jones G, Munro K, et al. Myths and realities of online clinical work. Cyberpsychology and Behav Impact Internet, Multimed Virtual Real Behav Soc. 2002;5(5):481–97. doi: 10.1089/109493102761022904. Available from: http://www.ncbi.nlm.nih.gov/pubmed/12448785 . [DOI] [PubMed] [Google Scholar]
- 22.Woodruff SI, Conway TL, Edwards CC, Elliott SP, Crittenden J. Evaluation of an Internet virtual world chat room for adolescent smoking cessation. Addict Behav. 2007;32(9):1769–86. doi: 10.1016/j.addbeh.2006.12.008. Available from: http://www.ncbi.nlm.nih.gov/pubmed/17250972 . [DOI] [PubMed] [Google Scholar]
- 23.Golkaramnay V, Bauer S, Haug S, Wolf M, Kordy H. The exploration of the effectiveness of group therapy through an Internet chat as aftercare: a controlled naturalistic study. Psychother Psychosom. 2006;76(4):219–25. doi: 10.1159/000101500. Available from: http://www.ncbi.nlm.nih.gov/pubmed/17570960 . [DOI] [PubMed] [Google Scholar]
- 24.Haug S, Sedway J, Kordy H. Group Processes and Process Evaluations in a New Treatment Setting: Inpatient Group Psychotherapy Followed by Internet–Chat Aftercare Groups. Int J Group Psychother. 2008;58(1):35–53. doi: 10.1521/ijgp.2008.58.1.35. Available from: http://www.tandfonline.com/doi/abs/10.1521/ijgp. 2008.58.1.35 . [DOI] [PubMed] [Google Scholar]
- 25.Haug S, Strauss B, Gallas C, Kordy H. New prospects for process research in group therapy: Text-based process variables in psychotherapeutic Internet chat groups. Psychother Res. 2008;18(1):88–96. doi: 10.1080/10503300701368008. Available from: http://www.tandfonline.com/doi/abs/10.1080/10503300701368008 . [DOI] [PubMed] [Google Scholar]
- 26.Tantam D. The machine as psychotherapist: impersonal communication with a machine. Adv Psychiatr Treat. 2006;12(6) Available from: http://apt.rcpsych.org/cgi/doi/10.1192/apt. 12.6.416 . [Google Scholar]
- 27.Massaro DW, Cohen MM, Daniel S, Cole RA. In: Human Performance and Ergonomics. Elsevier; 1998. Developing and Evaluating conversational Agents; pp. 173–94. Available from: http://linkinghub.elsevier.com/retrieve/pii/B9780123227355500087 . [Google Scholar]
- 28.Bartneck C. In: CHI ’01 extended abstracts on Human factors in computing systems. CHI ’01. ACM Press; 2000. Affective expressions of machines; p. 189. Available from: http://portal.acm.org/citation.cfm?doid=634067.634181 . [Google Scholar]
- 29.Bickmore TW, Picard RW. Establishing and maintaining long-term human-computer relationships. ACM Trans Comput Interact. 2005;12(2) Available from: http://portal.acm.org/citation.cfm?doid=1067860.1067867 . [Google Scholar]
- 30.Squires DD, Hester RK. Using technical innovations in clinical practice: the Drinker's Check-Up software program. J Clin Psychol. 2004;60(2):159–69. doi: 10.1002/jclp.10242. Available from: http://www.ncbi.nlm.nih.gov/pubmed/14724923 . [DOI] [PubMed] [Google Scholar]
- 31.Meredith SE, Alessi SM, Petry NM. Smartphone applications to reduce alcohol consumption and help patients with alcohol use disorder: a state-of-the-art review. Adv Health care Technol. 2015;1:47–54. doi: 10.2147/AHCT.S65791. Available from: http://www.ncbi.nlm.nih.gov/pubmed/27478863 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Sagi MR, Chand P, Narasimha VL, Murthy P, Mamatha M, Karthick C, et al. In: 2017 5th National Conference on E-Learning and E-Learning Technologies (ELELTECH) IEEE; A pilot from the virtual knowledge network (VKN) nimhans ECHO; pp. 1–6. Available from: http://ieeexplore.ieee.org/document/8075000 . [Google Scholar]
- 33.Chand P, Kandasamy A, S L, S M, R L, N K, et al. Virtual Knowledge Network NIMHANS ECHO: Innovative Tele-Mentoring model for skilled capacity building in mental health and addiction. In: The 7th International Conference on Transforming Healthcare with Information Technology. India: Journal of International society of telemedicine and eHealth. 2016 [Google Scholar]
- 34.Komaromy M, Duhigg D, Metcalf A, Carlson C, Kalishman S, Hayes L, et al. Project ECHO (Extension for Community Healthcare Outcomes): A new model for educating primary care providers about treatment of substance use disorders. Substance Abuse. 2016;37(1):20–4. doi: 10.1080/08897077.2015.1129388. Available from: http://www.tandfonline.com/doi/abs/10.1080/08897077.2015.1129388 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Yellowlees PM, Odor A, Parish MB, Iosif A-M, Haught K, Hilty D. A Feasibility Study of the Use of Asynchronous Telepsychiatry for Psychiatric Consultations. Psychiatric Services. 2010;61(8) doi: 10.1176/ps.2010.61.8.838. Available from: http://psychiatryonline.org/doi/abs/10.1176/ps. 2010.61.8.838 . [DOI] [PubMed] [Google Scholar]
- 36.Hilty DM, Ferrer DC, Parish MB, Johnston B, Callahan EJ, Yellowlees PM. The effectiveness of telemental health: a 2013 review. Telemedicine journal and e-health: the official journal of the American Telemedicine Association. 2013;19(6):444–54. doi: 10.1089/tmj.2013.0075. Available from: http://www.ncbi.nlm.nih.gov/pubmed/23697504 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Modai I, Jabarin M, Kurs R, Barak P, Hanan I, Kitain L. Cost effectiveness, safety, and satisfaction with video telepsychiatry versus face-to-face care in ambulatory settings. Telemedicine journal and e-health: the official journal of the American Telemedicine Association. 2006;12(5):515–20. doi: 10.1089/tmj.2006.12.515. Available from: http://www.ncbi.nlm.nih.gov/pubmed/17042703 . [DOI] [PubMed] [Google Scholar]
- 38.Siminerio L, Ruppert K, Huber K, Toledo FGS. Telemedicine for Reach, Education, Access, and Treatment (TREAT): linking telemedicine with diabetes self-management education to improve care in rural communities. The Diabetes educator. 2014;40(6):797–805. doi: 10.1177/0145721714551993. Available from: http://www.ncbi.nlm.nih.gov/pubmed/25253624 . [DOI] [PubMed] [Google Scholar]
- 39.Zheng W, Nickasch M, Lander L, Wen S, Xiao M, Marshalek P, et al. Treatment Outcome Comparison Between Telepsychiatry and Face-to-face Buprenorphine Medication-assisted Treatment for Opioid Use Disorder: A 2-Year Retrospective Data Analysis. Journal of addiction medicine. 2017;11(2):138–44. doi: 10.1097/ADM.0000000000000287. Available from: http://www.ncbi.nlm.nih.gov/pubmed/28107210 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Balasinorwala VP, Shah NB, Chatterjee SD, Kale VP, Matcheswalla YA. Asynchronous telepsychiatry in maharashtra, India: study of feasibility and referral pattern. Indian J Psychol Med. 2014;36(3):299–301. doi: 10.4103/0253-7176.135384. Available from: http://www.ncbi.nlm.nih.gov/pubmed/25035555 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Naskar S, Victor R, Das H, Nath K. Telepsychiatry in India-Where Do We Stand? A Comparative Review between Global and Indian Telepsychiatry Programs. Indian J Psychol Med. 2017;39(3):223–42. doi: 10.4103/0253-7176.207329. Available from: http://www.ncbi.nlm.nih.gov/pubmed/28615754 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Math SB, Moirangthem S, Kumar NC. Tele-Psychiatry: After Mars, Can we Reach the Unreached? Indian J Psychol Med. 2015;37(2):120–1. doi: 10.4103/0253-7176.155606. Available from: http://www.ncbi.nlm.nih.gov/pubmed/25969593 . [DOI] [PMC free article] [PubMed] [Google Scholar]