

Abstract
Objective
To characterize cerebrospinal fluid (CSF) YKL-40, a unique biomarker that reflects activation of microglial cells, in acute (AHI) and chronic HIV-1 infection (CHI) and to determine the effect of treatment initiation on levels of this marker.
Design
Cross-sectional study of two groups of HIV-infected participants at baseline and follow-up timepoints.
Methods
AHI (n=33) and CHI (n=34) participants underwent CSF and blood sampling before treatment initiation with combination antiretroviral therapy (cART) and at follow up on cART in a subset of these individuals (6 months in AHI participants [n=24], 1 year in CHI participants [n=10]). Measured parameters were analyzed at each timepoint. Analyses employed Mann-Whitney tests and Spearman correlations.
Results
Baseline median YKL-40 was higher in CHI than AHI (96844 versus 80754 ng/L; p=0.011). Elevations in the CHI group relative to the AHI group persisted at follow-up despite treatment (87414 versus 66130 ng/L; p=0.003). In untreated CHI, YKL-40 correlated with neopterin (r=0.51, p=0.0025), chemokine (CXC-motif) ligand-10 (r=0.44, p=0.011), and neurofilament light chain (r=0.56, p=0.0008) in CSF.
Conclusions
This study is the first to describe the dynamics of CSF YKL-40 in two groups of HIV-infected individuals before and after cART and demonstrates the value of this marker in understanding HIV neuropathogenesis. The results suggest the utility of further exploring the prognostic value of YKL-40, particularly in individuals with early HIV infection or those initiating treatment during CHI.
Background
Even in the age of widely available combination antiretroviral therapy (cART), the burden of neurologic disease in HIV-infected patients is significant and persistent.1,2 Investigations into the neuropathogenesis of HIV-1 in the central nervous system (CNS) demonstrate viral penetration into the cerebrospinal fluid (CSF) during acute infection,3 suggesting the virus could affect long-term neurologic outcomes from early timepoints.
Efforts to understand the pathogenesis of HIV-associated neurologic injury have accelerated as clinicians recognize the failure of cART to completely halt processes affecting cognitive functioning.4 While neurologic injury is not detected in the CSF immediately following infection, it develops in a subset of individuals during the first year5–8 and correlates with neuroinflammation.6 Persistent inflammation fostered by a cytokine milieu generated by activated microglia and astrocytes is hypothesized to lead to neuronal injury.9,10 This suggests that immediate cART initiation could preserve neuronal integrity, while later initiation may lead to incomplete improvement.7 Important questions remain regarding the time course of CNS immune activation with relation to HIV viral dynamics and treatment effects.
Inflammatory cells express the glycoprotein YKL-40 (human chitinase 3-like 1 [CHI3L1]) during differentiation; serum levels are elevated in inflammatory conditions11 and may have prognostic value in malignancies.12 In the CNS, YKL-40 is a marker of microglial activity,12 and efforts to investigate its role in inflammatory processes like multiple sclerosis and Alzheimer’s disease are expanding.13–16 There is interest in the potential of YKL-40 as a marker for the pathogenesis of HIV-related neurologic injury. This is partly due to work in macaques demonstrating that rising CSF concentrations predict SIV-associated encephalitis before symptoms,12 and in humans showing elevated levels in HIV encephalitis.12 Little is known, however, about CSF YKL-40 in acute and chronic HIV infection, or the effects of cART on this marker.
In this study, we characterize CSF YKL-40 levels in two cohorts of HIV-1-infected participants initiating cART at different timepoints in the disease course and correlate this marker with disease progression, neuroinflammation, and neuronal injury.
Methods
Participants were derived from three groups enrolled in studies at the SEARCH-Thailand research program, as previously described.3 Participants in SEARCH 010 (RV254/NCT 00796146) had acute HIV infection (AHI) and participants in SEARCH 011 (NCT 00782808) were treatment-naïve with chronic HIV infection (CHI) and met Thai guidelines for cART initiation (e.g., CD4+ T lymphocyte count <350 cells/uL or symptomatic disease). SEARCH 013 enrolled 18 cognitively normal HIV-uninfected Thai controls. All underwent blood and CSF sampling, neuropsychological testing, and proton-magnetic resonance spectroscopy, as described elsewhere.7
Following baseline assessment, HIV-infected individuals initiated cART, consisting of non-nucleoside reverse-transcriptase inhibitor (NNRTI)-based regimens available in Thailand (typically efavirenz, tenofovir, and emtricitabine or an intensified regimen including raltegravir and maraviroc) in SEARCH 010 and regimens with efavirenz or nevirapine and a nucleoside reverse-transcriptase inhibitor (NRTI) backbone of lamivudine, zidovudine, tenofovir, or stavudine in SEARCH 011.
CSF HIV RNA levels were measured using the Roche Amplicor kit (version 1.5), with lower limit of detection of 50 copies/mL in plasma and 100 copies/mL in CSF, due to sample dilution. Standard CSF parameters were measured at collection. Blood and CSF neopterin, CSF chemokine (CXC-motif) ligand 10 (CXCL10)/interferon gamma-induced protein-10 (IP-10) and CSF chemokine (CC-motif) ligand 2 (CCL2)/monocyte chemotactic protein-1 (MCP-1) were quantified using commercial assays.3 CSF neurofilament light chain (NFL) was measured using a quantitative immunoassay (Uman Diagnostics).7 Proton-MRS and neuropsychological testing procedures have been described.7
CSF YKL-40 levels were measured by solid phase sandwich ELISA (R&D Systems, Inc.) at baseline, 24 weeks, and 96 weeks after cART initiation in the AHI group and at baseline and 48 weeks after initiation in the CHI group.
The primary statistical endpoint was the CSF YKL-40 level before and after cART initiation. We used Mann-Whitney and Kruskal-Wallis tests to compare values between groups. For nonparametric correlations, we used Spearman rank correlation coefficients. We used SPSS (version 24.0) and GraphPad Prism (version 5.0d) to conduct analyses.
All participants provided written informed consent and protocols were approved by the Chulalongkorn Hospital Institutional Review Board and equivalent bodies at collaborating institutions.
Results
Baseline characteristics of participants
CSF was available for the first 33 participants with AHI and 34/61 participants with CHI. The AHI group had a higher proportion of males, and participants with higher CD4+ T lymphocyte counts and higher HIV RNA in the plasma and CSF (Table 1). Participants with CHI were found to have elevated CSF white blood cells, CSF CXCL10/IP-10, and CSF NFL, as described.7 Individuals with AHI were stratified by Fiebig stage;17 11/32 were stage I (35.5%), 2 were stage II (6.25%), 15 were stage III (46.9%), 1 was stage IV (3.1%), and 3 were stage V (9.4%).
Table 1.
Comparison of baseline data at week 0 pre-cART initiation for acute HIV infection, chronic HIV infection, and HIV-uninfected participants. Note that duration of infection for chronic group participants is time since diagnosis, which is subject to recall bias. WBC, white blood cells; CXCL10, chemokine CXC motif ligand 10; IP-10, interferon gamma induced protein 10; cART, combination antiretroviral therapy; NNRTI, non-nucleoside reverse-transcriptase inhibitor; RAL, raltegravir; MVC, miraviroc.
| Acute HIV Infection (n= 33) |
Chronic HIV Infection (n=34) |
HIV-Uninfected (n=18) |
p-value (acute vs chronic) |
|
|---|---|---|---|---|
| Age (years) | 29 (24–37) | 34 (29–36) | 33 (27–39) | 0.150 |
| % Male | 94 | 41 | 50 | < 0.001 |
| CD4 Count (cells/uL) | 401 (318–568) | 228 (146–342) | – | < 0.001 |
| Log Plasma HIV | 5.5 (4.9–6.3) | 4.8 (4.4–5.3) | – | 0.002 |
| Log CSF HIV | 3.1 (1.7–4.3) | 4.1 (3.7–4.8) | – | 0.006 |
| Estimated Time Infected* | 18 (13–24) days | 3.7 (0.9–6.4) years | – | – |
| CSF WBC (cells/uL) | 0 (0–3) | 3 (2–9) | 0 (0–0) | 0.003 |
| CSF CXCL10/IP-10 (pg/mL) | 539 (229–748) | 833 (566–1011) | - | 0.006 |
| CSF Neopterin (nmol/L) | 7.7 (4.7–13.5) | 9.3 (7.0–13.0) | 2.6 (1.9–2.9) | 0.381 |
| CSF Neurofilament (ng/L) | 243 (204–333) | 327 (251–568) | 299 (210–337) | 0.002 |
| Typical cART Regimens | NNRTI-based cART +/− RAL/MVC | NNRTI-based cART | – | – |
At baseline, the untreated CHI group had higher CSF YKL-40 levels compared with the AHI group (median 96844 versus 80754 ng/L; p=0.011; Figure 1a) and HIV-uninfected controls (median 86344; p=0.044). Median CSF YKL-40 levels were similar between AHI and control groups (p=0.80).
Figure 1.
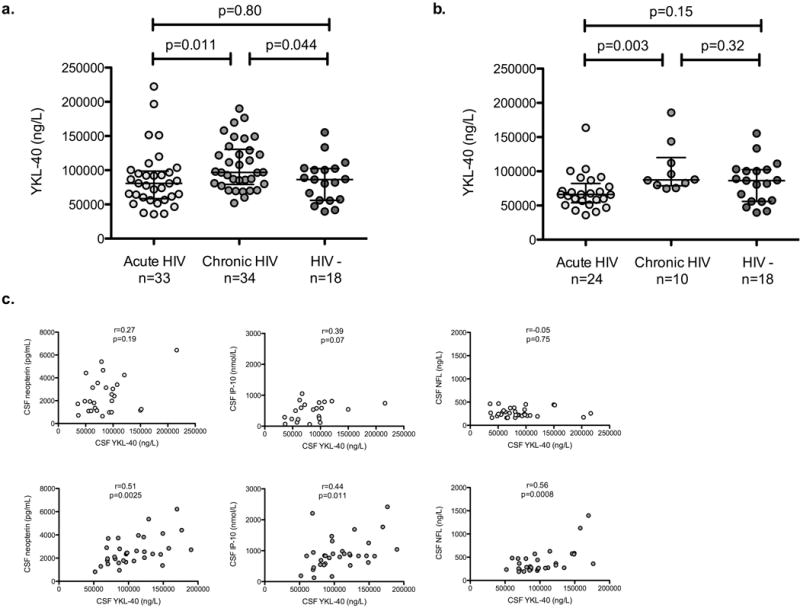
(a) Baseline YKL-40 levels in participants with acute HIV infection (AHI), chronic HIV infection (CHI), and HIV-uninfected controls. (b) Levels of YKL-40 in participants with AHI at 24-week follow-up, CHI at 48-week follow-up, and HIV-uninfected controls. (c) Baseline (pre-treatment) association between CSF YKL and CSF neopterin (left), CSF CXCL10/IP10 (middle), and CSF neurofilament light chain (right) in participants with AHI (top row) and CHI (bottom row).
Characteristics of participants on suppressive cART
At 24-week follow-up, plasma HIV RNA was suppressed in 23/25 (92%) AHI participants; two had low-level viremia (64 and 74 copies/mL). All were suppressed in the CSF. At 48-week follow-up, 10/10 CHI participants had suppressed plasma HIV RNA. One had CSF HIV RNA of 400 copies/mL.
There were decreases in median YKL-40 levels in participants with serial measurements (n=20 in AHI, n=8 in CHI). This trend approached significance in the AHI group (78273 ng/L at baseline versus 66207 ng/L at follow-up; p=0.097). While the median CSF YKL-40 level decreased at 48-week follow-up in the CHI group, no statistically significant difference was detected (102917 ng/L at baseline versus 84738 ng/L at follow-up; p=0.44).
Cross-sectional analysis at follow-up revealed that the median YKL-40 level was higher in CHI compared with AHI (p=0.003; Figure 1b), and there was no difference between the CHI group and HIV-uninfected controls (p=0.32). An analysis limited to “complete cases” (e.g., only participants for which CSF data were available at serial timepoints; n=20 in AHI and n=8 in CHI) revealed that between-group differences in YKL-40 were maintained at follow-up (66207 ng/L in treated AHI versus 84738 ng/L in treated CHI; p=0.01).
Correlates of CSF YKL-40
CSF YKL-40 did not correlate with standard parameters of HIV infection, such as CD4+ T-lymphocyte count, plasma HIV RNA, or CSF HIV RNA, in either group.
At baseline, there was a trend toward correlation between CSF YKL-40 and CXCL10/IP-10 in AHI (Figure 1c). We did not identify correlations between YKL-40 and neopterin, CXCL10/IP-10, and NFL in AHI at 24- or 96-week follow-up.
In CHI participants, CSF YKL-40 correlated with CSF neopterin, CXCL10/IP-10, and NFL before treatment (Figure 1c). We did not identify correlations between YKL-40 and neopterin, CXCL10/IP-10, and NFL at 48-week follow-up.
We identified no correlations between YKL-40 and proton-MRS neuroimaging markers or neuropsychological performance in either group at either timepoint (not shown).
Discussion
CSF YKL-40 is a unique biomarker that reflects activation of microglial cells, the CNS cell type most highly implicated in persistent HIV neuropathogenesis in the current era.9,10 This study is the first to describe the dynamics of CSF YKL-40 in two groups of HIV-infected individuals before and after cART and demonstrates the value of this marker in understanding HIV neuropathogenesis. The results suggest the utility of further exploring the prognostic value of YKL-40, particularly in individuals with early HIV infection or those initiating treatment during CHI.
Our results are consistent with the hypothesis that unchecked HIV replication in the brain results in activation of resident CNS cells such as microglia and astrocytes.18 In CHI prior to cART initiation, CSF YKL-40 correlated with CXCL10/IP-10 and neopterin, both produced by monocytes in response to activated T-cell-derived interferon-gamma. In AHI participants, we noted a trend toward correlation with CXCL10/IP-10 alone. CXCL10/IP-10 was significantly elevated in the CHI group compared with the AHI group.7 Overall, this pattern demonstrates that levels of activated monocytes and T cells in the CNS associate with microglial activation, a key feature of HIV neuropathogenesis.
CSF YKL-40 did not become elevated in AHI participants who immediately initiated cART. In fact, there was a trend toward decreased YKL-40 at 24-weeks compared with baseline. This highlights the anti-inflammatory aspects of cART, suggesting that early initiation could reduce microglial activation and prevent or mitigate downstream neuronal injury.
While CSF concentrations of YKL-40 in CHI appeared to decrease concurrent with cART, this comparison was not significant, although statistical power was limited by sample size. Prior work suggests a role for cART in reducing neuronal injury, which correlated with the inflammatory marker neopterin at the follow-up timepoint.7 YKL-40 remained elevated despite treatment in CHI compared with AHI, suggesting failure to completely halt or reverse neuroinflammation with later cART initiation. This ongoing immune activation likely explains the persistent neuronal injury demonstrated in individuals initiating treatment in CHI,7 and suggests it takes longer than one year to suppress CNS immune activation.
CSF YKL-40 correlated with neopterin in CHI, but not AHI, suggesting that at least in AHI, YKL-40 has biologically distinct origins or is stimulated by distinct mechanisms. Some reports suggest that YKL-40 is additionally a marker of activated astrocytes,16,19,20 suggesting it indicates pathology of a broader range of cells than neopterin. YKL-40 may be valuable in identifying subclinical cognitive impairment15 and neurodegenerative processes earlier than symptoms allow.16 This underscores the value of longitudinal follow-up of these cohorts, especially if early elevations correlate with later neurologic abnormalities.
This study is limited by its sample size and limited longitudinal data. Potential biases include enrolling lower-risk participants or biases related to selection for LP. The groups were similar in age, which correlates with YKL-40 levels;15 gender, which differed between groups, does not have an effect.15 Duration of therapy differed between groups, although evidence suggests neuroinflammation and neuronal injury would have been expected by six months in a subset of the AHI group, had they been untreated.6 Furthermore, YKL-40 did not normalize in the CHI group despite longer duration of therapy, suggesting its persistence is meaningful. Treatment regimens also differed, including 5-agent regimens in some AHI participants. These limitations require conservative interpretation of these data. While there are no established benchmarks for YKL-40 levels in Southeast Asian populations, the HIV-uninfected controls provide a basis for comparison.
We have characterized YKL-40 in the CSF of HIV-infected participants with AHI and CHI compared with relevant controls and demonstrated its elevation in HIV disease. Using this marker, we provide evidence for a benefit of cART in AHI compared with CHI, supporting a mechanism through which early cART confers neuroprotective effects. In the context of work suggesting damage to the immune system occurs early in HIV infection21 and the push to provide immediate cART regardless of CD4 count, our work provides specific information on the mechanism of benefit for early treatment. Finally, given the persistence of HIV-associated neurocognitive disorders despite widespread cART, the association between YKL-40 and NFL7 suggests the value of assessing whether it is possible to identify predispositions to neuronal injury using YKL-40 as a prognostic marker.
Acknowledgments
We thank our study participants and staff from the Thai Red Cross AIDS Research Centre, Chulalongkorn University and AFRIMS for their valuable contributions to this study. We are grateful to the Government Pharmaceutical Organization, Thailand (GPO), ViiV Healthcare, Gilead and Merck for providing the antiretroviral medications for this study. This work is supported by National Institutes of Health grants R01MH095613 (VV and SS), R01NS084911 (JA and SS), R01BS061696 (VV), and a cooperative agreement (W81XWH-07-2-0067) between the Henry M. Jackson Foundation for the Advancement of Military Medicine, Inc, and the U.S. Department of Defense (DoD).
Dr. Valcour reports grants from NIH, personal fees from ViiV Healthcare, personal fees from Merck, during the conduct of the study; personal fees from IAS USA, other from UCSF, outside the submitted work.
Dr. Ananworanich reports grants from US Army; cooperative Agreement No. W81XWH-11-2-0174, personal fees and non-financial support from ViiV Healthcare, personal fees and non-financial support from Merck, personal fees and non-financial support from Tetralogic, outside the submitted work.
Dr. Robb reports grants from Henry M Jackson Foundation, during the conduct of the study.
Dr. Gisslen reports grants and personal fees from Gilead Sciencies, personal fees from Abbvie, personal fees from BMS, personal fees from Janssen-Cilag, outside the submitted work.
Dr. Spudich reports grants from NIH/NIAID/NIMH; cooperative Agreement No. W81XWH-11-2-0174, grants from NIH/NINDS; R01NS084911, grants from NIH/NIMH; R01MH095613, during the conduct of the study.
Footnotes
Conflicts of Interest
Drs Peluso, Krebs, Hellmuth, Zetterberg have no interests to declare.
Disclaimer
The views expressed are those of the authors and should not be construed to represent the positions of the US Army or the Department of Defense.
References
- 1.Heaton RK, Franklin DR, Ellis RJ, et al. HIV-associated neurocognitive disorders before and during the era of combination antiretroviral therapy: differences in rates, nature, and predictors. Journal of neurovirology. 2011 Feb;17(1):3–16. doi: 10.1007/s13365-010-0006-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Sadek JR, Vigil O, Grant I, Heaton RK, Group H The impact of neuropsychological functioning and depressed mood on functional complaints in HIV-1 infection and methamphetamine dependence. Journal of clinical and experimental neuropsychology. 2007 Apr;29(3):266–276. doi: 10.1080/13803390600659384. [DOI] [PubMed] [Google Scholar]
- 3.Valcour V, Chalermchai T, Sailasuta N, et al. Central nervous system viral invasion and inflammation during acute HIV infection. The Journal of infectious diseases. 2012 Jul 15;206(2):275–282. doi: 10.1093/infdis/jis326. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Zayyad Z, Spudich S. Neuropathogenesis of HIV: from initial neuroinvasion to HIV-associated neurocognitive disorder (HAND) Current HIV/AIDS reports. 2015 Mar;12(1):16–24. doi: 10.1007/s11904-014-0255-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Abdulle S, Mellgren A, Brew BJ, et al. CSF neurofilament protein (NFL) – a marker of active HIV-related neurodegeneration. Journal of neurology. 2007 Aug;254(8):1026–1032. doi: 10.1007/s00415-006-0481-8. [DOI] [PubMed] [Google Scholar]
- 6.Peluso MJ, Meyerhoff DJ, Price RW, et al. Cerebrospinal fluid and neuroimaging biomarker abnormalities suggest early neurological injury in a subset of individuals during primary HIV infection. The Journal of infectious diseases. 2013 Jun 1;207(11):1703–1712. doi: 10.1093/infdis/jit088. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Peluso MJ, Valcour V, Ananworanich J, et al. Absence of Cerebrospinal Fluid Signs of Neuronal Injury Before and After Immediate Antiretroviral Therapy in Acute HIV Infection. The Journal of infectious diseases. 2015 May 20; doi: 10.1093/infdis/jiv296. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Jessen Krut J, Mellberg T, Price RW, et al. Biomarker evidence of axonal injury in neuroasymptomatic HIV-1 patients. PloS one. 2014;9(2):e88591. doi: 10.1371/journal.pone.0088591. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Walsh JG, Reinke SN, Mamik MK, et al. Rapid inflammasome activation in microglia contributes to brain disease in HIV/AIDS. Retrovirology. 2014;11:35. doi: 10.1186/1742-4690-11-35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Yadav A, Collman RG. CNS inflammation and macrophage/microglial biology associated with HIV-1 infection. Journal of neuroimmune pharmacology : the official journal of the Society on NeuroImmune Pharmacology. 2009 Dec;4(4):430–447. doi: 10.1007/s11481-009-9174-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Roslind A, Johansen JS. YKL-40: a novel marker shared by chronic inflammation and oncogenic transformation. Methods in molecular biology. 2009;511:159–184. doi: 10.1007/978-1-59745-447-6_7. [DOI] [PubMed] [Google Scholar]
- 12.Bonneh-Barkay D, Bissel SJ, Wang G, et al. YKL-40, a marker of simian immunodeficiency virus encephalitis, modulates the biological activity of basic fibroblast growth factor. The American journal of pathology. 2008 Jul;173(1):130–143. doi: 10.2353/ajpath.2008.080045. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kester MI, Teunissen CE, Sutphen C, et al. Cerebrospinal fluid VILIP-1 and YKL-40, candidate biomarkers to diagnose, predict and monitor Alzheimer’s disease in a memory clinic cohort. Alzheimer’s research & therapy. 2015;7(1):59. doi: 10.1186/s13195-015-0142-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Malmestrom C, Axelsson M, Lycke J, Zetterberg H, Blennow K, Olsson B. CSF levels of YKL-40 are increased in MS and replaces with immunosuppressive treatment. Journal of neuroimmunology. 2014 Apr 15;269(1-2):87–89. doi: 10.1016/j.jneuroim.2014.02.004. [DOI] [PubMed] [Google Scholar]
- 15.Craig-Schapiro R, Perrin RJ, Roe CM, et al. YKL-40: a novel prognostic fluid biomarker for preclinical Alzheimer’s disease. Biological psychiatry. 2010 Nov 15;68(10):903–912. doi: 10.1016/j.biopsych.2010.08.025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Wennstrom M, Surova Y, Hall S, et al. The Inflammatory Marker YKL-40 Is Elevated in Cerebrospinal Fluid from Patients with Alzheimer’s but Not Parkinson’s Disease or Dementia with Lewy Bodies. PloS one. 2015;10(8):e0135458. doi: 10.1371/journal.pone.0135458. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Fiebig EW, Wright DJ, Rawal BD, et al. Dynamics of HIV viremia and antibody seroconversion in plasma donors: implications for diagnosis and staging of primary HIV infection. Aids. 2003 Sep 5;17(13):1871–1879. doi: 10.1097/00002030-200309050-00005. [DOI] [PubMed] [Google Scholar]
- 18.Dunfee RL, Thomas ER, Gorry PR, et al. The HIV Env variant N283 enhances macrophage tropism and is associated with brain infection and dementia. Proceedings of the National Academy of Sciences of the United States of America. 2006 Oct 10;103(41):15160–15165. doi: 10.1073/pnas.0605513103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Bonneh-Barkay D, Zagadailov P, Zou H, et al. YKL-40 expression in traumatic brain injury: an initial analysis. J Neurotrauma. 2010 Jul;27(7):1215–1223. doi: 10.1089/neu.2010.1310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Burman J, Raininko R, Blennow K, et al. YKL-40 is a CSF biomarker of intrathecal inflammation in secondary progressive multiple sclerosis. J Neuroimmunology. 2016;292:52–57. doi: 10.1016/j.jneuroim.2016.01.013. [DOI] [PubMed] [Google Scholar]
- 21.Maduna PH, Dolan M, Kondlo L, et al. Morbidity and mortality according to latest CD4+ cell count among HIV positive individuals in South Africa who enrolled in project Phidisa. PloS one. 2015;10(4):e0121843. doi: 10.1371/journal.pone.0121843. [DOI] [PMC free article] [PubMed] [Google Scholar]