

Abstract
Objective:
Familial adenomatous polyposis (FAP), an autosomal dominant inherited disorder is characterized by the presence of multiple adenomatous colorectal polyps, which can develop into cancer during early adulthood. Therefore, early diagnosis is essential. Most FAP patients have several extracolonic manifestations, including congenital hypertrophy of the retinal pigment epithelium (CHRPE). Whereas genetic markers may provide the main route to detection of “at risk” subjects , at present this approach is clearly limited and searches for a noninvasive phenotypic marker continue to be high priority. The aim of this study was to describe the pattern of distribution of CHRPE lesions and evaluate their diagnostic value in FAP patients and their family members in a local population.
Methods:
A total of 23 FAP patients and 26 relatives belonging to 12 families at high risk of developing FAP were subjected to colonoscopic and ophthalmological examination.
Result:
Retinal examinations demonstrated prevalences of CHRPE in FAP patents and their siblings of 78% and 38%, respectively. We were able to illustrate a significant correlation between FAP disease and the presence of retinal lesions. Sensitivity and specificity of CHRPE as a screening test to detect the presence of FAP are 78.3% and 61.5%, respectively, with a positive predictive value of 64.3% and a negative predictive value of 76.2 %. A “lesion form” significant difference was found between FAP and normal participants. Spearman nonparametric analysis revealed no correlation between age and number or size of lesions.
Conclusion:
Multiple CHRPE lesions are a diagnostic feature of FAP patients They are specific and sensitive clinical markers of this disease (specificity 60% and sensitivity 77%).
Keywords: Congenital hypertrophy of the retinal pigment epithelium, familial adenomatous polyposis, Iran
Introduction
Familial adenomatous polyposis (FAP), an autosomal dominant inherited disorder is characterized by the presence of multiple adenomatous colorectal polyps, which can develop into cancer during early adulthood (Cruz-Correa and Giardiello, 2003). Therefore, early diagnosis and appropriate treatment are essential. Most FAP patients have several extracolonic manifestations including congenital hypertrophy of the retinal pigment epithelium (CHRPE) (Chen et al., 2006 ; Groen et al., 2008; Lynch et al., 2010). CHRPE is a darkly pigmented lesion with a depigmented halo in the retina (Anne and Christine, 1999). The reported prevalence of CHRPE in the general population is 1.25%, which increases its specificity for screening (Nusliha et al., 2014; Coleman and Barnard, 2007). CHRPE screening is relatively easy to perform, can be repeated, is safe, and is a widely accepted method to diagnose FAP. However, it is less commonly preferred for early diagnosis compared to other screening methods (Nusliha et al., 2014).
The APC gene is large in size, comprising 15 coding exons, among which exon 15 alone measures approximately 6.5 kb (Nallamilli and Hegde, 2017).
Detection of CHRPE primarily facilitates identifying mutations using genetic testing. Thus, genetic counseling in combination with an ophthalmic and colonoscopy examination can aid in risk assessment (Katsanos et al., 2003).
The aim of this study was to describe the pattern of distribution of CHRPE lesions and evaluate the diagnostic value of CHRPE lesions in FAP patients and their family members in a local population.
Materials and Methods
The study was approved by the research Ethics Committee of Tabriz University of Medical Sciences (IR.TBZMED.EC.1395.1023).
We studied colonoscopy and pathology reports and hospital records of patients with FAP at the time of their initial registration in local medical referral centers between 2006 and 2016 and drew a pedigree chart based on information obtained from genetic counseling sessions.
Homogeneity with family- The pedigree chart revealed an inherited autosomal dominant pattern in all families affected by FAP.
Patients and relatives at a higher risk of developing FAP were subjected to colonoscopy and ophthalmological examination. Diagnosis of FAP was confirmed based on pathological reports, which revealed more than 100 adenomatous colonic polyps. Inclusion and exclusion criteria used in our study are described in Figure 1.
Figure 1.
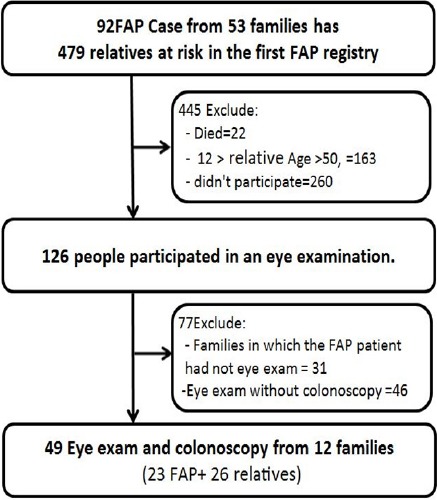
Flowchart of the Inclusion/Exclusion Criteria
Ophthalmic examination: All patients underwent a fundoscopic examination including slit lamp and indirect (90 and 20 diopter lenses, respectively) ophthalmoscopy following dilatation of the pupil using 1% tropic amide. For suspected cases of retinal pigment epithelium and differentiation with other pigmentation, Coherence tomography was used. Color fundus photographs were obtained to document the number and size of CHRPE lesions when possible (Figure 2).
Figure 2.
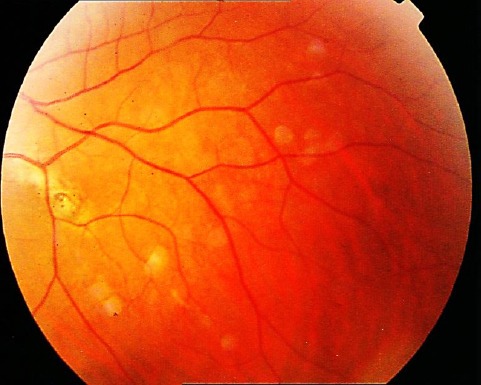
Grouped CHRPE: The Sectorial Pattern of Grouped CHRPE with Smaller and Lager Lesions in the Periphery (OS) with Peripheral Halo Depigmentation.
Statistical analysis: Ophthalmoscope data were analyzed using the chi-square test. Confidence limits were calculated to estimate the possible range for sensitivity, specificity, and predictive values. A p value < 0.05 was considered statistically significant.
Results
A retinal examination was performed on 23 FAP patients and their 26 relatives belonging to 12 families who were at risk of developing FAP. The mean (± SD) ages of participants belonging to the FAP and the high-risk groups were 33 (± 10.6) and 31 (± 8.8) years, respectively.
Patients’ relatives showing high risk of developing FAP revealed no polyps during colonoscopy examination and are undergoing surveillance for colonic polyps. The prevalence of CHRPE in FAP patents and their sibling were 78% (18 of 23) and 38% (10 of 26) respectively. Means (ranges) of the sizes and number (ranges) of CHRPE lesions were 1.4 (0.12-3) disk diameters and 4 (1-13), respectively.
We were able to illustrate a significant correlation between the FAP disease and the presence of retinal lesions (p = 0.005).
Sensitivity and specificity of CHRPE as a screening test to detect the presence of FAP are 78.26% [95% confidence interval (CI) 55.79-91.71] and 61.54% (95% CI 40.73-79.09), respectively.
The positive predictive value is 64.28% (95% CI 44.11-80.69) while the negative predictive value is 76.19 % (95% CI 52.45-90.88).
The Comparison of CHRPE lesion between FAP patients and normal colonoscopy result of their sibling is summarized in Table 1.
Table 1.
The Comparison of CHRPE Lesion between FAP Patients and Normal Colonoscopy Result
| CHRPE ††+: | Variable | colonoscopic findings | Chi-Square | |
|---|---|---|---|---|
| FAP (%) | Normal (%) | P Value | ||
| laterality | Bilateral | 8 (44.4) | 2 (20) | 0.19 |
| Unilateral | 10 (55.6) | 8 (80) | ||
| Lesion form | Multiple | 14 (77.8) | 4 (40) | 0.04 |
| solitary | 4 (22.2) | 6 (60) | ||
| Dominantly Side | Left | 9 (50) | 5 (50) | 0.99 |
| Right | 7 (38.9) | 4 (40) | ||
| Left= Right | 2 (11.1) | 1 (10) | ||
| Size | DD †<1 | 4 (22.2) | 4 (40) | 0.31 |
| DD ≥1 | 14 (77.8) | 6 (60) | ||
, Disc Diameter;
, Congenital Hypertrophy of the Retinal Pigment Epithelium.
No significant differences were noted in laterality, affected eye and size of CHRPE lesions between FAP and normal participants (p>0.05). However, in the case of “lesion form” significant difference was found between two groups (P=0.04). The specificity and sensitivity for this criterion were 60% and 77% respectively.
Spearman nonparametric analysis revealed no correlation between age and number of lesions (R/S = -0.05, P > 0.05) and also between age and size of lesions (R/S = 0.18, P > 0.05).
We didn’t find a significant relationship between the gender and retinal lesion (p = 0.62).
Discussion
The genetic marker to assist the main detection of “at risk” subjects but this technique has clearly limited (Tourino et al., 2004). Diagnosis of FAP is primarily based on evaluation of clinical findings (Jasperson et al., 2017; Aihara et al., 2014). The search for a noninvasive phenotypic marker to facilitate in the prediction of subjects at risk of FAP still continues to be a challenge.
Fundoscopy is used for early diagnosis of family members of FAP patients (Jasperson et al., 2017).
In CHRPE positive family, some FAP patients (22%) were not retinal lesions, so far no hypothesis has been reported theirs.
In this study, the sensitivity of CHRPE was noted to be 78%, which is comparable with findings revealed in other research (Nusliha et al., 2014; Anne et al., 1999). CHRPE occurs in three variant forms: either as solitary or grouped or multiple lesions (Youhnovska et al., 2013; Kurz et al., 1962). We do not have any patients with “grouped” form lesion in the present study. Several studies report that multiple CHRPE associated with FAP, these finding are similar to our study (P < 0.05) (Katsanos et al., 2003; Santos et al., 1994).
In the present study, we showed (Spearman analysis) that in FAP patients with different age groups, the different number and also the size of lesion can be found. We could not find any previous report in this case.
Within each family, we have observed similarity in the retinal lesion phenotypes. This issue is in line with report of earlier study (Tiret et al., 1997). A limitation of our study was that a patient’s relatives who were at risk of developing FAP were assessed using colonoscopic examination and not genetic studies.
In conclusions, multiple CHRPE lesions are one of the diagnostic features of FAP patient. They are specific and sensitive clinical markers of this disease (specificity 60% and sensitivity 77%).
Acknowledgements
This study was funded by a grant from Liver and Gastrointestinal Disease Research Center, Tabriz University of medical sciences.
References
- Aihara H, Kumar N, Thompson CC. Diagnosis, surveillance, and treatment strategies for familial adenomatous polyposis:rationale and update. Eur J Gastroenterol Hepatol. 2014;26:255–62. doi: 10.1097/MEG.0000000000000010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Anne T, Christine P. Fundus lesions of adenomatous polyposis. Curr Opin Ophthalmol. 1999;10:168–72. doi: 10.1097/00055735-199906000-00003. [DOI] [PubMed] [Google Scholar]
- Chen CS, Phillips KD, Grist S, et al. Congenital hypertrophy of the retinal pigment epithelium (CHRPE) in familial colorectal cancer. Familial Cancer. 2006;5:397–404. doi: 10.1007/s10689-006-0011-y. [DOI] [PubMed] [Google Scholar]
- Coleman P, Barnard NA. Congenital hypertrophy of the retinal pigment epithelium:prevalence and ocular features in the optometric population. Ophthalmic Physiol Opt. 2007;27:547–55. doi: 10.1111/j.1475-1313.2007.00513.x. [DOI] [PubMed] [Google Scholar]
- Cruz-Correa M, Giardiello FM. Familial adenomatous polyposis. Gastrointest Endosc. 2003;58:885–94. doi: 10.1016/s0016-5107(03)02336-8. [DOI] [PubMed] [Google Scholar]
- Groen EJ, Roos A, Muntinghe FL, et al. Extra-intestinal manifestations of familial adenomatous polyposis. Ann Surg Oncol. 2008;15:2439–50. doi: 10.1245/s10434-008-9981-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Katsanos KH, Marika Syrrou, Tsianos EV. The value of ophthalmic examinations in familial adenomatous polyposis syndrome screening. Ann Gastroenterol. 2003;16:287–99. [Google Scholar]
- Kurz GH, Zimmerman LE. Vagaries of the retinal pigment epithelium. Int Ophthalmol Clin. 1962;2:441–64. [Google Scholar]
- Lynch HT, Snyder C, Davies JM, et al. FAP, gastric cancer, and genetic counseling featuring children and young adults:a family study and review. Familial Cancer. 2010;9:581–8. doi: 10.1007/s10689-010-9352-7. [DOI] [PubMed] [Google Scholar]
- Nallamilli BR, Hegde M. Detecting mutations in the APC gene in familial adenomatous polyposis (FAP) Curr Protoc Hum Genet. 2017;10:1–16. doi: 10.1002/cphg.29. [DOI] [PubMed] [Google Scholar]
- Nusliha A, Dalpatadu U, Amarasinghe B, Chandrasinghe PC, Deen KI. Congenital hypertrophy of retinal pigment epithelium (CHRPE) in patients with familial adenomatous polyposis (FAP);a polyposis registry experience. BMC Research Notes. 2014;7:734–7. doi: 10.1186/1756-0500-7-734. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Santos A, Morales L, Hernandez-Quintela E, et al. Congenital hypertrophy of the retinal pigment epithelium associated with familial adenomatous polyposis. Retina. 1994;14:6–9. doi: 10.1097/00006982-199401000-00002. [DOI] [PubMed] [Google Scholar]
- Tiret A, Taiel-Satral M, Tiret E, Laroche L. Diagnostic value of fundus examination in familial adenomatous polyposis. Br J Ophthalmol. 1997;81:755–8. doi: 10.1136/bjo.81.9.755. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tourino R, Conde-Freire R, Cabezas-Agricola JM, et al. Value of the congenital hypertrophy of the retinal pigment epithelium in the diagnosis of familial adenomatous polyposis. Int Ophthamol. 2004;25:101–12. doi: 10.1023/b:inte.0000031739.62559.ac. [DOI] [PubMed] [Google Scholar]
- Youhnovska P, Toffoli D, Gauthier D. Congenital hypertrophy of the retinal pigment epithelium complicated by a choroidal neovascular membrane. Dig J Ophthalmol. 2013;19:24–7. doi: 10.5693/djo.02.2013.01.004. [DOI] [PMC free article] [PubMed] [Google Scholar]