

Abstract
Reduction of health disparities and advancement of health equity in the United States require high-quality data indicative of where the nation stands vis-à-vis health equity, as well as proper analytic tools to facilitate accurate interpretation of these data. This article opens with an overview of health equity and social determinants of health. It then proposes a set of recommended practices in measurement of health disparities, health inequities, and social determinants of health at the national level to support the advancement of health equity, highlighting that (1) differences in health and its determinants that are associated with social position are important to assess; (2) social and structural determinants of health should be assessed and multiple levels of measurement should be considered; (3) the rationale for methodological choices made and measures chosen should be made explicit; (4) groups to be compared should be simultaneously classified by multiple social statuses; and (5) stakeholders and their communication needs can often be considered in the selection of analytic methods. Although much is understood about the role of social determinants of health in shaping the health of populations, researchers should continue to advance understanding of the pathways through which they operate on particular health outcomes. There is still much to learn and implement about how to measure health disparities, health inequities, and social determinants of health at the national level, and the challenges of health equity persist. We anticipate that the present discussion will contribute to the laying of a foundation for standard practice in the monitoring of national progress toward achievement of health equity.
Keywords: health disparities, health equity, measurement, monitoring, social determinants of health, surveillance
Since the 1980s, there has been a growing call for nations across the globe to address health inequities, which are systematic, unfair, and avoidable differences in health outcomes and their determinants between segments of the population, such as by socioeconomic status (SES), demographics, or geography.1,2 A seminal paper by Margaret Whitehead3 in 1992 created international urgency for governments and all sectors of society to attend to differences in health that have been found to be associated with social position. Social position can be defined as “relative advantage and disadvantage in social hierarchies.”1(p180) Differences in health associated with social position can be considered unfair because they affect groups of people who are already at a disadvantage.4 In 2005, the World Health Organization (WHO) established the Commission on Social Determinants of Health to draw attention to the conditions of living that underlie inequitable differences in health. Social determinants of health are the “conditions in which people are born, grow, live, work and age. These circumstances are shaped by the distribution of money, power and resources at global, national and local levels.”5 The Commission on Social Determinants of Health’s final report was completed in 2008, and it reported that “within countries, the differences in life chances are dramatic and are seen in all countries—even the richest.”6(preface)
In the United States, a 1985 report by the US Department of Health and Human Services (HHS), the Secretary’s Task Force Report on Black and Minority Health, showed pervasive racial and ethnic differences in health outcomes,7 and this sparked concern nationwide. Decades later, in 2003, the Institute of Medicine report, Unequal Treatment: Confronting Racial and Ethnic Disparities in Healthcare, showed troubling racial and ethnic inequities in health care.8 The socioeconomic gradient of health is also well established in the United States and worldwide. For example, decades of research show a dose-response relationship between educational attainment and health in the United States. That is, the relationship between social advantage and health is incremental—with less advantaged groups experiencing a disproportionate burden of poor health and even relatively advantaged groups showing a deficit.9 Systematic differences in health based on race/ethnicity, sex, gender identity and sexual orientation, SES, age, disability status, geography, and primary language10 (among other characteristics) persist in the United States to the current day. Inasmuch as eliminating these differences—particularly those that are “avoidable or remediable”—remains a public health priority, a focus on health equity is no less timely now than it was in the 1980s. Addressing health equity has also been identified as an ethical imperative. Paula Braveman and Sir Michael Marmot, leaders in the field, have asserted, respectively, that “it is an ethical responsibility and consonant with principles of human rights to give special priority to action on important public-health problems that differentially affect those with fewer resources and/or greater obstacles to addressing problems”11(p185) and “the case is moral—reducing health inequities and improving health is a duty and should be a priority for governments and those with influence to improve health.”12(pS519)
The past several years have been characterized by an increasing focus on solutions (eg, see the reports by Meyer et al10 and Penman-Aguilar et al13). Health in All Policies is a “collaborative approach to improving the health of all people by incorporating health considerations into decision-making across sectors and policy areas.”14 This and other developments such as community-level interventions to address the social determinants of health and health systems changes to reduce health care inequities show promise.15
What is not measured cannot readily be remedied; thus, the provision of accurate and useful data is foundational.16 Many of the examples in this article are drawn from 2 priority national initiatives that provide such information and whose scopes include monitoring health disparities (including inequities) and social determinants of health—Healthy People and CDC (Centers for Disease Control and Prevention) Health Disparities and Inequalities Reports (CHDIRs).
At a national level in the United States, the Healthy People 2020 initiative sets national health objectives with benchmarks and monitors differences across population subgroups to advance the attainment of health equity. At its launch in 2010, Healthy People 2020 identified “achieve health equity, eliminate disparities and improve health of all groups” as one of its 4 overarching goals. The Healthy People 2020 definition of health equity is broader than the definition of inequities provided earlier, and it includes the “attainment of the highest level of health for all people. Achieving health equity requires valuing everyone equally with focused and ongoing societal efforts to address avoidable inequalities, historical and contemporary injustices, and the elimination of health and health care disparities.”17 Healthy People 2020 includes social determinants of health as one of its 12 leading health indicator topics and one of its 42 topic areas, reflecting the importance of conditions of living for health.18
CHDIRs provide “analysis and reporting of recent trends and ongoing variations in health disparities and inequalities for selected social and health indicators.”19 The inaugural CHDIR was published in 2011.20 The most recent CHDIR reported on 29 topics, including 6 that represent social or environmental determinants of health.19
The present discussion lays a foundation of recommended practices in measurement of health disparities, health inequities, and social determinants of health at the national level to support the advancement of health equity. The task is to routinely collect high-quality data indicative of where we stand as a nation, analyze it appropriately, and present it in ways that are meaningful to the broad spectrum of audiences upon whose effort the achievement of health equity depends. Although the article is primarily targeted to researchers interested in national systems for monitoring indicators of health equity (governmental or private), those involved in monitoring indicators of health equity at lower levels of geography (eg, state health departments) should find it useful, as should anyone who seeks to compare populations on specific health outcomes or determinants at national or subnational levels.
Two events led to the development of this article. First, CDC has convened a series of annual forums to engage public health scientists and practitioners in a shared vision of how the agency can contribute to the elimination of health disparities and the advancement of health equity. The 2013 forum focused on measurement and monitoring of health disparities, health inequities, and social determinants of health. On the basis of knowledge of the literature, the authors of this article outlined key principles of measurement in advance of this forum. These principles framed the presentations and question and answer sessions at the forum. A second pertinent event was the recent adoption by the Advisory Committee to the CDC Director (a group of external advisors) of a set of recommendations proposed by the Health Disparities Subcommittee of the Advisory Committee to the CDC Director (HDS). One of these recommendations was that CDC identify and monitor indicators of health equity. The CHDIRs have been CDC’s primary mechanism for reporting on national-level health equity–related indicators. Notably, the HDS commented on the need for greater attention to within-group heterogeneity in the CHDIRs, and attending to this heterogeneity is an emphasis of this article. Considering how one might adapt CDC’s reporting to address the HDS recommendation required a careful review of the literature. To this end, the lead author reviewed literature on measurement of health equity 121 sources were reviewed; these were chosen upon recommendation by authors and other subject matter experts), extracted “practices” (often congruent with the list developed for the 2013 forum), and shared them with coauthors and other subject matter experts for comment. When agreement was reached, the list of practices was finalized. As part of this process, practices were sometimes combined, split apart, or renamed to make them as intuitive as possible to the reader. The result was a set of recommended practices that we assert require consideration in the development of any set of indicators intended to assess the state of health equity in the United States.
It is beyond the scope of this article to attempt to account for all of the innovation that is occurring at various levels of society (eg, in communities, cities, and states, and among American Indian/Alaska Native Tribes) in how to monitor and address structural and contextual factors that are at the origin of inequities in health and health care. Even after such factors are identified through comprehensive research and analysis, the future of health equity remains dependent on continued innovation in developing methods to monitor them and intervene.
A Note About Terminology
Health disparities have been described as “differences in health outcomes and their determinants between segments of the population, as defined by social, demo graphic, environmental, and geographic attributes.”20* Although this definition of “health disparity” does not imply that something is avoidable or unfair, we consider reductions in health disparities to generally reflect progress toward health equity. Consistent with the definition provided earlier, we prefer the term “inequity” for those differences that are systematic, unfair, and avoidable. Notably, the international literature often uses the term “inequalities” to describe differences across individuals or across groups. It is also often used in reference to particular summary measures, such as those borrowed from the field of economics.20
Recommended Practices for Measurement to Advance Health Equity
Practice 1: Assess differences in health and its determinants that are associated with social position
The normative nature of the concept of equity means that health equity cannot be measured directly.2,11,21 The concept of equity is closely tied to fairness and justice, and what is considered fair and just depends on social norms; these norms may vary from society to society.22 In addition, there may be multiple valid approaches to operationalizing the concept of equity within the same social context.1,21,23 Thus, health equity poses measurement challenges. One approach to this dilemma is to operationalize health equity as the absence of that which is inequitable. Accordingly, the WHO defines equity as “the absence of avoidable or remediable differences among groups of people, whether those groups are defined socially, economically, demographically, or geographically.”24 Others have taken this idea a step further to focus, more specifically, on differences in health and its determinants (including social determinants) that are systematically associated with lower social position, asserting that such differences are unfair because they affect groups of people who are already at a disadvantage.4
While this approach to monitoring progress toward health equity may be viewed by some as an oversimplification,21 measuring differences in health and its determinants (including social determinants) that are associated with social position and assessing change over time is a prerequisite for timely assessment of the effects of policies on the health of different segments of the population.1 This implies a priori identification of characteristics of groups of people that are associated with more/less power and privilege11 or with higher/lower social position. Some domains within which such characteristics may be identified include race/ethnicity, sex, sexual orientation and gender identity, age, SES (including educational level, income, wealth, and occupation), country of birth, disability status, and geographic location.25 Toward this end, historic and current experiences of disadvantage can be ascertained through examining government reports, academic literature, and credible media reports.4 It is worth noting that although one’s social position may vary by one’s sex or age, some systematic differences in health outcomes by sex (eg, breast cancer) or age (eg, Alzheimer’s disease) cannot be deemed inequities.
As an example, the population characteristics of interest addressed in the CHDIRs included race and ethnicity, sex, sexual orientation, age, disability, SES, and geographic location. Whenever possible, disparities in health outcomes and their determinants were analyzed along these dimensions. In the most recent CHDIR, the most common dimension examined was race and ethnicity. Sexual orientation was examined for only one topic (HIV infection) because of data limitations.10
Practice 2: Assess social and structural determinants of health and consider multiple levels of measurement
There is preponderant evidence linking social determinants to health inequities in diverse settings and at different times in history12,26; social determinants explain some of the “avoidable or remediable” differences in health outcomes observed among groups with different social position. If we are to advance health equity and population health,9 then social determinants are critically important to monitor in their own right because they inform the prioritization of interventions that affect changes in these conditions. Rigorous monitoring of social determinants of health first requires understanding which social determinants are most important to monitor. For this reason, monitoring must be informed by prior research into the pathways through which social determinants affect health. Monitoring social determinants of health also necessitates moving beyond traditional health data sources. The practice of utilizing nonhealth data systems to monitor social determinants of health at the national level is still relatively uncommon and is far from routine, although some notable exceptions exist (eg, Healthy People 2020, as discussed earlier18).
Although considering social determinants of health measured at the individual level is important and illuminating, it is not a substitute for considering them at contextual levels (eg, neighborhood conditions), and vice versa. Decisions about the level of measurement should be made with care, and developing a rationale for choosing a particular level of measurement is essential. Structural determinants of health (including policies, programs, decision making/governance, and economics) require monitoring as well. Innovative approaches to assessing these important determinants of health have been proposed (eg, see the reports by Harrison and Dean27 and Sadana and Harper28).
Considering the 3 social determinants of health topic areas in the most recent CHDIR, the analysis of education and income relied on aggregated data collected at the individual level,29 as did the analysis of employment.30 The study of access to healthier food retailers used census tract–level data.31 Although rationales for choices of measurement level were not explicitly stated, they were implicit (in statements such as “purposes … are to discuss and raise awareness of differences in the characteristics of persons who are unemployed …”30) and multiple levels of measurement were used in the report as a whole, reflecting recognition that social determinants of health operate at multiple levels.
Practice 3: Provide reasons for methodological choices and clarify their implications
There is a need for better understanding—both among data analysts28 and among consumers of data32—of the weighty implications of analytic choices in measurement of health disparities, health inequities, and social determinants of health. Although providing reasons for methodological choices and clarifying their implications are important for any analysis undertaken in public health, experts in the field of health equity have emphasized this, perhaps because the potential for drawing different conclusions about health equity from the same data set has been described and demonstrated by Harper and colleagues,32–35 among others. Bias can stem not only from the value preferences or habits that inform choice of measurement practice(s) but also from the effect that different data presentation approaches have on audience perceptions or judgments of the resulting meaning of the data or analysis. Some key early considerations in measurement that have important implications for later interpretation of findings include (a) the point from which differences will be measured (the reference point), (b) whether differences will be measured on an absolute or relative scale, (c) whether the size of the social group will be accounted for, (d) whether differences will be evaluated with a pair-wise or summary approach, (e) and whether extra emphasis should be given to social groups that are of greater concern through differential weighting. Other considerations apply as well, and we cite several reports (eg, see the reports by Harper et al,33 World Health Organization,36 and Keppel et al37) that the reader can use as a selected bibliography of relevant literature.
Reference point
There are several choices for a reference point—the rate or other estimate from which differences are measured (for simplicity, we will refer to rates). Some of the options for a reference point include the largest social group, the social group with the most favorable rate for a health outcome or determinant, the group with the greatest social advantage, the total population, and a target chosen through a planning process, among others.11,37
A major health equity consideration in choosing a reference point for public health analyses is the level of health and its determinants one wishes to see achieved. For example, in the Healthy People 2020 framework, a lack of systematic differences among population groups is not sufficient to demonstrate health equity; the population also needs to be faring well. Under this framework, the total population level of a particular health outcome or determinant might not be the most appropriate reference point for evaluating progress toward health equity. Accordingly, Healthy People 201037 (and, subsequently, Healthy People 2020) used the group with the most favorable (or, alternatively, the least adverse) rate to highlight opportunities for improvement.
Absolute versus relative scale
Considering one scale versus the other can lead to different conclusions. For example, in the Figure, age-adjusted breast cancer death rates are decreasing for both non-Hispanic white and non-Hispanic black women. The simple difference (an absolute measure of disparity) between the rates also has decreased, by 0.8 per 100 000 (35.1 − 26.0 = 9.1 in 2001 vs 29.2 − 20.9 = 8.3 in 2013), although this change was not statistically significant. However, when one considers the rate ratio (a common relative measure in the epidemiologic literature), the relative disparity* between the 2 groups has increased (rate ratio 35.1 ÷ 26.0 = 1.35 in 2001 is less than the ratio 29.2 ÷ 20.9 = 1.40 in 2013).
FIGURE. Female Breast Cancer Deaths, 2001–2013a.
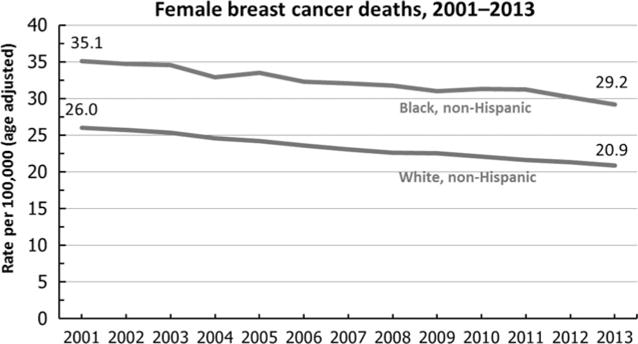
Abbreviation: ICD-10, International Classification of Diseases, Tenth Revision. aData are for ICD-10 code C50 reported as underlying cause of death and are age-adjusted using the year 2000 standard population. Prior to 2003, only 1 race category could be recorded; recording more than 1 race was not an option. Beginning in 2003, multiple-race data were reported by some states; multiple-race data were bridged to the single-race categories for comparability. From National Vital Statistics System–Mortality, National Center for Health Statistics, Centers for Disease Control and Prevention.
Beyond the potentially diverging conclusions that result from using one scale versus the other, the choice of an absolute or relative scale commits the user to implicit value judgments that have been elucidated in detail elsewhere.32 Broadly speaking, the relative scale does not take into account the magnitude of the underlying rates for the health outcome under consideration. Indeed, the rate ratio of 1.40 in 2013 would remain unchanged whether the breast cancer death rates for the 2 groups were doubled (58.4 ÷ 41.8 = 1.40) or halved (14.6 ÷ 10.4 = 1.40). On the contrary, the choice of the absolute scale reflects more concern with how each social group is faring on the health outcome and how the population is faring overall.
The simple difference between the 2 breast cancer death rates would not increase if the groups were to further improve in parallel. For example, if both rates were to demonstrate a 10% improvement, consistent with the corresponding Healthy People 2020 objective,† from 29.2 and 20.9 in 2013 to 26.3 and 18.8 in 2020, then the simple difference would decrease by an additional 0.8 per 100 000, from 8.3 to 7.5, which would reflect both an improvement in the groups’ health outcomes and a reduction in the gap between the groups.
For reasons that have been detailed elsewhere, both absolute and relative measures of disparity should be reported34,37 and considered in the assessment of progress toward health equity. The CHDIRs routinely present both relative and absolute measures of disparity, allowing the reader to take both into consideration in drawing conclusions.10,20
Accounting for group size
Measures of absolute or relative disparity are not sufficient for assessing the societal impact or burden of disparities, because the assessment of impact requires a “head count”—the number of persons affected in each group—a concept closely related to the size of groups.
Group size also is pertinent to the question of differential weighting, which is further discussed later. When all groups are weighted equally, irrespective of their size, an intervention that targets a relatively small group with a relatively large burden of disease can prove very effective in reducing measures of overall disparity. On the contrary, when groups are weighted according to their size, that same intervention will not have as much impact on reducing measures of overall disparity. This trade-off between individuals’ and groups’ burden of disease is referred to as the “health inequality paradox.”38,39
Pair-wise versus summary approach
Population breakdown by race and ethnicity, education, or income often results in 3 or more groups for comparison relative to the reference point. The resulting pair-wise differences between groups can be combined using summary measures. Summary measures have a long history and have been reviewed in the health economics literature (eg, see the reports by Wagstaff et al40 and Mackenbach et al41). Recent comparative studies of summary measures continue to explore their qualitative and quantitative features (eg, see the reports by Harper et al,33 Levy et al,42 and Talih43).
Summary measures are useful in that they quantify the relationship between the distributions of health outcomes and population shares. Summary measures are especially useful when comparisons among numerous populations as well as among different time periods are desired, because the alternative option of multiple pair-wise comparisons over time can be difficult to interpret. As an example, if non-Hispanic whites, non-Hispanic blacks, Hispanics, Asians (non-Hispanic), Pacific Islanders (non-Hispanic), and American Indians/Alaska Natives (non-Hispanic) were compared with the population average on a particular health outcome over time, there would be 6 different comparisons to monitor, whereas a summary measure monitored over time could indicate whether, overall, racial and ethnic differences for that outcome were increasing or decreasing over time.
Because many summary measures are centered on the relation between the distributions of health outcomes and population shares, they do not account for the association between SES and health outcomes. To address this need, the measurement literature includes the development of summary measures that account for the socioeconomic gradient.44–47
Differential weighting
Because of the “unfavorable social, economic, or political conditions that some groups of people systematically experience based on their relative position in social hierarchies,”23(pS151) some social groups may be deemed to be of greatest concern and merit extra emphasis (eg, in the design of interventions, applying a tailored approach to complement a universal approach48). Differential weighting can provide the analyst with the measurement tool to account for this. For example, if we consider it more inequitable when groups with lower SES experience worse health outcomes than groups with higher SES (vs the reverse situation of groups with higher SES showing worse outcomes), we can use socioeconomic health inequality measures to put more weight on groups with lower SES.
Measurement choices of a reference point, absolute versus relative scale, whether to account for group size, whether to adopt a pair-wise versus summary approach, and whether to use differential weighting affect the findings, which, in turn, affect conclusions drawn as to whether there are inequities and whether or not they have changed. Different conclusions can lead to different public health priorities and actions.34 For example, the trade-off between individuals’ and groups’ burden of disease (ie, health inequality paradox) means that conclusions about the potential impact of public health interventions can be very different depending on the measures used. All those who act to advance health equity (including government, communities, researchers and academia, and the private sector) would benefit from clear understanding that conclusions drawn about health equity heavily depend on the measures used.
Data analysts and those who design systems to monitor progress toward health equity can make reasoned methodological choices a priori, provide reasons for the choices, and clearly explain what findings mean33 to foster greater understanding of findings among those who must act on them.
Practice 4: Address within-group heterogeneity by comparing groups simultaneously classified by multiple social statuses
Because groups defined on the basis of social position show substantial internal heterogeneity in health and the conditions underlying health, multiple social statuses must be accounted for simultaneously in monitoring progress toward health equity. Only then is it possible to attend to the health of those with “fewer resources and/or greater obstacles to addressing problems”11(p185)—an orientation that necessarily underlies efforts to achieve health equity.
For example, in the United States, African Americans and Latinos have “less wealth at every level of income [and] higher exposure to occupational risks within the same occupational categories.”49(p1260) A particular source of heterogeneity among immigrant populations is length of time in the United States. Time since immigration moderates associations between SES and health risks and outcomes, with stronger associations being evident among those who have resided in the United States for longer periods of time. The same relationships hold for second- and later generation immigrants as compared with first-generation immigrants. Importantly, SES does not fully account for differences in health outcomes by race/ethnicity. Accounting for SES in an analysis can lessen apparent disparities by race/ethnicity, but it generally does not eliminate them.49,50
In the US context, attending to heterogeneity involves monitoring health and determinants at the intersection of race and ethnicity, SES, and sex. For population groups with a high proportion of immigrants (eg, Hispanics and Latinos), consideration of country of birth (eg, US-born vs foreign-born) and generational status (eg, first or second generation) are important, given that health may differ markedly along these dimensions, with, for example, foreign-born Hispanics and Latinos showing overall better health than their US-born counterparts.51 Other intersections require attention as well (eg, race/ethnicity, sex, and disability status; race/ethnicity, sex, and sexual orientation).
The CHDIRs have accounted for within-group heterogeneity for some topics but not for others.10,20 Although not a monitoring effort, an example of a national-level assessment that took heterogeneity into account was CDC’s first Vital Signs Morbidity and Mortality Weekly Report (MMWR) on Hispanic health.51 This nationally representative study compared Hispanics, Hispanic origin subgroups (eg, Cuban, Puerto Rican), and non-Hispanic whites by nativity (US-born vs foreign-born) and sex on causes of death, prevalence of disease and risk factors, and use of health services.
Practice 5: The need to communicate to a wide array of stakeholders can often be taken into consideration in the choice of measures and analytic methods
While other considerations, such as rigor, are primary, stakeholders and their communication needs can often be considered in the selection of measures and analytic methods. (As noted earlier, key actors in health equity include government, communities, researchers and academia, and the private sector.6) This is a delicate balance, however, and it cannot be emphasized enough that considering the needs of stakeholders creates the potential, intended or unintended, to bias the results and conclusions drawn. Thus, practice 5 is intimately tied to practice 3 (Provide reasons for methodological choices and clarify their implications). As noted in that section, implications can include effects on audience perceptions or judgments, and transparency is critical.
Benchmarking is a rigorous measurement practice that is intuitive in its appeal to a broad set of audiences. The WHO’s Gender, Health Equity and Human Rights Team promotes the use of benchmarking to place changes over time in context.36 Similarly, in the United States, the HHS Agency for Healthcare Research and Quality National Healthcare Quality and Disparities Reports52 estimate national benchmarks based on the average values for the 10% of states that have the best outcomes for a measure of interest. Differences between population groups can then be understood in the context of the projected time expected for these groups to achieve the designated benchmark, assuming that past trends continue.
For example, on the basis of 2008 data for the top 5 states, the 2013 Agency for Healthcare Research and Quality National Healthcare Disparities Report53 estimates that the achievable benchmark for female breast cancer deaths was 17 per 100 000 population (age-adjusted) and that, as of 2010, white women could achieve this benchmark in 9 years whereas black women could achieve it in 28 years. Time to achieve benchmark is a measure that is not only rigorous but also useful for audiences who seek to call attention to and mobilize action to address health inequities.
Discussion
The article aims to make explicit underlying concepts of health equity and challenges and opportunities associated with assessing and monitoring progress toward meeting the national goal of achieving health equity.
Measuring progress toward health equity is necessary
An overarching public health goal of the United States is to eliminate disparities in health and health care to improve the overall health of the nation and achieve health equity (Healthy People 2020). The 2011 Action Plan committed public health practitioners and policy makers to realize these goals at the national, state, and local levels.54
Accurate and timely assessment and monitoring of the magnitude and direction of change of health disparities and their determinants are necessary for public health evaluation of progress toward the US goals (Healthy People 2020). Increasingly, health disparities are showing stagnation or a widening of the “gap,” which is consistent with the “inverse equity hypothesis” that initially the benefit of interventions accrues to the more advantaged groups.55 Eventually, the magnitude of inequality declines with increasing access to the interventions by the more disadvantaged groups. Evidence from systematic reviews suggests that this phenomenon is not inevitable: “downstream” prevention interventions (directed at individual-level factors) are more likely than “upstream” interventions (directed at social or policy-level factors) to increase health disparities.56
Recognizing that measurement decisions will influence the results is important
Numerous measures for macro- and microlevel indicators have been suggested. Typically, health disparities are reported as relative measures (as ratios) derived by comparing the groups with the poorest and best levels of health. A recent review of studies reported in major journals showed that the use of relative measures of effect remains a common practice: almost 90% of studies reporting health disparities used relative measures.35 As discussed previously, the choice of the scale used may lead to different conclusions and reflects implicit value judgments. As a result, the choice of measurement scale may influence findings and hence policy formulation and allocation of resources.
Indeed, a suite of measures provides the most holistic picture of health disparities. A seminal monograph sponsored by the National Cancer Institute recommended employing a variety of measures on the same data to ensure a triangulated depiction of health disparities.34 This monograph laid the groundwork for the so-called Health Disparities Calculator (HD*Calc), developed by the National Cancer Institute as statistical software for calculating multiple measures to monitor and examine health disparities related to cancer. HD*Calc calculates 11 measures of health disparities that vary according to scale (absolute or relative), reference group, weighting, etc.57
More recently, the National Center for Health Statistics, in collaboration with the HHS Office of Disease Prevention and Health Promotion and HHS Office of Minority Health, has developed an online tool to help Healthy People 2020 stakeholders describe and analyze health disparities data. Publicly released in Spring 2015, the health disparities tool (“HD tool,” for short) is a new feature of the http://healthypeople.gov Web site designed to summarize health disparities as well as changes in disparities over time for all measurable population-based Healthy People 2020 objectives with available data. The HD tool produces detailed pair-wise comparisons, summaries of health disparities by population groups (eg, by sex, race/ethnicity, educational attainment, or family income), and graphical displays to visualize disparities as well as changes in disparities over time. The HD tool summary measures include both absolute and relative measures of disparity: simple difference between highest and lowest rates; ratio between highest and lowest rates; and a rate ratio between the best group rate and the average rate for all other groups. Other suites of measures have been developed as well.43,47
Currently, social determinants of health are often defined by individual attributes (eg, gender, educational attainment, poverty status, disability status)
This approach is unlikely to be sufficient to meet national goals to achieve health equity. Given that health inequities arise from the “immediate and structural conditions in which people are born, grow, live, work, and age,”58(p1661) it will be necessary to generate analytic data sets that routinely capture structural and contextual factors that are the origins of inequities in health and health care.59,60
It is critical that public health, in collaboration with health care and other sectors, continue to advance understanding of social determinants of health and the pathways through which they operate on specific health outcomes
Identifying these root causes, particularly those that impact a wide variety of health outcomes, can contribute to effective and efficient use of limited public health resources.12,26
Although improvements are regularly being made by various agencies and organizations, some national data systems are currently limited in many ways
Sample sizes are one obvious issue, especially for smaller demographic groups and geographies that may be of particular interest when considering issues related to equity. For some important characteristics, such as gender identity, sexual orientation, and disability status, the measurement of the characteristic itself has not yet been standardized, or in some cases implemented, across national data systems, although progress is being made.
Many public health researchers have little experience with the concepts of health equity and the measures discussed herein
Reduction of health disparities and progress to health equity are achievable if intensive and systematic training is available for the workforce at the national, state, and local levels.
Conclusions
Over the decades since the clarion call for health equity was raised domestically by the Secretary’s Task Force Report on Black and Minority Health7 and internationally by the writings of Margaret Whitehead3 and others, much has been learned about how to measure health disparities, health inequities, and social determinants of health at the national level to support the advancement of health equity. Nevertheless, there is still much to learn and implement, and the challenges of health equity persist. As the field of health equity continues to evolve, we anticipate that the present discussion will contribute to the laying of a foundation for standard practice in the monitoring of national progress toward achievement of health equity.
Acknowledgments
The authors acknowledge the contributions of Ms Monica Molina, who convened early discussions that led to the development of this report, as well as Dr Sonja Hutchins, who reviewed early versions of the material.
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Footnotes
The authors have no conflicts of interest to report.
Relative disparities also may be expressed as percent differences. For example, rate ratios of 1.0 or more are converted to percent differences by subtracting 1.0 and multiplying by 100%.
Healthy People 2020 objective C-3, to reduce the female breast cancer death rate, targets a 10% improvement in the age-adjusted breast cancer death rate, nationally, from 23.0 deaths per 100 000 population in 2007 to 20.7 per 100 000 by 2020. See http://www.healthypeople.gov/node/4069/data details.
Contributor Information
Dr Ana Penman-Aguilar, Office of Minority Health and Health Equity.
Dr Makram Talih, Centers for Disease Control and Prevention, Atlanta, Georgia; National Center for Health Statistics, Centers for Disease Control and Prevention, Hyattsville, Maryland.
Dr David Huang, Centers for Disease Control and Prevention, Atlanta, Georgia; National Center for Health Statistics, Centers for Disease Control and Prevention, Hyattsville, Maryland.
Dr Ramal Moonesinghe, Office of Minority Health and Health Equity.
Dr Karen Bouye, Office of Minority Health and Health Equity.
Dr Gloria Beckles, National Center for Chronic Disease and Health Promotion.
References
- 1.Braveman P. Health disparities and health equity: concepts and measurement. Annu Rev Public Health. 2006;27:167–194. doi: 10.1146/annurev.publhealth.27.021405.102103. [DOI] [PubMed] [Google Scholar]
- 2.Braveman P, Gruskin S. Defining equity in health. J Epidemiol Community Health. 2003;57(4):254–258. doi: 10.1136/jech.57.4.254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Whitehead M. The concepts and principles of equity and health. Int J Health Serv. 1992;22(3):429–445. doi: 10.2190/986L-LHQ6-2VTE-YRRN. [DOI] [PubMed] [Google Scholar]
- 4.Braveman P. What is health equity: and how does a life-course approach take us further toward it? Matern Child Health J. 2014;18(2):366–372. doi: 10.1007/s10995-013-1226-9. [DOI] [PubMed] [Google Scholar]
- 5.World Health Organization. What are social determinants of health? http://www.who.int/socialdeterminants/sdh_definition/en. Accessed January 3, 2015.
- 6.Commission on Social Determinants of Health. Closing the Gap in a Generation: Health Equity Through Action on the Social Determinants of Health Final Report of the Commission on Social Determinants of Health. Geneva, Switzerland: World Health Organization; 2008. [Google Scholar]
- 7.Heckler M. Report of the Secretary’s Task Force on Black & Minority Health Report of the Secretary’s Task Force on Black and Minority Health. Washington, DC: US Department of Health and Human Services; 1985. [Google Scholar]
- 8.Institute of Medicine. Unequal Treatment: Confronting Racial and Ethnic Disparities in Healthcare. Washington, DC: National Academies Press; 2003. [PubMed] [Google Scholar]
- 9.Braveman P, Egerter S, Williams DR. The social determinants of health: coming of age. Annu Rev Public Health. 2011;32:381–398. doi: 10.1146/annurev-publhealth-031210-101218. [DOI] [PubMed] [Google Scholar]
- 10.Meyer PA, Penman-Aguilar A, Campbell VA, Graffunder C, O’Connor AE, Yoon PW. Conclusion and future directions: CDC Health Disparities and Inequalities Report—United States, 2013. MMWR Surveill Summ. 2013;62(suppl 3):184–186. [PubMed] [Google Scholar]
- 11.Braveman PA. Monitoring equity in health and healthcare: a conceptual framework. J Health Popul Nutr. 2003;21(3):181–192. [PubMed] [Google Scholar]
- 12.Marmot M, Allen JJ. Social determinants of health equity. Am J Public Health. 2014;104(suppl 4):S517–S519. doi: 10.2105/AJPH.2014.302200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Penman-Aguilar A, Bouye K, Liburd LC. Background and rationale. MMWR Surveill Summ. 2014;63(suppl 1):3–4. [PubMed] [Google Scholar]
- 14.Rudolph L, Caplan J, Ben-Moshe K, Dillon L. Health in All Policies: A Guide for State and Local Governments. Washington, DC/Oakland, CA: American Public Health Association/Public Health Institute; 2013. [Google Scholar]
- 15.National Association of County & City Health Officials. Expanding the Boundaries: Health Equity and Public Health Practice. Washington, DC: National Association of County & City Health Officials; 2014. [Google Scholar]
- 16.Frieden TR. CDC Health Disparities and Inequalities Report—United States, 2013 [Foreword] MMWR Surveill Summ. 2013;62(suppl 3):1–2. [PubMed] [Google Scholar]
- 17.US Department of Health and Human Services, Office of Minority Health. National Partnership for Action to End Health Disparities. The National Plan for Action Draft as of February 17, 2010. http://www.healthypeople.gov/2020/about/foundation-health-measures/Disparities#5. Accessed January 9, 2015.
- 18.US Department of Health and Human Services, Office of Disease Prevention and Health Promotion. (Social determinants).Healthy People 2020. http://www.healthypeople.gov/2020/leading-health-indicators/2020-lhi-topics/Social-Determinants. Accessed February 26, 2015.
- 19.Centers for Disease Control and Prevention. CDC Health Disparities & Inequalities Report (CHDIR) http://www.cdc.gov/minorityhealth/CHDIReport.html. Accessed February 18, 2015.
- 20.Truman BI, Kay Smith C, Roy K, et al. et al. Rationale for regular reporting on health disparities and inequalities—United States. MMWR Surveill Summ. 2011;60(suppl):3–10. [PubMed] [Google Scholar]
- 21.Sen A. Why health equity? Health Econ. 2002;11(8):659–666. doi: 10.1002/hec.762. [DOI] [PubMed] [Google Scholar]
- 22.Gollust SE, Cappella JN. Understanding public resistance to messages about health disparities. J Health Commun. 2014;19(4):493–510. doi: 10.1080/10810730.2013.821561. [DOI] [PubMed] [Google Scholar]
- 23.Braveman PA, Kumanyika S, Fielding J, et al. Health disparities and health equity: the issue is justice. Am J Public Health. 2011;101(suppl 1):S149–S155. doi: 10.2105/AJPH.2010.300062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.World Health Organization. Health Systems. Equity. http://www.who.int/healthsystems/topics/equity/en. Accessed February 18, 2015.
- 25.Dean H. Sustaining a focus on health equity at the centers for disease control and prevention through organizational structures and functions. J Public Health Manage Pract. 2016;22(1 suppl):S60–S67. doi: 10.1097/PHH.0000000000000305. [DOI] [PubMed] [Google Scholar]
- 26.Braveman P, Krieger N, Lynch J. Health inequalities and social inequalities in health. Bull World Health Organ. 2000;78:232–235. [PMC free article] [PubMed] [Google Scholar]
- 27.Harrison KM, Dean HD. Use of data systems to address social determinants of health: a need to do more. Public Health Rep. 2011;126(suppl 3):1–5. doi: 10.1177/00333549111260S301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Sadana R, Harper S. Data systems linking social determinants of health with health outcomes: advancing public goods to support research and evidence-based policy and programs. Public Health Rep. 2011;126(suppl 3):6–13. doi: 10.1177/00333549111260S302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Beckles GL, Truman BI, Centers for Disease Control and Prevention Education and income—United States, 2009 and 2011. MMWR Surveill Summ. 2013;62(suppl 3):9–19. [PubMed] [Google Scholar]
- 30.Athar HM, Chang MH, Hahn RA, Walker E, Yoon P, Centers for Disease Control and Prevention Unemployment— United States, 2006 and 2010. MMWR Surveill Summ. 2013;62(suppl 3):27–32. [PubMed] [Google Scholar]
- 31.Grimm KA, Moore LV, Scanlon KS, Centers for Disease Control and Prevention Access to healthier food retailers—United States, 2011. MMWR Surveill Summ. 2013;62(suppl 3):20–26. [PubMed] [Google Scholar]
- 32.Harper S, King NB, Meersman SC, Reichman ME, Breen N, Lynch J. Implicit value judgments in the measurement of health inequalities. Milbank Q. 2010;88(1):4–29. doi: 10.1111/j.1468-0009.2010.00587.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Harper S, Lynch J, Meersman SC, Breen N, Davis WW, Reichman ME. An overview of methods for monitoring social disparities in cancer with an example using trends in lung cancer incidence by area-socioeconomic position and race-ethnicity, 1992-2004. Am J Epidemiol. 2008;167(8):889–899. doi: 10.1093/aje/kwn016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Harper S, Lynch J. Selected Comparisons of Measures of Health Disparities: A Review Using Databases Relevant to Healthy People 2010 Cancer-Related Objectives, in NCI Cancer Surveillance Monograph Series. Bethesda, MD: National Cancer Institute; 2007. [Google Scholar]
- 35.King NB, Harper S, Young ME. Use of relative and absolute effect measures in reporting health inequalities: structured review. BMJ. 2012;345:e5774. doi: 10.1136/bmj.e5774. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.World Health Organization. Handbook on Health Inequality Monitoring With a Special Focus on Low- and Middle-Income Countries. Geneva, Switzerland: World Health Organization; 2013. [Google Scholar]
- 37.Keppel K, Pamuk E, Lynch J, et al. Methodological issues in measuring health disparities. Vital Health Stat. 2005;2(141):1–16. [PMC free article] [PubMed] [Google Scholar]
- 38.Frohlich KL, Potvin L. Transcending the known in public health practice: the inequality paradox: the population approach and vulnerable populations. Am J Public Health. 2008;98(2):216–221. doi: 10.2105/AJPH.2007.114777. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Rose G. Sick individuals and sick populations. 1985. Bull World Health Organ. 2001;79(10):990–996. [PMC free article] [PubMed] [Google Scholar]
- 40.Wagstaff A, Paci P, van Doorslaer E. On the measurement of inequalities in health. Soc Sci Med. 1991;33(5):545–557. doi: 10.1016/0277-9536(91)90212-u. [DOI] [PubMed] [Google Scholar]
- 41.Mackenbach JP, Kunst AE. Measuring the magnitude of socio-economic inequalities in health: an overview of available measures illustrated with two examples from Europe. Soc Sci Med. 1997;44(6):757–771. doi: 10.1016/s0277-9536(96)00073-1. [DOI] [PubMed] [Google Scholar]
- 42.Levy JI, Chemerynski SM, Tuchmann JL. Incorporating concepts of inequality and inequity into health benefits analysis. Int J Equity Health. 2006;5:2. doi: 10.1186/1475-9276-5-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Talih M. A reference-invariant health disparity index based on Rényi divergence. Ann Appl Stat. 2013;7(2):1217–1243. doi: 10.1214/12-AOAS621. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Pamuk ER. Social class inequality in mortality from 1921 to 1972 in England and Wales. Popul Stud (Camb) 1985;39(1):17–31. doi: 10.1080/0032472031000141256. [DOI] [PubMed] [Google Scholar]
- 45.Pamuk ER. Social class inequality in infant mortality in England and Wales from 1921 to 1980. Eur J Popul. 1988;4(1):1–21. doi: 10.1080/0032472031000141256. [DOI] [PubMed] [Google Scholar]
- 46.Wagstaff A. Inequality aversion, health inequalities and health achievement. J Health Econ. 2002;21(4):627–641. doi: 10.1016/s0167-6296(02)00006-1. [DOI] [PubMed] [Google Scholar]
- 47.Talih M. Examining socioeconomic health disparities using a rank-dependent Rényi index. Ann Appl Stat. 2015;9(2):992–1023. doi: 10.1214/15-aoas822. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Hutchins SS, Jiles R, Bernier R. Elimination of measles and of disparities in measles childhood vaccine coverage among racial and ethnic minority populations in the United States. J Infect Dis. 2004;189(suppl 1):S146–S152. doi: 10.1086/379651. [DOI] [PubMed] [Google Scholar]
- 49.Williams DR, Kontos EZ, Viswnath K, et al. Integrating multiple social statuses in health disparities research: the case of lung cancer. Health Serv Res. 2012;47(3, pt 2):1255–1277. doi: 10.1111/j.1475-6773.2012.01404.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Palloni A, Arias E. Paradox lost: explaining the Hispanic adult mortality advantage. Demography. 2004;41(3):385–415. doi: 10.1353/dem.2004.0024. [DOI] [PubMed] [Google Scholar]
- 51.Dominguez K, Penman-Aguilar A, Chang MH, et al. Vital Signs: leading causes of death, prevalence of diseases and risk factors, and use of health services among Hispanics in the United States—2009-2013. MMWR Morb Mortal Wkly Rep. 2015;64(17):469–478. [PMC free article] [PubMed] [Google Scholar]
- 52.Agency for Healthcare Research and Quality. National Healthcare Quality & Disparities Reports. http://www.ahrq.gov/research/findings/nhqrdr/index.html. Accessed February 22, 2015.
- 53.Agency for Healthcare Research and Quality. 2013 National Healthcare Disparities Report. Rockville, MD: Agency for Healthcare Research and Quality, US Department of Health and Human Services; 2014. [Google Scholar]
- 54.Koh HK, Graham G, Glied SA. Reducing racial and ethnic disparities: the action plan from the department of health and human services. Health Aff (Millwood) 2011;30(10):1822–1829. doi: 10.1377/hlthaff.2011.0673. [DOI] [PubMed] [Google Scholar]
- 55.Victora CG, Vaughan JP, Barros FC, Silva AC, Tomasi E. Explaining trends in inequities: evidence from Brazilian child health studies. Lancet. 2000;356(9235):1093–1098. doi: 10.1016/S0140-6736(00)02741-0. [DOI] [PubMed] [Google Scholar]
- 56.Lorenc T, Petticrew M, Welch V, Tugwell P. What types of interventions generate inequalities? Evidence from systematic reviews. J Epidemiol Community Health. 2013;67(2):190–193. doi: 10.1136/jech-2012-201257. [DOI] [PubMed] [Google Scholar]
- 57.Breen N, Scott S, Percy-Laurry A, Lewis D, Glasgow R. Health disparities calculator: a methodologically rigorous tool for analyzing inequalities in population health. Am J Public Health. 2014;104(9):1589–1591. doi: 10.2105/AJPH.2014.301982. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Marmot M, Friel S, Bell R, et al. Closing the gap in a generation: health equity through action on the social determinants of health. Lancet. 2008;372(9650):1661–1669. doi: 10.1016/S0140-6736(08)61690-6. [DOI] [PubMed] [Google Scholar]
- 59.Ottersen OP, Dasgupta J, Blouin C, et al. The political origins of health inequity: prospects for change. Lancet. 2014;383(9917):630–667. doi: 10.1016/S0140-6736(13)62407-1. [DOI] [PubMed] [Google Scholar]
- 60.Braveman P, Gottlieb L. The social determinants of health: it’s time to consider the causes of the causes. Public Health Rep. 2014;129(suppl 2):19–31. doi: 10.1177/00333549141291S206. [DOI] [PMC free article] [PubMed] [Google Scholar]