

Abstract
Background:
The issue of menstrual hygiene is inadequately acknowledged in our nation. The use of sanitary pads and washing the genital area are essential practices for good menstrual hygiene. Poor menstrual hygiene may lead to itching or rashes in the perineal region, bad odor, and sometimes, major complications such as pelvic inflammatory disease and toxic shock syndrome. Therefore, the objective of this study was to assess the knowledge and practice of menstrual hygiene among reproductive age group women.
Methods:
A Community-based cross-sectional study design was employed. Study was conducted from January 2012 to April 2013. Data were collected using a pretested semi-structured structured questionnaire. The data were entered and analyzed into a computer using SPSS version 20.
Results:
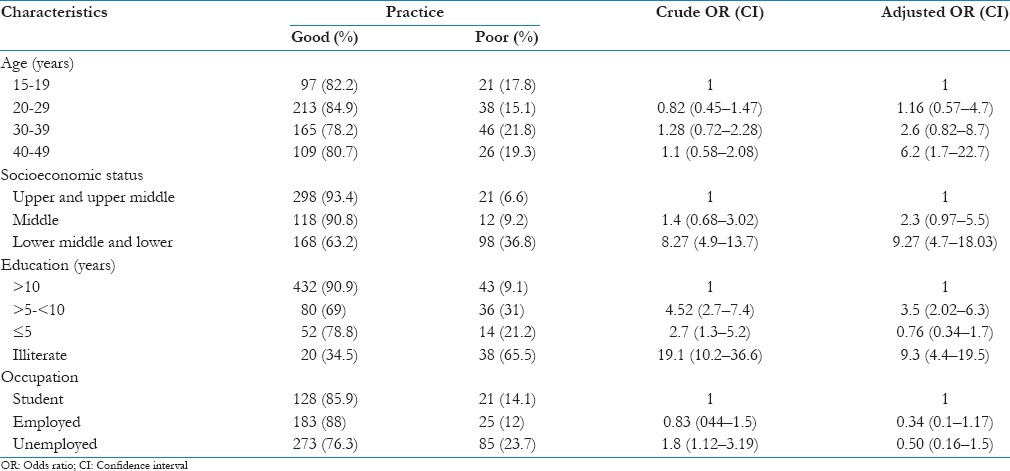
In this study, 584 (81.7%) respondents had good practice of menstrual hygiene. The findings of the study showed a significant positive association between good practices of menstrual hygiene and years of education of the study subject (adjusted odds ratio [AOR] =9.3, 95% confidence interval [CI]: 4.4–19.5), having a higher socioeconomic status (AOR = 9.27, 95% CI: 4.7–18.03).
Conclusions:
Awareness of good menstrual practices is of utmost importance. Health education regarding menstrual hygiene should be a part of school curriculum and health institutes. Social marketing of good quality, low-cost sanitary napkins at accessible outlets, provision for adequate water supply, vending machines for low-cost sanitary napkins, privacy and wall-mounted incinerators for disposal in schools, workplaces, and public places would go a long way in improving the menstrual hygiene and help them in securing healthy lifestyle.
Keywords: Menstrual hygiene, menstruation, practice, sanitary pads
Introduction
Menstrual hygiene is defined as the principle of maintaining cleanliness of the body during menstrual flow. It requires basic facilities such as appropriate clothes, soakage material, water, soap, and toilet facilities with privacy. Poor menstrual hygiene may lead to problems such as itching or rashes in the perineal region, bad odor, and also major complications such as pelvic inflammatory disease and toxic shock syndrome.[1] Women can also have related complications during conception and pregnancy. Unaddressed menstrual hygiene is also said to hamper the achievement of some of the millennium developmental goals.[2]
The issue of menstrual hygiene is inadequately acknowledged and has not received proper attention.[3] Good hygienic practices, such as the use of sanitary pads and adequate washing of the genital areas, are essential during the menstrual period. Women and girls of reproductive age need access to clean and soft absorbent sanitary products which in the long run protect their health from various infections.[4]
Studies in India have shown that at various places, the proportion of women using sanitary pads, still remain low, while the women with reproductive tract infections tend to have poorer menstrual hygiene practices.[5,6,7]
Most of the studies in India have been focusing on the menstrual hygiene practices among adolescent girls and not the whole of reproductive age group, therefore, this study was conducted in an urban area of southwest Delhi with an objective to study the menstrual hygiene practices and their determinants among women of reproductive age group.
Methods
Study design, settings, and participants
Community based cross-sectional study was conducted among reproductive age group women (15–49 years) residing in Sector 7, Dwarka area of Southwest Delhi, which is a field practice area under the Department of Community medicine, Lady Hardinge Medical College. The study period was January 2012–April 2013. The total population of the study area is approximately 10,000, residing in approximately 1200 households out of which 2170 were women of reproductive age group. All girls, over 15 years of age, who had attained menarche were included in the study while women in primary amenorrhea, who had not yet attained menarche, women who had attained menopause and had undergone hysterectomy were excluded from the study.
Sample size and sampling procedures
The sample size was determined using a formula for the estimation of single population proportion with the assumption of 95% confidence interval (CI), 5% margin of error, and prevalence of usage of sanitary pads 11.5%, and 2.5% absolute precision.[8] To compensate for the nonresponse rate, 10% of the determined sample was added up on the calculated sample size and the final sample size was found to be 715. To find the required sample size, approximately 30% of the population was covered. All the 8 blocks in the area were included by systematic random sampling. In each block, first house was selected randomly and every third house was visited to find women of reproductive age group.
Data collection procedures
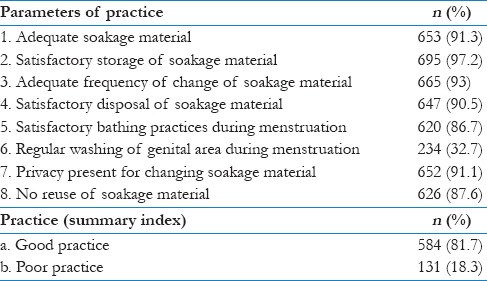
A semi-structured, pretested pro forma was used for data collection which included the general and sociodemographic information about the women, hygiene practices during menstruation, and problems faced by them after menstrual bleeding. The questionnaire was prepared in English and was translated into Hindi, the regional language of the area. The subject's menstrual hygiene score was calculated out of the eight specific questions [Table 1]. Each adequate/satisfactory response earned one point, whereas inadequate/unsatisfactory response attracted no mark and thus the sum score of menstrual hygiene was calculated. Accordingly, the median score of menstrual hygiene (7, IQR 7,8) was used to decide the cutoffs of the rank. Good practices of menstrual hygiene were given to those respondents who scored 7–8 points and poor practices menstrual hygiene was given to those respondents who scored 0–6 points.
Table 1.
Menstrual hygiene practices of the study subject (n=715)
Data processing and statistical analysis
Data were entered and analyzed into a using Statistical package for Social Sciences version 19.0 (IBM, PASW Statistics, India Country office, Bangalore, India). The descriptive analysis including proportions, percentages, frequency distribution, and measures of central tendency was done. Initially, bivariate analysis was performed between dependent variable (practice of menstrual hygiene) and each of the independent variables (Socio-demographic variables), one at a time. Their odds ratios (OR) at 95% CIs and P values were obtained, to identify important candidate variables for multivariate analysis. All variables found to be significant at bivariate level (at P < 0.05) were entered into multivariate analysis using a logistic regression model to control for confounding factors.
Ethical considerations
Ethical clearance and permission were obtained from the ethical review board of Lady Hardinge Medical College, New Delhi. The purpose of the study was explained to the participants, and written informed consent was obtained from each participant. Participants were informed of their full right to skip or ignore any question or withdraw from their participation at any stage of the study.
Results
Sociodemographic characteristics of respondents
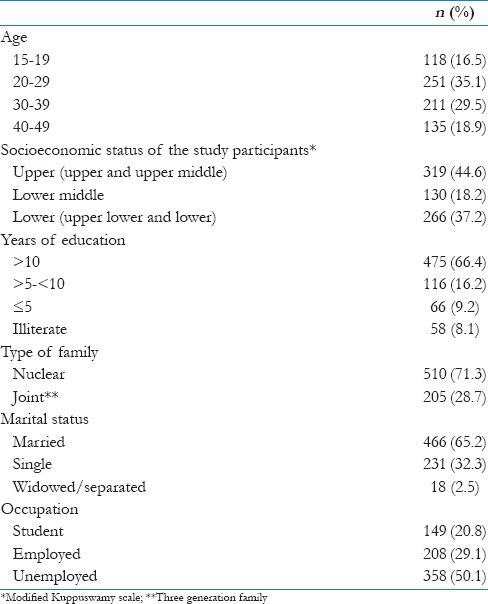
A total of 715 girls and women participated in the study. The largest proportion of women belongs to the age group of 20–29 years, i.e., 31.5% followed by 30–39 years and 40–49 years, which was 29.5% and 18.9%, respectively. Women in the age group of 15–19 years were 16.5%. Nearly 45% of the participants belonged to the upper (upper and upper middle) socioeconomic status followed by lower (Upper lower and lower) socioeconomic status which was 37.2%. Another 18.2% of participants belonged to lower middle socioeconomic status. More than half of the study participants (66.4%) had been formally educated for more than 10 years while 8.1% of study participants were illiterate. Majority of the study participants (71.3%) belonged to a nuclear family and more than half of the participants (65.2%) were married. One hundred and forty-nine participants (20.8%) were students in school or college and another 208 (29.1%) were employed [Table 2].
Table 2.
Sociodemographic profile of study participants (n=715)
Hygiene practices during menstruation
As to the data obtained, out of the total respondents, 584 (81.7%) of the respondents had good practices of menstrual hygiene. Majority of participants (91.3%), were using an adequate soakage material during menstruation, and almost all (97.2%) were storing the soakage material adequately. In addition, the majority of study participants (93%) used to change the soakage material at adequate intervals. Nearly 90% of participants disposed the material satisfactorily had satisfactory bathing practices during menstruation and did not reuse the soakage material. A small proportion of participants (32.7%) were seen to regularly wash their genital area after using toilet, during menstruation. The women who belonged lower socioeconomic status were 9.2 times more likely to have poor practices when compared with women belonging to the upper socioeconomic status (adjusted OR [AOR] = 9.27, 95% CI: 4.7–18.03). Respondents who were illiterate were also 9.3 times more likely to have poor practices, as compared to those who have had at least 10 years of formal education (AOR = 9.3, 95% CI: 4.4–19.5). Unemployed women were seen to have poorer practices in contrast to the students, on bivariate analysis but were seen to have no significant difference after adjustment [Table 3].
Table 3.
Predictors of practice of menstrual hygiene among study participants
Menstrual problems related to hygiene
Out of the total 715 study participants, a total of 55 (7.7%) had one or more problem, after menstrual bleeding. Most common problem reported was genital rashes and genital itching (56.4% and 34.5%, respectively). Burning micturition following menstrual bleeding was also reported in 5 (9.1%) of women having problems [Figure 1].
Figure 1.
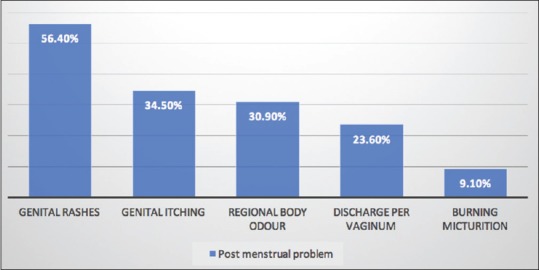
Postmenstrual problems among the study participants
Discussion
In this study, majority of the women (81.7%) had good menstrual hygiene practices. The findings of the study are similar to the studies conducted in Ethopia and Northwest Nigeria which were 90.9% and 88.7% while the proportion was much higher than studies conducted in Western Ethiopia and Jammu and Kashmir, India (3.1% and 39.9%, respectively).[5,9,10,11]
In this study, majority of study participants, i.e., 91.3% were using sanitary napkins as the soakage material which was much higher than the proportion seen in villages of Madhya Pradesh and Chhattisgarh found that 89% of the respondents use cloth as absorbents, 2% used pieces of cotton, 7% used sanitary napkins, and 2% used ash.[12] In another study in Nepal showed that 33% of girls used disposable sanitary pads, 40% used new cloth whereas 26% used old piece of cloth.[13] A study conducted in Delhi, in a similar age group, showed that 28.3% of the women were using sanitary napkins, 11.4% were using cloth, and the rest 60.3% were using both cloth and sanitary napkins.[14] The higher proportion of women using sanitary napkins in our study might attributable to a better socioeconomic and educational status.
In the current study, 93% of study participants had satisfactory frequency of changing of soakage material as compared to 70% in a study in Nigeria.[15] In our study, 32.7% of study participants washed genitals every time after micturition while the study in Nigeria found that 66% washed external genitalia with soap and water, and 83.5% would wash in Western Ethopia.[11]
In the present study, the disposal of soakage material was found to be unsatisfactory among 9.5% of study participants, i.e., either flushing the soakage material in the toilets or throwing them uncovered in an open park. In a study, in rural Pakistan,[3] (2011) 60% of the teachers demanded safe disposal equipments and 48% mothers demanded for special waste bins.[16] In our study, satisfactory bathing practices during menstruation were seen in 86.7% of study participants.
In our study, 7.7% of women had one or more postmenstrual problems. The most common problem faced was seen to be genital rashes (56.4%), followed by genital itching (34.5%), regional body odor (30.9%), discharge per vaginum (23.6%), and burning micturition (9.1%). These problems are less reported as they cause a short-term inconvenience, and usually, do not have a long-term affect.
The limitation of this study was the cross-sectional nature of data that could obscure the causal effect of different factors and it lacks qualitative data. The study has addressed the issue of menstrual hygiene, which is still associated with taboo and various myths, and might have some social desirability bias.
Conclusions
Menstrual hygiene practices determine the short-term inconvenience and are often a cause for discomfort. Social marketing of good quality, low-cost sanitary napkins at accessible outlets, provision for adequate water supply, vending machines for low-cost sanitary napkins, privacy and wall-mounted incinerators for disposal in schools, workplaces, and public places would go a long way in improving the menstrual hygiene and help them in securing healthy lifestyle. Women should be empowered by providing essential services for menstrual management and disposal which is scientifically sound, accessible, and at cost that the community and country can afford. Community needs assessment should also include the menstrual needs of women and not make them the vulnerable group.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Kasper DL, Fauci AS, Hauser SL, Longo DL, Jameson JL, Loscalzo J. Harrison's Principles of Internal Medicine. 18th ed. United States of America: The McGraw-Hill Companies; 2012. [Google Scholar]
- 2.Ten VT. Menstrual Hygiene: A Neglected Condition for Achievement of Several Millenium Development Goals. [Last accessed on 2017 Jan 15]. Available from: http://www.eepa.be/wcm/dmdocuments/BGpaper_Menstrual-Hygiene.pdf .
- 3.Water Aid: Menstrual Hygiene and Management an Issue for Adolescent School Girls. 2009. Mar, [Last accessed on 2017 Jan 15]. Available from: http://www.wateraid.org/nepal .
- 4.Narayan KA, Srinivasa DK, Pelto PJ, Veerammal S. Puberty rituals, reproductive knowledge and health of adolescent schoolgirls in South India. Asia Pac Popul J. 2001;16:225–38. [Google Scholar]
- 5.Dhingra R, Kumar A, Kour M. Knowledge and practices related to menstruation among tribal (Gujjar) adolescent girls. Ethno Med. 2009;3:43–8. [Google Scholar]
- 6.Kansal S, Singh S, Kumar A. Menstrual hygiene practices in context of schooling: A Community study among rural adolescent girls in Varanasi. Indian J Community Med. 2016;41:39–44. doi: 10.4103/0970-0218.170964. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Das P, Baker KK, Dutta A, Swain T, Sahoo S, Das BS, et al. Menstrual hygiene practices, WASH access and the risk of urogenital infection in women from Odisha, India. PLoS One. 2015;10:e0130777. doi: 10.1371/journal.pone.0130777. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Dasgupta A, Sarkar M. Menstrual hygiene: How hygienic is the adolescent girl? Indian J Community Med. 2008;33:77–80. doi: 10.4103/0970-0218.40872. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Lawan UM, Yusuf NW, Musa AB. Menstruation and menstrual hygiene amongst adolescent school girls in Kano, Northwestern Nigeria. Afr J Reprod Health. 2010;14:201–7. [PubMed] [Google Scholar]
- 10.Teklemariam G. Practice of menstrual hygiene and associated factors among female Mehalmeda high school students in Amhara Regional State, Ethiopia. Sci J Public Health. 2014;2:189–95. [Google Scholar]
- 11.Upashe SP, Tekelab T, Mekonnen J. Assessment of knowledge and practice of menstrual hygiene among high school girls in Western Ethiopia. BMC Womens Health. 2015;15:84. doi: 10.1186/s12905-015-0245-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Fernandes M. Freedom of Mobility: Experiences from Villages in the States of Madhya Pradesh & Chhattisgarh India. 2010. Feb, [Last accessed 2016 Aug 22]. Available from: http://www.wsscc.org/sites/default/files/publications/fernandes_wateraid_india-freedom_of_mobility.pdf .
- 13.Khisro SS, Rahman AU. Water Aid. Is Menstrual Hygiene and Management an Issue for Adolescent School Girls: A Comparative Study of Four Schools in Different Settings in Nepal. 2009. [Last accessed on 2013 Apr 06]. Available from: http://www.wsscc.org/sites/default/files/publications/khisro-rahman-mhm_pakistan_2012.pdf .
- 14.Baridalyne N, Reddaiah VP. Menstruation: Knowledge, beliefs and practices of women in the reproductive age group residing in an urban resettlement colony of Delhi. Health Popul. 2004;27:9–16. [Google Scholar]
- 15.Oche MO, Umar AS, Gana GJ, Ango JT. Menstrual health: The unmet needs of adolescent girls’ in Sokoto, Nigeria. Sci Res Essays. 2012;7:410–8. [Google Scholar]
- 16.Khisro SS, Rahman AU. Paving Way for Menstrual Hygiene Management in Rural Pakistan. 2012. [Last accessed 2016 Aug 22]. Available from: http://www.wsscc.org/sites/default/files/publications/khisro-rahman-mhm_Pakis .