

1. Introduction
Urogenital sarcoidosis is very rare. To date, only about 60 cases have been described in the literature.1 This corresponds to only 0.2% of all cases of sarcoidosis diagnosed. When the urogenital system is affected, it is usually the epididymis that is involved, followed by the testis and vas deferens.2 Sarcoidosis─also known as Boeck's sarcoid or Schaumann-Besnier disease─is a rare chronic disorder (prevalence of 1–40 per 100,000 inhabitants) characterised by non-necrotising, epitheloid cell granulomas occurring in different organs.3 The aetiology is still unclear, with the onset of disease typically in young adults. Familial clustering is seen in 5–19% of cases, which is why a significant genetic background is assumed.4,5 The clinical picture can take on very different forms, since basically any organ can be involved. It is often a chance finding made during other diagnostic procedures.3
2. Case presentation
A 29-year-old man presented with lumps in the right testis felt by chance. Urological history otherwise unremarkable. At ultrasound, the palpable masses were visualized as spermatoceles, and both epididymes were normal. On both sides, the testicular tissue showed scattered hypoechogenic foci of about 2 mm diameter; perfusion was otherwise normal (Fig. 1). Laboratory tests were negative for tumour markers and showed no signs of inflammation. A spermiogram showed teratozoospermia.
Fig. 1.

Ultrasound image of the testis with sarcoidal foci; dist 1. 2.17mm, dist 2: 2.01 mm.
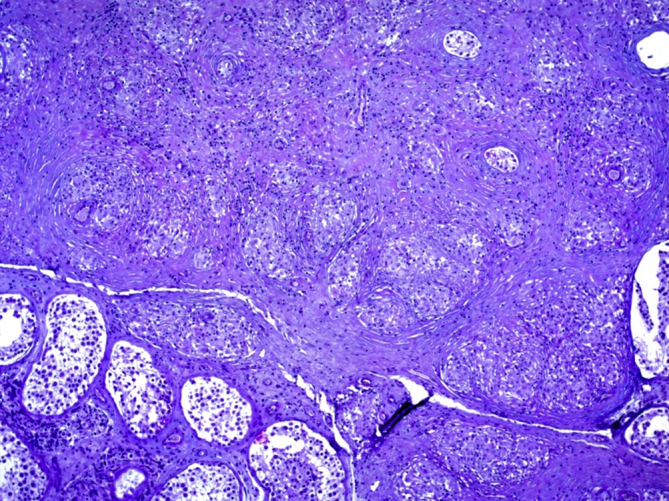
The patient was on treatment with topical cortisone for chronic bilateral uveitis of unclear origin, a suspected diagnosis of Boeck's sarcoid (sarcoidosis) was made, and a thoraco-abdomino-pelvic CT was performed. This showed fine nodular changes in the lungs, mediastinal and bihilar lymphadenopathy compatible with type II sarcoidosis. Histological findings in a testicular biopsy confirmed the suspected diagnosis (Fig. 2, Fig. 3). The patient had no family history of sarcoidosis. From a urological point of view, no active treatment was deemed necessary at the time of writing. A second spermiogram was recommended because of the teratozoospermia, but the patient said he would not have this done unless he decided to have children.
Fig. 2.
Epitheloid cell granulomas of sarcoidosis, mag. 50x.
Fig. 3.

Epitheloid cell granulomas of sarcoidosis, mag. 200x.
3. Discussion
Histological investigations are conducted in patients with suspected urogenital sarcoidosis to confirm the diagnosis and exclude malignancy at the same time. If the patient wishes to have children, the fertility should be investigated in a spermiogram since impaired sperm quality has been reported. Systemic corticosteroid therapy causes the typical space-occupying granuloma of sarcoidosis to regress, enabling the sperm quality to be considerably improved.2 Differential diagnoses to be excluded when investigating urogenital sarcoidosis are TB, malignant lymphoma, syphilis, and testicular tumour.
4. Conclusion
Testicular sarcoidosis is very rare. Ultrasound shows small hypoechogenic foci in the testicular tissue. This disease typically occurs in young adults and the aetiology is still unclear. A testicular biopsy should be taken to confirm the diagnosis and exclude malignancy.
Conflicts of interest
None.
Acknowledgment
Thanks to Alistair Reeves for editing the text.
Contributor Information
Christa Babst, Email: christa.babst@kssg.ch.
Alberto Piller, Email: alberto.piller@kssg.ch.
Jürg Boesch, Email: dr.boesch@hin.ch.
Hans-Peter Schmid, Email: hans-peter.schmid@kssg.ch.
References
- 1.Reineks E.Z., MacLennan G.T. Sarcoidosis of the testis and epididymis. J Urol. 2008;179:1147. doi: 10.1016/j.juro.2007.12.012. [DOI] [PubMed] [Google Scholar]
- 2.Pravin K., Rao M.D., Edmund S., Sabanegh M.D., Jr. Genitourinary sarcoidosis. Cleveland Clinic. Rev Urol. 2009;11:108–113. [PMC free article] [PubMed] [Google Scholar]
- 3.Finger R., Rodriguez R., Schönegg R., Kluckert T., Brutsche M. Sarkoidose: ein klinisch orientierter Überblick. Schweiz Med Forum. 2013;13:265–270. [Google Scholar]
- 4.McGrath D.S., Daniil Z., Foley P. Epidemiology of familial sarcoidosis in the UK. Thorax. 2000;55:751–754. doi: 10.1136/thorax.55.9.751. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Newman L.S., Rose C.S., Maier L.A. Sarcoidosis. N Engl J Med. 1997;336:1224–1234. doi: 10.1056/NEJM199704243361706. [DOI] [PubMed] [Google Scholar]