

Abstract
Neurosyphilis (NS) is an important component of central nervous system diseases among HIV-infected patients. However, its characteristics are not very clear. A retrospective analysis of clinical and laboratory findings was performed in 92 NS patients with HIV infection from a tertiary hospital in Shanghai, China. The patients had a median age of 38 years and a median CD4 count of 198 cells/μL. In all, 44.6% (41/92) were diagnosed as asymptomatic NS (ANS), 23.9% (22/92) as syphilitic meningitis, 17.4% (16/92) as cerebrovascular NS, and 14.1% (13/92) as parenchymal syphilis. A quarter of patients (23/92) complicated with ocular syphilis (OS), 60.9% (14/23) of which were ANS. The serum tolulized red unheated serum test (TRUST) titers were ≤1:8 in 15 patients (16.3%), 1:16–1:128 in 51 patients (55.4%), and ≥1:256 in 26 patients (28.3%). Sixty-nine patients (75.0%) had both cerebrospinal fluid (CSF) TRUST and Treponema pallidum particle assay reactive. CSF pleocytosis and protein elevation were found in 58.7% and 53.3% of patients, respectively. Syphilitic meningitis was more likely to present with CSF pleocytosis than ANS (P = .001), cerebrovascular NS (P < .001), and parenchymal NS (P < .001). The proportion of patients with CSF elevated protein was lower in ANS group than that in syphilitic meningitis (P = .003), cerebrovascular NS (P = .001), and parenchymal NS groups (P = .025), and was higher in sero-TRUST titers ≤1:8 group than that in 1:16–1:128 (P = .01) and 1:256–1:1024 groups (P = .005).
This study revealed that ANS was the most common clinical type of NS in HIV-infected patients, which should be considered in HIV and syphilis co-infection patients without neurologic symptoms, especially in those with OS. Different patterns of NS might have different CSF features which may also vary with sero-TRUST titers.
Keywords: AIDS, human immunodeficiency virus, neurosyphilis
1. Introduction
Syphilis and HIV coinfection are common, because they have the same route of transmission, especially in men who have sex with men.[1] Syphilis has a rising trend of incidence and is the most common sexually transmitted infection among HIV-infected persons in China, even in the era of highly active antiretroviral therapy (HAART).[2,3]
Neurosyphilis (NS) can occur at any stage of syphilis, with various clinical presentations, such as cranial nerve dysfunction, meningitis, acute or chronic change in mental status, loss of vibration sense, stroke, and auditory or ophthalmic abnormalities. However, NS may also be asymptomatic. Syphilis infection can impact the natural course of HIV disease[4]; otherwise, HIV infection may shift the clinical manifestations of syphilis, making clinical lesions more apparent, and may accelerate the progression of syphilitic disease.[5] There is a study suggesting that a CD4 cell count of <350 cells/μL is a risk factor for NS[6]. Neurosyphilis is an important component of central nervous system (CNS) diseases in HIV-infected patients. However, the characteristics of NS in HIV-infected patients are not very clear. There were studies showing that concomitant uveitis and asymptomatic NS (ANS) may be more common in HIV-infected persons.[7,8]
Because of its features of “great imitator” or presenting as an asymptomatic infection, the misdiagnosis rate of NS among the HIV population may be high, which may delay the diagnosis and treatment of NS, and cause severe sequelae in these patients.[8,9] Thus, it is of great importance to cognize the disease. In this article, we describe the clinical and laboratory features of 92 NS cases with HIV-infection from the Shanghai Public Health Clinical Center, a tertiary hospital in Shanghai, China.
2. Methods
We retrospectively analyzed data from the clinical records of all HIV-infected patients with the diagnosis of NS admitted to the Shanghai Public Health Clinical Center, affiliated to Fudan University (Shanghai, China) from August 2009, to June 2017. A total of 92 subjects were included in the study, and their clinical and laboratory data were collected, including sex, age, history of syphilis, clinical manifestations, laboratory and imaging materials, and duration of HAART at the time of admission. The study protocols were approved by the Shanghai Public Health Clinical Center Ethics Committee.
HIV infection was diagnosed by anti-HIV antibody test, which was screened by enzyme-linked immunosorbent assay (ELISA) and confirmed by Western blotting. Syphilis was diagnosed with tolulized red unheated serum test (TRUST, Shanghai Rongsheng-biotech, China) and Treponema pallidum particle assay (TPPA, SERODIA-TPPA, Zhu Hai Livzon Diagnostics Inc., China).
According to the 2014 Chinese treatment guideline for syphilis, which recommended that lumbar puncture should be performed in all AIDS patients with syphilis, and the findings of published studies,[10,11] all the newly diagnosed AIDS patients were routinely screened for syphilis in our clinic, and those with positive serologic test results were informed about the risks of NS. Then, lumbar puncture (LP) was carried out after informed consent was obtained.
Lumbar puncture was performed in all the 92 subjects. All of the cerebrospinal fluid (CSF) specimens underwent testing with TRUST and TPPA and were assessed for white blood cell (WBC) count and protein level. As we know, CSF venereal disease research laboratory (VDRL) test is the reference test for the laboratory diagnosis of NS; however, it has low sensitivity and is a complicated and time-consuming test procedure. In addition, there are no commercial VDRL reagents approved by the State Food and Drug Administration for CSF-VDRL examination in China. There are study results suggesting that CSF-TRUST can be considered as an alternative test for NS diagnosis in HIV-negative populations when the CSF-VDRL is not available.[12,13]
Mild CSF pleocytosis and CSF protein elevation may be common in HIV-infected persons who are not receiving HAART, so the criteria for the diagnosis of NS in AIDS patients were rigorously defined as follows in our study: both serum TPPA and TRUST were reactive; the presence of ≥1 of the following abnormal findings: a reactive CSF-TRUST, CSF pleocytosis (CSF WBC ≥20 cells/μL), and elevated protein (>500 mg/L); if CSF-TRUST was nonreactive, there was no evidence of other CNS diseases which can cause CSF pleocytosis or elevated protein. The syphilis stage was determined according to the Centers for Disease Control and Prevention guidelines.[14] In addition, NS was categorized as ANS and symptomatic NS, according to the absence or presence of neurologic symptoms or signs, and the latter involved syphilitic meningitis, cerebrovascular NS, and parenchymal syphilis.
Data were analyzed using SPSS version 22 (IBM Corp., Armonk, NY). Continuous data with normal distribution were expressed as means ± standard deviation (χ ± SD) and compared using t tests; continuous data with skewed distribution were expressed as median (inter-quartile range, IQR) and compared using the Kruskal–Wallis test. Categorical data were expressed as frequencies and percentages and compared using the chi-square (χ2) test. P < .05 was considered to be statistically significant.
3. Results
A total of 92 HIV-infected patients with diagnosis of NS were included in the study. There were 90 male cases (97.8%) and 2 female cases (2.2%). The median age was 38 years (range: 20–71 years, IQR: 29–51 years). Of the 92 patients, 17 (18.5%) had a previous history of syphilis, 14 of whom had been treated with ceftriaxone, azithromycin, doxycycline, or benzathine penicillin, and 3 had received no treatment. Seventy patients (76.1%) were newly diagnosed with HIV infection within 1 year. A similar number were not on HAART at the time of admission. Among the 20 patients already on HAART on admission, 8 cases were given HAART for more than half a year. The median CD4 count of the 92 included patients was 198 cells/μL (range: 1–936 cells/μL, IQR: 71–308 cells/μL). A total of 47 patients (51.1%) had a CD4 count ≤200 cells/μL, 30 patients (32.6%) had a CD4 count of 200 to 350 cells/μL, and 15 patients (16.3%) had a CD4 count ≥350 cells/μL. In addition, 45 patients underwent testing for HIV viral load, with the results of ≥100,000 copies/mL in 33 patients, and <40 copies/mL in 7 patients, who had been exposed to HAART for at least 6 months.
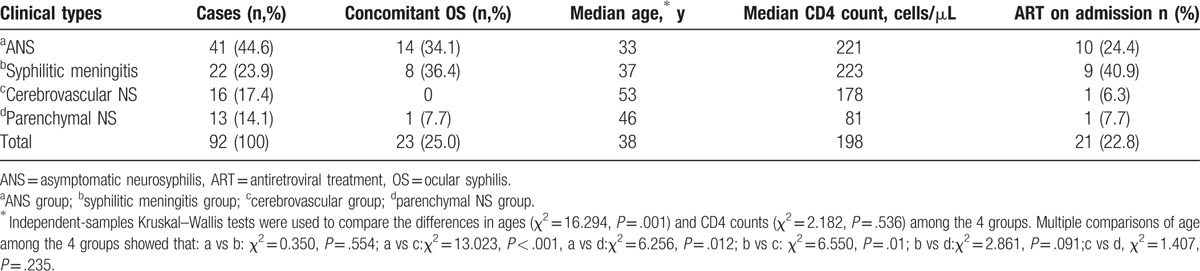
Among the 92 cases of NS in AIDS patients, 41 cases (44.6%) were asymptomatic and 51 cases (55.4%) were symptomatic. A total of 22 (23.9%) patients with symptomatic NS were classified as syphilitic meningitis with presentations of headache (11 cases), vision impairment or loss (7cases), hearing impairment (5 cases), and dizziness (4 cases). Sixteen cases (17.4%) were classified as cerebrovascular NS with presentations of weakness of limbs or hemiplegia (11 cases), dizziness (3 cases), aphasia (4 cases), vision impairment or loss (2 cases), headache (1 case), and cognitive disorder (3 cases). And, 13 (14.1%) were classified as parenchymal syphilis with neurologic manifestations including cognitive impairment (7 cases), mental disorder (4 cases), weakness of limbs (4 cases), ataxia (3 cases), character change (2 cases), and seizure (1 case). Ocular syphilis (OS) was concomitant in 25% (23/92) of cases, including uveitis in 17 cases, retinitis in 3 cases, and optic neuritis in 3 cases. All the cases diagnosed with OS were confirmed by an ophthalmologist. Of the 41 ANS patients, 15 (36.6%) were hospitalized with complaints of ophthalmic abnormalities. Before admission, 16 cases of cerebrovascular NS had been misdiagnosed as “cerebral stroke.” One patient had manifestations of primary syphilis, and 8 patients had manifestations of secondary syphilis. Patients in the cerebrovascular NS group were older than those in the ANS group (P < .001). There were no significant differences in CD4 counts among the ANS, syphilitic meningitis, parenchymal NS, and cerebrovascular NS groups (P = .536) (Table 1).
Table 1.
Distribution of clinical types among 92 NS patients.
All the patients tested both serum TPPA and serum TRUST reactive. The serum TRUST titers were ≤1:8 in 15 patients (16.3%), 1:16–1:128 in 51 patients (55.4%), and ≥1:256 in 26 patients (28.3%). In addition, 69 CSF samples (75.0%) were both TRUST and TPPA reactive. Fifty-four patients (58.7%) had CSF pleocytosis and 49 (53.3%) had CSF protein elevation. Thirty-three patients (35.9%) had both CSF pleocytosis and CSF protein elevation, while 21 (22.8%) had both normal CSF WBC and protein levels (Table 2).
Table 2.
The laboratory findings in 92 NS patients.
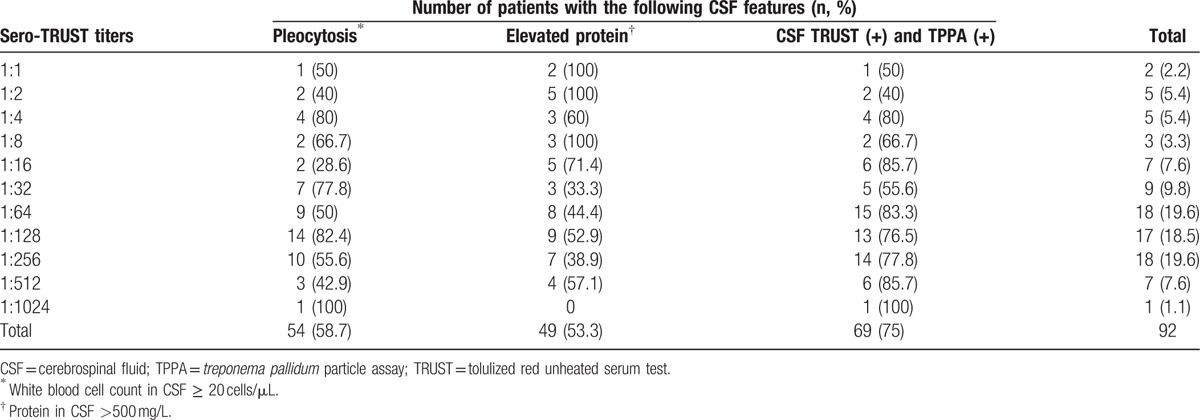
The 92 patients were divided into the following 3 groups based on their sero-TRUST titers: ≤1:8, 1:16–1:128, and 1:256–1:1024. Then, CSF features of the patients with different sero-TRUST titers were analyzed among the 3 groups. The proportion of patients with CSF pleocytosis (χ2 = 0.146, P = .702) and CSF TRUST (+) (χ2 = 0.185, P = .667) was not significantly different. However, there was significant difference in the proportion of patients with elevated CSF protein (χ2 = 7.712, P = .005). Multiple comparisons showed that the proportion of patients with elevated CSF protein in sero-TRUST titers of ≤1:8 group was higher than that in the 1:16–1:128 group (χ2 = 6.726, P = .010) and the 1:256–1:1024 group (χ2 = 7.712, P = .005) (see Table 2).
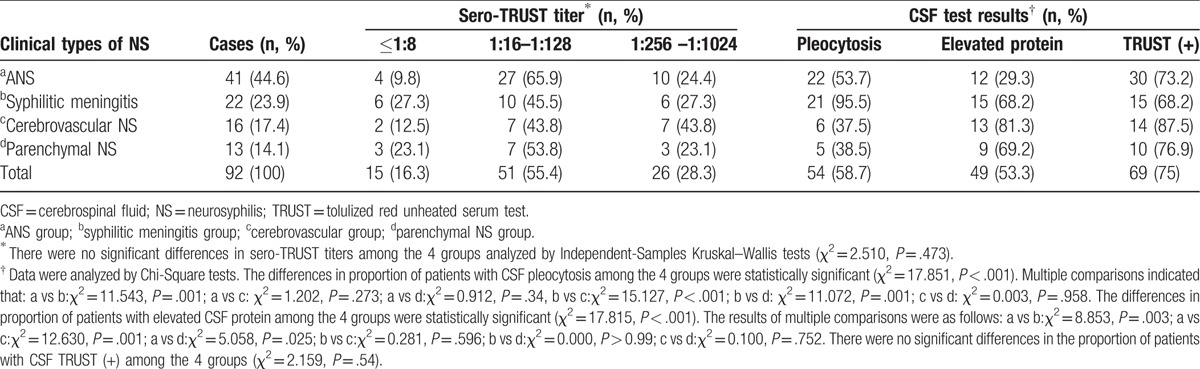
There was no significant difference in sero-TRUST titers among the 4 clinical types of NS groups. CSF test results of the 4 groups revealed that patients with syphilitic meningitis were more likely to have CSF pleocytosis than those with ANS (P = .001), cerebrovascular NS (P < .001), and parenchymal NS (P < .001). The proportion of patients with CSF elevated protein in the ANS group was lower than that in syphilitic meningitis (P = .003), cerebrovascular NS (P = .001), and parenchymal NS groups (P = .025). However, there were no statistically significant differences in the proportion of patients with CSF TRUST (+) among the 4 groups (P = .540) (Table 3).
Table 3.
Laboratory findings in different clinical types of NS patients.
Our study showed that NS could occur in AIDS patients with different CD4 levels and was seen most frequently (51.1%, 47/92) in those with CD4 counts ≤200 cells/μL. There were 15 patients with CD4 counts ≥350 cells/μL, and 8 of them had ANS. There were no significant differences in CD4 counts among the 4 groups of different clinical types of NS (P = .536) (Table 1). In addition, there were no significant differences in sero-TRUST titers (P = .254), proportion of patients with CSF pleocytosis (P = .645), elevated protein (P = .380), and TRUST-reactivity (P = .134), among 3 groups of patients with CD4 counts of ≤200 cells/μL, 201 to 349 cells/μL, and ≥350 cells/μL (Table 4). This revealed that the immune status of AIDS patients might not have influence on the clinical manifestation of NS and CSF features.
Table 4.
Sero-TRUST and CSF test results of NS patients with different CD4 levels.

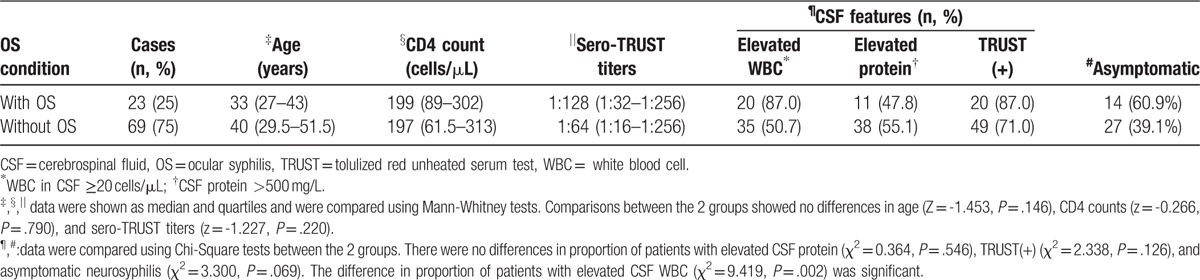
In our study, there were 25% (23/92) of NS cases in AIDS patients combined with OS, including 17 cases of uveitis, 3 cases of retinitis, and 3 cases of optic neuritis. Comparison between the 2 groups (with and without OS) showed that there were no significant differences in age (P = .146), CD4 count (P = .790), sero-TRUST titers (P = .22), proportion of patients with elevated CSF protein (P = .546), and TRUST-reactive (P = .126) patients. However, NS patients with OS were more likely to have CSF WBC elevation than those without OS (P = .002). In addition, patients with OS had a higher proportion of asymptomatic NS (60.9%, 14/23) than those without OS (39.1%, 27/69); however, this difference was not statistically significant (P = .069) (Table 5).
Table 5.
Characteristics of NS patients with and without ocular syphilis.
Without the presence of neurologic signs and symptoms, 41 cases (44.6%) were categorized as having ANS, of which 36.6% (15/41) were hospitalized with complaints of ophthalmic abnormalities, 24.4% (10/41) were routinely screened for syphilis after the diagnosis of HIV-related diseases, 4 cases had rash of secondary syphilis, and 12 patients had neither AIDS- nor syphilis-related symptoms and signs.
A total of 57 patients underwent brain magnetic resonance imaging (MRI). Of these, 40 (70.2%) cases had abnormal findings, including cerebral infarction (CI) or lacunar CI in 22 patients (55.0%), encephalitis and/or meningitis in 6 patients (15.0%), cerebrovascular disease in 5 patients (12.5%), hydrocephalus in 2 patients (5.0%), cerebral atrophy in 2 patients (5.0%), leukoaraiosis in 1 patient (2.5%), and lesion of unknown origin in 6 patients (15.0%).
4. Discussion
Neurosyphilis may occur more frequently in the presence of HIV infection because of immunodeficiency.[15,16] So, it is important to recognize the characteristics of NS in HIV-infected persons. In this study, we described the clinical and laboratory features of NS among HIV-infected persons and found that NS was most commonly seen in those with CD4 count ≤200 cells/μL and sero-TRUST titers ≥1:32; ANS was the most common clinical type of NS, and OS was frequently concomitant; different clinical types of NS might present with different CSF features, which may also vary with sero-TRUST titers.
Neurosyphilis is characterized by clinical polymorphism, and there are significant differences in its epidemiological, clinical, and laboratory profile when HIV-infected patients are compared with HIV-negative patients, as is showed in the published study: HIV-infected patients were younger, presented with a higher frequency of the early forms of NS, higher titers of serum VDRL.[17] In our study, the patients had a median age of 38 years, and nearly half of them (44.6%) were asymptomatic. Patients in the cerebrovascular NS group were older than those in ANS group. This is probably because the older adults might have a longer duration of syphilis infection and are susceptible to cerebrovascular diseases, while the younger people are more likely to have undergone regular screening tests for syphilis, so early diagnosis was possible when they were asymptomatic.
Without the presence of neurologic signs and symptoms, ANS may be frequently missed, especially in HIV-infected patients in whom there was a high proportion of ANS, and CSF abnormalities were necessary for the diagnosis of ANS. There are many studies that had attempted to demonstrate the criteria for performance of LP in HIV-infected patients with syphilis and no neurologic symptoms, which includes rapid plasma reagin assay ≥1:32, CD4 counts ≤350 cell/μL, serologic nonresponse to syphilis therapy or concomitant OS.[7,10,18–21] Also, there are studies that showed CD4 cell counts <350 cells/μL and viral load≥10000 copies/mL were risk factors of NS.[6,11] Our study indicated that NS could occur in AIDS patients with different CD4 levels, most commonly (51.1%) seen in those with CD4 count ≤200 cells/μL, and most of (76.1%) them had the sero-TRUST titers ≥1:32. However, there were 4 cases of ANS with sero-TRUST titers ≤1:8 and 8 cases of ANS with CD4 counts ≥350 cells/μL in this study, which highlights the importance of expansion of indications of LP in AIDS patients. CSF examination may be needed to exclude NS for all the AIDS patients with syphilis regardless of neurologic symptoms, CD4 levels, and the stage of syphilis.
Syphilitic uveitis or other ocular manifestations can be associated with NS. Some studies suggested that OS was likely associated with the CNS involvement, especially in HIV-infected persons with high serum TRUST titers.[16,22] In our study, OS coexisted in 25% of all the patients, and even more in patients with syphilitic meningitis (36.4%). It is suggested that a CSF examination be performed in all instances of OS, even in the absence of clinical neurologic findings.[14]
We analyzed the laboratory findings in 92 NS patients and found that different clinical types of NS might present with different CSF features. Syphilitic meningitis was more likely to have CSF pleocytosis than other clinical types, and the proportion of patients with CSF elevated protein in ANS group was lower than that in other clinical types. We also found that the proportion of patients with elevated CSF protein in sero-TRUST titers of ≤1:8 group was higher than that ≥1:16, which indicated that CSF features may vary with sero-TRUST titers. The reasons for such phenomenon are not clear. Perhaps, it is associated with the duration of syphilis infection, the infection site of the brain, or the immunity of host, which need further study. There were no significant differences in CD4 counts among 4 different clinical types of NS. This indicated that the immune status of AIDS patients may not have influence on the pattern of manifestation of NS.
The imaging manifestations of NS are various. Cerebrovascular NS is characterized by CI in brain MRI images, which may lead to the misdiagnosis of it as “cerebral stroke.” According to a study, the misdiagnosis rate of neurosyphilitic ischemic stroke was as high as 80.95%.[8] In our study, 16 cases of cerebrovascular NS had been misdiagnosed with “cerebral stroke” before admission. So, NS should be considered in the differential diagnosis of CNS diseases occurring in AIDS patients with syphilis, especially in those advanced AIDS patients, in which AIDS-defining diseases frequently occur, including cryptococcal/tubercular meningitis, Toxoplasma gondii encephalitis, progressive multifocal leukoencephalopathy, primary CNS lymphoma, and HIV-associated dementia syndrome.[23] If there are other CNS diseases identified in an HIV/syphilis coinfected patient, CSF WBC and protein level, and neurologic manifestations are not sufficient for the diagnosis of NS. In such circumstances, CSF-VDRL (or CSF-TRUST) reactive is indispensable for making the NS diagnosis.
In all, 18.5% of the NS cases in this study occurred in those with a previous history of syphilis, the reasons for which were considered as follows: the disease progressed to involve the CNS without any treatment or an optimal regimen; the underlying NS was not recognized in the previous course of syphilis, or managed with the corresponding recommended therapy; repeat infection after the previous episode of syphilis. For each syphilitic patient, clinicians should carefully judge whether NS is present, offer the optimal regimen, and clinical and serologic follow-up after treatment. Repeat infections could be detected by retesting after treatment. Treatment failure might be the result of unrecognized CNS infection, and CSF examination can be considered in such situations.[14]
A possible limitation of this study is selection bias of the participants. The subjects included in this study were those who had signed the informed consent form for the performance of LP, and they cannot represent the whole HIV-infected population with syphilis that needs to be examined for the presence of NS. Another limitation is the small sample size. Third, the diagnostic criterion for NS in our study was based on CSF-TRUST test other than the reference test CSF VDRL.
In conclusion, this study revealed that ANS was the most common clinical type of NS in HIV-infected patients, and OS was frequently concomitant. Asymptomatic NS should be considered in HIV and syphilis coinfection patients without neurologic symptoms, especially in those with OS. The clinical manifestations of NS are various and nonspecific; neurosyphilis should be considered in the differential diagnosis of CNS diseases occurring in AIDS patients with syphilis. Different clinical types of NS might present with different CSF features, that may also vary with sero-TRUST titers. Expanding the indications of LP for CSF examination in HIV-infected population with syphilis may be needed to avoid the misdiagnosis of NS, regardless of neurologic symptoms, CD4 levels, and the stage of syphilis.
Footnotes
Abbreviations: NS = neurosyphilis, OS = ocular syphilis, ANS = asymptomatic NS, TRUST = tolulized red unheated serum test, TPPA = Treponema pallidum particle assay, CSF = cerebrospinal fluid, HAART = highly active antiretroviral therapy, CNS = central nervous system, ELISA = enzyme linked immunosorbent assay, LP = lumbar puncture, WBC = white blood cell, VDRL = venereal disease research laboratory, IQR = inter-quartile range, MRI = magnetic resonance imaging, CI = cerebral infarction.
This study was supported by the China's Thirteenth Five-Year major national science and technology projects: AIDS and hepatitis, and other major infectious disease control and prevention (No.2017ZX10202101) and Outstanding Youth Grant from Shanghai Municipal Commission of Health and Family Planning of China (No.20144Y0074).
The authors have no conflicts of interest to disclose.
References
- [1].He H, Wang M, Zaller N, et al. Prevalence of syphilis infection and associations with sexual risk behaviours among HIV-positive men who have sex with men in Shanghai, China. Int J STD AIDS 2014;25:410–9. [DOI] [PubMed] [Google Scholar]
- [2].Chen YC, Liu HY, Li CY, et al. The rising trend of sexually transmitted infections among HIV-infected persons: a population-based cohort study in Taiwan, 2000 through 2010. J Acquir Immune Defic Syndr 2015;68:432–8. [DOI] [PubMed] [Google Scholar]
- [3].Chang YH, Liu WC, Chang SY, et al. Associated factors with syphilis among human immunodeficiency virus-infected men who have sex with men in Taiwan in the era of combination antiretroviral therapy. J Microbiol Immunol Infect 2014;47:533–41. [DOI] [PubMed] [Google Scholar]
- [4].Palacios R, Jimenez-Onate F, Aguilar M, et al. Impact of syphilis infection on HIV viral load and CD4 cell counts in HIV-infected patients. J Acquir Immune Defic Syndr 2007;44:356–9. [DOI] [PubMed] [Google Scholar]
- [5].Musher DM, Hamill RJ, Baughn RE. Effect of human immunodeficiency virus (HIV) infection on the course of syphilis and on the response to treatment. Ann Intern Med 1990;113:872–81. [DOI] [PubMed] [Google Scholar]
- [6].Ghanem KG, Moore RD, Rompalo AM, et al. Neurosyphilis in a clinical cohort of HIV-1-infected patients. AIDS 2008;22:1145–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Tucker JD, Li JZ, Robbins GK, et al. Ocular syphilis among HIV-infected patients: a systematic analysis of the literature. Sex Transm Infect 2011;87:4–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Branger J, van der Meer JT, van Ketel RJ, et al. High incidence of asymptomatic syphilis in HIV infected MSM justifies routine screening. Sex Transm Dis 2009;36:84–5. [DOI] [PubMed] [Google Scholar]
- [9].Liu LL, Zheng WH, Tong ML, et al. Ischemic stroke as a primary symptom of neurosyphilis among HIV-negative emergency patients. J Neurol Sci 2012;317:35–9. [DOI] [PubMed] [Google Scholar]
- [10].Ghanem KG, Moore RD, Rompalo AM, et al. Lumbar puncture in HIV-infected patients with syphilis and no neurologic symptoms. Clin Infect Dis 2009;48:816–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Wang YJ, Chi CY, Chou CH, et al. Syphilis and neurosyphilis in human immunodeficiency virus-infected patients: a retrospective study at a teaching hospital in Taiwan. J Microbiol Immunol Infect 2012;45:337–42. [DOI] [PubMed] [Google Scholar]
- [12].Gu W, Yang Y, Wu L, et al. Comparing the performance characteristics of CSF-TRUST and CSF-VDRL for syphilis: a cross-sectional study. BMJ Open 2013;3:e002204.doi:10.1136/bmjopen-2012-002204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [13].Zhu L, Gu X, Peng RR, et al. Comparison of the cerebrospinal fluid (CSF) toluidine red unheated serum test and the CSF rapid plasmareagin test with the CSF venereal disease research laboratory test for diagnosis of neurosyphilis among HIV-negative syphilis patients in China. J Clin Microbiol 2014;52:736–40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Workowski KA, Bolan GA. Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm Rep 2015;6:1–37. [Google Scholar]
- [15].Zetola NM, Klausner JD. Syphilis and HIV infection: an update. Clin Infect Dis 2007;44:1222–8. [DOI] [PubMed] [Google Scholar]
- [16].Lasso MB, Balcells M, Fernández ME, et al. Neurosyphilis in the patients with and without HIV infection: description and comparison of two historical cohorts. Rev Chilena Infectol 2009;26:540–7. [PubMed] [Google Scholar]
- [17].Gitaí LL, Jaláli PS, Takayanagui OM. Neurosyphilis in the age of AIDS: clinical and laboratory features. Neurol Sci 2009;30:465–70. [DOI] [PubMed] [Google Scholar]
- [18].Chan DJ. Syphilis and HIV: when is lumbar puncture indicated? Curr HIV Res 2005;3:95–8. [DOI] [PubMed] [Google Scholar]
- [19].Marra CM, Déjà vu. All over again: when to perform a lumbar puncture in HIV-infected patients with syphilis. Sex Transm Dis 2007;34:145–6. [DOI] [PubMed] [Google Scholar]
- [20].Libois A, De Wit S, Poll B, et al. HIV and syphilis: when to perform a lumbar puncture. Sex Transm Dis 2007;34:141–4. [DOI] [PubMed] [Google Scholar]
- [21].Marra CM, Maxwell CL, Smith SL, et al. Cerebrospinal s. J Infect Dis 2004;189:369–76. [DOI] [PubMed] [Google Scholar]
- [22].Lee SY, Cheng V, Rodger D, et al. Clinical and laboratory characteristics of ocular syphilis: a new face in the era of HIV co-infection. J Ophthalmic Inflamm Infect 2015;5:26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [23].Panel on Opportunistic Infections in HIV-Infected Adults and Adolescents. Guidelines for the prevention and treatment of opportunistic infections in HIV-infected adults and adolescents: recommendations from the Centers for Disease Control and Prevention, the National Institutes of Health, and the HIV Medical Association of the Infectious Diseases Society of America. Available at http://aidsinfo.nih.gov/contentfiles/lvguidelines/adult_oi.pdf. [Google Scholar]