

Abstract
Context:
Root canal anatomy is evaluated using different methodologies.
Aims:
The aim of this study is to evaluate and classify root canal morphology and dentin thicknesses (DT), comparing radiographic and micro-computed tomography (CT) analysis.
Materials and Methods:
Canal diameter and DT of mandibular incisors (n = 520) were evaluated using digital radiographs in buccolingual (BL) and mesiodistal (MD) directions. The diameter ratio (DR) BL/MD was classified: flattened (FL, DR >4); oval (OV, 2≤ DR ≥4); rounded (RN, 1.1< DR >2); round (RO, 0.9≤ DR ≥1.1); and with BL flatness (BL, DR <0.9). OV (n = 110) were subjected to micro-CT. DT and DR were evaluated at 3, 6, and 9 mm. ANOVA, Tukey, and paired Wilcoxon tests (P < 0.05) were used.
Results:
Radiographic classification was 23.3% FL, 41.3% OV, 27.3% RN, 4.5% RO, and 3.6% BL. DT was similar. Radiographic DT at 3 and 9 mm was greater than micro-CT (P < 0.05) and was similar at 6 mm (P > 0.05). DR differed between the analyses. Oval canals were predominant at all levels radiographically and at 9 and 6 mm in micro-CT analysis, with greater variation at 3 mm.
Conclusion:
Oval root canals are predominant in mandibular incisors at 9 mm. Radiographic DT is larger than observed in micro-CT at 3 and 9 mm, and the classification differed in each root level. The classification at 9 mm is indicated.
Keywords: Endodontics, radiography, root canal anatomy, X-ray microtomography
INTRODUCTION
Root canal morphology is evaluated using different methodologies, such as staining and clearing techniques, radiographic, cone-beam computed tomography (CT),[1] or microtomographic analysis.[2,3,4] Mandibular incisors are commonly used for different analysis, especially considering the number of main and accessory canals.[5] Mandibular incisors are also widely used in endodontic studies because they have flattened and oval canals. The cross-section morphology of the root canal is classified according to the radiographic measurement of the mesiodistal (MD) and buccolingual (BL) diameter ratio (DR):[6,7] round (similar DR), oval (DR two times larger), long oval (DR up to 4 times larger), flattened (DR 4 or more), and irregulars (undefined values).[7] It has been defined based on different root levels[7] or sections at 1, 2, 3, 4, and 5 mm from the apex (DR ≥2).[6]
Mandibular incisors commonly have a single canal[8] and high prevalence of oval root canal[2,3] been extensively used to the evaluation of root canal cleaning and preparation using different instruments.[9,10] Microtomographic analysis has also been widely used to evaluate this morphology, such as root canal preparation, root canal filling, and retreatment protocols.[11,12]
Dentin thickness (DT) of root walls at the different levels is important to the planning of root canal preparation maintaining the root strength.[13] Roots with a MD dimension smaller than the BL are more susceptible to fracture, as observed in maxillary premolars, mesial roots of mandibular molars, and mandibular incisors.[14] Moreover, planning for intracanal posts[15] depends on evaluating the remaining DT.[16] This thickness may be evaluated radiographically,[6] with possible occurrence of distortions due to superimposition of root wall structures. Evaluation using microtomographic analysis obtains precise measurements of this thickness.[2,17]
Considering the importance of root canal morphology and DT of root walls for research protocols and clinical procedures, the aims of this study are to evaluate and classify the root canal shape and dentin wall thicknesses of mandibular incisors and compare radiographic and micro-CT analyses.
MATERIALS AND METHODS
Five hundred and twenty mandibular incisors approved by the Ethics Committee (#699.061) were radiographed (Kodak RVG 6100 Atlanta, GA, USA) in the BL and MD directions to select teeth with single canal, absence of endodontic treatment, and without extensive restorations.
Radiographic analysis
The images obtained were analyzed by CTAn (V1.11.8; SkyScan, Belgium) software, measuring the root canal diameter in the buccal-lingual (BL) and mesiodistal (MD) direction (n = 520). These measurements were made at 9 mm from the apex (middle third) to classify the root canal shape. Using the BL/MD diameter ratio (DR), different classifications were obtained: flattened canals (FL, DR >4); and oval canals (OV, 2≤ DR ≥4) according to Jou et al.,[7]; and an additional classification, with rounded canals (RN, 1.1< DR >2); round (RO, 0.9≤ DR ≥1.1), and with flattening BL (BL, DR <0.9) [Figure 1a].
Figure 1.

(a) Buccolingual and mesiodistal radiographic images (I). Analysis of mesiodistal and buccolingual diameter (D) of root canal at 9 mm from the apex (II). Classification according to the observed diameter ratio buccolingual/mesiodistal (III). (b) Radiographic images (I) used to analysis the dentin thickness of mesial (M) and distal (D) (II) dentin walls and e buccal (B) and lingual (L) (III) at 3 and at 9 mm from the apex
Microtomographic and radiographic analysis
At this stage, a hundred and ten mandibular incisors radiographically classified as oval were subjected to microtomographic scannings using the micro-CT scanner (SkyScan 1176, Bruker-microCT, Kontich, Belgium). The scanning parameters were based on a pilot study and were performed at 70 kV, 353 mA and 360° rotation, and a 0.5° rotation step, resulting in an image with a 17.42-μm voxel size, filter made of aluminum, and duration time of 23 min 14 s.
Thereafter, the images were reconstructed using NRecon (V1.6.4,7; SkyScan, Belgium) software. The adjustment of reconstruction parameters was made to suppress noises. Fine-tuning function enabled set artifact correction values, such as Gaussian filter, beam hardening correction, postalignment, and ring artifact correction.
The resulting images were processed in Data Viewer (V1.5.1.2; SkyScan, Belgium) software, to obtain sagittal sections and were analyzed with CTAn (V1.11.8; SkyScan, Belgium) [Figure 2a]. The BL/MD DR and DT of mesial and distal walls of the samples were measured at 3, 6, and 9 mm from the apex [Figure 2b], as previously described. These 110 samples were also evaluated radiographically again, with the DR and DT being measured at 3, 6, and 9 mm from the apex.
Figure 2.

(a) Diameter mesiodistal (a1, a3, a5) and buccolingual (a2, a4, a6) evaluated in radiographic images (red lines). Diameter ratio (b1, b2, b3) observed (blue lines) in micro CT images at 3 (I), 6 (II) e 9 (III) mm from the apex. (b) Images obtained using CTAn software and measurements of dentin thickness (white lines) of mesial (M) e distal (D) dentin walls at 3 (IV), 6 (V), and 9 (VI) mm from the apex. Different letters in each column indicate statistically significant differences (P < 0.05)
Statistical analysis
The data obtained were submitted to the ANOVA and Tukey tests and Wilcoxon paired correlation test, at a 5% level of significance.
RESULTS
Radiographic analysis
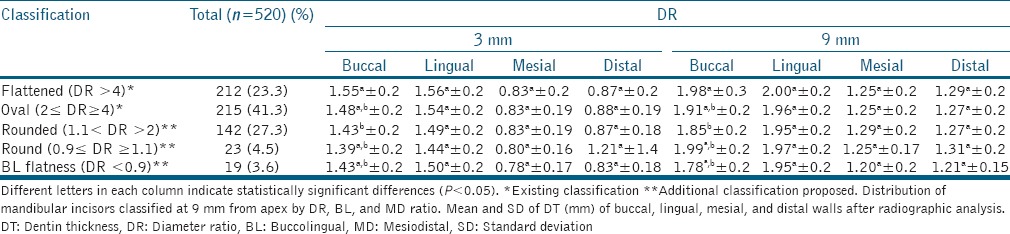
The 520 mandibular incisors evaluated at 9 mm from the apex were classified: 121 (23.3%) flattened; 215 (41.3%) oval; 142 (27.3%) rounded; 23 (4.5%) round; and 19 (3.6%) with BL flatness. As regards the dentin wall measurements, the thicknesses at 3 and 9 mm from the apex were similar between the different classifications, except for the buccal wall that was greater for flattened canals compared with those considered rounded, both at 3 and at 9 mm [Table 1].
Table 1.
Radiographic evaluation of diameter ration (DR) of mandibular incisors (n=520) with single canal
Microtomographic and radiographic analysis
A hundred and ten samples radiographically considered oval were evaluated. A comparison between the values obtained radiographically and by micro-CT analysis was performed. The radiographic DT was greater than that obtained by micro-CT for the mesial and distal walls at 3 and 9 mm (P < 0.05) and was similar at 6 mm (P > 0.05) [Table 2].
Table 2.
Analyses of the dentin thickness and canal diameters using radiographic and microtomographic measurements

With regard to root canal diameters obtained in measurements at 3, 6, and 9 mm from the apex, all the radiographic and micro-CT analyses presented statistically significant difference for BL and MD diameter values (P < 0.05), with exception of the BL diameter at 3 mm, that showed no statistically significant difference (P > 0.05) [Table 2].
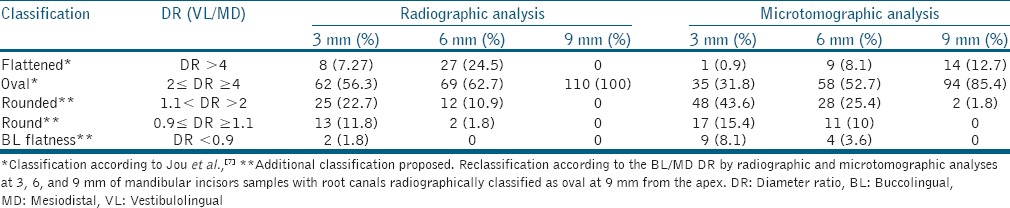
Based on the values for the DR at the 3 root levels, the authors reclassified the samples considered oval by the radiographic examination at 9-mm level. Therefore, using micro-CT at 9-mm level, the classification was: 94 (85.4%) oval; 14 (12.7%) flattened; and 2 (1.8%) rounded. By the micro-CT analysis at 6 mm: 58 (52.7%) were oval; 9 (8.1%) flattened; 28 (25.4%) rounded; 11 (10%) round; and 4 (3.6%) with BL flatness. At 3 mm, 35 (31.8%) were considered oval; 1 (0.9%) flattened; 48 (43.6%) rounded; 17 (15.4%) round; and 9 (8.1%) with BL flatness. Radiographically at 9 mm, the 110 samples were classified as oval. However, at 6 mm, 69 (62.7%) were considered oval; 27 (24.5%) flattened; 12 (10.9%) rounded; and 2 (1.8%) round, and at 3 mm, 62 (56.3%) were considered oval; 8 (7.27%) flattened; 25 (22.7%) rounded; 13 (11.8%) round; and 2 (1.8%) with BL flatness [Table 3].
Table 3.
Reclassification of diameter ratio (DR) in oval canals using radiographic and microtomographic measurements
DISCUSSION
In the present study, high variability of the DR BL/MD was observed using radiographic measurements at 9 mm from the apex. This DR showed values ranging from 0.9 to values higher than 4. The root canal morphology is classified by means of various criteria, and it is normally considered oval when the DR values are over 2.[9] Therefore, considering this variability and the need for standardizing the planning of different studies in endodontics, it was considered: flattened (FL, DR >4) and oval (OV, 2≤ DR ≥4) canals, as previously described,[7] as well as an additional classification: rounded (RN, 1.1< DR >2), round (RO, 0.9≤ DR ≥1.1), and BL flatness (BL, DR <0.9).
The root level used to determine the classification of cross-section morphology of the root canal is variable and frequently not specifically described.[14,18,19] The authors observed high variability in the values for DR used in teeth selection,[12,20] as well as divergence between the classification of oval or flattened canals.[10,13] This study used specific values to determine the points of measurement for the analysis (3, 6, and 9 mm) to achieve more standardized definition for the different types of studies. Cross-section morphology of the root canal considered oval after radiographic classification at 9 mm from the apex presented other classifications at 3 and 6 mm from the apex, corroborating with previous studies.[17] Moreover, radiographic and microtomographic analyses showed no correlation, demonstrating different classifications between them. Many studies make this measurement in the apical third[4,13] since an oval morphology is commonly found at 3 mm from the apex. However, at this distance, the authors found higher percentages of samples considered rounded (43.6%) in micro-CT, corroborating with previous study.[2] At 9 mm, a higher correlation to the DR was obtained, with lower variability and a higher prevalence of oval morphology at this point [Table 3]. This higher prevalence of oval classification for mandibular incisors was also reported, varying from 76.2% at 3 mm;[2] 56% at 5 mm;[6] or even 88% from 3 to 5 mm.[11]
In the present study, the MD canal diameter at 3 mm was 0.22 mm, corroborating with previous study a constant MD distance in the 3 mm apical measurements, with values between 0.20 and 0.25 mm.[2] In the remaining levels of measurement (6 and 9 mm), the MD and BL diameters showed values increasing progressively in the coronal direction [Table 2]. These variations in diameter significantly interfere in the BL/MD DRs of root canals, influencing the distribution of classifications [Table 3].
The mesial and distal DT showed values between 0.9 and 1.0 at 6 mm level, without difference between the radiographic and microtomographic analyses. However, the measurements at 3 and 9 mm showed values between 0.71 and 1.26, with difference between them [Table 2]. The analyses using micro-CT show values closer to real[21] since they eliminate the superimposition of structures. Moreover, it is possible to observe the flattening dentin wall, especially evaluating the sagittal section [Figure 2]. In spite of being a simpler method, radiographic evaluation may show a larger thickness than that obtained by micro-CT, due to this superimposition of structures and distortions of the image. No flattened areas (apical or middle third) were shown in the radiographs, and this may influence planning of apical instrumentation or preparation for intracanal posts. Although radiographic is clinically the most widely used method, microtomography is suggested as a tool for the selection of samples to be used in different studies, especially when specific morphologies are selected, standardizing results with high clinical relevance. A poorer image detail was observed, for example, to cone-beam CT in comparison to micro-CT, with difference when used in the different root thirds.[17]
The root wall morphology and structure has a direct influence on planning of root canal preparation[13] and intracanal posts.[15] An incorrect planning may favor microcracks or diminish the strength of the root. Smaller DT may increase susceptibility root fracture.[22] Although fractures predominantly occur in the BL direction,[23] a considerable number of fractures in the MD direction were observed,[24] with different types of cracks and DT values (DT ≤0.3 or DT ≥0.3). Therefore, the proximal DT observed [values ≥0.3 – as demonstrated in Table 2] may be used for planning studies about the influence of it on apical instrumentation of the root canal or the use of intracanal posts.
CONCLUSION
Oval root canals are predominant in mandibular incisors with a single canal, after radiographic and micro-CT analysis at 9 mm from the apex. In radiographic analysis, DT is similar between the different classifications (i.e., oval, round, and flattened). However, when comparing the radiographic and micro-CT analysis of oval canals, the radiographic mesial and distal thickness is greater at 3 and 9 mm, and the DR values vary according to the root level. The classification at 9 mm from the apex showed greater proximity between the analyses and must be indicated for root canal classification.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Lin Z, Hu Q, Wang T, Ge J, Liu S, Zhu M, et al. Use of CBCT to investigate the root canal morphology of mandibular incisors. Surg Radiol Anat. 2014;36:877–82. doi: 10.1007/s00276-014-1267-9. [DOI] [PubMed] [Google Scholar]
- 2.Milanezi de Almeida M, Bernardineli N, Ordinola-Zapata R, Villas-Bôas MH, Amoroso-Silva PA, Brandão CG, et al. Micro-computed tomography analysis of the root canal anatomy and prevalence of oval canals in mandibular incisors. J Endod. 2013;39:1529–33. doi: 10.1016/j.joen.2013.08.033. [DOI] [PubMed] [Google Scholar]
- 3.Leoni GB, Versiani MA, Pécora JD, Damião de Sousa-Neto M. Micro-computed tomographic analysis of the root canal morphology of mandibular incisors. J Endod. 2014;40:710–6. doi: 10.1016/j.joen.2013.09.003. [DOI] [PubMed] [Google Scholar]
- 4.Freire LG, Gavini G, Cunha RS, Santos Md. Assessing apical transportation in curved canals: Comparison between cross-sections and micro-computed tomography. Braz Oral Res. 2012;26:222–7. doi: 10.1590/s1806-83242012000300007. [DOI] [PubMed] [Google Scholar]
- 5.Vertucci FJ. Root canal anatomy of the mandibular anterior teeth. J Am Dent Assoc. 1974;89:369–71. doi: 10.14219/jada.archive.1974.0391. [DOI] [PubMed] [Google Scholar]
- 6.Wu MK, R'oris A, Barkis D, Wesselink PR. Prevalence and extent of long oval canals in the apical third. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000;89:739–43. doi: 10.1067/moe.2000.106344. [DOI] [PubMed] [Google Scholar]
- 7.Jou YT, Karabucak B, Levin J, Liu D. Endodontic working width: Current concepts and techniques. Dent Clin North Am. 2004;48:323–35. doi: 10.1016/j.cden.2003.12.006. [DOI] [PubMed] [Google Scholar]
- 8.Boruah LC, Bhuyan AC. Morphologic characteristics of root canal of mandibular incisors in North-East Indian population: An in vitro study. J Conserv Dent. 2011;14:346–50. doi: 10.4103/0972-0707.87195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Siqueira JF, Jr, Alves FR, Almeida BM, de Oliveira JC, Rôças IN. Ability of chemomechanical preparation with either rotary instruments or self-adjusting file to disinfect oval-shaped root canals. J Endod. 2010;36:1860–5. doi: 10.1016/j.joen.2010.08.001. [DOI] [PubMed] [Google Scholar]
- 10.de Melo Ribeiro MV, Silva-Sousa YT, Versiani MA, Lamira A, Steier L, Pécora JD, et al. Comparison of the cleaning efficacy of self-adjusting file and rotary systems in the apical third of oval-shaped canals. J Endod. 2013;39:398–401. doi: 10.1016/j.joen.2012.11.016. [DOI] [PubMed] [Google Scholar]
- 11.Paes da Silva Ramos Fernandes LM, Rice D, Ordinola-Zapata R, Alvares Capelozza AL, Bramante CM, Jaramillo D, et al. Detection of various anatomic patterns of root canals in mandibular incisors using digital periapical radiography, 3 cone-beam computed tomographic scanners, and micro-computed tomographic imaging. J Endod. 2014;40:42–5. doi: 10.1016/j.joen.2013.09.039. [DOI] [PubMed] [Google Scholar]
- 12.Crozeta BM, Silva-Sousa YT, Leoni GB, Mazzi-Chaves JF, Fantinato T, Baratto-Filho F, et al. Micro-computed tomography study of filling material removal from oval-shaped canals by using rotary, reciprocating, and adaptive motion systems. J Endod. 2016;42:793–7. doi: 10.1016/j.joen.2016.02.005. [DOI] [PubMed] [Google Scholar]
- 13.Abou El Nasr HM, Abd El Kader KG. Dentinal damage and fracture resistance of oval roots prepared with single-file systems using different kinematics. J Endod. 2014;40:849–51. doi: 10.1016/j.joen.2013.09.020. [DOI] [PubMed] [Google Scholar]
- 14.Rivera ER, Walton RE. Longitudinal tooth fractures: Findings that contribute to complex endodontic diagnoses. Endod Top. 2009;16:82–111. [Google Scholar]
- 15.Cheung W. A review of the management of endodontically treated teeth. Post, core and the final restoration. J Am Dent Assoc. 2005;136:611–9. doi: 10.14219/jada.archive.2005.0232. [DOI] [PubMed] [Google Scholar]
- 16.Alomari QD, Barrieshi KM, Al-Awadhi SA. Effect of post length and diameter on remaining dentine thickness in maxillary central and lateral incisors. Int Endod J. 2011;44:956–66. doi: 10.1111/j.1365-2591.2011.01917.x. [DOI] [PubMed] [Google Scholar]
- 17.Marca C, Dummer PM, Bryant S, Vier-Pelisser FV, Só MV, Fontanella V, et al. Three-rooted premolar analyzed by high-resolution and cone beam CT. Clin Oral Investig. 2013;17:1535–40. doi: 10.1007/s00784-012-0839-5. [DOI] [PubMed] [Google Scholar]
- 18.Arruda MP, Carvalho Junior JR, Miranda CE, Paschoalato C, Silva SR. Cleaning of flattened root canals with different irrigating solutions and nickel-titanium rotary instrumentation. Braz Dent J. 2009;20:284–9. doi: 10.1590/s0103-64402009000400004. [DOI] [PubMed] [Google Scholar]
- 19.Versiani MA, Pécora JD, Sousa-Neto MD. Microcomputed tomography analysis of the root canal morphology of single-rooted mandibular canines. Int Endod J. 2013;46:800–7. doi: 10.1111/iej.12061. [DOI] [PubMed] [Google Scholar]
- 20.Rechenberg DK, Paqué F. Impact of cross-sectional root canal shape on filled canal volume and remaining root filling material after retreatment. Int Endod J. 2013;46:547–55. doi: 10.1111/iej.12027. [DOI] [PubMed] [Google Scholar]
- 21.Balto K, Müller R, Carrington DC, Dobeck J, Stashenko P. Quantification of periapical bone destruction in mice by micro-computed tomography. J Dent Res. 2000;79:35–40. doi: 10.1177/00220345000790010401. [DOI] [PubMed] [Google Scholar]
- 22.Wilcox LR, Roskelley C, Sutton T. The relationship of root canal enlargement to finger-spreader induced vertical root fracture. J Endod. 1997;23:533–4. doi: 10.1016/S0099-2399(97)80316-0. [DOI] [PubMed] [Google Scholar]
- 23.Bellucci C, Perrini N. A study on the thickness of radicular dentine and cementum in anterior and premolar teeth. Int Endod J. 2002;35:594–606. doi: 10.1046/j.1365-2591.2002.00537.x. [DOI] [PubMed] [Google Scholar]
- 24.Sathorn C, Palamara JE, Palamara D, Messer HH. Effect of root canal size and external root surface morphology on fracture susceptibility and pattern: A finite element analysis. J Endod. 2005;31:288–92. doi: 10.1097/01.don.0000140579.17573.f7. [DOI] [PubMed] [Google Scholar]