

Abstract
Aim:
The aim of this study is to compare and to evaluate effect of curing light and curing modes on the nanohybrid composite resins with conventional Bis-GMA and novel tricyclodecane (TCD) monomers.
Methodology:
Two nanohybrid composites, IPS empress direct and charisma diamond were used in this study. Light-emitting diode (LED)-curing unit and quartz-tungsten-halogen (QTH)-curing unit which were operated into two different modes: continuous and soft start. Based on the composite resin, curing lights, and mode of curing used, the samples were divided into 8 groups. After polymerization, the samples were stored for 48 h in complete darkness at 37°C and 100% humidity. The Vickers hardness (VK) of the surface was determined with Vickers indenter by the application of 200 g for 15 s. Three VK readings were recorded for each sample surface both on top and bottom surfaces. For all the specimens, the three hardness values for each surface were averaged and reported as a single value. The mean VK and hardness ratio were calculated. The depth of cure was assessed based on the hardness ratio.
Results:
Comparison of mean hardness values and hardness ratios was done using ANOVA with post hoc Tukey's test.
Conclusion:
Both QTH- and LED-curing units had shown the adequate depth of cure. Soft-start-curing mode in both QTH- and LED-curing lights had effectively increased microhardness than the continuous mode of curing. TCD monomer had shown higher hardness values compared with conventional Bis-GMA-containing resin.
Keywords: Curing modes, polymerization shrinkage, soft start, tricyclodecane
INTRODUCTION
Composite resins have revolutionized modern restorative dentistry mainly because of their esthetic quality and good physical properties. Since they were first developed, many efforts have been made to improve the clinical behavior of these restorative materials. The clinical performance of composite resins is directly related to the degree of monomer conversion after photopolymerization.[1] There are many parameters that influence the degree of polymerization of composite resins such as their composition, shade and translucency, characteristics of the light-curing unit (LCU) used, rate of curing, distance between light-curing tip and restoration surface, duration of photopolymerization, and composite temperature.[2,3] Although various factors might influence the material behavior, composition, light cure unit, and rate of curing are the most important factors related to improvement in the mechanical properties of composite resins.[4,5]
Photopolymerization is of fundamental importance for optimization of the physical and mechanical properties and clinical results of composite material. Inadequate polymerization results in decrease in hardness, bond strength between tooth and the restoration, potential, pulpal damage, greater cytotoxicity, and increase in water sorption and solubility.[1,3] Dentists have a choice of various types of curing lights such as conventional quartz-tungsten-halogen (QTH), light-emitting diode (LED), plasma arc, or laser-curing lights. These lights have different characteristics and claimed advantages, but the most favorable irradiation for photocuring-resin composite restorations has not yet been determined. QTH is the most traditional and most commonly used curing unit. It produces light by incandescence. Filters are needed to restrict the emitted light to the blue region of the spectrum for the polymerization and to reduce the heat energy transferred to the oral structure. With the objective of overcoming limitations inherent to halogen lamps, LED-curing units were introduced. LEDs use a combination of two different doped semiconductors, instead of hot filament. The advantages of the LEDs are they produce less heat; therefore, no cooling fan is required. They are small in size and cordless. Moreover, LEDs can operate for thousands of hours with a constant light output in power and spectrum.[5]
The polymerization of composite resins occurs in two phases: pregel phase and postgel phase. During the pregel phase, the organic matrix can flow and undergo molecular rearrangement, compensating the shrinkage forces. During this phase, there is a predominance of linear polymer chains, following which the resin reaches a viscous state, establishing its gel point. The period after the gel point where the resin loses its flowing ability is referred to as the postgel phase. During this phase, the polymerization shrinkage stress is transferred to the tooth restoration interface. To minimize polymerization shrinkage of composite without affecting the degree of conversion, various polymerization modes have been formulated such a soft start, pulse delay, pulse cure, and ramp mode. In soft start mode, curing begins initially at low-light intensity followed by full-light intensity to permit greater flow and stress relief in the composite.[6,7]
During the last decades of composite development, the main advancements were done in the filler system. Only few efforts were made to design new matrix systems. Therefore, the majority of composites rest on the 50 years old Bis-GMA-cross linker matrix. Bis-GMA is a very rigid crosslinker with very high viscosity. Addition of diluents such as TEGDMA and lowering the Bis-GMA part leads to higher shrinkage and shrinkage stresses in the composite. To overcome the shrinkage issue, a complete new crosslinker technology tricyclodecane (TCD) was developed. Several studies have compared the efficacy of QTH LCU with LED LCU using nanohybrid composite resins. However, the curing efficacy of these recently developed nanohybrid, with novel monomer has not been studied extensively with different curing modes. Hence, this study was undertaken to compare the efficacy of polymerization of nanohybrid composite resins cured with QTH, and LED LCUs by different curing modes.
METHODOLOGY
Two nanohybrid-resin composites used for the present study IPS Empress Direct (Ivoclar Vivadent) and Charisma Diamond (Heraeus Kulzer). These resin composites were cured with LED- and QTH-curing units by continuous and soft-start mode. The LED light cure unit used in the study was Bluephase N (Ivoclar Vivadent) which is cordless unit with a light output of 1,200 mW/cm2 and features Polywave Technology. The QTH light cure unit used was Spectrum® 800 (Dentsply) variable intensity-curing light with intensity from 300 mW/cm2 up to 800 mW/cm2. Two different light-curing modes were used for each material: continuous 30 s: 600 mW/cm2 for 30 s; soft-start 30 s: 0–600 mW/cm2 for 5 s + 1200 mW/cm2 for 25 s.
Based on the composite resin, curing light, and method of polymerization used, 80 samples were prepared and divided into 8 groups (10 samples per each group n = 10):
Group 1: IPS empress direct nanohybrid composite cured with QTH-curing light in soft-start mode
Group 2: IPS empress direct nanohybrid composite cured with QTH-curing light in continuous mode
Group 3: IPS empress direct nanohybrid composite cured with LED-curing light in soft-start mode
Group 4: IPS empress direct nanohybrid composite cured with LED-curing light in continuous mode
Group 5: Charisma diamond nanohybrid composite cured with QTH-curing light in soft-start mode
Group 6: Charisma diamond nanohybrid composite cured with QTH-curing light in continuous mode
Group 7: Charisma diamond nanohybrid composite cured with LED-curing light in continuous mode
Group 8: Charisma diamond nanohybrid composite cured with LED-curing light in soft-start mode.
Preparation of samples
Samples were prepared using stainless steel mold with diameter 7 mm and height 2 mm. The molds were placed on a dark opaque paper background covered with a polyester matrix strip and filled with composite. This arrangement minimized the possibility of obtaining artificially higher hardness due to reflection of light. The polyester matrix strip was placed on the top of the filled mold and glass slide was pressed against the film to extrude the excess of material and form a flat surface. The tip of the light guide was placed against the surface of the matrix strip and positioned concentrically with the mold, and the material was then light-cured from the top.
After polymerization, the samples were stored for 48 h in complete darkness at 37°C and 100% humidity. The Vickers hardness (VK) of the surface was determined with a microhardness tester using a Vickers diamond indenter with 200 g load applied for 15 s [Figures 1-4]. Three VK readings were recorded for each sample surface both on top and bottom surfaces. Hardness measurements were not taken at more than 4 mm from the specimen center to avoid any possible effect of the mold on polymerization. For all the specimen, the three hardness values for each surface were averaged and reported as a single value. The mean VK and hardness ratio of the specimens were calculated and tabulated using the formula:
Figure 1.
Vickers indentation of specimen cured with light-emitting diode soft start mode
Figure 4.
Vickers indentation of specimen cured with quartz-tungsten halogen continuous mode
Figure 2.
Vickers indentation of specimen cured with light-emitting diode continuous mode
Figure 3.
Vickers indentation of specimen cured with quartz-tungsten halogen soft-start mode
Hardness ratio = VK of bottom surface/VK of top surface.
The depth of cure was assessed based on the hardness ratio. If bottom: top hardness ratios (B/T ratios) value exceeded 0.8, specimens were considered as adequately polymerized. Comparison of mean hardness values was done using ANOVA with post hoc Tukey's test.
Statistical analysis
All the analysis was done using SPSS version 16 (SPSS Inc. Version 16, Chicago, USA). P < 0.05 was considered statistically significant. Comparison of mean values was done using ANOVA with post hoc Tukey's test [Tables 1, 2 and Chart 1].
Table 1.
Intergroup comparison of Vickers hardness numbers
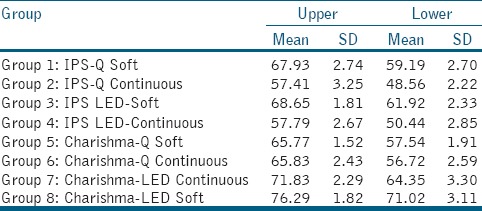
Table 2.
Intergroup comparision of Vickers hardness ratios
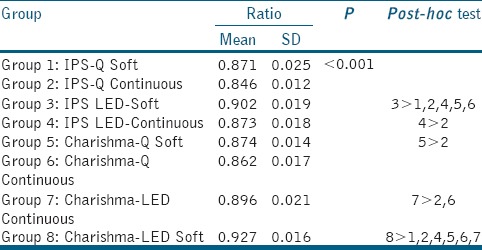
Chart 1.
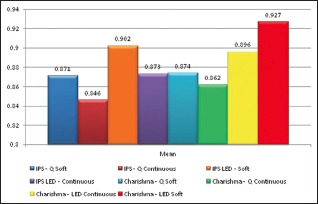
Vickers hardness ratios
DISCUSSION
Adequate polymerization is a crucial factor in obtaining optimal physical properties of composite materials and is related to better clinical performance.[8,9] Although high degree of cure is desirable, it inherently results in shrinkage which is inevitable. The postgel shrinkage results in significant stresses in the surrounding tooth structure and composite tooth bond.[10] These stresses may produce defects in the composite-tooth bond, leading to bond failure, microleakage, postoperative sensitivity, recurrent caries, decreased mechanical properties, and tooth fracture.
With the recent advances in material aspect of the composite resin and curing technologies, the problem of polymerization shrinkage without altering the degree of cure has been proposed. Two general approaches have been followed to overcome the problem of stress concentration and polymerization shrinkage with light-activated resins (1) reduction in volume contraction by altering the chemistry and/or composition of the resin systems and (2) clinical techniques designed to offset the effect of polymerization shrinkage. Intensive research and development efforts are currently in progress to develop resins with low shrinkage and low thermal expansion. With the advancement in the filler technology, composite with reduced shrinkage and thermal expansion were developed. The development in the matrix chemistry led to the invention of new monomers with high degree of conversion, low-shrinkage properties, and enhanced mechanical behavior.
The present study compared the curing efficacy of QTH- and LED-curing units. The QTH-curing unit used in the present study was Spectrum® 800. It is a variable intensity-curing unit by which intensity can be adjusted from 300 mW/cm2 up to 800 mW/cm2 in increments of 50 mW/cm2. This curing unit has high light output power (up to 800 mW/cm2) and Built-in Radiometer. Bluephase N, is cordless LEDlight curing unit with intensity 1,200 mW/cm2 and features Polywave Technology. Polywave technology features a second spectral peak at approximately 410 nm in addition to the peak at approximately 470 nm. The Bluephase N offers 3 programs, high power (1,200 mW/cm2), low power (800 mW/cm2), and soft start where the curing begins at low intensity of 600 mW/cm2 and finishes with high intensity of 1200 mW/cm2.
Several direct and indirect methods can be used to evaluate the degree of polymerization of resin composites. As the direct methods such as infrared spectroscopy and laser Raman spectroscopy are complex and expensive, the indirect methods such as visual, scrape, and hardness testing are more frequently assessed. Furthermore, many studies have found that hardness values show a positive correlation with degree of conversion.[1,4] Knoops and VK tests have been widely used to assess the depth of cure of composite resins.[11,12] Advantages of the surface hardness tests is that surface hardness is a good predictor for resin conversion as it is especially sensitive to small changes in polymer cross-linking in areas of high conversion.[13,14] Surface hardness tests furthermore allow for measurements at specific locations within the sample while its simplicity allows the evaluation of large number of specimens.
The depth of cure defined as the level at which hardness value is equivalent to at least 90% of the hardness as the top of the composite. Depth of cure for light-activated composites resins has often been evaluated indirectly by the measurement of the hardness of the material at specific.[15,16,17] Hence, in the present study bottom: top hardness ratios (B/T ratios) was used to obtain a percentage depth of cure, and if that value exceeded 80%, specimens were considered to be adequately polymerized. Furthermore, a B/T ratio of 80% corresponds to 90% of the maximum conversion possible at the top surface of a composite.[17,18] The VK method is therefore used to evaluate the depth of cure of composites.
The percentage depth of cure calculated as such, however, can easily be misinterpreted as a specimen could have been cured poorly throughout, and still provided a ratio that exceeds 80%.[17] Bouschlicher and Rueggeberg suggest that this problem can be overcome by normalizing the maximum hardness at the sample's top surface. This can be achieved by allowing top surface conversion to go on beyond the exposure time recommended by the manufacturer. If this is done, B/T hardness ratios can be used to compare the relative extent of cure of different composites with different curing strategies.[15] As the previous study, Bouschlicher and Rueggeberg, Leung et al., and Price et al. suggested that with the modern high-intensity LCUs, exposure time of 20s/2 mm increment can be sufficient to obtain a high degree of conversion.[15,16,17] Hence, in the present study, an exposure time of 30 s was used to cure the increments of 2 mm depth to achieve maximum hardness at the top surface, thus enabling to compare the relative extent of cure of two different composites used in the study.
The VHNs achieved in the present study at the top surface of composite specimens were higher compared to the bottom surface in all experimental groups. In addition to this present study, all the experimental groups met with the ISO requirement of ≥80% bottom/top microhardness percentage at 2 mm depth irrespective of the curing light used and mode of the curing. The results in the present study show that higher hardness values with the LED-curing unit when compared with QTH on both the upper and lower surfaces. In addition, the depth of cure with LED-curing unit was significantly higher than QTH regardless of the composite resin used. The results of the present study are in accordance with several other previous studies. Yaman et al. concluded that LED LCUs are found to be more successful than the halogen units with respect to both curing depth and microhardness properties.[18] Albino et al. have concluded that there is significant increase in microhardness of nanocomposite cured with LED compared with QTH.[19] Sharma et al. concluded that LEDs cause greater degree of conversion than QTH and there was a significant increase in depth of cure for nanocomposite.[20] However, there are few studies contradicting to the results of the present study due to the difference in the study design which may be due difference in intensity of the curing units, energy density, nature of wavelength spectrum, spectral distribution, and photoinitiators used in the composite resin.
Another approach that is used to offset photo polymerization stress build up is by providing an initial low rate of polymerization, thereby extending the time available for stress relaxation before reaching the gel point. This can be accomplished using a soft-start technique, where by curing begins at low-light intensity and finishes with high intensity. This approach allows for a slow initial rate of polymerization and a high initial level of stress relaxation during the early stages, and it ends at the maximum intensity once the gel point has been reached. This drives the curing reaction to the highest possible conversion only after much of the stress has been relieved. A number of studies have shown that varying levels of stress reduction in tooth cavity walls can be achieved with soft-start technique without increasing total exposure time or sacrificing either degree of conversion or depth of cure.[21,22] The results in the present study showed that greater hardness was achieved with the soft-start mode when compared with the continuous mode with both the LED and QTH LCUs. There was a statistically significant difference in the hardness both in the upper and lower surface of the samples cured with the soft-start mode. Maximum surface hardness of both the upper and lower surfaces was shown by LED light cure unit when operated in soft-start mode. In addition, the depth of cure was statistically more with the LED LCU with soft-start mode when compared with all other groups. The results of the present study are in accordance with several other previous studies. In a study, Ilie et al. concluded that soft-start polymerization concept is still valid for less deep cavities (2 mm), even by curing with high-power LED-curing units.[23] In a study, Soh et al. concluded that soft-start polymerization was as good as or better than those obtained using conventional continuous curing method.[21] Price et al. concluded that in soft-start mode decreasing the stress which occurs during polymerization and maintains optimal mechanical properties.[24]
It was previously thought that filler content is mainly responsible for mechanical properties of composite resins. However, the matrix components will also influence the overall mechanical performance of composites.[9] As the composites that were evaluated in the present study showed similarity in the composition of filler components, the influence of matrix on the overall mechanical properties of composites was evaluated. The monomer in charisma diamond is TCD and in IPS empress direct is conventional Bis-GMA.
The results in present study showed that charisma diamond had significantly higher surface hardness values when compared with IPS empress direct. TCD monomer reduces this vibration of monomers and minimizes the distance between themselves and results in reduced polymerization shrinkage. These novel monomers such as TCD are very reactive crosslinkers when compared with Bis-GMA monomer. Hence, it would have produced a higher degree of conversion compared with conventional Bis-GMA-based composites resulting in better mechanical strength. Because of this elastic behavior shrinkage, stress during light curing is reduced and binding areas in all planes which would have promoted the formation of a 3D-network and contributed to mechanical strength. Frauscher et al. concluded that novel monomer-like TCD showed higher degree of conversion and better mechanical properties such as surface hardness when compared with conventional Bis-GMA and TEGDMA monomers.[9] These results are in accordance with our present study. Ilie et al. concluded that even after the artificial aging TCD showed high VK values and better resistance to hydrolytic degradation when compared with conventional Bis-GMA monomer.[25,26]
However, the susceptibility to variation in irradiance proved to be material dependent and thus properties measured under clinically simulated curing conditions might vary to a different extend from those measured under ideal curing conditions.
CONCLUSION
Within the limitations of the present study, it can be concluded that LED-curing unit has performed better when compared with QTH unit. Irrespective of the curing light used soft-start mode has resulted in better depth of cure and surface hardness. TCD monomer showed better surface hardness when compared conventional Bis-GMA monomer. However, more emphasis has to be done on behavior of this novel monomer with different curing lights and curing modes to validate results in the present study.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Poggio C, Lombardini M, Gaviati S, Chiesa M. Evaluation of Vickers hardness and depth of cure of six composite resins photo-activated with different polymerization modes. J Conserv Dent. 2012;15:237–41. doi: 10.4103/0972-0707.97946. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Price RB, Ehrnford L, Andreou P, Felix CA. Comparison of quartz-tungsten-halogen, light-emitting diode, and plasma arc curing lights. J Adhes Dent. 2003;5:193–207. [PubMed] [Google Scholar]
- 3.Choudhary S, Suprabha B. Effectiveness of light emitting diode and halogen light curing units for curing microhybrid and nanocomposites. J Conserv Dent. 2013;16:233–7. doi: 10.4103/0972-0707.111322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.DeWald JP, Ferracane JL. A comparison of four modes of evaluating depth of cure of light-activated composites. J Dent Res. 1987;66:727–30. doi: 10.1177/00220345870660030401. [DOI] [PubMed] [Google Scholar]
- 5.Jadhav S, Hegde V, Aher G, Fajandar N. Influence of light curing units on failure of direct composite restorations. J Conserv Dent. 2011;14:225–7. doi: 10.4103/0972-0707.85793. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Mutluay MM, Rueggeberg FA, Price RB. Effect of using proper light-curing techniques on energy delivered to a Class 1 restoration. Quintessence Int. 2014;45:549–56. doi: 10.3290/j.qi.a31959. [DOI] [PubMed] [Google Scholar]
- 7.Kumar CN, Gururaj M, Paul J. A comparative evaluation of curing depth and compressive strength of dental composite cured with halogen light curing unit and blue light emitting diode: An in vitro study. J Contemp Dent Pract. 2012;13:834–7. doi: 10.5005/jp-journals-10024-1238. [DOI] [PubMed] [Google Scholar]
- 8.Asmussen E, Peutzfeldt A. Light-emitting diode curing: Influence on selected properties of resin composites. Quintessence Int. 2003;34:71–5. [PubMed] [Google Scholar]
- 9.Frauscher KE, Ilie N. Depth of cure and mechanical properties of nano-hybrid resin-based composites with novel and conventional matrix formulation. Clin Oral Investig. 2012;16:1425–34. doi: 10.1007/s00784-011-0647-3. [DOI] [PubMed] [Google Scholar]
- 10.Feilzer AJ, Dooren LH, de Gee AJ, Davidson CL. Influence of light intensity on polymerization shrinkage and integrity of restoration-cavity interface. Eur J Oral Sci. 1995;103:322–6. doi: 10.1111/j.1600-0722.1995.tb00033.x. [DOI] [PubMed] [Google Scholar]
- 11.Agrawal A, Manwar NU, Hegde SG, Chandak M, Ikhar A, Patel A, et al. Comparative evaluation of surface hardness and depth of cure of silorane and methacrylate-based posterior composite resins: An in vitro study. J Conserv Dent. 2015;18:136–9. doi: 10.4103/0972-0707.153070. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Dionysopoulos D, Papadopoulos C, Koliniotou-Koumpia E. Effect of temperature, curing time, and filler composition on surface microhardness of composite resins. J Conserv Dent. 2015;18:114–8. doi: 10.4103/0972-0707.153071. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Dietschi D, Marret N, Krejci I. Comparative efficiency of plasma and halogen light sources on composite micro-hardness in different curing conditions. Dent Mater. 2003;19:493–500. doi: 10.1016/s0109-5641(02)00095-7. [DOI] [PubMed] [Google Scholar]
- 14.Poskus LT, Placido E, Cardoso PE. Influence of placement techniques on Vickers and Knoop hardness of class II composite resin restorations. Dent Mater. 2004;20:726–32. doi: 10.1016/j.dental.2003.10.006. [DOI] [PubMed] [Google Scholar]
- 15.Bouschlicher MR, Rueggeberg FA, Wilson BM. Correlation of bottom-to-top surface microhardness and conversion ratios for a variety of resin composite compositions. Oper Dent. 2004;29:698–704. [PubMed] [Google Scholar]
- 16.Leung RL, Fan PL, Johnston W. Post-irradiation polymerization of visible-light-activated composite resins. J Dent Res. 1983;62:363–5. [Google Scholar]
- 17.Price RB, Felix CA, Andreou P. Knoop hardness of ten resin composites irradiated with high-power LED and quartz-tungsten-halogen lights. Biomaterials. 2005;26:2631–41. doi: 10.1016/j.biomaterials.2004.06.050. [DOI] [PubMed] [Google Scholar]
- 18.Yaman BC, Efes BG, Dörter C, Gömeç Y, Erdilek D, Büyükgökçesu S, et al. The effects of halogen and light-emitting diode light curing on the depth of cure and surface microhardness of composite resins. J Conserv Dent. 2011;14:136–9. doi: 10.4103/0972-0707.82613. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Albino LG, Rodrigues JA, Kawano Y, Cassoni A. Knoop microhardness and FT-Raman evaluation of composite resins: Influence of opacity and photoactivation source. Braz Oral Res. 2011;25:267–73. doi: 10.1590/s1806-83242011000300013. [DOI] [PubMed] [Google Scholar]
- 20.Sharma RD, Sharma J, Arunagiri D. A comparative study of degree of conversion of hybrid composite resins with nanocomposite resins when exposed to visible light cure unit and light emitting diodes: An in-vitro study. Indian J Dent Sci. 2010;2:6–10. [Google Scholar]
- 21.Soh MS, Yap AU, Siow KS. Post-gel shrinkage with different modes of LED and halogen light curing units. Oper Dent. 2004;29:317–24. [PubMed] [Google Scholar]
- 22.Yap AU, Soh MS, Siow KS. Effectiveness of composite cure with pulse activation and soft-start polymerization. Oper Dent. 2002;27:44–9. [PubMed] [Google Scholar]
- 23.Ilie N, Jelen E, Hickel R. Is the soft-start polymerisation concept still relevant for modern curing units? Clin Oral Investig. 2011;15:21–9. doi: 10.1007/s00784-009-0354-5. [DOI] [PubMed] [Google Scholar]
- 24.Price RB, Rizkalla AS, Hall GC. Effect of stepped light exposure on the volumetric polymerization shrinkage and bulk modulus of dental composites and an unfilled resin. Am J Dent. 2000;13:176–80. [PubMed] [Google Scholar]
- 25.Schmidt C, Ilie N. The effect of aging on the mechanical properties of nanohybrid composites based on new monomer formulations. Clin Oral Investig. 2013;17:251–7. doi: 10.1007/s00784-012-0707-3. [DOI] [PubMed] [Google Scholar]
- 26.Frauscher KE, Ilie N. Degree of conversion of nano-hybrid resin-based composites with novel and conventional matrix formulation. Clin Oral Investig. 2013;17:635–42. doi: 10.1007/s00784-012-0736-y. [DOI] [PubMed] [Google Scholar]