

Abstract
Aims:
This study is the first of its kind in the United Arab Emirates, where these herbal plant extracts are commonly incorporated into toothpaste. The present study compares two herbal toothpastes (Meswak extract and tea tree oil [TTO]) and analyses their efficiency in reducing plaque accumulation.
Materials and Methods:
A total of 25 patients were examined for plaque and assigned a plaque score. They were then randomly assigned to use either Meswak-based toothpaste or TTO-based toothpaste. After 24 h, a new plaque score was recorded, and the patients used their regular brand for 2 weeks. The patients were then instructed to use the second of the two study toothpastes for 24 h, and a third set of plaque scores was obtained. Statistical data were analyzed using the SPSS software with a significance of P < 0.05 and Kruskal–Wallis test.
Results:
Analysis of plaque scores showed a reduction in plaque index after using either of the two herbal-based toothpastes; however, when compared with TTO, Meswak-based toothpaste resulted in significantly less plaque.
Conclusions:
Brushing with Meswak-based toothpaste gave a significant drop in plaque score when compared with TTO-based paste.
KEYWORDS: Chewing stick, herbal toothpaste, Meswak, Miswak, plaque index, Siwak, tea tree oil
INTRODUCTION
Dental plaque forms continuously on tooth surfaces in all age groups and must be removed to promote oral hygiene. However, the only way to remove plaque accumulation is by brushing with a toothbrush.
The first natural brush in existence was the Meswak chewing stick [Figure 1]. Various studies have been undertaken to elucidate the general effect of Meswak on oral health, and currently, Meswak extract is used in toothpaste as both an active ingredient and as flavoring. Natural Meswak is found in the roots, twigs, and stems of the Salvadora persica tree[1] [Figure 2]. This tree is widely distributed from India in the east through southern Arabia, Iran, Iraq, Palestine, Egypt west to Mauritania and south through Sudan, Ethiopia, and central Africa to the southwest[2] [Figure 3]. On chemical analysis, Meswak bark and stems have high concentrations of chlorides, salvadourea, and gypsum.[3,4,5] Organic compounds such as pyrrolidine, pyrrole, and piperidine derivatives;[6] glycosides such as salvadoraside;[7] and flavonoids including kaempferol, quercetin, rutin, and a quercetin glucoside[8] are also present. In addition, β-sitosterol, m-Anisic acid, and elemental sulfur have been detected,[9] as well as a high ratio of alkaloids such as salvadorine and trimethylamine in the roots and bark.
Figure 1.

Meswak chewing stick
Figure 2.

Salvadora persica tree
Figure 3.

Distribution of Salvadora persica
The biological activities of the components of Meswak are varied. Repeated chewing of Meswak releases fresh sap containing fluoride; this may have an anticariogenic effect.[10] Silica acts as an abrasive material, which is effective in plaque removal combined with mechanical movement. Sulfur is found in the ash of S. persica roots in high concentrations, at almost 4.73%.[6] Sulfur has a bactericidal effect. Tannins act as an astringent and are suggested to reduce gingivitis. Tannins have been found to inhibit the action of glucosyltransferase, which reduces plaque formation and gingivitis.[11] Vitamin C facilitates tissue healing and repair. Sodium bicarbonate is present in Meswak and has mild abrasive properties in addition to having a mild germicidal action.[11]
High concentrations of chloride inhibit calculus formation and help remove stains from teeth. Calcium saturation of saliva prevents demineralization and promotes remineralization.[11] It has also been suggested that the high concentrations of sodium chloride, potassium chloride, sulfur-containing organic substances, and alkaloid trimethylamine are the agents responsible for the antibacterial effect and gingival stimulation effect.[12] Meswak also has antifungal properties and has been found to inhibit Candida albicans.[11,13] It also acts against both aerobic and anaerobic bacteria.
Another herbal extract known for its antiplaque properties is tea tree oil (TTO). TTO is derived from the leaves of Melaleuca alternifolia [Figure 4]. TTO has a remarkable property that makes it a powerful healing substance: it is a strong organic solvent that dissolves the clumps of white blood cells that make pus. The bloodstream is then able to clean them away, helping to clear infections such as boils, sores, and ulcers.[5] It is a fast-acting, efficient antiseptic with antibacterial properties. This is especially important for gum diseases. Moreover, TTO is unique in that it kills bacteria even more effectively in living tissue than in vitro, unlike most other currently used synthetic antiseptics. It is soothing on application and quickly relieves gum pain. Many in vitro studies confirmed that TTO has a powerful effect against Salmonella typhi, Staphylococcus aureus, and other Staphylococcus species, Escherichia coli, Proteus vulgaris, Enterococcus species, Enterobacter species, Mycobacterium smegmatis, Clostridium perfringens, Lactobacillus acidophilus, Bacteroides fragilis, Bacillus subtilis, and other Gram-positive and Gram-negative bacteria.[14] TTO has a similar range of antimicrobial activity to chlorhexidine, although their mechanisms of action differ.[15,16]
Figure 4.

Tea tree oil shrub (Melaleuca alternifolia)
Although both Meswak- and TTO-containing toothpastes are known to reduce plaque accumulation, it is currently unknown whether one is more effective than the other. Accordingly, we undertook this study to compare the effects of Meswak and TTO on plaque removal. To the best of our knowledge, this is the first study to compare Meswak and TTO in an attempt to analyze their efficiency in reducing plaque accumulation.
MATERIALS AND METHODS
Approval was obtained from the Ethics Committee of Ajman University (Ref. SSF-2016/17-04). The study included 25 students from the Ajman University Faculty of Dentistry; these 25 students were selected due to their availability for participation. Since comparative analysis between the two herbal products was less in literature, participant sample size was restricted to a minimum. All participants were willing and provided informed consent. Inclusion criteria were nonsmoking, no systemic disease, Grade 2 or 3 plaque score on at least one of the Oral Hygiene Index teeth (teeth 16, 11, 26, 36, 31, and 46), age 20–40 years of either sex, and a minimum of 24 teeth present in oral cavity. The participants were confirmed to not use Meswak- or TTO-based toothpaste as their regular toothpaste. Exclusion criteria were the presence of mild, moderate, or severe periodontitis, in which clinical attachment loss was between 2 and 5 mm, the presence of systemic disease, smoking, use of any medication, habits such as tobacco chewing, and use of Meswak- or TTO-based toothpaste.
MATERIALS
The study materials comprised two herbal toothpastes (one containing Meswak and one containing TTO).
PATIENT EXAMINATION
Plaque scores were assigned for all 25 patients and to each tooth according to the following criteria: 0 = no plaque; 1 = plaque deposits present on up to 1/3 of tooth surface; 2 = plaque deposits present on >1/3 but <2/3 of tooth surface; and 3 = plaque deposits present on >2/3 of tooth surface. Plaque score was determined by taking a sum of all individual scores and dividing the sum by the number of teeth for which the scores were recorded.
After examination, each patient was randomly given one of the herbal toothpastes without specific instructions for use; this prevented any alteration of data collected and reduced the possibility of error. For standardization, the patients were instructed to brush only once a day.
Patients were instructed to appear for follow-up after 24 h for examination. A new plaque score was recorded. The patients were then instructed to use their regular toothpaste for 2 weeks (wash-off period). After 2 weeks, the patients were given the other herbal-based toothpaste and recalled after 24 h to record a third plaque score. All patients completed the study successfully.
STATISTICAL ANALYSIS
Data were analyzed using the IBM corp.2013.IBM SPSS statistics for macintosh, version 22.0 with a significance of P < 0.05 and Kruskal–Wallis test.
RESULTS
Observational results combined with statistical analysis showed a noticeable change between initial plaque index, post-Meswak toothpaste plaque index, and post-TTO toothpaste plaque index. Either toothpaste resulted in a lower plaque index compared with the initial plaque index. However, use of Meswak toothpaste resulted in a smaller plaque index than the use of TTO toothpaste. Brushing with TTO toothpaste reduced the initial plaque score by 35%, while brushing with Meswak toothpaste reduced the initial plaque score by 67.3%, nearly double that of the TTO toothpaste. In some patients, Meswak-associated plaque reduction reached 90%–100%; this degree of plaque reduction was not observed after the use of TTO-containing toothpaste. Statistical analyses of changes in plaque index are presented in Tables 1–4 and Figures 5–7. Of note, among the 25 patients, only one disliked the taste of the Meswak toothpaste, whereas 18 patients disliked the alkaline taste of the TTO toothpaste.
Table 1.
Plaque index (mean and standard deviation)
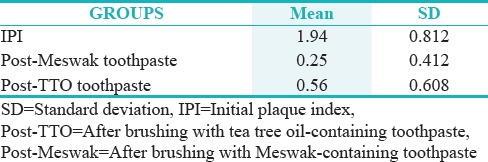
Table 4.
Paired samples test (t-test)
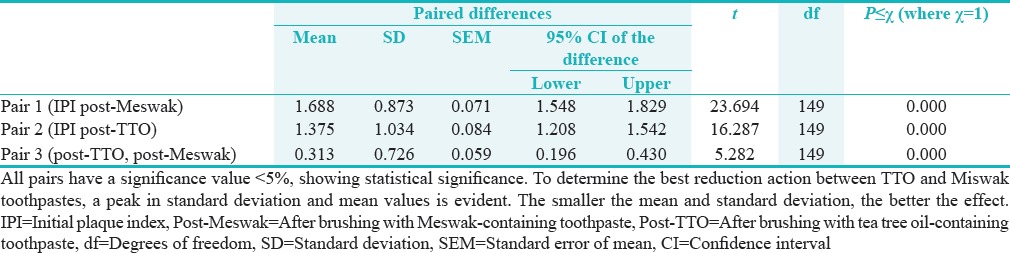
Figure 5.
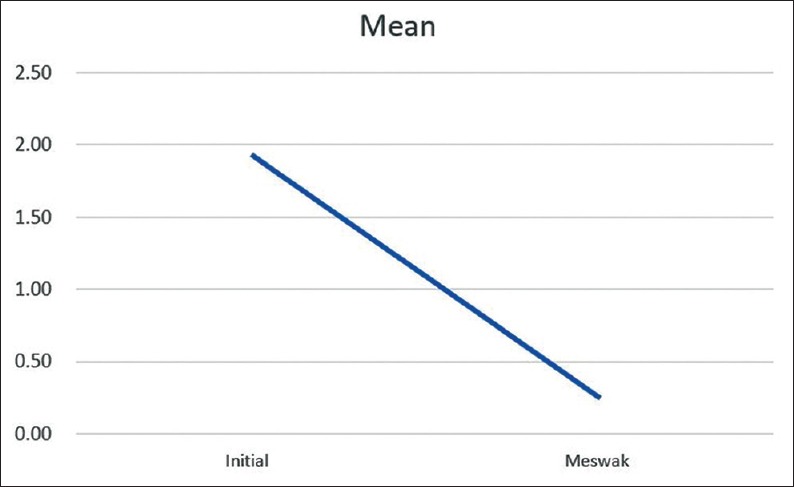
Diagram comparing the plaque index after Meswak toothpaste use to the initial plaque index
Figure 7.
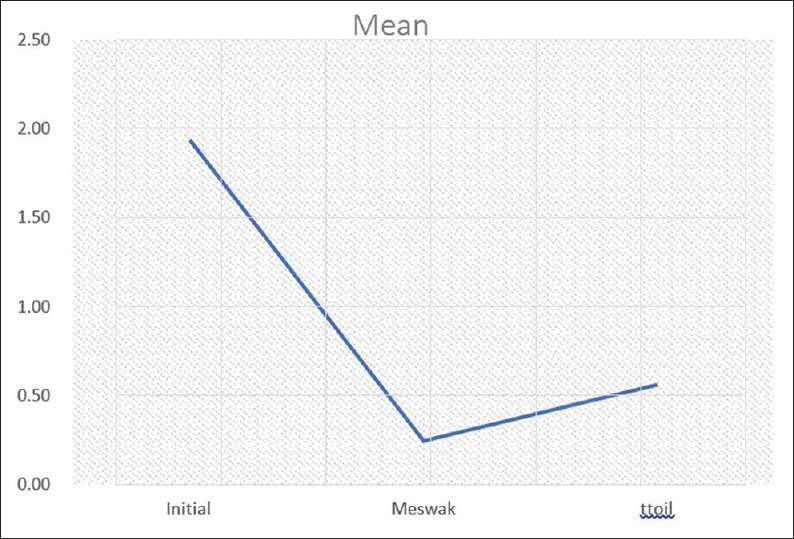
A comparison of the improvement in plaque index after use of Meswak- and tea tree oil (ttoil)-based toothpastes
Table 2.
Plaque index: Paired sample statistics
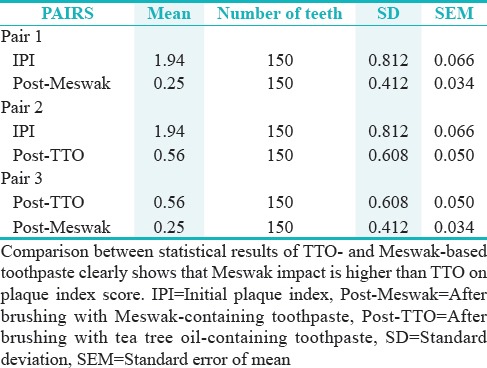
Table 3.
Paired sample correlations
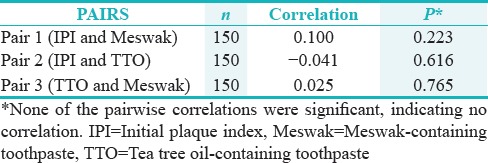
Figure 6.
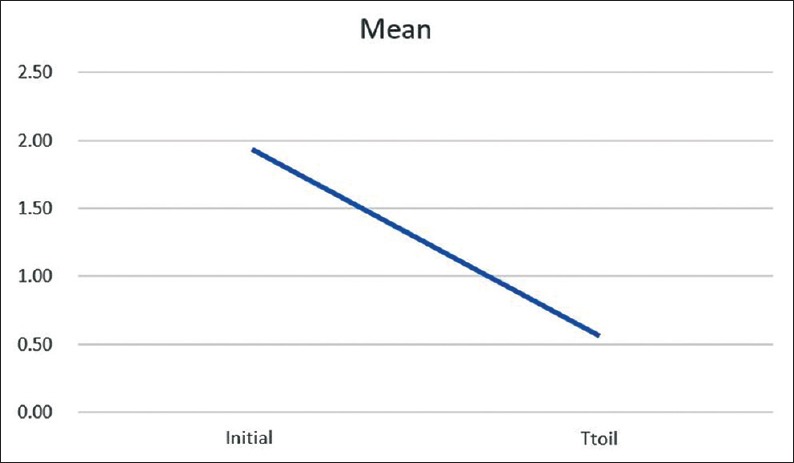
Diagram comparing the plaque index after tea tree oil toothpaste use to the initial plaque index
DISCUSSION
The Meswak tree, known as “Miswak” “Siwak” and “Arak” in Arabic regions, “koyoji” and “qisa” in Aramic, and “mastic” in Latin[17,18,19] is a common source of dental cleaning sticks. In countries where S. persica is absent, alternative chewing sticks are used such as those from lime trees (Citrus aurantifolia), orange trees (Citrus sinensis), and senna (Caesalpinioideae – Fabaceae) in southwest Africa,[20] and neem trees (Azadirachta indica) in India.[10] Tea tree leaves were used by Australian aboriginal people to treat cuts and wounds, and their use as a folk medicine spread among Europeans as they settled Australia in the 19th century. TTO was so effective as a basic antiseptic that soldiers were issued a bottle along with their first-aid kit during World War II as treatment for cuts, burns, scratches, and infections.[21,22]
Our study was a randomized, controlled, parallel group design clinical trial, whereby our aim was to evaluate mainly the plaque reduction parameter using both the toothpaste. The positives from our study could be underlined about the fact that the clinical trial involved comparative evaluation between two herbal pastes which have plaque reducing capabilities. It also showed that meswak was superior to TTO in terms of plaque reducing capabilities.[23,24]
Meswak chewing sticks have been evaluated with respect to antibacterial properties. A study was conducted that compared 1-month-old Meswak and fresh Meswak with a neem chewing stick.[25] The results suggested that there is no significant difference in effect between fresh and 1-month-old Meswak, and the antibacterial effects of both Meswak extract and a Meswak stick were stronger than that of the neem stick. Both Meswak and neem suppressed Streptococcus mutans and Streptococcus faecalis at a 50% concentration, but Meswak was more effective even in low concentrations.[25] The antimicrobial effect may be linked to salivary peroxidase.[26]
A study conducted in Sudan reported less caries prevalence among people who use chewing sticks compared with those who use toothbrushes,[27] without consideration of the individual's carbohydrate-rich diets and lack of modern dental knowledge and hygiene.[28,29] Another study compared the World Health Organization decayed, missing, and filled teeth index between an Iraqi population of school children who do not use Meswak with a similar population from Sudan who uses Meswak. It was found that Sudanese students had lower caries prevalence than Iraqi students.[27,30] This finding was similar to that of a study conducted in children from Saudi Arabia between ages 13 and 15 years and Western countries.[31,32,33]
There is evidence that Meswak effectively reduces plaque and gingivitis scores,[34,35,36] and several studies revealed that Meswak removes dental plaque more effectively than toothbrushing alone.[32,37] In our study, Meswak reduced plaque scores by a mean of 67.3%, which was similar to previously published studies.[18,25,26] One study reported a reduction of plaque by 75% after use of Meswak for 8 days.[27] Another study found Meswak-containing toothpaste to be significantly effective in removing dental plaque when compared with Oral-B toothpaste.[23] However, in contrast, Eid et al. reported that Meswak had a negligible effect on gingival health and accumulation of plaque.[24]
In the 1930s, investigations into TTO revealed its antimicrobial properties; it was found to be more effective than carbolic acid on typhus bacilli and could be used directly on open wounds without any adverse effect on the wounded tissues.[14] In the 1970s, TTO was shown to have an antibacterial effect against S. aureus, S. typhi, and various Gram-positive and Gram-negative bacteria.[14] More recently, an in vitro study into the bacteriostatic, bactericidal, and fungicidal properties of TTO showed that it had a strong effect against Actinobacillus actinomycetemcomitans, Fusobacterium nucleatum, and Porphyromonas gingivalis, and a weaker effect on S. mutans and Prevotella intermedia.[38] Furthermore, it has been shown that 0.0008% and 0.0009% solutions of TTO reduce the formation of herpes simplex virus 1 and herpes simplex virus 2 colonies after 1 h of exposure, respectively.[39,40]
TTO is further advocated to reduce immunomodulatory mechanisms in oral cancer patients who shows symptoms of oral candidiasis.[41] Its role to bring suppression of fungal growth had been proven with limitations.
Its role along with other herbal extracts in the treatment of periodontal conditions and also conservative dental treatment has been established but with minimal clinical significance.[42,43]
Its use in endodontic treatment and also in symptomatic cases where the periradicular tissue is compromised due to a chronic condition is noteworthy but questionable. Its actual mode of action in these cases needs to be evaluated more and patients need to be put on a follow-up to see results.[44,45]
The results of our study showed a lower plaque index score with Meswak when compared with TTO, which was significant and was in agreement with a previous study using Meswak alone by Akhtar and Ajmal.[18] Brushing with Meswak-based toothpaste gave a significant drop in plaque score when compared with TTO-based paste. Total plaque scores were significantly reduced using Meswak, which was in agreement with Almas and Darout.[26,27]
Our study has some limitations. Although some participants reported reduction or elimination of bleeding after brushing with Meswak-containing toothpaste, we did not formally assess changes in gingival inflammation.
To the best of our knowledge, this is the first study to compare the effects of Meswak and TTO herbal toothpastes on dental plaque. Our study revealed that toothpaste composition has an effect on plaque accumulation which was in agreement with an earlier study.[25] Meswak-based toothpaste was more effective in reducing the plaque index than TTO-based toothpaste. A detailed study is needed to elucidate the long-term effects of each component. It is important to thoroughly investigate TTO to better understand its effect on dental hygiene. Further investigations using more advanced technology will enhance our understanding of the mechanisms of action of both Meswak and TTO.
CONCLUSIONS
The use of herbal-based dentifrices is increasing among the population and the use of unique herbal extracts among the population is more rampant. Though in our study meswak was superior to tea tree oil in plaque reduction. The efficacy of TTO in other oral disease process needs to be evaluated and documented. Area such as periodontal microbiology and immunology where most disease processes are studied, and with the advent of next-generation sequencing techniques, it will give a clear picture of the role of TTO in various periodontal disease processes.
FINANCIAL SUPPORT AND SPONSORSHIP
Nil.
CONFLICTS OF INTEREST
There are no conflicts of interest.
REFERENCES
- 1.Elvin-Lewis M, Hall JB, Adut-Tutu M, Afful Y, Asante-Appiah K, Lieberman D. The dental health of chewing stick users of Southern Ghana: Preliminary findings. J Prev Dent. 1980;6:151–9. [Google Scholar]
- 2.Engler A, Prantl K. the natural plant families. 2nd. Leipzig: Engelmann; 1942. p. 20b. [Google Scholar]
- 3.Ray AB, Chand L, Dutta SC. Salvadourea: New urea derivative from Salvadora persica. Chem Ind (London) 1975;12:517–8. [Google Scholar]
- 4.Massassati A, Frank RM, Arends J, Klein JP. Ultrastructural studies crystallographic and microbiological to. sticks rubs - teeth (Miswak ) used for dental hygiene in the countries. J Biol Buccale. 1981;9:53–60. [Google Scholar]
- 5.Porteres R. A curious Arab- Islamic cultural element and Neo- Africa : The chopped vegetable sticks serving as toothpicks. J Agric Trop Bot. 1974;21:1–36. [Google Scholar]
- 6.Galletti GC, Chiavari G, Kahie YD. Pyrolysis/gas chromatography/ion-trap mass spectrometry of the 'tooth brush' tree (Salvadora persica L.) Rapid Commun Mass Spectrom. 1993;7:651–5. [Google Scholar]
- 7.Ohtani K, Kasai R, Yamasaki K, Tanaka O, Kamel MS, Assaf MH, et al. Lignan glycosides from stems of Salvadora persica. Phytochemistry. 1992;31:2469–71. [Google Scholar]
- 8.Abdel-Wahab S, Selim M, El-Fiki N. Investigation of the flavonoid content of Salvadora persica L. Bull Fac Pharm Cairo Univ. 1990;28:67–70. [Google Scholar]
- 9.Ezmirly ST, Cheng JC, Wilson SR. Saudi Arabian medicinal plants: Salvadora persica. Planta Med. 1979;35:191–2. doi: 10.1055/s-0028-1097205. [DOI] [PubMed] [Google Scholar]
- 10.Almas K, al-Lafi TR. The natural toothbrush. World Health Forum. 1995;16:206–10. [PubMed] [Google Scholar]
- 11.Gazi MI, Davies TJ, al-Bagieh N, Cox SW. The immediate- and medium-term effects of Meswak on the composition of mixed saliva. J Clin Periodontol. 1992;19:113–7. doi: 10.1111/j.1600-051x.1992.tb00449.x. [DOI] [PubMed] [Google Scholar]
- 12.Dorner WG. Active substances from African and Asian natural toothbrushes. Chem Rundsch. 1981;34:19–23. [Google Scholar]
- 13.Al lafi T, Ababneh H. The effect of the extract of the miswak (chewing sticks) used in Jordan and the Middle East on oral bacteria. Int Dent J. 1995;45:218–22. [PubMed] [Google Scholar]
- 14.Markham JL. Biological activity of tea tree oil. In: Southwell I, Lowe R, editors. Tea Tree: The Genus Melaleuca. USA: Harwood Academic Publishers CRC Press; 1999. pp. 169–90. [Google Scholar]
- 15.Fine DH, Furgang D, Barnett ML, Drew C, Steinberg L, Charles CH, et al. Effect of an essential oil-containing antiseptic mouthrinse on plaque and salivary Streptococcus mutans levels. J Clin Periodontol. 2000;27:157–61. doi: 10.1034/j.1600-051x.2000.027003157.x. [DOI] [PubMed] [Google Scholar]
- 16.Juergens UR, Stöber M, Schmidt-Schilling L, Kleuver T, Vetter H. Antiinflammatory effects of euclyptol (1.8-cineole) in bronchial asthma: Inhibition of arachidonic acid metabolism in human blood monocytes ex vivo. Eur J Med Res. 1998;3:407–12. [PubMed] [Google Scholar]
- 17.Salvatori C, Barchi L, Guzzo F, Gargari M. A comparative study of antibacterial and anti-inflammatory effects of mouthrinse containing tea tree oil. Oral Implantol (Rome) 2017;10:59–70. doi: 10.11138/orl/2017.10.1.059. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Akhtar MS, Ajmal M. Significance of chewing-sticks (miswaks) in oral hygiene from a pharmacological view-point. J Pak Med Assoc. 1981;31:89–95. [PubMed] [Google Scholar]
- 19.Soukoulis S, Hirsch R. The effects of a tea tree oil-containing gel on plaque and chronic gingivitis. Aust Dent J. 2004;49:78–83. doi: 10.1111/j.1834-7819.2004.tb00054.x. [DOI] [PubMed] [Google Scholar]
- 20.Saxer UP, Stäuble A, Szabo SH, Menghini G. Effect of mouthwashing with tea tree oil on plaque and inflammation. Eur J Dent. 2003;113:985–96. [PubMed] [Google Scholar]
- 21.Raut CP, Sethi KS. Comparative evaluation of co-enzyme Q10 and Melaleuca alternifolia as antioxidant gels in treatment of chronic periodontitis: A clinical study. Contemp Clin Dent. 2016;7:377–81. doi: 10.4103/0976-237X.188572. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Rahman B, Alkawas S, Al Zubaidi EA, Adel OI, Hawas N. Comparative antiplaque and antigingivitis effectiveness of tea tree oil mouthwash and a cetylpyridinium chloride mouthwash: A randomized controlled crossover study. Contemp Clin Dent. 2014;5:466–70. doi: 10.4103/0976-237X.142813. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Moustafa MH, Abd el-All MM, Abo el-Fadl KM. Reduced plaque formation by miswak-based mouthwash. Egypt Dent J. 1987;33:375–84. [PubMed] [Google Scholar]
- 24.Hattab FN. Meswak: The natural toothbrush. J Clin Dent. 1997;8:125–9. [PubMed] [Google Scholar]
- 25.Haque MM, Alsareii SA. A review of the therapeutic effects of using miswak (Salvadora persica) on oral health. Saudi Med J. 2015;36:530–43. doi: 10.15537/smj.2015.5.10785. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Almas K, Al-Bagieh NH. The antimicrobial effects of bark and pulp extracts of miswak, Salvadora persica. Biomed Lett. 1999;60:71–5. [Google Scholar]
- 27.Darout IA, Albandar JM, Skaug N. Periodontal status of adult Sudanese habitual users of miswak chewing sticks or toothbrushes. Acta Odontol Scand. 2000;58:25–30. doi: 10.1080/000163500429398. [DOI] [PubMed] [Google Scholar]
- 28.Kothiwale SV, Patwardhan V, Gandhi M, Sohoni R, Kumar A. A comparative study of antiplaque and antigingivitis effects of herbal mouthrinse containing tea tree oil, clove, and basil with commercially available essential oil mouthrinse. J Indian Soc Periodontol. 2014;18:316–20. doi: 10.4103/0972-124X.134568. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Carl W, Zambon JJ. Dental health of the Rendille and Samburu of the northern frontier district of Kenya. N Y State Dent J. 1993;59:35–9. [PubMed] [Google Scholar]
- 30.Piekarz T, Mertas A, Wiatrak K, Rój R, Kownacki P, Śmieszek-Wilczewska J, et al. The influence of toothpaste containing Australian Melaleuca alternifolia oil and ethanolic extract of polish propolis on oral hygiene and microbiome in patients requiring conservative procedures. Molecules. 2017;22:pii: E1957. doi: 10.3390/molecules22111957. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Char D, Dogao A, Dogan M. SEM, XRF, and EMPA evaluation of Middle Eastern toothbrush “Salvadora persica”. J Electron Microsc Technol. 1987;5:145. [Google Scholar]
- 32.Younes SA, El-Angbawi MF. Dental caries prevalence in intermediate Saudi schoolchildren in Riyad. Community Dent Oral Epidemiol. 1982;10:74–6. doi: 10.1111/j.1600-0528.1982.tb00366.x. [DOI] [PubMed] [Google Scholar]
- 33.al-Khateeb TL, O'Mullane DM, Whelton H, Sulaiman MI. Periodontal treatment needs among Saudi Arabian adults and their relationship to the use of the miswak. Community Dent Health. 1991;8:323–8. [PubMed] [Google Scholar]
- 34.Santamaria M., Jr Petermann KD, Vedovello SA, Degan V, Lucato A, Franzini CM, et al., editors. Antimicrobial effect of Melaleuca alternifolia dental gel in orthodontic patients. Am J Orthod Dentofacial Orthop. 2014;145:198–202. doi: 10.1016/j.ajodo.2013.10.015. [DOI] [PubMed] [Google Scholar]
- 35.Olsson B. Efficiency of traditional chewing sticks in oral hygiene programs among Ethiopian schoolchildren. Community Dent Oral Epidemiol. 1978;6:105–9. doi: 10.1111/j.1600-0528.1978.tb01131.x. [DOI] [PubMed] [Google Scholar]
- 36.Al-Otaibi M, Al-Harthy M, Söder B, Gustafsson A, Angmar-Månsson B. Comparative effect of chewing sticks and toothbrushing on plaque removal and gingival health. Oral Health Prev Dent. 2003;1:301–7. [PubMed] [Google Scholar]
- 37.Guile EE. Periodontal status of adults in central Saudi Arabia. Community Dent Oral Epidemiol. 1992;20:159–60. doi: 10.1111/j.1600-0528.1992.tb01554.x. [DOI] [PubMed] [Google Scholar]
- 38.Eid MA, Selim HA, al-Shammery AR. Relationship between chewing sticks (Miswak) and periodontal health. Part 1. Review of the literature and profile of the subjects. Quintessence. 1990;21:913–7. [PubMed] [Google Scholar]
- 39.Kulik E, Lenkett K, Meyer J. Antimicrobial effect of. Tea tree oil (Melaleuca alternifolia ) on oral microorganisms. Acta Med Dent Helv. 2000;5:125–30. [PubMed] [Google Scholar]
- 40.Schnitzler P, Schön K, Reichling J. Antiviral activity of Australian tea tree oil and eucalyptus oil against herpes simplex virus in cell culture. Pharmazie. 2001;56:343–7. [PubMed] [Google Scholar]
- 41.Ramage G, Milligan S, Lappin DF, Sherry L, Sweeney P, Williams C, et al. Antifungal, cytotoxic, and immunomodulatory properties of tea tree oil and its derivative components: Potential role in management of oral candidosis in cancer patients. Front Microbiol. 2012;3:220. doi: 10.3389/fmicb.2012.00220. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Patri G, Sahu A. Role of herbal agents-tea tree oil and Aloe vera as cavity disinfectant adjuncts in minimally invasive dentistry – An in vivo comparative study. J Clin Diagn Res. 2017;11:DC05–9. doi: 10.7860/JCDR/2017/27598.10147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Hans VM, Grover HS, Deswal H, Agarwal P. Antimicrobial efficacy of various essential oils at varying concentrations against periopathogen Porphyromonas gingivalis. J Clin Diagn Res. 2016;10:ZC16–9. doi: 10.7860/JCDR/2016/18956.8435. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Agrawal V, Kapoor S, Agrawal I. Critical review on eliminating endodontic dental infections using herbal products. J Diet Suppl. 2017;14:229–40. doi: 10.1080/19390211.2016.1207004. [DOI] [PubMed] [Google Scholar]
- 45.Dagli N, Dagli R, Mahmoud RS, Baroudi K. Essential oils, their therapeutic properties, and implication in dentistry: A review. J Int Soc Prev Community Dent. 2015;5:335–40. doi: 10.4103/2231-0762.165933. [DOI] [PMC free article] [PubMed] [Google Scholar]