

Abstract
Aims and Objectives:
Dental pain and anxiety are important factors that prevent patients from seeking dental care. The aim of this study was to assess the relationship between trait anxiety and state anxiety and also to determine the effects of age and sex on pain perception after periodontal flap surgery.
Materials and Methods:
In this descriptive-analytical study, 50 patients who need periodontal flap surgery were assessed in a private periodontal specialty clinic in Babol city. The amount of anxiety was measured by the Spielberger State-Trait Anxiety Inventory test, and visual analog scale scores were used for postsurgical pain perceptions in 7 times (immediately after surgery and days 1–6 after surgery). Data were analyzed and evaluated by SPSS V22.0 software (IBM, United States).
Results:
In the trait anxiety study, there was a significant difference in pain perception between different anxiety classes at times immediately after surgery, 1st day, and 2nd day after surgery (P < 0.05), and in the state anxiety study, there was a significant difference in pain perception between different anxiety classes at times immediately after surgery until the 5th day after surgery (P < 0.05). Furthermore, the results indicate that the pain perception in female was significantly higher than male, at times immediately after surgery, 3rd day, and 5th day after surgery (P < 0.05). However, there was no association between age and pain perception in different times (P > 0.05).
Conclusions:
Anxiety is associated with pain perception following periodontal flap surgery, and female experience more pain after surgery, whereas the amount of pain perception is not related to age.
KEYWORDS: Periodontal flap surgery, state anxiety, trait anxiety, visual analog scale
INTRODUCTION
Anxiety is an emotional reaction that is defined as stress, fear, nervousness, and concerns. Anxiety is due to an intangible risk and autonomic nervous system activity and describes by two methods: Trait anxiety and state anxiety.[1]
Trait anxiety is a relatively stable tendency of anxiety that anyone can be harassed when confronted with threatening situations. State anxiety is an unstable emotional state due to the pressure and fear and increased activity of the autonomic nervous system, which dental anxiety is a state anxiety kind.[1] Dental anxiety was defined by Klinberg and Broberg as a fear of a terrible occurrence in dental treatment.[2] State and the trait anxiety are independent in the sense, so that a person with trait anxiety may not show a state anxiety at a specific time, and on the contrary, a person without anxiety attribute can be anxious in a definite position.[3]
Many studies have been performed on the effect of anxiety on patients' pain during and after surgery, and it has been shown that high patient anxiety could have a negative effect on the person's physical and mental improvement, such as longer recovery time and more need for analgesia.[4]
Flap surgery is one of the variety of periodontal surgeries that can be affected by several factors such as the method of treatment, type of instrument, tissue invasion, incision, pain period, and recovery after surgery that these factors can changes it into a stressful treatment, and it has a range of pain and disabling responses based on degrees of discomfort.[5]
Pain is an unpleasant sensation associated with true tissue damage that transmitted to the brain by certain neural fibers. This definition shows that the pain has many psychological, moderator, and annoying transitional components.[6]
With this explanation and considering that a similar study has not been conducted in the country so far, this study aimed to investigate the effect and role of state and trait anxiety on the perception of pain after periodontal flap surgery.
MATERIALS AND METHODS
This descriptive-analytical study was done periodically in a period of 10 months (from November 2016 to August 2017) on 50 patients who were referred to a private periodontal specialty clinic in Babol city and need periodontal flap surgery. The sample size was determined based on sample size correlation formula.
The present study under the code MUBABOL.REC.1395.202 was approved by Ethics Committee of Babol University of Medical Sciences.
INCLUSION CRITERIA
Over 18 years of age
Nonspecific systemic disease
Moderate chronic periodontitis patients that require periodontal flap surgery (an undisplaced flap with resective osseous surgery)
Patient without the history of periodontal surgery and
The patient's ability to read, understand, and answer questions in the questionnaire.
EXCLUSION CRITERIA
Need for pretreatment sedation
History of analgesics consumption in the presurgical period (aspirin, etc.)
Patients with mental retardation, serious suicidal thoughts, dementia, and psychosis
Patients undergoing prolonged surgical procedures and prescribed corticosteroids and
Patients with the history of temporomandibular joint disorders, allergy to epinephrine, history of damage or paresthesia, and pregnancy.
After receiving explanations regarding the study process and guidelines for filling in the questionnaire, conscious consent was obtained from patients. Then, data on sex and age of the patient, medical history, smoking history, surgical duration, occupation, and civil status were recorded. This study was performed during the first periodontal flap surgery. The patient was requested to complete Spielberger State-Trait Anxiety Inventory-Trait (STAI-T), and Spielberger STAI-State questionnaires before giving any surgical information to the patient (30 min before surgery). The STAI showed good internal consistency (Cronbach's alpha = 0.89).[7] Mahram translated the scale into Farsi and confirmed the validity of the instrument. The internal consistency of the Farsi state (Cronbach's alpha = 0.91) and trait (Cronbach's alpha = 0.90) items were excellent.[8]
Trait anxiety refers to a general feeling and anxiety of the patient. Trait anxiety questionnaire consisted of 20 questions that have 4 levels of response, from almost never to almost always, and indicates different levels of anxiety in relation to the conditions that a person considers to be a threat. In contrast, state anxiety has been defined as an individual's sense and anxiety at the moment, and its questionnaire consisted of 20 questions that have 4 levels from at all to so much and evaluates the emotional moment state of a person. State anxiety can be different in various times. Then, the information about the surgery and related conditions were given to the patients. Interpretation of the questionnaires will be on the base of patient's answers.
Surgery was performed at a private clinic in the same and quiet place by one periodontist. All surgical procedures were performed by infiltration with lidocaine carpals 2% and epinephrine 1: 100,000 (DrouPakhsh Company-Iran) under local anesthesia. The wound was closed with 3/0 silk (Supa Company, Iran) and the surgical area was covered with COE-PAK. All patients received amoxicillin 500 mg (Loghman Company, Iran) 3 times a day for 7 days and analgesic ibuprofen 400 mg (pharmaceutical company, Arya) every 6 h and chlorhexidine 0.2% mouthwash (Shahr Darou Laboratory Company, Iran). After 1 week, the sutures were removed in all patients.
Visual analogue scale (VAS) is a measurement instrument that is often used for the assessment of pain perception in patients. It is a simple, reliable, and valid pain measurement scale that has been used for evaluating dental pain.[9] In this study, VAS was used for assessing the pain perception based on a horizontal linear scale from 0 to 10. On this scale, 0 being “no pain and discomfort at all” and 10 being “the most severe pain or discomfort” for the patient. The patient was requested to mark this test immediately after surgery (T0) and at all times until removing of sutures (T1–T6) at about the same time of surgery.
Furthermore, the patient was requested to note the time and number of doses of consumed analgesic in this week.
One-way repeated measures ANOVA, Tukey's, and independent t-test were used to analyze the data.
RESULTS
A total of 23 male and 27 female patients in three group age (<30-year-old; between 30 and 40-year-old, and > 40-year-old) were evaluated in this study. The mean amount of surgical duration was 47.24 ± 9.70 min. At first, the amount of consumed analgesic was evaluated in the studied groups (including trait anxiety, state anxiety, sex, and age) and there was no significant difference between the studied groups.
Due to the lack of samples in intense anxiety and very intense anxiety groups, the remaining four groups (mild anxiety, moderate-to-low anxiety, moderate-to-high anxiety, and relatively intense) were compared.
In trait anxiety groups, the mean and standard deviation of pain variables analysis by repeated measures ANOVA and Greenhouse-Geisser correction showed that the time has a significantly effect on pain perception in the 7 times (T0 and T1 to T6) (F = 76.07; df = 2.87 and P < 0.0001) and the perception of pain has reduced during the time. Furthermore, impact of trait anxiety (F = 5.23, df = 3 and P = 0.003) and interaction between time and trait anxiety (F = 4.74, df = 8.61 and P < 0.0001) were significantly different between groups. One-way ANOVA and post hoc Tukey test were used to compare pain perception at different times, separately.
There was a significant difference in pain perception between mild and moderate-to-low classes with relatively intense class immediately after surgery (T0). On the 1st day after surgery (T1), a significant difference in pain perception was observed between mild and moderate-to-low classes with moderate-to-high and relatively intense classes, and in 2nd day after surgery (T2), difference between mild class with moderate-to-high and relatively intense classes was significant. No significant difference was observed between groups in other days [Table 1 and Figure 1].
Table 1.
Pain perception at different times according to the trait anxiety variable
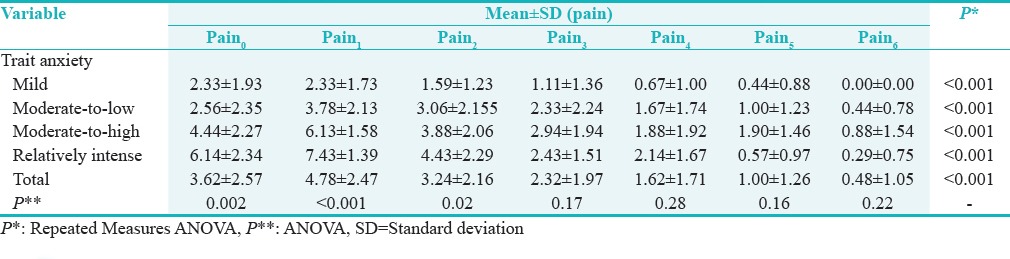
Figure 1.
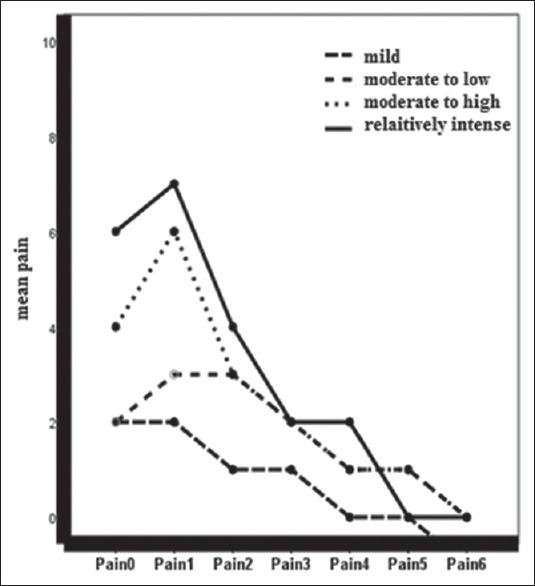
The mean pain perception at different times according to the trait anxiety variable
In state anxiety groups, the mean and standard deviation analysis of pain variable by repeated measures ANOVA and Greenhouse-Geisser correction showed that the time has a significant effect on pain perception in the 7 times (F = 56.32; df = 2.83 and P < 0.0001) and the perception of pain has reduced during the time. Furthermore, impact of state anxiety (F = 15.77, df = 3, and P = 0.0001) and interaction between time and state anxiety (F = 8.50, df = 2.92, and P < 0.004) were significantly different between groups.
One-way ANOVA and post hoc Tukey test were separately used to compare pain perception at different times.
There was a significant difference in pain perception between mild and moderate-to-low classes with moderate-to-high and relatively intense classes immediately after surgery until the 5th day after surgery, but no significant difference was observed between groups on the 6th day [Table 2 and Figure 2].
Table 2.
Pain perception at different times according to the state anxiety variable
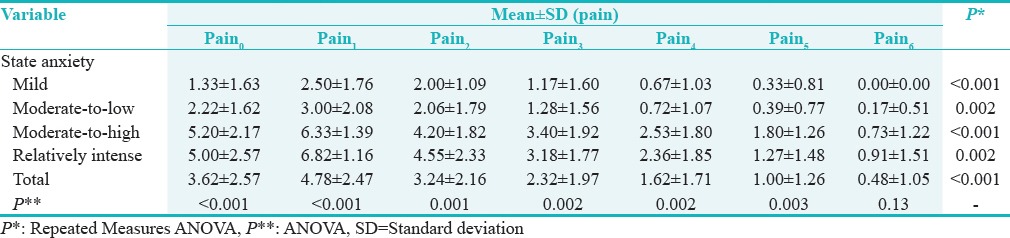
Figure 2.
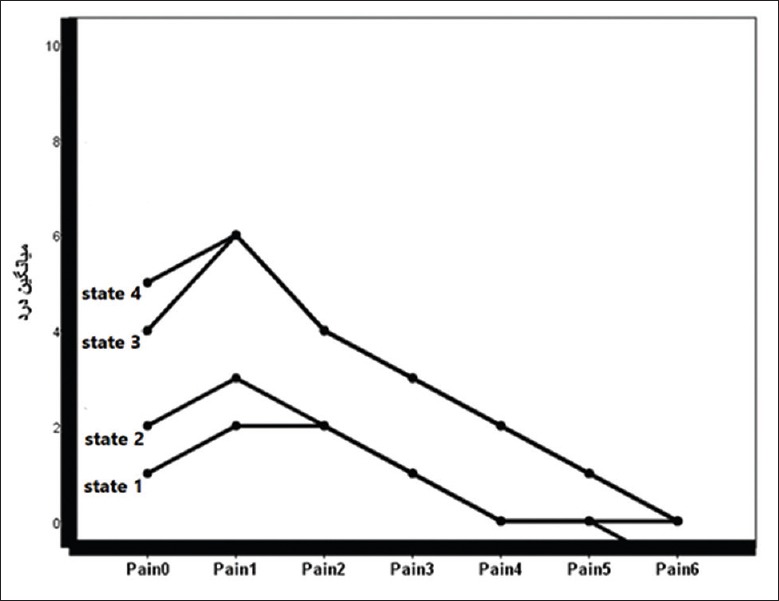
The mean pain perception at different times according to the state anxiety variable
On the base of repeated measures ANOVA and Greenhouse-Geisser correction analysis, significant differences were detected among pain perception and sex in the seven times (F = 57.30, df = 2.79, and P < 0.0001) and the pain perception has reduced during the time. Sex impact on pain perception was significantly difference (F = 5.09, df = 1 and P = 0.02) but the interaction among time and sex variable was not significant (F = 2.09, df = 2.09 and P = 0.10). The t-test analysis was separately used to compare pain perception at different times, and results indicate that pain perception in female was significantly higher than male, in the immediately after surgery (P = 0.009), 3rd day (P = 0.03) and 5th day after surgery (P = 0.01) [Table 3 and Figure 3].
Table 3.
Pain perception at different times according to the sex variable

Figure 3.
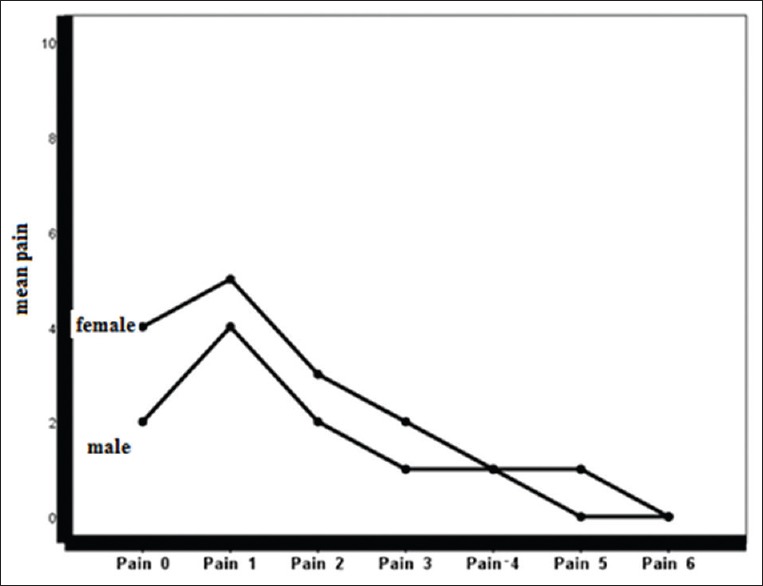
The mean pain perception at different times according to the sex variable
On the base of repeated measures ANOVA and Greenhouse-Geisser correction analysis, significant differences were detected among pain perception and age in the 7 times (F = 61.61, df = 2.71, and P < 0.0001) and the pain perception has reduced during the time, but no significant differences were detected in impact of age variable (F = 1.86, df = 2, and P = 0.16) and interaction between time and age (F = 0.56, df = 5.43, and P = 0.74). One-way ANOVA and post hoc Tukey test were separately used to compare pain perception at different times, and no significant difference was observed between groups in different times [Table 4 and Figure 4].
Table 4.
Pain perception at different times according to the age
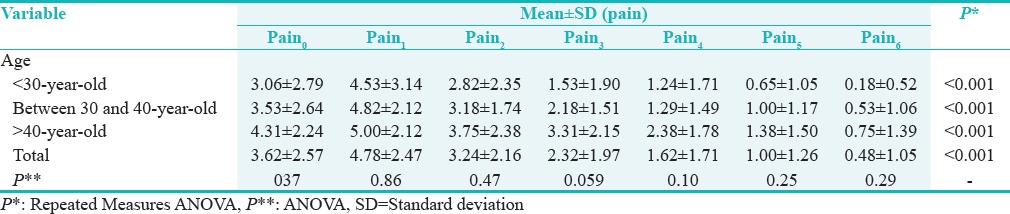
Figure 4.
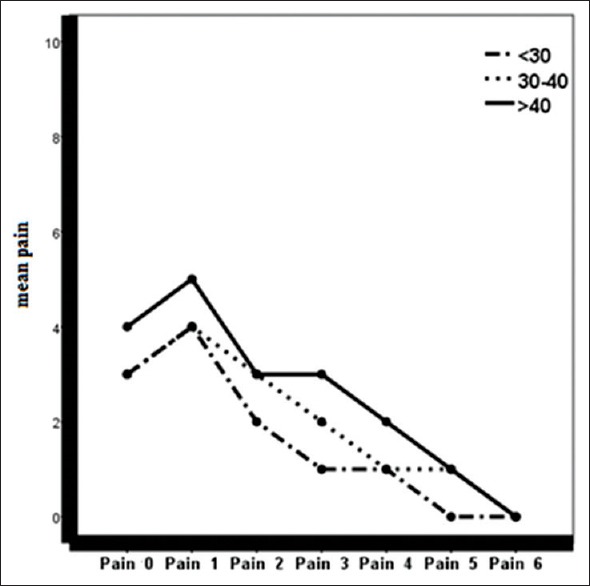
The mean pain perception at different times according to the age
DISCUSSION
In this study, the relationship between anxiety and pain perception was investigated after periodontal flap surgery, and the VAS scale was used for the evaluation of pain every day until removing of sutures which was similar to the study of Torres-Lagares et al.[1] Finally, in the trait anxiety assessment, significant differences were detected in pain perception between mild and moderate-to-low anxiety classes with relatively intense anxiety class immediately after surgery, between mild and moderate-to-low classes with moderate-to-high and relatively intense classes 1st day after surgery, and mild class with moderate-to-high and relatively intense classes in 2nd day after surgery, and in state anxiety study, significant differences were found in pain perception between mild and moderate-to-low anxiety classes with moderate-to-high and relatively intense classes immediately after surgery until the 5th day and these findings are coherent with studies of Torres-Lagares et al.,[1] González-Lemonnier et al.,[10] and Taenzer et al.[11] Furthermore, Vallerand et al. reported that trait anxiety is an accurate predictor of pain perception after surgery and recovery after oral surgery[12] that it has been approved for other types of surgeries.[13]
Daniel Torres-lagares et al. investigated the infl uence of state anxiety and trait anxiety in postoperative in oral surgery. The results of their studies showed that consumption of analgesic drugs was higher in positive trait anxiety group,[1] while in our study, no significant difference was detected between the mean of analgesic drugs consumption in the studied groups that it can be due to differences in culture in different societies, the threshold of pain tolerance and fear of drug side effects.
According to the results of Khorshidi et al.[14] and Kim et al.,[15] in this study, the pain perception in female was significantly higher than male, in immediately after surgery, 3rd day, and 5th day after surgery that can be due to the difference in pain tolerance in male and female and the tendency of women to express their problems.
Some previous studies have shown that the pain tolerance threshold increases with age which can be due to decreased blood flow, fatty changes in bone tissue, and tissue changes.[16] While there was no significant difference between age and pain perception in our study which is in agreement with results of Kim et al.,[15] Croog et al.,[5] and Sharma et al.[17] This inconsistency can be due to the difference in age groups and the investigated population in various studies.
One of the limitations of this study was that the scales were self-reported. It is suggested that in later studies, the patients are evaluated by structured interview.
Pain measurement is inherently difficult as it has both physical and psychological aspects[9] and is completely dependent on an individual's perceptions; therefore, the same therapeutic environment is necessary. Thus, surgery was performed in the same and quiet place and away from confusing factors by one periodontist. In this study, the effect of both aspects of state and trait anxiety on pain perception was studied after periodontal flap surgery, while in previous studies, only the effect of state anxiety was determined.
Research indicates that stress can have many physical effects, such as increase in sympathetic-adrenergic activity and reduce in postsurgical recovery.[18] Furthermore, it has been shown that anxious people overstate the severity of distressing events, such as fear and pain.[19] Unlike the past that surgical techniques and surgeons' skills were known as the most important factors affecting the success of surgery, nowadays control of patient's emotions is considered as a requirement for success. It is, therefore, important for dentists to have a thorough understanding of the factors influencing the pain and anxiety experienced by their patients. In this study, the factors affecting pain perception and the impact of these factors on improving the relationship between the dentist and patient, and reducing the pain perception after surgery, were investigated and identified.
CONCLUSIONS
According to the results obtained, anxiety is associated with pain perception following periodontal flap surgery, and female experience more pain after surgery, whereas the amount of pain perception is not related to age. Hence, regarding the association of anxiety with these factors, the use of anxiety reduction protocols can help reducing the pain experience in patients during the postoperative period.
FINANCIAL SUPPORT AND SPONSORSHIP
The study was supported financially by the Deputy of Research of Babol University of Medical Sciences.
CONFLICTS OF INTEREST
There are no conflicts of interest.
ACKNOWLEDGMENT
The authors thank Mrs. Mesgarian for collecting data. This study was supported financially by the Deputy of Research of Babol University of Medical Sciences.
REFERENCES
- 1.Torres-Lagares D, Recio-Lora C, Castillo-Dalí G, Ruiz-de-León-Hernández G, Hita-Iglesias P, Serrera-Figallo MA, et al. Influence of state anxiety and trate anxiety in postoperative in oral surgery. Med Oral Patol Oral Cir Bucal. 2014;19:e403–8. doi: 10.4317/medoral.19604. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Guzeldemir E, Toygar HU, Cilasun U. Pain perception and anxiety during scaling in periodontally healthy subjects. J Periodontol. 2008;79:2247–55. doi: 10.1902/jop.2008.080152. [DOI] [PubMed] [Google Scholar]
- 3.Lago-Méndez L, Diniz-Freitas M, Senra-Rivera C, Seoane-Pesqueira G, Gándara-Rey JM, García-García A, et al. Postoperative recovery after removal of a lower third molar: Role of trait and dental anxiety. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;108:855–60. doi: 10.1016/j.tripleo.2009.07.021. [DOI] [PubMed] [Google Scholar]
- 4.Janssen KJ, Kalkman CJ, Grobbee DE, Bonsel GJ, Moons KG, Vergouwe Y, et al. The risk of severe postoperative pain: Modification and validation of a clinical prediction rule. Anesth Analg. 2008;107:1330–9. doi: 10.1213/ane.0b013e31818227da. [DOI] [PubMed] [Google Scholar]
- 5.Croog SH, Baume RM, Nalbandian J. Pre-surgery psychological characteristics, pain response, and activities impairment in female patients with repeated periodontal surgery. J Psychosom Res. 1995;39:39–51. doi: 10.1016/0022-3999(94)00089-n. [DOI] [PubMed] [Google Scholar]
- 6.Sanikop S, Agrawal P, Patil S. Relationship between dental anxiety and pain perception during scaling. J Oral Sci. 2011;53:341–8. doi: 10.2334/josnusd.53.341. [DOI] [PubMed] [Google Scholar]
- 7.Barnes LL, Harp D, Jung WS. Reliability generalization of scores on the Spielberger State-trait anxiety inventory. Educ Psychol Meas. 2002;62:603–18. [Google Scholar]
- 8.Mahram B. Validity of Spielberger State-Trait Anxiety Inventory (STAI) in Mashhad City. Tehran: Allameh Tabatabaei University; 1993. [Google Scholar]
- 9.Canakci V, Canakci CF. Pain levels in patients during periodontal probing and mechanical non-surgical therapy. Clin Oral Investig. 2007;11:377–83. doi: 10.1007/s00784-007-0126-z. [DOI] [PubMed] [Google Scholar]
- 10.González-Lemonnier S, Bovaira-Forner M, Peñarrocha-Diago M, Peñarrocha-Oltra D. Relationship between preoperative anxiety and postoperative satisfaction in dental implant surgery with intravenous conscious sedation. Med Oral Patol Oral Cir Bucal. 2010;15:e379–82. doi: 10.4317/medoral.15.e379. [DOI] [PubMed] [Google Scholar]
- 11.Taenzer P, Melzack R, Jeans ME. Influence of psychological factors on postoperative pain, mood and analgesic requirements. Pain. 1986;24:331–42. doi: 10.1016/0304-3959(86)90119-3. [DOI] [PubMed] [Google Scholar]
- 12.Vallerand WP, Vallerand AH, Heft M. The effects of postoperative preparatory information on the clinical course following third molar extraction. J Oral Maxillofac Surg. 1994;52:1165–70. doi: 10.1016/0278-2391(94)90536-3. [DOI] [PubMed] [Google Scholar]
- 13.Chapman CR, Cox GB. Anxiety, pain, and depression surrounding elective surgery: A multivariate comparison of abdominal surgery patients with kidney donors and recipients. J Psychosom Res. 1977;21:7–15. doi: 10.1016/0022-3999(77)90020-4. [DOI] [PubMed] [Google Scholar]
- 14.Khorshidi H, Lavaee F, Ghapanchi J, Golkari A, Kholousi S. The relation of preoperative stress and anxiety on patients' satisfaction after implant placement. Dent Res J (Isfahan) 2017;14:351–5. doi: 10.4103/1735-3327.215968. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Kim S, Lee YJ, Lee S, Moon HS, Chung MK. Assessment of pain and anxiety following surgical placement of dental implants. Int J Oral Maxillofac Implants. 2013;28:531–5. doi: 10.11607/jomi.2713. [DOI] [PubMed] [Google Scholar]
- 16.Canakçi CF, Canakçi V. Pain experienced by patients undergoing different periodontal therapies. J Am Dent Assoc. 2007;138:1563–73. doi: 10.14219/jada.archive.2007.0105. [DOI] [PubMed] [Google Scholar]
- 17.Sharma S, Majumder K, Dayashankara Rao JK, Arya V, Siwach V, Gulia S. Assessment of relationship between pain and anxiety following dental extraction a prospective study. Pain Stud Treat. 2015;3:23–30. [Google Scholar]
- 18.Wolfer JA, Davis CA. Assessment of surgical patients' preoperative emotional condition and postoperative welfare. Nurs Res. 1970;19:402–14. [PubMed] [Google Scholar]
- 19.van Wijk AJ, Hoogstraten J. Experience with dental pain and fear of dental pain. J Dent Res. 2005;84:947–50. doi: 10.1177/154405910508401014. [DOI] [PubMed] [Google Scholar]