

Abstract
Background
The proportion of elderly people living in Poland has risen in recent years. With rising life expectancy, there is likely to be a concurrent increase in the incidence of chronic diseases and disabilities. Therefore, this study aimed to analyze the prevalence of chronic diseases and disability of the elderly in order to help guide strategies of prevention and public health control.
Material/Methods
This was a cross-sectional study of 1,000 randomly-selected residents living in the Podkarpackie region of Poland. The WHODAS 2.0 questionnaire was used to assess the disability and functioning of the participants across six domains of functioning using the following scores: no disability (0–4%), mild disability (5–24%), moderate disability (25–49%), severe disability (50–95%), and extreme disability (96–100%).
Results
The presence of at least one chronic disease was identified in 84.1% of participants. The most common diseases were: circulatory diseases (59.10%), spinal pain syndromes (51.50%), degenerative joint diseases (50.30%), and rheumatic diseases (23.90%). Severe or extreme disability was found in 8.46% of patients with circulatory disease, 9.32% of patients with spinal pain syndromes, 9.34% of patients with degenerative joint diseases, and 12.13% of patients with rheumatic diseases.
Conclusions
Based on our findings, we recommend an emphasis be placed on early diagnosis of chronic diseases. We also recommend implementing methods of primary and secondary prevention aimed at reducing or eliminating disability resulting from chronic diseases. Our research highlights the need to plan targeted support and prevention programs using strategies that optimize social participation of older people with various chronic diseases.
MeSH Keywords: Aged, Chronic Disease, Disabled Persons
Background
Global aging of society has caused worldwide concern, primarily due to the increased burden placed on social and healthcare systems [1]. As people age, their physical and mental health and quality of life may deteriorate due to increased occurrence of diseases and/or disability [2]. Therefore, identifying diseases that affect health and functioning in the elderly population may be helpful in defining strategies for prevention and public health control [3].
In recent decades, developments in medicine and public health, improved living conditions, and increased education have contributed to the reduction of mortality and to greater life expectancy in most regions around the world [4]. In 2015, just over 96 million people aged 65 and older lived in the European Union (EU) Member States, constituting 18.9% of the population; this was a 32.7 million increase since 1985 [5]. In Poland, the number of people aged 65 and older was 5.8 million in 2014, with forecasts of reaching over 8 million by 2030 [6].
Data from the Global Burden Disease Study (2010) showed that even though the average life expectancy increased between 1990 and 2010, the average healthy life expectancy increased more slowly, and relatively little progress has been observed in the reduction of chronic diseases [4]. The study also noted that for every one-year increase in average life expectancy for men, only 0.75 years were spent in a healthy condition; for women this was only 0.77 years [4]. Poland has some of the lowest rates compared to other EU member states: the average healthy life expectancy for women aged 65 years is 7.8 years (EU average=10.3) and for men, 7.2 years (EU average=10.4) [7].
Increasing population life expectancy leads to a concurrent increase in the occurrence of chronic diseases [8]. In addition, the number of chronic diseases occurring in one person also increases with age [9]. According to Barnett et al., multimorbidity occurs in 65% of people aged 64–84 years and in 82% of those aged over 85 years [10]. Prince et al. showed that 23% of the total disease burden affects people aged 60 years and older [11]. The authors pointed out that cardiovascular diseases, malignant neoplasms, chronic respiratory diseases, musculoskeletal diseases, as well as mental and neurological disorders are the main contributors to disease burden.
The increased prevalence of chronic diseases among the elderly may lead to an increased prevalence of disability [12]. According to the World Report on Disability, 15% of people worldwide live with disabilities, including 2–4% experiencing serious problems in their functioning [13]. Furthermore, the data presented by Eurostat indicated that 28% of people in Europe suffer from a disease and/or difficulty with basic activities [14]. In Poland, the number of people with disabilities accounts for 12.2% of the population, including 10.1% who need help with basic everyday activities [15].
Recent studies investigating the current and predicted state of health of people aged older than 60 years have, however, have shown conflicting results. Some predicted a decrease in disability in elderly populations compared to previous generations [16–18], while others indicated that increasing life expectancy will be accompanied by an increase in disability among people older than the age of 60, mainly due to a higher incidence of chronic diseases [19,20]. Finally, some studies have predicted a reduction in the number of older people with moderate and severe disabilities, and a growing proportion of older people with mild disabilities [21].
As research trends in morbidity and disability in the elderly population have presented contradictory conclusions so far, more studies are encouraged [22]. In particular, studies using similar methodologies are necessary to accurately compare the relationships between aging and levels of functioning on an international scale. In order to solve this problem, the World Health Organization (WHO) introduced a tool to assess disability based on the International Classification of Functioning, Health, and Disability (ICF) – Disability Assessment Schedule-3.6 (WHODAS 2.0) [23].
In this study, we aimed to analyze the prevalence of chronic diseases and disability across the six domains of functioning among an elderly population in Poland. This is the first study to use the ICF-based tool in Poland to measure the health status of a population and to indicate the burden of disability according to the most prevalent long-term diseases among the elderly.
Material and Methods
This was a cross-sectional study representative of residents living in the Podkarpackie region of south-eastern Poland. The primary study population of 1,000 participants was randomly selected without replacement (using IBM SPSS Statistics v.23) from the Universal Electronic System for Registration of the Population (PESEL) database (full name, address, and PESEL number). The remaining 5,029 people in the PESEL database constituted a reserve population.
A questionnaire was completed via the Pen and Paper Interview (PAPI) method at participants’ homes. We focused on participants aged 60–70 years old with proper cognitive state. The study population also included participants in the pre-retirement age group, in which there are particular expectations to maintain effective professional activity.
The study protocol received approval by the Bioethical Committee of the University of Rzeszów and all participants signed an informed consent.
Research tools
Basic sociodemographic data was collected for all participants, including age, gender, place of living, marital status, education, status in the labor market, and income.
Disability was measured with the 36-item WHODAS 2.0 tool developed based on the ICF [23]. This tool measures the levels of functioning across six domains of life: cognition (Domain 1); mobility (Domain 2); self-care (Domain 3); getting along (Domain 4); life activities — domestic responsibilities (Domain 5.1); work and school (Domain 5.2 — results in this domain were only received from professionally active people, i.e., only 9.20% of the study population and therefore were not included in the current analysis); and participation (Domain 6) [24]. The questionnaire was translated and adapted for Polish conditions by a team of experts, who were members of the Council for the ICF.
When assessing the level of disability with the WHODAS 2.0, the following scale (consistent with the ICF) was used: no disability or an insufficient problem (0–4%), mild disability or a small problem (5–24%), moderate disability or a significant problem (25–49%), severe disability or a big problem (50–95%), and extreme disability or a total problem (96–100%) [25].
Statistical analysis
The obtained data were analyzed by STATISTICA version 10 and presented as the mean and standard deviation (SD) unless otherwise indicated. The following statistical tests were used: descriptive statistics and an independent chi-square test. Statistical significance was set at p < 0.05.
Results
Table 1 presents the basic socio-demographic characteristics of the study population. The occurrence of at least one chronic disease diagnosed by a physician was identified in 84.1% of the population. The number of chronic diseases increased with age (p<0.001; Table 2). As for people aged 60 to 65 years, the proportion of people without chronic illnesses was significantly higher than people aged 66–70 years (it was 11.58% higher). The opposite situation was found in the case of five or more chronic diseases, where in the 60–65 year age group this proportion was 11.83% lower than among people aged 66–70 years. The mean number of chronic diseases diagnosed by a physician was 4.17 per individual (SD=3.61). We found that as the number of chronic diseases increased, the level of disability also increased (p<0.001; Table 3).
Table 1.
Sociodemographic characteristics of the study population.
| Demographic characteristics | Age 60–65 years (n=570) | Age 66–70 years (n=430) | ||
|---|---|---|---|---|
| Number (n) | Percentage (%) | Number (n) | Percentage (%) | |
| Gender | ||||
| Female | 325 | 57.02 | 237 | 55.12 |
| Male | 245 | 42.98 | 193 | 44.88 |
| Place of living | ||||
| City/town | 257 | 45.09 | 196 | 45.58 |
| Countryside | 313 | 54.91 | 234 | 54.42 |
| Marital status | ||||
| Bachelor/spinster | 37 | 6.49 | 12 | 2.79 |
| Married | 449 | 78.77 | 300 | 69.77 |
| Separated/divorced | 22 | 3.86 | 7 | 1.63 |
| Widower/widow | 55 | 9.65 | 107 | 24.88 |
| Living with a partner | 7 | 1.23 | 4 | 0.93 |
| Education | ||||
| Primary | 130 | 22.81 | 147 | 34.19 |
| Vocational education | 197 | 34.56 | 110 | 25.58 |
| Secondary comprehensive | 53 | 9.30 | 37 | 8.60 |
| Secondary vocational | 123 | 21.58 | 86 | 20.00 |
| Tertiary | 67 | 11.75 | 50 | 11.63 |
| Status on the labour market | ||||
| Working | 86 | 15.08 | 6 | 1.39 |
| Not working | 484 | 84.92 | 424 | 98.61 |
| Income per person per month | ||||
| Up to 1000 PLN* | 53 | 9.30 | 43 | 10.00 |
| 1001–2000 PLN | 137 | 20.04 | 137 | 31.86 |
| 2001–3000 PLN | 80 | 14.04 | 70 | 16.28 |
| 3001 PLN and more | 65 | 11.40 | 48 | 11.16 |
| No data | 235 | 41.23 | 132 | 30.70 |
PLN – (Polish zloty) – the official name of the Polish currency.
Table 2.
Structure of the study population depending on the age and number of diseases.
| Age | Total | ||||
|---|---|---|---|---|---|
|
| |||||
| 60–65 years | 66–70 years | ||||
| The number of diseases | 0 | Population | 119 | 40 | 159 |
| % | 20.88% | 9.30% | 15.90% | ||
|
| |||||
| 1–2 | Population | 132 | 99 | 231 | |
| % | 23.16% | 23.02% | 23.10% | ||
|
| |||||
| 3–4 | Population | 120 | 90 | 210 | |
| % | 21.05% | 20.93% | 21.00% | ||
|
| |||||
| 5 and more | Population | 199 | 201 | 400 | |
| % | 34.91% | 46.74% | 40.00% | ||
|
| |||||
| Total | Population | 570 | 430 | 1 000 | |
| % | 100.00% | 100.00% | 100.00% | ||
Using chi square test.
Table 3.
Structure of the study population according to the number of diseases and level of disability.
| Number of diseases | Total | ||||||
|---|---|---|---|---|---|---|---|
|
| |||||||
| 0 | 1–2 | 3–4 | 5 or more | ||||
| Disability | No disability | Population | 136 | 97 | 44 | 53 | 330 |
| % | 85.53% | 41.99% | 20.95% | 13.25% | 33.00% | ||
|
| |||||||
| Mild disability | Population | 19 | 115 | 125 | 203 | 462 | |
| % | 11.95% | 49.78% | 59.52% | 50.75% | 46.20% | ||
|
| |||||||
| Moderate disability | Population | 2 | 13 | 32 | 98 | 145 | |
| % | 1.26% | 5.63% | 15.24% | 24.50% | 14.50% | ||
|
| |||||||
| Severe or extreme disability | Population | 2 | 6 | 9 | 46 | 63 | |
| % | 1.26% | 2.59% | 4.29% | 11.50% | 6.30% | ||
|
| |||||||
| Total | Population | 159 | 231 | 210 | 400 | 1 000 | |
| % | 100.00% | 100.00% | 100.00% | 100.00% | 100.00% | ||
Using chi square test.
The most common diseases in the study population were: circulatory diseases (59.10% of the studied population) including hypertension (51.0%) and coronary disease (23.8%); spinal pain syndromes (51.50%) including lumbar spine (41.5%) and cervical spine (31.2%); degenerative joint diseases (50.30%) including degenerative spine disease (39.0%) and peripheral joints (33.3%); and rheumatic diseases (23.9%).
A similar degree of disability was observed in individuals with at least one disease (circulatory, spinal pain syndrome, degenerative or rheumatic disease). Mild disability was discovered in about half (on average) of the population suffering from at least one disease from the aforementioned groups. Moderate disability was observed in every fifth person. The number of people with moderate disability was 28.03% in the case of rheumatic diseases alone. Severe and extreme disability was noted in almost 10.00% of the study population with at least one circulatory or degenerative disease, or with spinal pain syndrome. As for rheumatic diseases, there were slightly more individuals with severe or extreme disability (12.13%; Table 4).
Table 4.
Degree of disability of the study population in each group of diseases.
| Types of diseases | ||||||
|---|---|---|---|---|---|---|
|
| ||||||
| Circulatory diseases | Spinal pain syndromes | Degenerative diseases | Rheumatic disease | |||
| Disability | No disability | Population | 126 | 80 | 84 | 24 |
| % | 21.32% | 15.53% | 16.70% | 10.04% | ||
|
| ||||||
| Mild disability | Population | 303 | 284 | 271 | 119 | |
| % | 51.27% | 55.15% | 53.88% | 49.79% | ||
|
| ||||||
| Moderate disability | Population | 112 | 103 | 101 | 67 | |
| % | 18.95% | 20.00% | 20.08% | 28.03% | ||
|
| ||||||
| Severe or extreme disability | Population | 50 | 48 | 47 | 29 | |
| % | 8.46% | 9.32% | 9.34% | 12.13% | ||
|
| ||||||
| Total | Population | 591 | 515 | 503 | 239 | |
| % | 100.00% | 100.00% | 100.00% | 100.00% | ||
In people with circulatory diseases, the greatest problems with functioning were observed within the participation domain (Domain 6): almost 90% of this subgroup had difficulty in normal participation in social life, with 45.18% experiencing at least moderate problems. The problems were mainly caused by a significant amount of time devoted to health-related issues and a negative impact of the disease on the emotional condition and financial status of the patients. Problems in mobility (Domain 2) were also observed in those with circulatory diseases: 36.21% had at least moderate problems moving around. These were primarily related to standing longer than 30 minutes and walking long distances (e.g., 1 km). Moreover, older people with circulatory diseases tended to experience limitations in their activity and carrying out life activities (Domain 5.1), as well as difficulty in getting along (Domain 4). The least significant problem in this subgroup was observed in the domain of self-care, such as maintaining hygiene, getting dressed, eating, and staying home alone (Figure 1).
Figure 1.
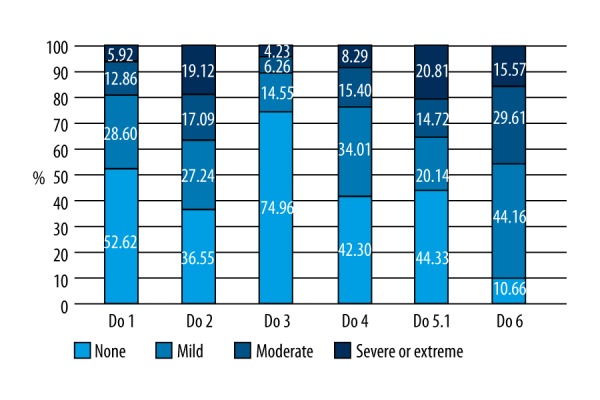
Disability in each domain among people with circulatory diseases
Similar problems were observed among people with degenerative diseases of the joints and spinal pain syndromes. The greatest limitations in this subgroup were observed within the participation domain (Domain 6) and were mainly attributed to the health condition itself and spending too much time on health-related issues. More than 90% of those with degenerative diseases of the joints and spinal pain syndromes experienced limitations in participating in social life. More than two thirds of people with musculoskeletal diseases also suffered from mobility problems (Domain 2), including difficulty in standing for more than 30 minutes, standing after sitting, and walking long distances. People in this subgroup also experienced significant limitations in carrying out complex life activities in their households (Domain 5.1); further difficulties pertained to getting along (Domain 4), including sexual activity. Cognitive distortions related to understanding and communication (Domain 1) occurred in more than half of the people with degenerative diseases of the joints and spinal pain syndromes. The least problematic domain for this subgroup was the one covering self-care (Domain 3) (Figures 2, 3).
Figure 2.

Disability in each domain among people with degenerative diseases of the joints
Figure 3.

Disability in each domain among people with spinal pain syndrome
People with rheumatic diseases showed even poorer functioning in each domain, with the greatest problems pertaining to participation (Domain 6). As many as 96.23% of this subgroup had difficulty in normal participation in social life; 59.41% experienced at least moderate problems. Mobility (Domain 2) was another area where significant limitations in functioning occurred: 51.05% had at least moderate problems with movement. People with rheumatic diseases also showed great difficulty in performing complex life activities in their households (Domain 5.1): 47.28% reported at least moderate problems with doing their household duties. Indeed, those with rheumatic diseases are often unable to perform all household duties or do them more slowly. Those with rheumatic diseases also showed significant problems in getting along with others (Domain 4). In addition, cognitive distortion related to understanding and communication (Domain 1) was observed in 59% of patients with rheumatic diseases. Self-care (Domain 3) was ranked as a minor problem in this subgroup of people (Figure 4).
Figure 4.

Disability in each domain among people with rheumatic diseases
The mean time of temporary disability for the entire study population was 2.82 days for limitations in doing life activities or work, and 2.02 days for complete inability to perform life activities or work. As the number of chronic diseases increased, the length of temporary disability in performing life activities or work was also extended. The more chronic diseases a person suffers from, the more likely they are to limit or refrain from doing usual life activities or work (Table 5).
Table 5.
Limitations or completely giving up doing life activities or work within the last 30 days due to ill health.
| Number of chronic diseases per person | Number of people with a specific number of chronic diseases | Number (%) of people with limitations in doing life activities/work within the last 30 days | Number (%) of people who completely gave up doing life activities/ work within the last 30 days | Mean number of the days of temporary disability | Standard deviation |
|---|---|---|---|---|---|
| 0 | 159 | 7 (4.40%) | 5 (3.14%) | 0.50 | 3.46 |
| 1–2 | 231 | 36 (15.58%) | 22 (9.52%) | 1.36 | 4.75 |
| 3–4 | 210 | 67 (31.90%) | 65 (30.95%) | 2.87 | 7.21 |
| 5 and more | 400 | 201 (50.25%) | 164 (41.00%) | 4.55 | 7.95 |
The average time of indisposition of people without chronic illnesses in the past 30 days was 0.5 days of restricted normal activities or work and 0.41 days of complete cessation of normal activities or work. The average time of indisposition increased with the number of chronic diseases occurring in one person. The average duration of restriction of normal activities or work was 9 times longer among people with five or more chronic diseases than those without any chronic diseases, whereas the average time of complete cessation of normal activities or work was 8 times longer.
The mean time of temporary disability for people with the most common chronic diseases was much longer than the mean time of temporary disability calculated for the entire study population (Table 6).
Table 6.
Number of people and mean time of temporary disability among people with the most common chronic diseases.
| Group of chronic diseases | Number of people in whom at least one disease from the group was identified | Number of people (%) in whom at least 1 chronic disease was diagnosed, which limited their working capacity or ability to do life activities | Mean number of days of limited working capacity or ability to do life activities | Number of people (%) in whom at least 1 chronic disease was diagnosed, which completely prevented them from working or doing life activities | Mean number of days of completely refraining from work or doing life activities |
|---|---|---|---|---|---|
| Circulatory diseases | 591 | 238 (40.27%) | 8.69 | 206 (34.86%) | 7.42 |
| Spinal pain syndromes | 515 | 217 (42.14%) | 9.16 | 175 (33.98%) | 7.83 |
| Degenerative diseases | 503 | 219 (43.54%) | 9.21 | 190 (37.77%) | 8.01 |
| Rheumatic diseases | 239 | 114 (47.70%) | 9.28 | 95 (39.75%) | 8.23 |
The mean time of temporary disability in the last 30 days among people with the most common chronic diseases was between 8.69 and 9.28 days of limited capacity to do common life activities or work, and between 7.42 and 8.23 days for complete inability to perform usual life activities or work.
Discussion
Our study involved an analysis of the prevalence of chronic diseases and disability among older people living in south eastern Poland. We found that the prevalence of at least one disease diagnosed by a physician in people aged 60–70 years was as high as 84.10%; and an older person suffered from an average of four chronic diseases. The most common reported diseases were circulatory diseases (59.10%), spinal pain syndromes (51.50%), degenerative joint diseases (50.30%), and rheumatic diseases (23.90%). Our analysis showed that, as the number of diseases increased, the degree of disability of the study persons increased significantly. We have observed a pattern of limitations leading to disability among the elderly regardless the type of chronic diseases. The biggest problem was in social participation. Another area of concern was mobility, mainly related to difficulty standing for long periods of time and walking long distances. The next most commonly occurring problem was carrying out complex life activities in the household.
There was a very high prevalence of chronic diseases among the inhabitants of south eastern Poland (the Podkarpackie region) who were aged 60–70 years: almost 85% of the study population had at least one diagnosed chronic disease. Similarly, a study carried out by GUS (The Central Statistical Office of Poland) on the health of the Polish population showed that the average number of chronic diseases among a group of people aged 60–69 years was 3.1 in 2016 [26]. With regards to the Podkarpackie region, we found the mean was higher at 4.16 (median=4, SD=3.6) in 2016. We also observed that the more chronic diseases a person suffered from, the higher their degree of disability.
The most common health problems of those aged 60–70 years in the Podkarpackie region were chronic circulatory diseases and musculoskeletal diseases. Our study results were consistent with GUS data on the most common chronic diseases among older people in Poland [26]. Similarly, Eurostat studies have indicated that the main and long-term diseases among the elderly include cardiovascular diseases, cancer, mental health problems, diabetes, respiratory diseases, and musculoskeletal diseases [27]. Moreover, according to the Global Burden of Disease Study, disability was most often caused by musculoskeletal disorders and depressive disorders during 2005 to 2015 [28].
Circulatory diseases were observed in 59.1% of our study population in the Podkarpackie region, most commonly hypertension, coronary disease, atherosclerosis, myocardial infarction, and stroke. Indeed, previous studies have indicates circulatory diseases were a strong predictor of the prevalence of disability in elderly populations [29,30]. While developments in cardiology have reduced mortality rates and incidence of severe disability associated with circulatory diseases [31], they have also resulted in a longer life expectancy that is not necessarily of high quality and individuals are often limited in their functional efficiency [32]. Indeed, circulatory diseases are among the most common causes of inability to live independently [33]. Therefore, disability related to circulatory diseases remains a major public health problem [30].
The most common chronic musculoskeletal diseases observed in our study population were spinal pain syndromes (51.50%), degenerative diseases of the spinal column and peripheral joints (50.30%), and rheumatic diseases (23.90%). Musculoskeletal diseases, including pain syndromes, represent some of the most common chronic diseases, especially among people older than the age of 60 [34]. Indeed, chronic diseases together with the associated pain and structural limitations of the body in conjunction with environmental barriers cause disability in patients with different degrees of severity [35]. In addition, musculoskeletal disorders are often closely linked to working conditions [36]. In studies carried out in Poland with regard to the adaptation of work places for older people, it was found that efforts to promote health, as well as the organisation and adaptation of working 7conditions to the needs of the elderly, are only taken into consideration to a small extent [37]. Furthermore, actions aimed at employing older workers and age management are only conducted in a few companies in Poland, and less than 7% of companies provide advice on healthcare. Therefore, programs aimed at extending working life and the ability to work longer are currently very poorly implemented in Poland [38].
Among those with diagnosed chronic diseases in our study, almost half (40–47%) were limited in their ability to perform ordinary life activities or work for 8.69 to 9.28 days on average in the last 30 days, and more than one third (35–40%) had refrained entirely from performing ordinary activities or work for 7.42 to 8.23 days on average. Similarly, Van Houtum et al. indicated that in a group of more than 1,500 people with chronic diseases, 37% experienced difficulty in their daily lives, of which 20% reported a problem in their basic daily activities [39]. Elderly people with chronic diseases were also previously shown to need support (apart from traditional medical care) in dealing with everyday problems and with life situations that are important to them [40].
We found the degree of disability among those with diagnosed chronic diseases was high in Poland. Moderate, severe, and extreme disability (i.e., disability that disrupts normal human functioning to a great extent) occurred in 30–40.06% of the study population with the most common chronic diseases. These people with a severe or extreme disability will require occasional or regular assistance in their everyday life. Similarly, a study involving a Spanish population revealed that 51.5% of the elderly had moderate disability, which was significantly associated with cognitive impairment, cerebrovascular diseases, and locomotor diseases [41]. In contrast, a study conducted in the United States reported a lower incidence of disability among the elderly (25.4%) [42]. Therefore, the rate of disability among the elderly appears to be country specific. Indeed, another study found that disability associated with aging was primarily related to older people in low- and middle-income countries [43].
Among the elderly Polish population, we found the greatest problem in the domain of participating in social life. More than 90% of participants mentioned problems in this area, with almost half experiencing at least moderate problems. This domain measures a person’s involvement in life situations and their motivation to take actions. The problem that a person can experience in various life situations depends on two factors: their abilities and the actual performance of activity. A careful analysis of the responses from the study population revealed that health problems limited their participation in social life, including difficulties in overcoming environmental barriers relating to their health problems. Their emotional condition and financial status were also negatively affected. We found problems in participation in social life were closely related to difficulties associated with mobility and performing complex life activities, such as standing longer than 30 minutes, standing from a sedentary position, walking long distances, carrying out all household duties, and the speed in which activities were completed. Indeed, according to Warren et al., a slower pace of walking was significantly associated with reduced participation of older people in social life [44]. Furthermore, dysfunctions in the lower limbs and pain associated with coexisting diseases have previously been shown to have a direct and indirect impact on social roles [45]. Previous studies also point to the fact that older people who are more active in social life are also more physically active and have lower levels of disability [46,47]. Finally, Tomioka et al. stated that social activity influences the maintenance of independence, but this differs according to gender: that is, increasing social activity was significantly related to a lower amount of functional limitations for women in particular [48].
Conclusions
The health status of the elderly depends on various factors, and those with multimorbidity appear to be most affected. About 80% of the elderly with multimorbidity live their remaining years with disability [49]. However, some older people are able to achieve lower levels of deficiency and disability so that they can prolong their professional life. We observed a high incidence of chronic diseases and an associated high level of disability among elderly people in the Podkarpackie region. To overcome the burden this is placing on our social and healthcare systems, we recommend that emphasis be placed on early diagnosis of chronic diseases in Poland. We also recommend that systems of primary and secondary prevention be developed, aimed at reducing or even eliminating disability resulting from chronic disease in the elderly. Our research highlights the need to plan targeted support and prevention programs using strategies that optimize social participation of older people suffering from various chronic diseases.
Acknowledgements
The authors thank “IBERiS” Evaluation, Market and Social Sciences Research Institute for professional help to carry out the survey. The authors also thank Proper Medical Writing sp. z. o.o. for making linguistic corrections of the article.
Footnotes
Conflict of interests
None.
Source of support: This work was supported by a statutory research grant from the University of Rzeszów
References
- 1.Jagger C, Gillies C, Moscone F, et al. Inequalities in healthy life years in the 25 countries of the European Union in 2005: A cross-national meta-regression analysis. Lancet. 2008;372:2124–31. doi: 10.1016/S0140-6736(08)61594-9. [DOI] [PubMed] [Google Scholar]
- 2.Yang M, Ding X, Dong B. The measurement of disability in the elderly: A systematic review of self-reported questionnaires. J Am Med Dir Assoc. 2014;150:e1–e9. doi: 10.1016/j.jamda.2013.10.004. [DOI] [PubMed] [Google Scholar]
- 3.Bauer UE, Briss PA, Goodman RA, Bowman BA. Prevention of chronic disease in the 21st century: Elimination of the leading preventable causes of premature death and disability in the USA. Lancet. 2014;384:45–52. doi: 10.1016/S0140-6736(14)60648-6. [DOI] [PubMed] [Google Scholar]
- 4.Salomon JA, Wang H, Freeman MK, et al. Healthy life expectancy for 187 countries, 1990–2010: A systematic analysis for the Global Burden Disease Study 2010. Lancet. 2012;380(9859):2144–62. doi: 10.1016/S0140-6736(12)61690-0. [DOI] [PubMed] [Google Scholar]
- 5.Eurostat. Population structure and ageing. Available from: URL: http://ec.europa.eu/eurostat/statistics-explained/index.php/Population_structure_and_ageing [cited 2017 May 28]
- 6.The Central Statistical Office. [The demographic structure of the population aged 60 years in Poland]. Warsaw: 2016. [in Polish] [Google Scholar]
- 7.The Central Statistical Office. [The demographic structure of older people and the consequences of the ageing of the population in the light of the Polish forecasts for the period 2014–2015]. Warsaw: 2014. [in Polish] [Google Scholar]
- 8.Orueta JF, Nuño-Solinis R, et al. Monitoring the prevalence of chronic conditions: Which data should we use? BMC Health Serv Res. 2012;12:365. doi: 10.1186/1472-6963-12-365. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Salisbury C, Johnson L, Purdy S, et al. Epidemiology and impact of multimorbidity in primary care: A retrospective cohort study. Br J Gen Pract. 2011;61:12–21. doi: 10.3399/bjgp11X548929. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Barnett K, Mercer SW, Norbury M, et al. Epidemiology of multimorbidity and implications for health care, research, and medical education: A cross-sectional study. Lancet. 2011;380:37–43. doi: 10.1016/S0140-6736(12)60240-2. [DOI] [PubMed] [Google Scholar]
- 11.Prince MJ, Wu F, Guo Y, et al. The burden of disease in older people and implications for health policy and practice. Lancet. 2015;385(9967):549–62. doi: 10.1016/S0140-6736(14)61347-7. [DOI] [PubMed] [Google Scholar]
- 12.Yokota RT, Berger N, Nusselder WJ, et al. Contribution of chronic diseases to the disability burden in a population 15 years and older, Belgium, 1997–2008. BMC Public Health. 2015;15:229. doi: 10.1186/s12889-015-1574-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.World Health Organization. World Report on Disability. Geneva, Switzerland: 2011. [Google Scholar]
- 14.Eurostat. Disability statistics. Available from: URL: http://ec.europa.eu/eurostat/statistics-explained/index.php/Disability_statistics_-_health [cited 2017 May 29]
- 15.The Central Statistical Office. [People with disabilities on the labour market in 2011]. Warsaw: 2012. [in Polish] [Google Scholar]
- 16.Doblhammer G, Kytir J. Compression or expansion of morbidity? Trends in healthy-life expectancy in the elderly Austrian population between 1978 and 1998. Soc Sci Med. 2001;52:385–91. doi: 10.1016/s0277-9536(00)00141-6. [DOI] [PubMed] [Google Scholar]
- 17.Manton KG. Recent declines in chronic disability in the elderly US population: Risk factors and future dynamics. Annu Rev Publ Health. 2008;29:91–113. doi: 10.1146/annurev.publhealth.29.020907.090812. [DOI] [PubMed] [Google Scholar]
- 18.Ziegler U, Doblhammer G. Cohort changes in the incidence of care need in West Germany between 1986 and 2005. Eur J Popul. 2008;24:347–62. [Google Scholar]
- 19.Crimmins EM. Trends in the health of the elderly. Annu Rev Publ Health. 2004;25:79–98. doi: 10.1146/annurev.publhealth.25.102802.124401. [DOI] [PubMed] [Google Scholar]
- 20.Lahariya C, Khandekar J, Pradhan SK. Effect of impairment and disability on health related quality of life of elderly: A community based study from urban India. Indian J Community Med. 2012;37(4):223–26. doi: 10.4103/0970-0218.103469. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Perenboom RJ, van Herten LM, Boshuizen HC, van den Bos GA. Trends in disability-free life expectancy. Disabil Rehabil. 2004;26(7):377–86. doi: 10.1080/0963828032000174098. [DOI] [PubMed] [Google Scholar]
- 22.Christensen K, Doblhammer G, Rau R, Vaupel JW. Ageing populations: The challenges ahead. Lancet. 2009;374(9696):1196–208. doi: 10.1016/S0140-6736(09)61460-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Federici S, Meloni F, Mancini A, et al. World health organization disability assessment schedule II: Contribution to the Italian validation. Disabil Rehabil. 2009;31(7):553–64. doi: 10.1080/09638280802240498. [DOI] [PubMed] [Google Scholar]
- 24.Üstün TB, Kostanjsek N, Chatterji S, Rehm J. Measuring health and disability manual for WHO disability Assessment Schedule WHODAS 2.0. WHO; 2010. [Google Scholar]
- 25.The World Health Organization. [International Classification of Functioning Disability and Health (ICF), Centre for Health information systems]. Warsaw: 2009. [in Polish] [Google Scholar]
- 26.The Central Statistical Office. Population aged 60+. Demographic structure and health. Warsaw: 2016. [in Polish] [Google Scholar]
- 27.Eurostat. Major and chronic diseases. Available from: URL: https://ec.europa.eu/health/major_chronic_diseases/diseases_en [cited 2017 May 31]
- 28.GBD 2015 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388(10053):1545–602. doi: 10.1016/S0140-6736(16)31678-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Li C, Chiu Y, Chang H, et al. Association of geriatric conditions and cardiovascular diseases with disability in older adults with diabetes: Findings from a nationally representative survey. Geriatr Geronto Int. 2013;13(3):563–70. doi: 10.1111/j.1447-0594.2012.00935.x. [DOI] [PubMed] [Google Scholar]
- 30.Wang Z, Cao C, Guo C, et al. Socioeconomic inequities and cardiovascular disease-related disability in China: A population-based study. Medicine. 2016;95(32):e4409. doi: 10.1097/MD.0000000000004409. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Błędowski P, Wilmowska-Pietruszyńska A. [Long-term care organization in Poland-problems and related solutions]. Social Policy. 2009;7:9–13. [in Polish] [Google Scholar]
- 32.Wróblewska W. [Extending the life and changes in the health status of the population]. Social Policy. 2012:14–20. [in Polish] [Google Scholar]
- 33.Golinowska S, Sowa A. [Health and efficiency. Transformation in Poland]. Social Policy. 2012:6–14. [in Polish] [Google Scholar]
- 34.Miranda V, de Carvalho V, Machado L, Dias J. Prevalence of chronic musculoskeletal disorders in elderly Brazilians: A systematic review of the literature. BMC Musculoskel Dis. 2012;13(1):82–92. doi: 10.1186/1471-2474-13-82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.da Costa B, Vieira E. Risk factors for work-related musculoskeletal disorders: A systematic review of recent longitudinal studies. Am J Ind Med. 2010;53(3):285–323. doi: 10.1002/ajim.20750. [DOI] [PubMed] [Google Scholar]
- 36.Hildt-Ciupińska K, Bugajska J. Evaluation of activities and needs of older workers in the context of maintaining their employment. Med Pr. 2013;64(3):297–306. [PubMed] [Google Scholar]
- 37.Bugajska J, Hildt-Ciupińska K. World Report on Disability. Geneva, Switzerland: 2011. Evaluation of activities targeted at employability of older workers in World Health Organization. [Google Scholar]
- 38.Bugajska J, Hildt-Ciupińska K. [Evaluation of activities targeted at employability of older workers in Polish enterprises]. Med Pr. 2012;63(4):453–62. [in Polish] [PubMed] [Google Scholar]
- 39.van Houtum L, Rijken M, Groenewegen P. Do everyday problems of people with chronic illness interfere with their disease management? BMC Public Health. 2015;15:1000. doi: 10.1186/s12889-015-2303-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Cramm JM, Nieboer AP. Chronically ill patients’ self-management abilities to maintain overall well-being: what is needed to take the next step in the primary care setting? BMC Fam Pract. 2015;16:123. doi: 10.1186/s12875-015-0340-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Rodríguez-Blázquez C, Damián J, Andrés-Prado MJ, et al. Associations between chronic conditions, body functions, activity limitations and participation restrictions: A cross-sectional approach in Spanish non-clinical populations. BMJ Open. 2016;6(6):e010446. doi: 10.1136/bmjopen-2015-010446. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Hung WW, Ross JS, Boockvar KS, Siu AL. Recent trends in chronic disease, impairment and disability among older adults in the United States. BMC Geriatr. 2011;11:47. doi: 10.1186/1471-2318-11-47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Biritwum RB, Minicuci N, Yawson AE, et al. Prevalence of and factors associated with frailty and disability in older adults from China, Ghana, India, Mexico, Russia and South Africa. Maturita. 2016;91:8–18. doi: 10.1016/j.maturitas.2016.05.012. [DOI] [PubMed] [Google Scholar]
- 44.Warren M, Ganley KJ, Pohlb PS. The association between social participation and lower extremity muscle strength, balance, and gait speed in US adults. Prev Med Rep. 2016;4:142–47. doi: 10.1016/j.pmedr.2016.06.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Beauchamp MK, Jette AM, Ni P, et al. Leg and trunk impairments predict participation in life roles in older adults: Results from Boston RISE. J Gerontol A Biol Sci Med Sci. 2016;71(5):663–69. doi: 10.1093/gerona/glv157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.James BD, Boyle PA, Buchman AS, et al. Relation of late-life social activity with incident disability among community-dwelling older adults. J Gerontol A Biol Sci Med Sci. 2011;66A:467–73. doi: 10.1093/gerona/glq231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Kanamori S, Kai Y, Aida J, et al. Social participation and the prevention of functional disability in older Japanese: The JAGES cohort study. PLoS One. 2014;9:e99638. doi: 10.1371/journal.pone.0099638. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Tomioka K, Kurumatani N, Hosoi H. Association between social participation and 3-year change in instrumental activities of daily living in community-dwelling elderly adults. J Am Geriatr Soc. 2017;65(1):107–13. doi: 10.1111/jgs.14447. [DOI] [PubMed] [Google Scholar]
- 49.Rizzuto D, Melis RJF, Angleman S, et al. Effect of chronic diseases and multimorbidity on survival and functioning in elderly adults. J Am Geriatr Soc. 2017;65(5):1056–60. doi: 10.1111/jgs.14868. [DOI] [PubMed] [Google Scholar]