

Abstract
Objectives
To investigate the long-term efficacy and results of surgical management of conjunctival melanoma reconstructed with amniotic membrane transplantation.
Materials and Methods
Conjunctival melanoma in 10 patients (5 female, 5 male) was totally excised with adjunctive cryotherapy to the surgical margins, corneal epitheliectomy with absolute alcohol in cases of corneal involvement, lamellar sclerectomy in cases with episcleral involvement, and ocular surface grafting with cryopreserved amniotic membrane. Complications and tumor control rates were evaluated.
Results
The mean age of the patients was 57.4±15.2 (range, 37-84) years. The mean diameter of the tumors was 15.5±4.9 (range, 10-25) mm and histopathologically confirmed complete excision was performed in all cases. Mild limbal stem cell deficiency (2 eyes) and subclinical symblepharon (3 eyes) were observed as long-term complications. In a mean follow-up of 56.7±40.4 (range, 30-132) months, only one local tumor recurrence was detected. Despite retreatment, exenteration was performed in this patient due to re-recurrence. One patient died due to disseminated metastasis despite the absence of local recurrence.
Conclusion
In large conjunctival melanomas, reconstruction of the ocular surface is usually very challenging. The use of cryopreserved amniotic membrane for conjunctival defect repair is safe and effective with mild complications, and allows the excision of wider margins around the tumor.
Keywords: Amniotic membrane, conjunctiva, cryotherapy, melanoma, tumor
Introduction
Although conjunctival melanoma is rare, it is the most malignant tumor of the ocular surface. It can arise from primary acquired melanosis (PAM), preexisting conjunctival nevus, or de novo.1,2,3 It manifests with a painless melanotic or amelanotic mass on the ocular surface and is usually accompanied by a persistent dilated feeder blood vessel.1,2,3 It can originate from all three parts of conjunctiva (bulbar, forniceal, tarsal), or from the caruncle.1
In the treatment of conjunctival melanoma, total tumor resection is essential for avoiding local invasion, recurrence, and metastasis. Surgical management of conjunctival melanoma includes tumor resection using no-touch technique and achieving tumor free margins, partial lamellar sclerectomy, double freeze thaw cryotherapy, and corneal epitheliectomy with alcohol for tumors located at the limbal region. Conjunctival defect might be closed either primarily or with conjunctival flap, a graft from the opposite conjunctiva, oral mucosa, or amniotic membrane (AM), depending on the defect size.1,2,3 All these methods have both advantages and disadvantages.4
De Rotth5 described the use of fetal membrane allografts for ophthalmic purposes. Tseng et al.6,7 later reported using AM transplantation (AMT) for the surgical treatment of pterygia, corneal defects, symblepharon, and neoplasia. The structural and biochemical composition of AM induces epithelisation by acting as a substrate for epithelial cell growth and also works as an antiangiogenic, antiinflammatory, and antifibrotic agent.7,8 The use of AM is safe if the preparation is done according to the standard protocol.6,7,8
There are various reports on the use of AMT for ocular surface reconstruction in conjunctival melanoma. However, the long-term results of this method (in four patients) are reported in only one article.9 Herein, we report the long-term success (over 30 months, up to 132 months) and outcomes of conjunctival melanoma surgical management, reconstructed with cryopreserved AM.
Materials and Methods
Ten patients (10 eyes) who underwent resection of conjunctival melanoma and reconstruction with AMT between January 2005 and September 2013 were included in the study. All operations were performed by the same surgeons. Anterior segment slit-lamp examination and ocular surface staining with fluorescein were performed at every follow-up visit. Any problems regarding ocular surface homeostasis and any signs of complications or recurrences were noted. The patients’ findings, ocular surface photographs, histopathologic slides, and any possible extension of melanoma into surrounding tissues such as the eyelid, lacrimal sac, or orbit were retrospectively analysed. Every tumor was staged using American Joint Committee on Cancer (AJCC) classification.10 Success was defined as complete epithelisation of the wound with no significant accompanying complications or recurrence of the tumor. All patients underwent head-neck examination and soft tissue ultrasonography in order to detect any regional or lymphatic involvement, and systemic evaluation was performed in order to detect any metastasis. None of the patients had any detectable metastatic disease prior to excision.
All surgeries were performed under local anesthesia. All melanomas were excised using “no touch” technique with at least 2 mm safe margins (clinically normal conjunctiva).11,12 All resected specimens were sent for histopathological evaluation. In order to destroy any residual tumor cells, double freeze-thaw cryotherapy was applied to the conjunctival margins. In cases with corneal involvement, absolute alcohol corneal epitheliectomy was performed prior to tumor excision. In cases with scleral involvement, lamellar sclerectomy was performed and absolute alcohol was applied for 30 seconds to the excised tumor area. The conjunctival defects were repaired with cryopreserved single-layer AM placed stromal side down and fixed with 8/0 vicryl sutures. Largest AM diameter varied between 14 and 28 mm according to defect size. A pressure bandage was applied for 3 days. Topical antibiotic and corticosteroid eye drops were used 4 times a day for 1 month. No additional topical treatment, including interferon alpha-2b or mitomycin C, was used. Postoperative examinations were performed at 2 weeks, 4 weeks, 3 months, and every 6 months thereafter in order to detect any complications or local recurrences. Limbal stem cell deficiency was diagnosed in the presence of findings of superficial corneal vascularisation with whorled epithelium at the excision area.
Informed consent was obtained from all subjects participating in the study. This retrospective study was conducted in accordance with the Declaration of Helsinki of 1975 (as revised in Tokyo in 2004). Ege University Ethics Committee.
Results
The mean age of the 10 patients (5 female, 5 male) was 57.4±15.2 (range, 37-84) years. The right eye was affected in 4 patients and the left in 6 patients. According to the AJCC 8th edition classification for conjunctival melanoma, 3 of the tumors were T1c (>2 but <3 quadrants), 4 were T1d (>3 quadrants), and 3 were T2b (noncaruncular and ≥1 quadrant nonbulbar conjunctiva).10 No local invasions to the surrounding tissues or orbit, or lymph node metastases were present prior to surgery. However, 2 patients had history of incomplete excision elsewhere.
Histopathologically confirmed complete tumor excision was achieved in all eyes (100%). The mean diameter of the tumors was 15.5±4.9 (range, 10-25) mm. In 3 cases, the forniceal conjunctiva was involved. The limbal area was invaded in 8 cases (80%). The mean limbal involvement was 4±2.5 (range, 2-8) clock hours. The tumor invaded the cornea in 6 cases (60%) and corneal epitheliectomy was required. In 5 cases (50%), lamellar sclerectomy and absolute alcohol to the tumor base were also performed due to scleral involvement. Histopathologic types of the tumors were epitheloid in 1 eye and mixed in 9 eyes. Primary pathological tumor diagnosis according to AJCC 8th edition was T1a for 5 tumors (50%), T1b for 2 (20%), T2a for 2 (20%), T2b for 1 (10%) tumor. Mean tumor thickness was 1.82±0.70 (range, 1.13-3.00) mm.
No intraoperative complications were observed. The AM covered the surgical defect in all cases. Ocular surface irritation and mild lacrimation resolved in 2-3 weeks. In a mean follow-up of 56.7±40.4 (range, 30-132) months, one local recurrence was detected. Exenteration was performed in this patient, who had undergone two surgeries elsewhere prior to our surgical treatment. She is still alive after 20 months with no metastasis. One patient died due to disseminated metastasis although no recurrence was evident in the eye.
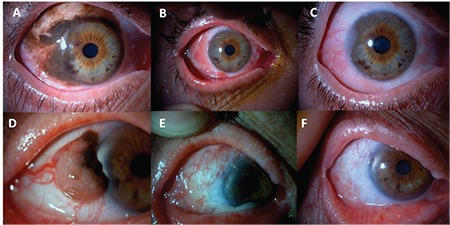
No recurrence was observed in the remaing 8 patients in a follow-up time of 58.78±44.4 (range, 30-132) months. The patients reported no signs or symptoms related to the ocular surface and all were satisfied with their cosmetic appearance. All exhibited a healthy ocular surface with no inflammation or dry eye symptoms (Figure 1A-F). Mild limbal stem cell deficiency with no ocular vision disturbance was detected in 3 eyes with tumors invading more than 180 degrees of the limbus (Figure 2A-C). Symblepharon which did not interfere with eye movements was diagnosed in 2 eyes. All ocular surfaces except the two with symblepharon were smooth (Figure 2D-F).
Figure 1. A) Preoperative picture of a 58-year-old male with conjunctival melanoma involving the temporal conjunctiva arising from primary acquired melanosis. B) Early postoperative picture showing the amniotic membrane. C) Late postoperative (22 months) appearance of the eye. D) Preoperative picture of a 55-year-old male with conjunctival melanoma involving the temporal conjunctiva arising from a nevus. E) Early postoperative picture showing the ocular surface and amniotic membrane. F) Late postoperative (32 months) appearance of the eye.
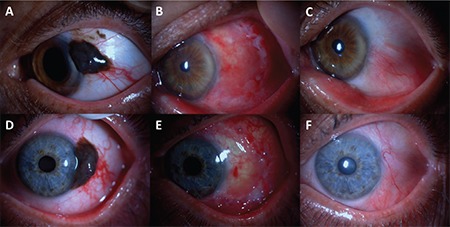
Figure 2. A) Preoperative picture of a 50-year-old male with extensive conjunctival melanoma arising from primary acquired melanosis. B) Early postoperative picture showing the ocular surface. C) Late postoperative (20 months) appearance of the eye with evident superotemporal limbal stem cell deficiency; D) Preoperative picture of a 84-year-old female with conjunctival melanoma. E) Early postoperative picture showing the amniotic membrane. F) Late postoperative (30 months) appearance of the eye.
Discussion
Conjunctival melanoma demonstrates many clinical variabilities. Shields et al.2, reported the mean age at presentation to be 61 years in 382 conjunctival melanoma patients (48% male, 52% female). Most of the melanomas had originated from PAM (76%), followed by nevus (6%) and de novo (17%).2 In the present study, the male-female ratio was 1:1, and 70% of the tumors arose from PAM, 20% were de novo, and 10% originated from nevus.
Conjunctival melanoma can develop on any part of the conjunctiva (bulbar, forniceal or tarsal) or in the caruncle. In an analysis of 382 conjunctival melanomas, the AJCC classification distribution was T1: 57%, T2: 32%, and T3: 11%.13 Invasion of the melanoma was observed in the corneal epithelium (40%), corneal stroma (3%), sclera (3%), eyelid (1%), orbit (2%), and canaliculus/lacrimal sac (1%).13 Twenty percent of the tumors were nonpigmented, 59% were pigmented, and 21% were mixed.13 In the present study, the mean diameter of the tumors was 15.5±4.9 (range, 10-25) mm. The corneal stroma was invaded in 6 eyes (60%) and the sclera in 5 eyes (50%). Forniceal conjunctiva was involved in 3 cases (30%). No eyelid, orbit, canaliculus or lacrimal sac involvement was observed. The tumor was pigmented in 8 (80%) and mixed in 2 (20%) cases.
The successful treatment of conjunctival melanoma depends on the extension of the tumor. Important rules of conjunctival melanoma surgery are to use the no-touch technique and to let the ocular surface dry until the tumor is completely removed so as to not seed the malignancy.1,2 For larger tumors involving the forniceal area, excision should be more generous and tumor-free margins should be ascertained. Conjunctival flaps, contralateral eye conjunctival grafts, buccal mucosa, or AMT might be used for reconstruction of these defects.1,2 However, the main disadvantage of autologous grafts and flaps is the insufficiancy of the utilisable tissue.14 Furthermore, excising large enough conjunctival autografts might cause donor site morbidity.15 Besides, many patients are not eager to have their healthy eye manipulated. Moreover, thick mucosal grafts usually cause unsatisfactory cosmetic results and also inhibit visualisation of the underlying structures for early recurrence detection.15 Thus, AM is a nearly perfect reconstruction material for large conjunctival tumors.
The good success and efficacy of AM for ocular surface reconstruction are due to enhanced epithelisation, antiinflammatory, antifibrotic, and antiangiogenic effects.16 Epithelisation is promoted by the basement membrane of the AM, which inhibits epithelial apoptosis and serves as a substrate for normal migration, differentiation, and adhesion of epithelial cells.17 On the other hand, the stromal portion promotes ocular surface healing by producing various growth factors such as epidermal growth factor, hepatocyte growth factor, basic fibroblast growth factor, and keratinocyte growth factor.18 The antiinflammatory activity of AM may be attributed to the presence of receptor antagonists of inflammatory mediators.19 The downregulation of transforming growth factor b signaling and the suppression of fibroblast differentiation to myofibroblasts are responsible for the anti-scarring effect.20
The antiangiogenic effects of AM are a result of the expression of tissue metalloproteinase and endostatin inhibitors, as well as proteins which stimulate corneal epithelial proliferation and suppress vascular endothelial cell growth.21 Moreover, AM has been proven to not only reduce inflammation but also enable goblet and non-goblet cell repopulation.22,23
Metastatic disease and local recurrence of conjunctival melanoma are usually detected in eyes with tumors located in the forniceal, carunclar, or tarsal regions and those with histopathologically tumor-positive margins.2 Even with total microscopic excision of the lesion, further disease is reported to develop from associated PAM in 26% of patients in 5 years and 65% of patients in 15-year follow-up.2 Numerous recurrences require orbital exenteration. Neighbouring (preauricular or submandibular) lymph nodes, lung, brain, and liver are the most common sites of metastasis. In our series, a patient who underwent two inadequate operations elsewhere (T1d AJCC stage) developed recurrence at 20 months and exenteration was performed. One patient (T1c AJCC stage) died due to disseminated metastasis (preauriculer lymph node, lung, brain) although the eye was apparently normal for 37 months. No recurrence or metastasis were observed in the remaing 8 patients in a follow-up time of 58.78±44.4 months. At the last follow-up, no surgery-related problems were reported and all patients were happy with the cosmetic appearance, similar to the results of Dalla Pozza et al.9
Conclusion
In conclusion, although AMT itself is not directly related to outcome in terms of local tumor control, it provides a more generous amount of tissue for conjunctival reconstruction in especially extensive conjunctival melanoma and promises a healthy ocular surface. In most cases, complete homeostasis of the ocular surface with no complications can be achieved.
Footnotes
Ethics
Ethics Committee Approval: Ege University Ethics Committee (13 March 2017 17-2/16).
Informed Consent: It vas taken.
Peer-review: Externally and internally peer-reviewed.
Authorship Contributions
Concept: Melis Palamar, Ayşe Yağcı, Design: Melis Palamar, Ayşe Yağcı, Data Collection or Processing: Melis Palamar, Banu Yaman, Analysis or Interpretation: Melis Palamar, Banu Yaman, Taner Akalın, Ayşe Yağcı, Literature Search: Melis Palamar, Writing: Melis Palamar, Banu Yaman.
Conflict of Interest: No conflict of interest was declared by the authors.
Financial Disclosure: The authors declared that this study received no financial support.
References
- 1.Shields JA, Shields CL. Eyelid, Conjunctival, and Orbital Tumors. An Atlas and Textbook. 2nd ed. Philadelphia: Lippincott Williams and Wilkins; 2008. [Google Scholar]
- 2.Shields CL, Markowitz JS, Belinsky I, Schwartzstein H, George NS, Lally SE, Mashayehi A, Shields JA. Conjunctival melanoma. Outcomes based on tumor origin in 382 consecutive cases. Ophthalmology. 2011;118:389–395. doi: 10.1016/j.ophtha.2010.06.021. [DOI] [PubMed] [Google Scholar]
- 3.Shields CL, Kels JG, Shields JA. Melanoma of the eye: Revealing hidden secrets, one at a time. Clin Dermatol. 2015;33:183–196. doi: 10.1016/j.clindermatol.2014.10.010. [DOI] [PubMed] [Google Scholar]
- 4.Asoklis RS, Damijonaityte A, Butkiene L, Makselis A, Petroska D, Pajaujis M, Juodkaite G. Ocular surface reconstruction using amniotic membrane following excision of conjunctival and limbal tumors. Eur J Ophthalmol. 2011;21:552–558. doi: 10.5301/EJO.2010.6192. [DOI] [PubMed] [Google Scholar]
- 5.De Rotth A. Plastic repair of conjunctival defects with fetal membrane. Arch Ophthalmol. 1940;23:522–525. [Google Scholar]
- 6.Prabhasawat P, Barton K, Burkett G, Tseng SC. Comparison of conjunctival autografts, amniotic membrane grafts, and primary closure for pterygium excision. Ophthalmology. 1997;104:974–985. doi: 10.1016/s0161-6420(97)30197-3. [DOI] [PubMed] [Google Scholar]
- 7.Tseng SC, rabhasawat P, Lee SH. Amniotic membrane transplantation for conjunctival surface reconstruction. Am J Ophthalmol. 1997;124:765–774. doi: 10.1016/s0002-9394(14)71693-9. [DOI] [PubMed] [Google Scholar]
- 8.Dua HS, zuara-Blanco A. Amniotic membrane transplantation. Br J Ophthalmol. 1999;83:748–752. doi: 10.1136/bjo.83.6.748. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Dalla Pozza G, Ghirlando A, Busato F, Midena E. Reconstruction of conjunctiva with amniotic membrane after excision of large conjunctival melanoma: a long-term study. Eur J Ophthalmol. 2005;15:446–450. doi: 10.1177/112067210501500404. [DOI] [PubMed] [Google Scholar]
- 10.AJCC Cancer Staging Manual (8th ed). Switzerland: Springer; 2017. pp. 795–803. [Google Scholar]
- 11.Azuaro-Blanco A, Pillai CT, Dua HS. Amniotic membrane transplantation for ocular surface reconstruction. Br J Ophthalmol. 1999;83:399–402. doi: 10.1136/bjo.83.4.399. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Shields JA, Shields CL, De otter P. Surgical management of conjunctival tumors. The 1994 Lynn B. McMahan Lecture. Arch Ophthalmol. 1997;115:808–815. doi: 10.1001/archopht.1997.01100150810025. [DOI] [PubMed] [Google Scholar]
- 13.Shields CL, Kaliki S, Al-Daamash SA, Lally SE, Shields JA. American Joint Committee on Cancer (AJCC) Clinical Classification Predicts Conjunctival Melanoma Outcomes. Ophthal Plast Reconstr Surg. 2012;5:313–323. doi: 10.1097/IOP.0b013e3182611670. [DOI] [PubMed] [Google Scholar]
- 14.Palamar M, Kaya E, Egrilmez S, Akalin T, Yagci A. Amniotic membrane transplantation in surgical management of ocular surface squamous neoplasias: long-term results. Eye (Lond). 2014;28:1131–1135. doi: 10.1038/eye.2014.148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Gündüz K, Ucakhan OO, Kanpolat A, Gunalp I. Nonpreserved human amniotic membrane transplantation for conjunctival reconstruction of extensive ocular surface neoplasias. Eye (Lond). 2006;20:351–357. doi: 10.1038/sj.eye.6701890. [DOI] [PubMed] [Google Scholar]
- 16.Dua HS, Gomes JA, Kinng AJ, Maharajan VS. The amniotic membrane in ophthalmology. Surv Ophthalmol. 2004;49:51–77. doi: 10.1016/j.survophthal.2003.10.004. [DOI] [PubMed] [Google Scholar]
- 17.Grueterich M, Tseng SCG. Human limbal progenitor cells expanded on intact amniotic membrane ex-vivo. Arch Ophthalmol. 2002;120:783–790. doi: 10.1001/archopht.120.6.783. [DOI] [PubMed] [Google Scholar]
- 18.Koizumi NJ, Inatomi TJ, Sotozono CJ, Fullwood NJ, Quantock AJ, Kinoshita S. Growth factor mRNA and protein in preserved human amniotic membrane. Curr Eye Res. 2000;20:173–177. [PubMed] [Google Scholar]
- 19.Lee SB, Li DQ, Tan DT, Meller DC, Tseng SC. Suppression of TGF β signalling in both normal conjunctival fibroblasts and pterygial body fibroblasts by amniotic membrane. Curr Eye Res. 2000;20:325–334. [PubMed] [Google Scholar]
- 20.Tseng SC, Li DQ, Max X. Suppression of transforming growth factor-beta isoforms, TGF-β receptor II, and myofibroblast differentiation in cultured human corneal and limbal fibroblasts by amniotic membrane matrix. J Cell Physiol. 1999;179:325–335. doi: 10.1002/(SICI)1097-4652(199906)179:3<325::AID-JCP10>3.0.CO;2-X. [DOI] [PubMed] [Google Scholar]
- 21.Hao Y, Ma DH, Hwang DG, Kim WS, Zhang F. Identification of antiangiogenic and antiinflammatory proteins in human amniotic membrane. Cornea. 2000;19:348–352. doi: 10.1097/00003226-200005000-00018. [DOI] [PubMed] [Google Scholar]
- 22.Barabino S, Rolando M. Amniotic membrane transplantation elicits goblet cell repopulation after conjunctival reconstruction in a case of severe ocular cicatricial pemphigoid. Acta Ophthalmol Scand. 2003;81:68–71. doi: 10.1034/j.1600-0420.2003.00019.x. [DOI] [PubMed] [Google Scholar]
- 23.Meller D, Dabul V, Tseng SC. Expansion of conjunctival epithelial progenitor cells on amniotic membrane. Exp Eye Res. 2002;74:537–545. doi: 10.1006/exer.2001.1163. [DOI] [PubMed] [Google Scholar]