

Abstract
Introduction:
Very little is known about the hard to reach tribal communities in India and one such community is a primitive hidden and isolated tribe group of Bharia people in Patalkot. Their health problems need special attention as they have very limited access to health care. The aim of this study is to assess the oral hygiene and periodontal status in the primitive tribe group of Bharias in Patalkot, Madhya Pradesh, India.
Materials and Methods:
A descriptive cross-sectional study was undertaken with sample size of 462 patients. The sample was selected using simple random technique. A predefined pro forma was used to record information about oral hygiene practices and tobacco-related habits. Oral Hygiene Index-simplified (OHI-S), Community Periodontal Index (CPI), and loss of attachment (LOA) were used to assess oral hygiene and periodontal status, respectively.
Results:
The prevalence of periodontal disease based on CPI scores showed that 35.4 % had periodontal pocket > 6mm. It was also found that 27.9% people had attachment loss of 6-8mm. Mean Debris Index-simplified, Calculus Index-simplified, and OHI-S for the participants were 1.59 ± 0.73, 0.99 ± 0.70, and 2.56 ± 1.36, respectively. Poor oral hygiene status was found in 36.3% of Bharias.
Conclusion:
Higher prevalence of periodontal diseases and poor oral hygiene status in Bharia people can be attributed mainly to their difficult terrain, isolation, very low literacy level, socioeconomic status, and cultural practices.
Key words: Community Periodontal Index, loss of attachment, Oral Hygiene Index-simplified, periodontal status, tribals
INTRODUCTION
People living in isolation in natural and unpolluted surroundings maintaining their traditional values, customs, beliefs, and myths commonly known as tribes are considered to be the indigenous people of the land and are living far away from modern civilization.[1]
India has the second largest concentration of tribal population in the World, which constitutes around 8.2 percent of nation's total population, according to the census of India 2001.[2] There are 635 tribes in India located in 5 major tribal belts across the country, out of which there are only 75 primitive tribes.[3] The total population of Bharias in Patalkot was 2801, and the total number of households was 579 according to the census of India 2001.[2] These primitive tribal communities have been identified by the Government of India on the basis of their preagricultural level of technology, extremely low level of literacy, and small, stagnant, or diminishing population.[4]
The health problems need special attention in the context of tribal communities of India. Available research studies point out that the tribal population has distinctive health problems, which are mainly governed by their habitat, difficult terrains, and ecologically variable niches.[5]
The accessibility of these tribes to medical and dental care is minimal.[6] As periodontal disease is one of the primary causes of tooth loss and is also associated with health problems such as cardiovascular diseases, cerebrovascular accidents, diabetes mellitus, and pregnancy-associated complications, the estimation of its prevalence in the population and the identification of high-risk groups are of great importance.[7] Worldwide, studies have been reported on the oral health status and treatment needs of tribal population.[8] Very little is known about the hard to reach communities in India and one such community is a primitive tribe group of Bharia people in Patalkot. They live in isolation and are so well hidden that people on the outside world did not even know it ever existed; hence, the name came from Sanskrit word “Patal” that means very deep.[9]
Till date, there is no study available which describes the oral health-related behavior of the Bharia tribe of Madhya Pradesh. Hence, in the present study, an attempt has been made to assess the oral hygiene and periodontal status of the Bharia tribe, based on which their oral health needs can be assessed, and this information can serve as a baseline data for the future researches as well as for the policy-makers to implement appropriate measures for improving oral health-related behavior of Bharia people.
MATERIALS AND METHODS
A descriptive cross-sectional study was undertaken, and 462 participants from the age of 6–82 years were selected using simple random sampling technique. A predefined pro forma was used to record information about oral hygiene practices, tobacco-related habits, knowledge and experience of periodontal disease, and dental treatments. Oral Hygiene Index-simplified (OHI-S), Community Periodontal Index (CPI), and loss of attachment (LOA) were used to assess oral hygiene and periodontal status, respectively. Before starting the final study, a pilot study was conducted on 72 Bharia tribe people from Patalkot to know the prevalence of periodontal disease and to check the reliability of the examiner.
Exclusion criteria
Tribal people of Gond tribe, though few in number and living in Patalkot, were excluded from the study
Children under the age of 5 years were excluded from the study
Participants who were absent on the day of examination and those who did not cooperate and who were systemically ill were also excluded from the study.
Obtaining approval from the authorities: Before the start of the survey, permission to interview and examine the tribal people was obtained from Directorate of Primitive Tribe Group, Satpura Bhawan, Bhopal (Madhya Pradesh). Ethical clearance was obtained from the Regional Ethical Committee. A list of all 12 villages of Bharia tribe inhabiting Patalkot was prepared out of which 6 (50%) villages were randomly selected using lottery method. Then, the Head/Sarpanch/Pradhan of each of the selected villages was contacted, and with their help, a list of the head of the families for each selected villages were made. Among those names, 88 names were selected using simple random sampling method (lottery method). Households of the 88 selected names were visited, and each member of that household was included in the final sample of the present study.
The study showed the prevalence of periodontal disease to be 48%. The intraexaminer reliability was assessed using the weighted kappa statistics, which was 83% and 84%, respectively, for CPI and OHI-S. All the clinical examinations were carried out by single examiner using standardized equipment using in natural daylight.
Statistical analysis was done using the Statistical Package of the Social Sciences (SPSS Version 17.0; Chicago Inc., USA). Statistical tests employed for the obtained data comparison in the study are Chi-square test and analysis of variance. Significance level was fixed at P < 0.05.
RESULTS
A total of 462 tribals comprised the sample. Tribals were classified age wise in 8 groups ranging from 6 to 82 years. Majority of tribals, i.e., 110 (23.8%) were from the age group of 6–14 years. Gender-wise sample comprised of 242 (52.3%) males and 220 (47.6%) females [Table 1]. Majority, i.e., 380 (82.2%) of the participants were illiterate [Figure 1].
Table 1.
Age-wise and gender-wise distribution of study population
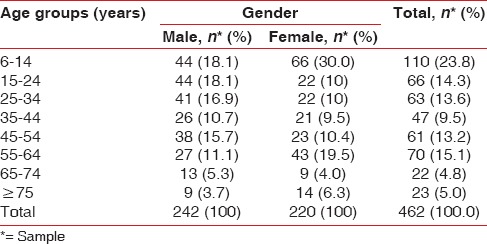
Figure 1.
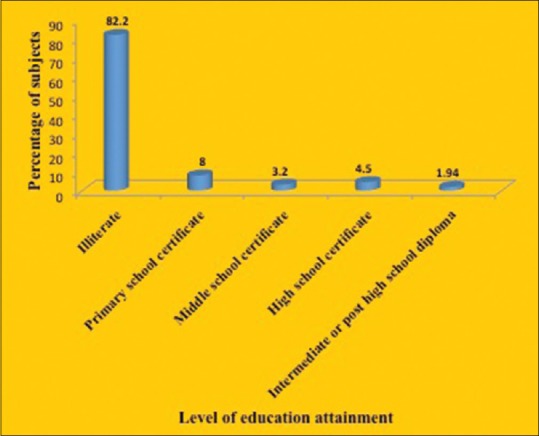
Distribution of study population according to education attained
Oral hygiene practices among tribal were found to be minimal and were not up to the mark. For cleaning teeth chewing, sticks were mainly used by majority (56.7%) of the participants. Furthermore, 7.7% of participants reported to use gudaku (a tobacco product) and 4.7% used salt for cleaning their teeth. There was no significant difference observed between males and females [Table 2]. Tobacco-related habits were prevalent among 30.9% males and 16.3% females. Difference found between was statistically significant (P > 0.05) [Table 3].
Table 2.
Gender-wise distribution of study population according to oral hygiene practices
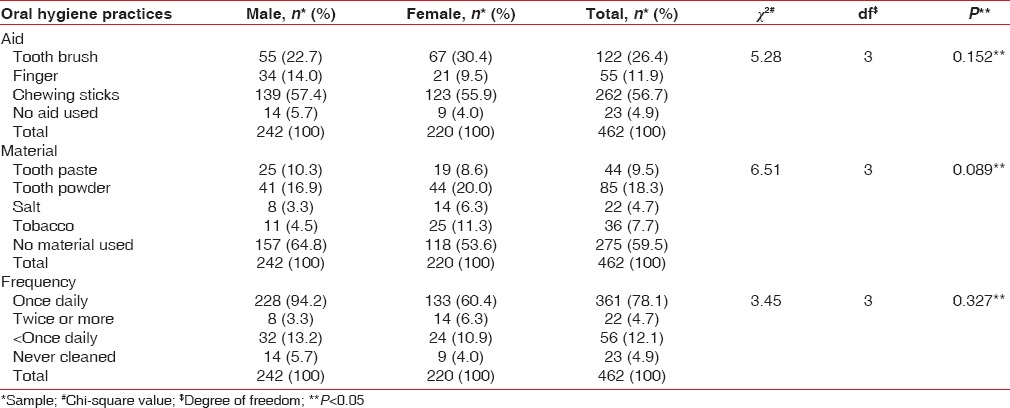
Table 3.
Gender-wise distribution of study participants according to the presence and absence of any tobacco-related habits

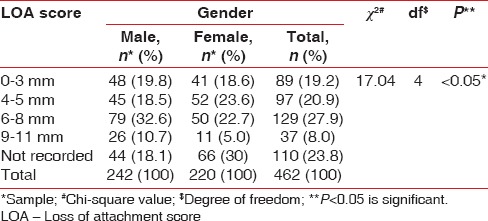
Based on CPI scores, 25.3% of the total population had healthy periodontium, 15.5% had bleeding on probing, the presence of calculus was seen in 2.1%, whereas 21.4% had periodontal pocket 4–5 mm and 35.4% had periodontal pocket ≥6 mm. In 6–14 years' age group, 82.7% of participants had healthy periodontium, and as the age increases, 82.6% of participants in the age group of 75 years or more had deep pockets. The differences for the CPI scores in various age groups were statistically significant (P < 0.05) [Table 4]. The prevalence of periodontal disease based on 'Loss of Attachment' found 19.2% population with no LOA (0-3mm). About 20.9% had LOA of 4–5 mm; 27.9% had LOA of 6–8 mm; 8.0% had LOA of 9–11 mm; 8.9% had LOA ≥12 mm; and 26.4% of the population had healthy periodontium. Gender-wise LOA was more in males, and the differences were statistically significant (P < 0.05) [Table 5].
Table 4.
Age-wise distribution of participants with healthy periodontal tissue, with bleeding on probing only, with calculus, with shallow pocket (4-5 mm), and with deep pocket (≥6 mm)
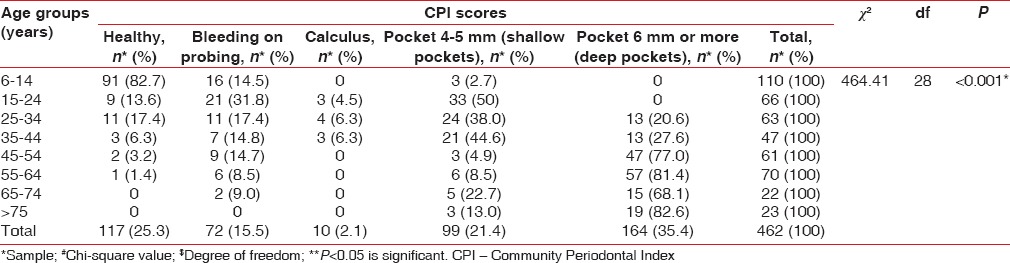
Table 5.
Gender-wise distribution of participants with respect to loss of attachment scores
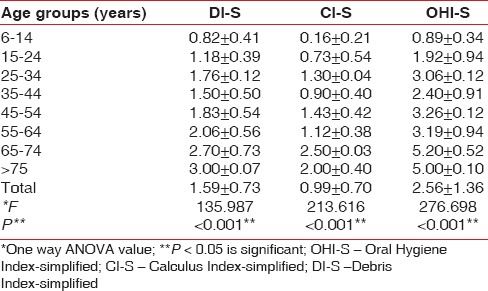
Oral hygiene status was recorded using OHI (S). Mean Debris Index-simplified (DI-S), Calculus Index-simplified (CI-S), and OHI-S for the participants were 1.59 ± 0.73, 0.99 ± 0.70, and 2.56 ± 1.36, respectively. The highest mean DI-S and OHI-S scores, i.e., 3.00 ± 0.07 and 5.00 ± 0.10, respectively, were in the participants of 75 years and above age group. Age-wise statistical difference was found significant [Table 6].
Table 6.
Mean Debris Index-simplified, Calculus Index-simplified, and Oral Hygiene Index-simplified score according to various age groups
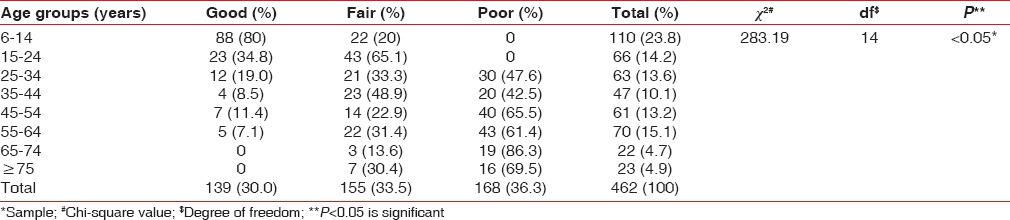
Poor oral hygiene status was found in 36.3% of Bharias. Majority (80%) of the participants in 6–14 years' age group had good oral hygiene whereas 86.3% of participants of 65–74 years' age group had poor oral hygiene. The results were found significant (P < 0.05) [Table 7].
Table 7.
Age-wise distribution of participants on the basis of good, fair, and poor oral hygiene
DISCUSSION
The present study was conducted to assess the oral hygiene and periodontal health status of people belonging to a primitive tribe group of Bharia residing in Patalkot, Madhya Pradesh [Figure 2]. These primitive tribal communities have been identified by the Government of India on the basis of their preagricultural level of technology, extremely low level of literacy, and small, stagnant, or diminishing population.[4] Their health problems need special attention.
Figure 2.
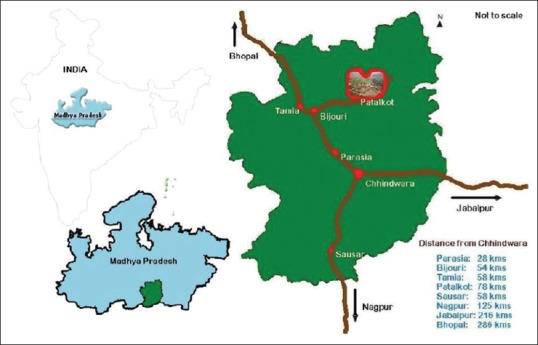
Geographic representation of population
The educational level definitely has an effect on behavioral pattern regarding dental care and its overall result on health. In the present study, 82.2% of the study participants were illiterate that this is similar to a study by Basu where a very low level (25.9%) of literacy was found among the tribal population in India.[10]
In the tribal population of Bharia, majority (56.7%) clean their teeth are usually by chewing sticks of beri, imli, and jamun and rinsing of mouth with plain water. The findings of the present study were in accordance with Bhasin where most of the Bhils in Rajasthan used twigs of Rattanjot and Jhatbor as toothbrush.[11] The finding also being similar to a study conducted by Bhowate et al. where the use of toothpaste and brush was found to be very low in tribal children of Sewagram, Maharashtra.[12]
Kumar et al. reported that 58% of the tribal population of Kundam block of Jabalpur district (Madhya Pradesh) used tobacco in one form or the other which was higher than the present study finding (24.0%).[13] Usually, the use of bidi, gutka, and nasmanjan was prevalent in the Bharia community which were available at nearest markets or haats. Most of them start smoking for pleasure, but at the same time, they also use tobacco to get relief from toothache (23.4%) and for cleaning teeth (19.8%). This could be due to lack of awareness (95.2%) about harmful effect of tobacco.
The present study shows that 74.7% of Bharia population suffers from one or the other form of periodontal disease as assessed by CPI. This was comparable to a study by Padma et al. on Iruliga tribal community, Karnataka, where 87.8% of population suffered periodontal problems.[14] Furthermore, the prevalence of periodontal disease increased with age was in accordance with National Oral Health Survey and Fluoride Mapping India (2002).[15] In the present study, none of the participants belonging to the age groups of 15–24 and 26–34 had periodontal pockets of more than 6 mm; the finding was consistent with Kumar et al.[16] Oral hygiene plays a key role to prevent dental problems. In the present study, mean DI-S, CI-S, and OHI-S were 1.59 ± 0.73, 0.99 ± 0.70, and 2.56 ± 1.36, respectively, which were comparable with study by Kumar et al. on Bhils of Southern Rajasthan, where mean DI-S, CI-S, and OHI-S scores were 1.84 ± 0.57, 1.61 ± 0.76, and 3.41 ± 1.22, respectively.[16] In the same study by Kumar et al., majority, i.e., 57.0% of participants reported to have poor oral hygiene, which was in accordance with the present study where majority (36.3%) had poor oral hygiene, and this can be attributed to their minimal oral hygiene practices, poor economic conditions, and low level of education.[16]
Maurya et al.[17] had conducted study on populations of Dogra community in Jammu region, India, and concluded that there was an increased prevalence of caries and periodontal problem personnel residing in Jammu. High need seemed to be due to lack of time and awareness about dental health, unfavorable environmental, and difficult terrain. The present study also strengthens the role of environment and difficult terrain in such population in oral hygiene and periodontal status.
CONCLUSION
Higher prevalence of periodontal diseases and poor oral hygiene status in Bharia people can be attributed to their difficult terrain, very low literacy level, socioeconomic status, isolation, superstition, cultural practices, underutilization of basic health-care facilities, and above all lack of oral health-care facilities. Thus, Bharias in Patalkot comprise a particularly vulnerable group with low rates of access to care and high rates of unmet dental needs. In spite of the tremendous advancement in the field of dental science, the oral health-care delivery services in these primitive tribal people are still poor and need to be strengthened in order to achieve the goal of oral health for all in the country.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Scheduled Tribes, Scheduled Areas and Tribal Areas in India. Ministry of Social Justice and Empowerment (Tribal Division) [Last accessed on 2010 Apr 09]. Available from: http://www.tribal.nic.in/
- 2.Registrar General of India. Census of India. 2001. [Last accessed on 2010 Apr 10]. Available from: http://www.censusindia.net/
- 3.Sharma AN. Adak (ed) Demography and Health Profile of the Tribal: A study of M.P. New Delhi: Anmol; 2003. Trends of morbidity among Bharias of Patalkot, Madhya Pradesh; pp. 202–10. [Google Scholar]
- 4.Pandey GD. Some aspects of population growth of the primitive tribes of M.P. J Fam Welfare. 2000;46:66–72. [Google Scholar]
- 5.Verma IC, Puri RK, Auroma RK. Medical Genetics in India. 2nd ed. Ponducherry: Auro Enterprises Publications; 1978. Medico-genetic problems of primitive tribal communities; pp. 149–70. [Google Scholar]
- 6.Biju P, Koshy C, Subramanian V, Arun M. Prevalence of periodontal diseases among the adult tribal population in Nilgiris – An epidemiological study. Int J Public Health Dent. 2013;4:8–12. [Google Scholar]
- 7.Lai H, Lo MT, Wang PE, Wang TT, Chen TH, Wu GH, et al. Acommunity-based epidemiological study of periodontal disease in Keelung, Taiwan: A model from Keelung community-based integrated screening programme (KCIS no 18) J Clin Periodontol. 2007;34:851–9. doi: 10.1111/j.1600-051X.2007.01121.x. [DOI] [PubMed] [Google Scholar]
- 8.African Tribes and Nutritional diseases. [Last accessed on 2010 Apr 12]. Available from: http://www.modern-diets-and-nutritional-diseases.com/african-tribes.html .
- 9.Dolla CK, Meshram P, Verma A, Shrivastav P, Karforma C, Patel ML. Health and morbidity profile of Bharias – A primitive tribe of Madhya Pradesh. J Hum Ecol. 2006;19:139–41. [Google Scholar]
- 10.Basu S. Dimensions of tribal health in India. Health and Population. Perspectives and Issues. 2000;23:61–70. [Google Scholar]
- 11.Bhasin V. Oral health behavior among Bhils of Rajasthan. J Soc Sci. 2004;8:1–5. [Google Scholar]
- 12.Bhowate RR, Borle SR, Chinchkhede DH, Gondhalekar RV. Dental health amongst 11-15-year-old children in Sevagram, Maharashtra. Indian J Dent Res. 1994;5:65–8. [PubMed] [Google Scholar]
- 13.Kumar S, Das D, Kumar D. Tobacco use among gonds of Kundam, Jabalpur: Some preliminary findings update. Biannual Newsl Reg Med Res Cent Tribals Jabalpur. 2008;5:1–3. [Google Scholar]
- 14.Padma B, Sushi K. Periodontal health status and oral hygiene practices of Iruliga tribal community residing at Ramanagar district, Karnataka, India. J Int Oral Health. 2010;2:17–26. [Google Scholar]
- 15.National Oral Health Survey and Fluoride Mapping 2002-2003 Madhya Pradesh. [Last accessed on 2010 Mar 20]. Available from: http://www.at.iaphd.org/statesurvey/MadhyaPradesh.pdf .
- 16.Kumar TS, Dagli RJ, Mathur A, Jain M, Balasubramanyam G, Prabu D, et al. Oral health status and practices of dentate Bhil adult tribes of Southern Rajasthan, India. Int Dent J. 2009;59:133–40. [PubMed] [Google Scholar]
- 17.Maurya R, Kundu D, Singh H, Mishra H. Oral health status, dental caries experience and treatment needs of population of Jammu city. Int J Oral Health Dent. 2015;1:164–7. [Google Scholar]