

Abstract
Objectives
To quantify the risk of pneumococcal pneumonia (PP) and invasive pneumococcal disease (IPD) in adults aged ≥19 years with underlying medical conditions compared with healthy adults of the same age in Japan.
Design
An observational, retrospective, cohort study using two healthcare claims databases in Japan: Japan Medical Data Center (JMDC) and Medical Data Vision (MDV) databases.
Participants
A total of 10.4 million individuals, representing 9.3 million person-years of follow-up, were included in the analysis. Eleven medical conditions as well as PP and IPD were identified by the International Statistical Classification of Diseases and Related Health Problems version 10 diagnostic codes and/or local disease codes used in Japan.
Primary outcome measures
Adjusted rate ratios (RRs) for PP and IPD in adults with a medical condition versus adults without any medical condition were calculated using multivariate Poisson regression models with age and/or sex as covariates.
Results
In the JMDC and MDV databases, respectively, adults ≥19 years with a medical condition (RRs for PP: 3.3 to 13.4, 1.7 to 5.2; RRs for IPD: 12.6 to 43.3, 4.4 to 7.1), adults with two or more medical conditions (PP: 11.6, 2.8; IPD: 18.7, 5.8) and high-risk adults (PP: 12.9, 1.8; IPD: 29.7, 4.0) were at greater risk of PP and IPD compared with their healthy counterparts. Adults aged 50–64 years with an underlying medical condition (PP rate: 38.6 to 212.1 per 100 000 person-years) had a higher rate of PP than those aged ≥65 years without any condition (PP rate: 13.2 to 93.0 per 100 000 person-years).
Conclusions
Adults of all ages with an underlying medical condition are at greater risk of PP and IPD compared with adults without any medical condition. This risk increases with the number of underlying medical conditions. Our results support extending pneumococcal vaccination to younger adults with an underlying medical condition, especially those aged 50–64 years.
Keywords: pneumococcal pneumonia, invasive, pneumococcal disease, chronic medical condition
Strengths and limitations of this study.
Given the well-known differences in the genetic makeup of the Japanese population, data specific to Japan are important to formulate a national immunisation strategy and to protect vulnerable populations.
Our study results may contribute to further knowledge on the risk of pneumococcal disease in Japanese individuals aged ≥19 years with an underlying medical condition.
As this study was a retrospective analysis based on insurance claims data, the coding of medical conditions and episodes of pneumococcal pneumonia and invasive pneumococcal disease by the International Statistical Classification of Diseases and Related Health Problems version 10 codes may lead to misclassification, and pneumococcal pneumonia may be undercoded.
These analyses did not consider potential confounders other than age and sex, such as pneumococcal vaccination history and residential environment, which might significantly influence the risk of pneumococcal pneumonia and invasive pneumococcal disease.
Results from only one database cannot be extrapolated to the general population of adults in Japan, and subjects in the two databases may be representative of different adult populations.
Introduction
Pneumococcal disease, caused by encapsulated Streptococcus pneumoniae, is a major cause of community-acquired pneumonia, meningitis, septicaemia, osteomyelitis, septic arthritis and bacteraemia worldwide. Older adults and children, as well as immunosuppressed individuals, such as those with HIV, are susceptible to pneumococcal disease.1 2 In addition, adults with certain chronic medical conditions, such as diabetes, chronic lung disease and chronic heart disease, are also at increased risk of pneumococcal disease.3 4 These high-risk groups have been targeted for pneumococcal vaccination to reduce the burden of pneumococcal disease in many countries, including the USA, Canada, the UK and Germany.5–8
The 23-valent pneumococcal polysaccharide vaccine (PPV23) was licensed in 1988 in Japan, and studies have revealed the protective effects of PPV23 against invasive pneumococcal disease (IPD) and pneumococcal pneumonia (PP).9–12 Since 2014,13 the National Immunisation Programme in Japan has implemented the use of PPV23 for adults aged 60–64 years with underlying medical conditions, in addition to adults aged ≥65 years. Since 2007,14 15 the Japanese Respiratory Society has advocated an expansion of the programme to individuals aged 2–64 years with chronic or immunosuppressive conditions.
Several studies have been conducted in the USA and Germany to examine the burden of pneumococcal disease in persons with underlying medical conditions.16 17 A retrospective analysis of three healthcare claims repositories in the USA showed that PP and IPD rates were approximately three times higher in immunocompetent adults with one or more chronic conditions (‘at-risk’ adults) compared with age-matched healthy adults. Additionally, these rates were approximately 4–7 times and 4–10 times higher in adults who were immunocompromised or receiving immunosuppressive therapy (‘high-risk’ adults), respectively, compared with age-matched healthy adults.4 A separate study using the same databases demonstrated that associated healthcare costs for IPD were approximately 3–4 times and 5–10 times higher in at-risk adults and high-risk adults, respectively, compared with age-matched healthy counterparts.18
The risk of pneumococcal disease in individuals with underlying medical conditions is not well characterised in Japan. As differences in the genetic makeup of the Japanese population may lead to different risk patterns of pneumococcal disease compared with other countries, information specific to Japan is important for healthcare professionals to identify patients at increased risk of pneumococcal disease, and for policy makers to formulate a national immunisation strategy to protect vulnerable populations. Therefore, the objective of this study was to quantify the burden of pneumococcal disease in adults aged ≥19 years with an underlying medical condition in Japan.
Methods
Data source
Two healthcare claims databases, the Japan Medical Data Center (JMDC) database and the Medical Data Vision Company (MDV) database, were used in our study. The JMDC database contains claims data from the Japanese union-managed health insurance system, comprising 10 insurance societies since 2005. The JMDC database includes workers (mostly aged <65 years) employed by mid-sized to large-sized companies and their dependents, and excludes individuals aged ≥75 years. It has records of >3 million individuals.19 The MDV database contains health insurance claims, administrative data, and laboratory values stored in the electronic records of 16 secondary hospitals with an average of 300 beds, which represented 9% of acute care hospitals in Japan. This database contains records for 7.4 million individuals who received healthcare services at these hospitals since 2003.20 21 Subjects in the MDV database can be lost to follow-up. Both databases have been used in multiple studies published in peer-reviewed journals.22–24
Study design and population
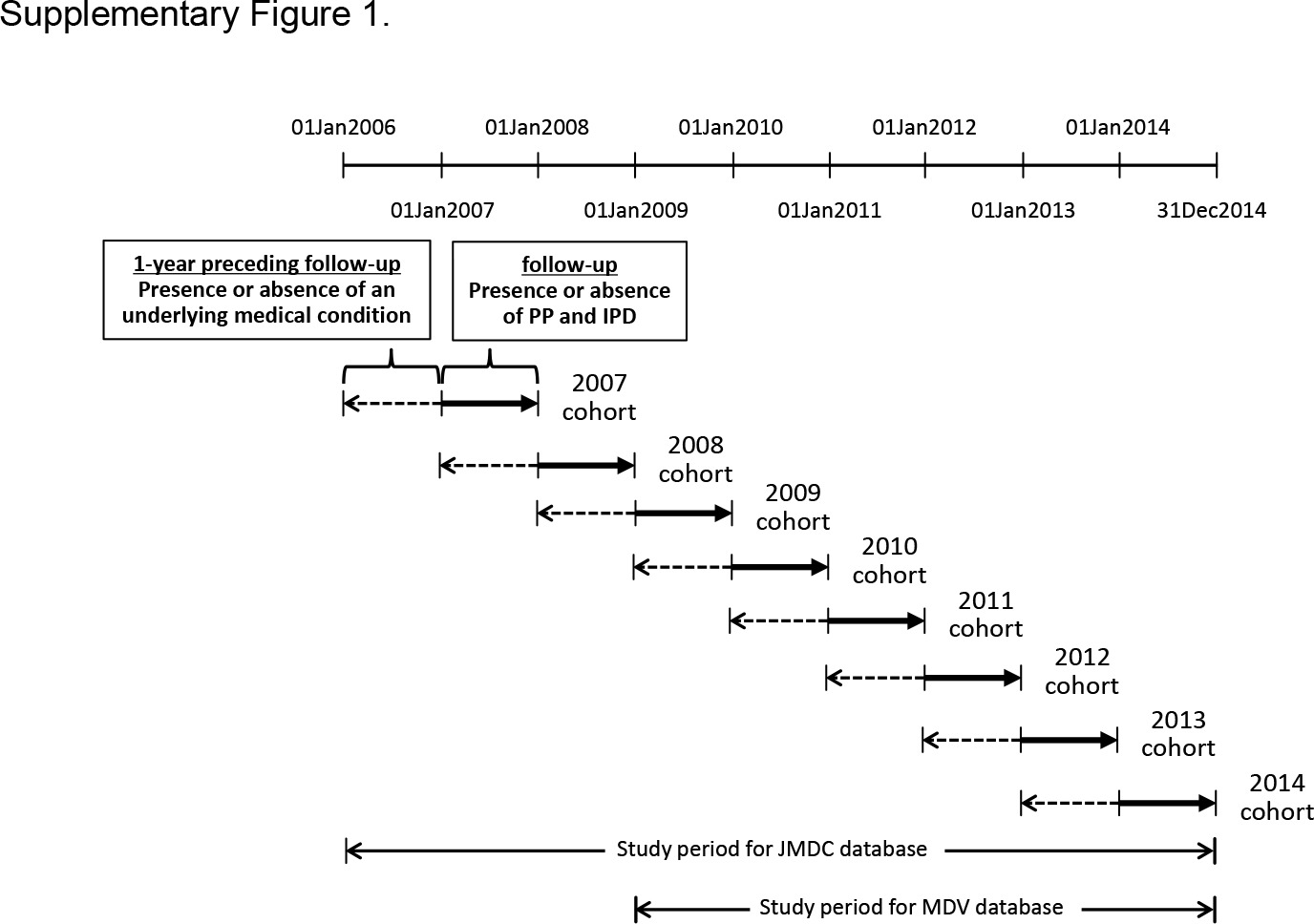
This was an observational, retrospective, cohort study. The study design was based on those of the studies by Shea et al4 and Weycker et al18 conducted in the USA, and that by Pelton et al conducted in Germany.25 The study period spanned from 1 January 2006 to 31 December 2014 for the JMDC database and from 1 January 2009 to 31 December 2014 for the MDV database. Adults were included in each yearly cohort if they were aged ≥19 years on the first day of the calendar year and were continuously enrolled over the period from 1 year before to 1 year after 1 January of the calendar years 2007 to 2014 for the JMDC database and 2009 to 2014 for the MDV database. There were no exclusion criteria in this study.
Adults were classified as healthy or having an underlying medical condition based on whether they had the medical conditions of interest during the year preceding 1 January of each calendar year included in the study. If a patient had multiple conditions of interest in the previous year, the patient was assigned to all diagnosed conditions. Subjects without evidence of these conditions were classified as healthy. For each yearly cohort, episodes of pneumococcal disease were identified during the 1-year period from 1 January to 31 December. Multiple yearly cohorts were identified at the beginning of each calendar year during the study period. Subjects who met the inclusion criteria in multiple calendar years were included in corresponding yearly cohorts. The study design is summarised in online supplementary figure 1.
bmjopen-2017-018553supp001.jpg (132.5KB, jpg)
{kind=link}
Study variables
According to guidelines and recommendations in the USA, England and Japan5 7 13 14 this study included 11 medical conditions of interest: chronic heart disease, chronic lung disease, diabetes mellitus, chronic liver disease, chronic renal disease, cancer, HIV/AIDS, functional or anatomic asplenia, organ transplantation, alcoholism and cerebrospinal fluid leakage. At-risk conditions included chronic heart disease, chronic lung disease, diabetes mellitus, chronic liver disease and alcoholism. High-risk conditions included chronic renal disease, cancer, HIV/AIDS, functional or anatomic asplenia, organ transplantation and cerebrospinal fluid leakage.26 Medical conditions were identified by the International Statistical Classification of Diseases and Related Health Problems version 10 (ICD-10) diagnostic codes and/or local disease codes defined by the Ministry of Health, Labour and Welfare (MHLW) in Japan.27 Detailed definitions of each medical condition are described in online supplementary table 1.
bmjopen-2017-018553supp002.pdf (129.9KB, pdf)
Adults were classified as healthy or having an underlying medical condition based on whether they had the medical conditions of interest during the 1-year period preceding follow-up. Adults were classified as having a confirmed medical condition if at least two ICD-10 codes for the condition were recorded in the preceding calendar year. If a patient had multiple conditions of interest in the 1-year period preceding follow-up, the patient was assigned to all diagnosed conditions. Adults without evidence of these conditions were classified as healthy. In addition, adults were classified by the number of medical conditions of interest (0, 1 and 2+ conditions), risk status (healthy, at-risk conditions and high-risk conditions), age (19–49, 50–64 and ≥65 years) and sex (male, female), based on the recommendations for pneumococcal vaccination by the MHLW in Japan,13 and the recommending bodies in other countries, including the USA,5 26 England7 and Germany.8 Patients with multiple chronic medical conditions were included in all applicable chronic medical condition cohorts. For example, a patient with diabetes mellitus and heart disease in 2007 was included in both the diabetes cohort and the heart disease cohort. This patient, if coded only for heart disease in 2008 (without being coded for diabetes mellitus), was not counted in the diabetes cohort, and thus was counted only in the heart disease cohort of 2008.
Episodes of PP and IPD were identified by the ICD-10 diagnostic codes and/or local disease codes defined by the MHLW in Japan27 in each calendar year. Episodes were considered distinct if they were separated by an interval of 90 days.4 PP was defined according to the code of PP alone, the code of pneumococcal bronchitis alone, combined codes of pneumonia and pneumococcal infection at the same day or other codes. IPD was defined according to the code of IPD, pneumococcal sepsis, pneumococcal meningitis or others. Detailed definitions of PP and IPD are described in online supplementary table 1.
Statistical analysis
PP and IPD rates per 100 000 person-years were calculated for the overall sample and by age, sex, medical condition, number of medical conditions and risk status. Unadjusted rate ratios (RRs) of PP and IPD in adults with and without a medical condition were calculated by comparing the rates of PP and IPD between adults with and those without a medical condition. Multivariate Poisson regression models, with age and/or sex as covariates, were used to determine age-adjusted and sex-adjusted or sex-adjusted RRs of PP and IPD. Analyses were conducted using SAS V.9.3 (SAS Institute, Cary, North Carolina, USA).
Results
Characteristics of the study population
A total of 10.4 million individuals, representing 9.3 million person-years of follow-up, were included in the analysis (comprising 6.7 million person-years from the JMDC databases and 2.6 million person-years from the MDV database). In the JMDC database, 78% of adults were aged19–49 years, 20% were aged 50–64 years, 2% were aged ≥65 years and the mean age was 39.6 years. Furthermore, 56% were men, 89% had no medical condition, 3% had two or more conditions, 10% had at-risk conditions and 3% had high-risk conditions. In the MDV database, 18% of adults were aged 19–49 years, 26% were aged 50–64 years, 55% were aged ≥65 years and the mean age was 62.0 years. Furthermore, 46% were men, and 48% had no medical condition, 23% had two or more conditions, 40% had at-risk conditions and 22% had high-risk conditions. Few study subjects with HIV/AIDS, alcoholism, asplenia, organ transplantation and cerebrospinal fluid leakage were identified in both databases. Characteristics of the study subjects from the JMDC and MDV databases are shown in table 1.
Table 1.
Characteristics of study subjects from the JMDC and MDV database
| JMDC | MDV | |||||||||
| Cumulative number of adults | Person-years* | PP | IPD | Cumulative number of adults | Person-years* | PP | IPD | |||
| % | Events | Events | % | Events | Events | |||||
| Overall | 7 433 221 | 6 721 329 | 100 | 840 | 80 | 2 967 475 | 2 565 033 | 100 | 2569 | 117 |
| Age (years) | ||||||||||
| 19–49 | 5 744 222 | 5 211 057 | 78 | 433 | 28 | 566 908 | 470 300 | 18 | 117 | 7 |
| 50–64 | 1 522 054 | 1 368 055 | 20 | 296 | 45 | 776 809 | 679 365 | 27 | 318 | 26 |
| ≥65† | 166 945 | 142 218 | 2 | 111 | 7 | 1 623 758 | 1 415 368 | 55 | 2134 | 84 |
| Sex | ||||||||||
| Female | 3 326 903 | 2 957 528 | 44 | 327 | 20 | 1 620 634 | 1 394 668 | 54 | 1109 | 61 |
| Male | 4 106 318 | 3 763,802 | 56 | 513 | 60 | 1 346 841 | 1 170 364 | 46 | 1460 | 56 |
| Risk status‡ | ||||||||||
| Healthy (no condition) | 6 603 349 | 5 975 767 | 89 | 436 | 33 | 1 494 204 | 1 242 491 | 48 | 691 | 23 |
| At-risk conditions | 758 769 | 681 915 | 10 | 380 | 37 | 1 151 533 | 1 038 332 | 40 | 1725 | 83 |
| High-risk conditions | 128 966 | 113 909 | 2 | 154 | 28 | 628 565 | 556 208 | 22 | 752 | 48 |
| Medical conditions§ | ||||||||||
| No condition | 6 603 349 | 5 975 767 | 89 | 436 | 33 | 1 494 204 | 1 242 491 | 48 | 691 | 23 |
| Chronic heart disease | 144 228 | 1 27 884 | 2 | 120 | 21 | 5 22 688 | 4 71 870 | 18 | 972 | 44 |
| Chronic lung disease | 313 269 | 2 81 336 | 4 | 261 | 19 | 299 695 | 2 68 656 | 10 | 1014 | 37 |
| Diabetes mellitus | 283 483 | 253 904 | 4 | 178 | 31 | 594 890 | 540 680 | 21 | 761 | 46 |
| Chronic liver disease | 232 397 | 208 938 | 3 | 75 | 23 | 334 107 | 302 832 | 12 | 443 | 27 |
| Chronic renal disease | 40 585 | 36 286 | 0.5 | 55 | 6 | 122 872 | 109 707 | 4 | 217 | 10 |
| Cancer | 91 004 | 79 882 | 1 | 103 | 23 | 529 116 | 466 966 | 18 | 589 | 40 |
| HIV/AIDS | NR | NR | NR | NR | NR | 521 | 480 | 0.02 | 1 | 0 |
| Alcoholism | 2366 | 2078 | 0.03 | 1 | 0 | 2744 | 2421 | 0.09 | 4 | 0 |
| Asplenia | 1732 | 1538 | 0.02 | 30 | 16 | 6799 | 6031 | 0.2 | 26 | 1 |
| Organ transplantation | 2525 | 2214 | 0.03 | 17 | 16 | 3895 | 3535 | 0.1 | 21 | 2 |
| Cerebrospinal fluid leakage | 298 | 264 | 0.004 | 0 | 0 | 355 | 318 | 0.01 | 0 | 0 |
| Number of conditions | ||||||||||
| 0 | 6 603 349 | 5 975 767 | 89 | 436 | 33 | 1 494 204 | 1,242 491 | 48 | 691 | 23 |
| 1 | 614 013 | 554 305 | 8 | 157 | 12 | 824 413 | 736 812 | 29 | 640 | 23 |
| ≥2 | 215 859 | 191 257 | 3 | 247 | 35 | 648 858 | 585 730 | 23 | 1238 | 71 |
*Per 100 000 person-years.
†Adults ≥75 years were not included in the JMDC database.
‡For risk status, some totals exceed 100% as some patients were included in more than one subcategory.
§For medical condition, some totals exceed 100% as some patients had more than one medical condition.
IPD, invasive pneumococcal disease; JMDC, Japan Medical Data Center; MDV, Medical Data Vision; NR, not recorded; PP, pneumococcal pneumonia.
The burden of PP and IPD
Rates and RRs for PP are shown in table 2 for the JMDC database and in table 3 for the MDV database. Rates and RRs for IPD are shown in table 4 for the JMDC database and in table 5 for the MDV database.
Table 2.
Rates and RRs of pneumococcal pneumonia in the JMDC database
| All ages (≥19 years*) |
Age subgroups | |||||||
| 19–49 years | 50–64 years | ≥65 years* | ||||||
| Rate† | RR‡ (95% CI) | Rate† | RR§ (95% CI) | Rate† | RR§ (95% CI) | Rate† | RR§ (95% CI) | |
| Overall | 12.5 | 8.3 | 21.6 | 78.0 | ||||
| Risk status | ||||||||
| Healthy (no condition) | 7.3 | 1.0 | 6.3 | 1.0 | 11.5 | 1.0 | 13.2 | 1.0 |
| At-risk conditions | 55.7 | 5.3 (4.5 to 6.2) | 33.6 | 5.4 (4.3 to 6.6) | 59.1 | 5.0 (4.0 to 6.4) | 180.8 | 8.2 (4.3 to 15.5) |
| High-risk conditions | 135.2 | 12.9 (10.4 to 16.0) | 104.4 | 17.2 (12.6 to 23.4) | 115.0 | 10.2 (7.5 to 13.8) | 325.2 | 16.3 (8.3 to 32.0) |
| Medical condition¶ | ||||||||
| No condition | 7.3 | 1.0 | 6.3 | 1.0 | 11.5 | 1.0 | 13.2 | 1.0 |
| Chronic heart disease | 93.8 | 7.1 (5.7 to 8.8) | 78.4 | 12.5 (8.5 to 18.3) | 68.5 | 5.6 (4.0 to 7.8) | 206.8 | 10.1 (5.2 to 19.7) |
| Chronic lung disease | 92.8 | 10.8 (9.2 to 12.6) | 51.6 | 8.2 (6.6 to 10.4) | 143.1 | 12.8 (9.9 to 16.6) | 356.4 | 18.8 (9.8 to 36.3) |
| Diabetes mellitus | 70.1 | 5.7 (4.8 to 6.9) | 35.9 | 5.7 (3.9 to 8.3) | 65.9 | 5.4 (4.1 to 7.0) | 187.9 | 9.0 (4.7 to 17.3) |
| Chronic liver disease | 35.9 | 3.3 (2.6 to 4.3) | 24.3 | 3.9 (2.6 to 5.9) | 38.6 | 3.2 (2.2 to 4.7) | 87.5 | 4.3 (2.0 to 9.4) |
| Chronic renal disease | 151.6 | 13.4 (10.1 to 17.9) | 148.2 | 23.6 (15.6 to 35.8) | 67.8 | 5.6 (3.0 to 10.5) | 517.2 | 23.7 (11.3 to 49.7) |
| Cancer | 128.9 | 11.2 (9.0 to 14.1) | 72.1 | 11.5 (7.4 to 18.0) | 137.2 | 12.5 (9.1 to 17.1) | 261.5 | 11.9 (5.8 to 24.1) |
| Number of conditions | ||||||||
| 0 | 7.3 | 1.0 | 6.3 | 1.0 | 11.5 | 1.0 | 13.2 | 1.0 |
| 1 | 28.3 | 3.2 (2.6 to 3.8) | 19.4 | 3.1 (2.3 to 4.1) | 32.9 | 2.8 (2.1 to 3.8) | 86.3 | 3.9 (1.9 to 8.0) |
| ≥2 | 129.1 | 11.6 (9.7 to 13.9) | 108.2 | 17.4 (13.4 to 22.6) | 104.9 | 8.9 (6.9 to 11.6) | 272.5 | 11.9 (6.2 to 22.8) |
*Adults ≥75 years were not included in the JMDC database.
†Per 100 000 person-years.
‡Age-adjusted and sex-adjusted RR.
§Sex-adjusted RR.
¶Results of subgroups with other medical conditions, including HIV/AIDS, alcoholism, asplenia, organ transplantation and cerebrospinal fluid leakage, are not shown.
JMDC, Japan Medical Data Center; RR, rate ratio.
Table 3.
Rates and RRs of pneumococcal pneumonia in the MDV database
| All ages (≥19 years) |
Age subgroups | |||||||
| 19–49 years | 50–64 years | ≥65 years | ||||||
| Rate* | RR† (95% CI) | Rate* | RR‡ (95% CI) | Rate* | RR‡ (95% CI) | Rate* | RR‡ (95% CI) | |
| Overall | 100.2 | 24.9 | 46.8 | 150.8 | ||||
| Risk status | ||||||||
| Healthy (no condition) | 55.6 | 1.0 | 17.8 | 1.0 | 30.2 | 1.0 | 93.0 | 1.0 |
| At-risk conditions | 166.1 | 2.3 (2.1 to 2.5) | 50.9 | 2.9 (1.9 to 4.2) | 78.4 | 2.5 (2.0 to 3.2) | 216.6 | 2.2 (2.0 to 2.5) |
| High-risk conditions | 135.2 | 1.8 (1.6 to 2.0) | 48.0 | 2.7 (1.7 to 4.4) | 54.0 | 1.7 (1.3 to 2.3) | 177.1 | 1.8 (1.6 to 2.0) |
| Medical condition§ | ||||||||
| No condition | 55.6 | 1.0 | 17.8 | 1.0 | 30.2 | 1.0 | 93.0 | 1.0 |
| Chronic heart disease | 206.0 | 2.6 (2.3 to 2.9) | 53.2 | 3.2 (1.7 to 6.0) | 79.2 | 2.4 (1.8 to 3.2) | 249.0 | 2.5 (2.3 to 2.8) |
| Chronic lung disease | 377.4 | 5.2 (4.7 to 5.7) | 97.8 | 5.6 (3.6 to 8.5) | 212.1 | 6.8 (5.2 to 8.9) | 479.2 | 4.9 (4.4 to 5.5) |
| Diabetes mellitus | 140.7 | 1.9 (1.7 to 2.1) | 42.7 | 2.6 (1.5 to 4.5) | 60.8 | 1.8 (1.4 to 2.5) | 182.1 | 1.8 (1.6 to 2.1) |
| Chronic liver disease | 146.3 | 2.1 (1.9 to 2.4) | 42.6 | 2.5 (1.4 to 4.5) | 80.7 | 2.5 (1.9 to 3.4) | 198.0 | 2.0 (1.8 to 2.3) |
| Chronic renal disease | 197.8 | 2.6 (2.2 to 3.0) | 85.5 | 5.0 (2.5 to 10.2) | 88.3 | 2.7 (1.7 to 4.3) | 248.0 | 2.5 (2.1 to 2.9) |
| Cancer | 126.1 | 1.7 (1.5 to 1.9) | 45.1 | 2.5 (1.5 to 4.3) | 48.3 | 1.6 (1.2 to 2.2) | 165.5 | 1.7 (1.5 to 1.9) |
| Number of conditions | ||||||||
| 0 | 55.6 | 1.0 | 17.8 | 1.0 | 30.2 | 1.0 | 93.0 | 1.0 |
| 1 | 86.9 | 1.3 (1.2 to 1.5) | 31.1 | 1.7 (1.1 to 2.7) | 41.3 | 1.3 (1.0 to 1.8) | 122.4 | 1.3 (1.1 to 1.4) |
| ≥2 | 211.4 | 2.8 (2.5 to 3.0) | 75.4 | 4.2 (2.6 to 6.7) | 98.2 | 3.1 (2.4 to 4.0) | 257.9 | 2.7 (2.4 to 3.0) |
*Per 100 000 person-years.
†Age-adjusted and sex-adjusted RR.
‡Sex-adjusted RR.
§Results of subgroups with other medical conditions, including HIV/AIDS, alcoholism, asplenia, organ transplantation and cerebrospinal fluid leakage, are not shown.
MDV, Medical Data Vision; RR, rate ratio.
Table 4.
Rates and RRs of invasive pneumococcal diseases in the JMDC database
| All ages (≥19 years*) |
Age subgroups | |||||||
| 19–49 years | 50–64 years | ≥65 years* | ||||||
| Rate† | RR‡ (95% CI) | Rate† | RR§ (95% CI) | Rate† | RR§ (95% CI) | Rate† | RR§ (95% CI) | |
| Overall | 1.2 | 0.5 | 3.3 | 4.9 | ||||
| Risk status | ||||||||
| Healthy (no condition) | 0.6 | 1.0 | 0.3 | 1.0 | 1.6 | 1.0 | 1.2 | 1.0 |
| At-risk conditions | 5.4 | 5.3 (3.2 to 8.8) | 1.4 | 4.6 (1.7 to 12.7) | 9.3 | 5.7 (3.1 to 10.5) | 11.1 | 4.3 (0.4 to 41.3) |
| High-risk conditions | 24.6 | 29.7 (16.9 to 2.1) | 20.0 | 79.0 (34.4 to 182) | 28.7 | 18.2 (9.2 to 36.1) | 22.7 | 14.9 (1.6 to 143) |
| Medical condition¶ | ||||||||
| No condition | 0.6 | 1.0 | 0.3 | 1.0 | 1.6 | 1.0 | 1.2 | 1.0 |
| Chronic heart disease | 16.4 | 15.7 (8.8 to 28.0) | 10.8 | 33.6 (11.1 to 102) | 20.0 | 11.2 (5.5 to 22.8) | 14.4 | 10.8 (1.1 to 104) |
| Chronic lung disease | 6.8 | 16.4 (9.0 to 30.2) | 0.0 | 0 | 19.7 | 12.9 (6.4 to 25.8) | 26.4 | 5.1 (0.4 to 63.4) |
| Diabetes mellitus | 12.2 | 12.6 (7.4 to 21.2) | 4.8 | 14.7 (4.8 to 44.3) | 16.3 | 10.3 (5.5 to 19.5) | 13.7 | 2.8 (0.2 to 33.3) |
| Chronic liver disease | 11.0 | 13.0 (7.5 to 22.7) | 1.0 | 4.1 (0.5 to 31.9) | 20.4 | 11.9 (6.2 to 22.9) | 17.5 | 13.3 (1.4 to 128) |
| Chronic renal disease | 16.5 | 25.2 (10.3 to 61.8) | 12.4 | 120.7 (25.0 to 583) | 6.2 | 4.2 (0.6 to 31.5) | 77.6 | 51.3 (5.3 to 493) |
| Cancer | 28.8 | 43.3 (24.7 to 76.2) | 24.0 | 206.6 (80.6 to 530) | 39.2 | 26.5 (13.4 to 52.5) | 0.0 | 0 |
| Number of conditions | ||||||||
| 0 | 0.6 | 1.0 | 0.3 | 1.0 | 1.6 | 1.0 | 1.2 | 1.0 |
| 1 | 2.2 | 3.6 (1.8 to 7.1) | 1.3 | 5.3 (1.7 to 16.2) | 3.9 | 2.4 (1.0 to 5.5) | 0.0 | 0 |
| ≥2 | 18.3 | 18.7 (10.9 to 32.1) | 14.1 | 42.2 (18.5 to 96.6) | 19.8 | 11.9 (6.2 to 22.8) | 22.7 | 8.2 (0.9 to 79.2) |
*Adults ≥75 years were not included in the JMDC database.
†Per 100 000 person-years.
‡Age-adjusted and sex-adjusted RR.
§Sex-adjusted RR.
¶Results of subgroups with other medical conditions, including HIV/AIDS, alcoholism, asplenia, organ transplantation and cerebrospinal fluid leakage, are not shown.
JMDC, Japan Medical Data Center; RR, rate ratio.
Table 5.
Rates and RRs of invasive pneumococcal disease in the MDV database
| All ages (≥19 years) |
Age subgroups | |||||||
| 19–49 years | 50–64 years | ≥65 years | ||||||
| Rate* | RR† (95% CI) | Rate* | RR‡ (95% CI) | Rate* | RR‡ (95% CI) | Rate§ | RR‡ (95% CI) | |
| Overall | 4.6 | 1.5 | 3.8 | 5.9 | ||||
| Risk status | ||||||||
| Healthy (no condition) | 1.9 | 1.0 | 0.9 | 1.0 | 0.9 | 1.0 | 3.0 | 1.0 |
| At-risk conditions | 8.0 | 3.8 (2.4 to 6.2) | 4.0 | 4.0 (0.9 to 18.4) | 7.7 | 9.2 (2.7 to 31.1) | 8.7 | 3.0 (1.7 to 5.1) |
| High-risk conditions | 8.6 | 4.0 (2.4 to 6.7) | 4.2 | 4.7 (0.8 to 28.1) | 8.6 | 9.8 (2.8 to 34.7) | 9.2 | 3.1 (1.7 to 5.6) |
| Medical condition§ | ||||||||
| No condition | 1.9 | 1.0 | 0.9 | 1.0 | 0.9 | 1.0 | 3.0 | 1.0 |
| Chronic heart disease | 9.3 | 4.7 (2.8 to 7.9) | 17.7 | 18.4 (4.0 to 84.2) | 6.4 | 8.0 (2.0 to 32.0) | 9.6 | 3.3 (1.8 to 5.8) |
| Chronic lung disease | 13.8 | 7.1 (4.2 to 12.0) | 5.9 | 6.5 (1.1 to 39.0) | 18.4 | 21.4 (5.9 to 77.8) | 13.8 | 4.7 (2.5 to 8.7) |
| Diabetes mellitus | 8.5 | 4.4 (2.6 to 7.3) | 10.7 | 11.0 (2.4 to 50.6) | 8.5 | 10.4 (2.9 to 37.2) | 8.3 | 2.8 (1.6 to 5.2) |
| Chronic liver disease | 8.9 | 4.7 (2.7 to 8.2) | 5.7 | 5.9 (1.0 to 36.1) | 5.8 | 6.9 (1.6 to 28.9) | 11.1 | 3.8 (2.0 to 7.2) |
| Chronic renal disease | 9.1 | 4.7 (2.2 to 10.0) | 0 | 0 | 12.6 | 15.4 (3.1 to 76.8) | 9.3 | 3.2 (1.3 to 7.7) |
| Cancer | 8.6 | 4.4 (2.6 to 7.4) | 5.3 | 6.0 (1.0 to 36.2) | 7.6 | 8.6 (2.3 to 31.9) | 9.3 | 3.2 (1.8 to 5.9) |
| Number of conditions | ||||||||
| 0 | 1.9 | 1.0 | 0.9 | 1.0 | 0.9 | 1.0 | 3.0 | 1.0 |
| 1 | 3.1 | 1.6 (0.9 to 2.8) | 0 | 0 | 2.8 | 3.3 (0.8 to 13.4) | 4.0 | 1.4 (0.7 to 2.7) |
| ≥2 | 12.1 | 5.8 (3.6 to 9.5) | 11.6 | 11.6 (2.5 to 54.0) | 12.9 | 16.2 (4.7 to 55.7) | 11.9 | 4.1 (2.3 to 7.1) |
*Per 100 000 person-years.
†Age-adjusted and sex-adjusted RR.
‡Sex-adjusted RR.
§Results of subgroups with other medical conditions, including HIV/AIDS, alcoholism, asplenia, organ transplantation and cerebrospinal fluid leakage, are not shown.
MDV, Medical Data Vision; RR, rate ratio.
In both databases, PP and IPD rates increased with age. In the JMDC database, the rate of PP increased from 8.3 per 100 000 person-years in adults aged 19–49 years and 21.6–78.0 per 100 000 person-years in adults aged 50–64 years and those aged ≥65 years, respectively. The rate of IPD increased from 0.5 per 100 000 person-years in adults aged 19–49 years and 3.3–4.9 per 100 000 person-years in adults aged 50–64 years and ≥65 years, respectively. In the MDV database, the rate of PP increased from 24.9 per 100 000 person-years to 46.8 and 150.8 per 100 000 person-years in adults aged 50–64 years and those aged ≥65 years, respectively. The IPD rate increased from 1.5 per 100 000 person-years in adults aged 19– 49 years and 3.8–5.9 per 100 000 person-years in adults aged 50–64 years and those aged ≥65 years, respectively.
Compared with healthy adults of the same age in the JMDC database, the risk of PP in younger and older adults was highest in patients with chronic renal disease (RR=23.6 (19–49 years); RR=23.7 (≥65 years)), whereas the risk of PP in adults aged 50–64 years was highest in patients with chronic lung disease (RR=12.8). In the MDV database, the risk of PP was highest in patients with chronic lung disease across all age groups compared with healthy adults of the same age (RR=5.6 (19–49 years); RR=6.8 (50–64 years); RR=4.9 (≥65 years)).
Compared with healthy adults of the same age, the risk of IPD was highest in adults with cancer aged 19–49 years and 50–64 years in the JMDC database (RR=206.6 and 26.5, respectively), whereas the risk of IPD was highest in older adults with chronic renal disease (RR=51.3). In the MDV database, the risk of IPD was highest in young adults with chronic heart disease (RR=18.4), and adults aged 50–64 years and those aged ≥65 years with chronic lung disease (RR=21.4 and 4.7, respectively) compared with healthy adults of the same age.
Across all ages, PP and IPD rates were highest in adults with two or more medical conditions. PP rates in adults with two or more underlying medical conditions were 9–17 times and 3–4 times the rate in healthy adults of the same age in the JMDC and MDV databases, respectively. IPD rates in adults with two or more underlying medical conditions were 8–42 times and 4–16 times the rates in healthy adults in the JMDC and MDV databases, respectively. The PP rates in high-risk adults were 10–17 times and 2–3 times the rate in healthy adults of the same age in the JMDC and MDV databases, while the IPD rates were 15–79 times and 3–10 times the rates in healthy adults in the JMDC and MDV databases, respectively.
Discussion
The Japanese Respiratory Society Guidelines for the Management of Community-Acquired Pneumonia in Adults14 recommend pneumococcal vaccination for individuals aged 2–64 years who have an underlying medical condition. However, little is known about the real-world burden of pneumococcal disease in Japanese adults with these conditions. This retrospective cohort study used two healthcare databases to evaluate the burden of pneumococcal disease in at-risk adults and adults with high-risk medical conditions to close this data gap in Japan.
Similar to previous research,4 18 25 the principal findings of our study revealed that adults with an underlying medical condition were at increased risk of PP and IPD, compared with adults without these conditions. This was found among older adults aged ≥65 years and among younger adults aged 19–64 years. Our study also showed that the risk of PP and IPD increased with the number of underlying medical conditions in both younger and older adults, supporting the concept of ‘risk-stacking’ demonstrated by previous studies.3 17 18 28
We also found some differences in the conditions that place individuals at increased risk of pneumococcal disease between younger and older adults. While the risk of PP and IPD was highest in older adults with chronic renal and lung diseases, the risk of PP and IPD in adults aged 50–64 years was highest among patients with chronic lung disease and cancer. These results are similar to those of a previous study in which adults with chronic obstructive pulmonary disease were found to have the highest risk of IPD.28
In adults aged 50–64 years with an underlying medical condition, PP rates in the JMDC database and IPD rates in both the JMDC and MDV databases were higher than the rates in healthy older adults aged ≥65 years, while the same trend was not observed for PP rates in the MDV database. Although pneumococcal vaccination history was not available in the two databases, the pneumococcal vaccination rate was considered low in adults aged ≥65 years during our study period, which ended in 31 December 2014. This is because there was little overlap between our study period and the National Immunisation Programme in Japan, which has provided a subsidy for PPV23 vaccination for adults aged ≥65 years as of 1 October 2014.13 The influence of the subsidy for PPV23 vaccination on the PPV23 vaccination rate in adults aged ≥65 years was considered marginal during our study period. Thus, our results imply that adults aged 50–64 years with an underlying medical condition may be at a greater risk of pneumococcal disease compared with healthy adults aged ≥65 years.
The 7-valent pneumococcal conjugate vaccine (PCV7) has been routinely used in children in Japan since 2010, although it has been replaced with the 13-valent PCV (PCV13) since 2013. Estimated PCV7 vaccination rates in Japan were reported to be <10% in 2010, 50–60% in 2011 and 80–90% in 2012.29 Therefore, it is important to consider the potential indirect effect of the childhood PCV programme on RR estimates of adult diseases, because our study spans several years before and after the introduction of the childhood PCV programme. A post hoc analysis to explore rates and RR for PP and IPD before (2010 or earlier) and after (2011 or later) the routine use of PCVs (online supplementary table 2–5) demonstrated that the risk of PP and IPD in adults with an underlying medical condition remained consistently high over both time periods, suggesting that an indirect effect in adults had not yet been observed. Thus, we concluded that the childhood PCV programme did not significantly impact the risk of PP and IPD in adults with an underlying medical condition during our study period.
The rates of PP and IPD were higher in the MDV than in the JMDC database in adults with and without an underlying medical condition across all age subgroups. This may not be surprising given that the two databases are drawn from different adult populations in Japan. Adults in the JMDC database represent a population of younger working adults, while those in the MDV database represent a population in need of healthcare services (ie, hospitalised patients and outpatients). These differences in background characteristics may explain the variation in risk of PP and IPD between the two databases. Thus, the results from either database alone may not be generalisable to the general population of adults in Japan. Nonetheless, results from both databases indicate that both younger and older adults with an underlying medical condition in Japan are at increased risk of pneumococcal disease compared with healthy adults of the same age. The findings observed in Japan are consistent with similar studies conducted in the USA and Germany.3 17 18 25
Limitations
This study had some limitations. Regarding the internal validity, using ICD-10 codes to identify medical conditions and episodes of PP and IPD may lead to misclassification. In addition, PP is often undercoded in claims data. Owing to the limited data availability in the two databases, these analyses did not consider potential confounders other than age and sex, such as pneumococcal vaccination history, residential environment and lifestyle factors, such as smoking and drinking, which might significantly influence the risk of PP and IPD. Regarding external validity, results from only one database cannot be extrapolated to the general population of adults in Japan, as subjects in the two databases may be representative of different adult populations.
Conclusion
Adults of all ages with an underlying medical condition, including immunocompetent and immunocompromised adults, are at greater risk of pneumococcal disease, compared with adults without any condition in Japan. This risk increases with the number of underlying medical conditions. Adults aged 50–64 years with an underlying medical condition have a greater risk of pneumococcal disease than adults aged ≥65 years without any condition. Our study findings can help healthcare practitioners and policy makers identify patient groups that are vulnerable to pneumococcal disease and can benefit from pneumococcal vaccination. Adults aged ≥65 years as well as adults aged 60–64 years with a specific medical condition are eligible to receive the subsidy for PPV23 under the National Immunisation Programme in Japan.13 However, our results support extending the pneumococcal vaccination to younger adults with an underlying medical condition, especially those aged 50–64 years.
Supplementary Material
Acknowledgments
This study was supported by MSD K.K. (Japan). The authors thank Keri Yang, Aya Yano, Kayoko Yoshinuma, Mio Komura and Megumi Yoshinaga for contributing to the development of the study concept and protocol. The authors thank William Ng, MD, PhD and J Ludovic Croxford, PhD, for providing medical writing support.
Footnotes
Contributors: KI contributed to the conception or design of the study, and the acquisition, analysis, interpretation of the data and drafting the manuscript. TP and MAK contributed to interpretation of the data and revision of the paper for important intellectual content. KN and MA contributed to interpretation of data and provided comments from a pulmonologist’s point of view. AS contributed to analysis of the data and revision of the paper. SK contributed to the conception and design of the study, the acquisition and interpretation of data and drafting the manuscript. All authors gave final approval of the version to be published.
Funding: This study was funded by MSD K.K.
Competing interests: KI, AS and SK are employees of MSD K.K., a group of Merck Sharp & Dohme Corp., which is a subsidiary of Merck & Co., Inc. (Kenilworth, New Jersey, USA). KN and MA received research grants and lecture fees from MSD K.K. TP and MAK are employees of Merck & Co., Inc. Employees may hold stock and/or stock options in the company. The study sponsor, Merck & Co., Inc., and MSD K.K. reviewed the study design; participated in the collection, analysis and interpretation of the data; critically reviewed the report and decided to submit the paper for publication.
Patient consent: Not required.
Ethics approval: This study was approved by the ethics committee of Kameda Medical Center, Chiba, Japan, in October 2015, before the initiation of this study.
Provenance and peer review: Not commissioned; externally peer reviewed.
Data sharing statement: Data are available on request from the corresponding author.
Presented at: Abstract and poster (#301) at the 10th International Symposium on Pneumococci and Pneumococcal Diseases, 26–30 June 2016, Glasgow, Scotland. Joint meeting of the 59th Annual Meeting of the Japanese Association for Infectious Diseases in the Central Japan Region, the 86th Annual Meeting of the Japanese Association for Infectious Diseases in the Western Japan Region and the 64th Annual Meeting of the Western Chapter of the Japanese Society of Chemotherapy, 24–26 November 2016, Okinawa, Japan.
References
- 1.Blasi F, Mantero M, Santus P, et al. . Understanding the burden of pneumococcal disease in adults. Clin Microbiol Infect 2012;18(Suppl 5):7–14. 10.1111/j.1469-0691.2012.03937.x [DOI] [PubMed] [Google Scholar]
- 2.Drijkoningen JJ, Rohde GG. Pneumococcal infection in adults: burden of disease. Clin Microbiol Infect 2014;20(Suppl 5):45–51. 10.1111/1469-0691.12461 [DOI] [PubMed] [Google Scholar]
- 3.Kyaw MH, Rose CE, Fry AM, et al. . Active Bacterial Core Surveillance Program of the Emerging Infections Program Network. The influence of chronic illnesses on the incidence of invasive pneumococcal disease in adults. J Infect Dis 2005;192:377–86. 10.1086/431521 [DOI] [PubMed] [Google Scholar]
- 4.Shea KM, Edelsberg J, Weycker D, et al. . Rates of pneumococcal disease in adults with chronic medical conditions. Open Forum Infect Dis 2014;1:ofu024 10.1093/ofid/ofu024 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Bridges CB, Coyne-Beasley T. Advisory Committee on Immunization Practices Recommended Immunization Schedule for Adults Aged 19 Years or Older: United States, 2014*. Ann Intern Med 2014;160:190-197 10.7326/M13-2826 [DOI] [PubMed] [Google Scholar]
- 6.Public Health Agency of Canada. Recommendations for use of pneumococcal 23-valent polysaccharide vaccine during shortage. http://www.phac-aspc.gc.ca/publicat/ccdr-rmtc/04vol30/acs-dcc-4/index-eng.php.
- 7.Joint Committee on Vaccination and Immunisation. Statement on the wider use of pneumococcal conjugate vaccines in the UK. 2013. https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/224765/JCVI_statement_on_pneumococcal_vaccination_for_clinical_risk_groups_Final.pdf.
- 8.German Standing Committee on Vaccination. Recommendations of the standing committee on vaccination (stiko) at the robert koch institute - 2016/2017. http://www.rki.de/EN/Content/infections/Vaccination/recommandations/34_2016_engl.pdf?__blob=publicationFile.
- 9.Moberley S, Holden J, Tatham DP, et al. . Vaccines for preventing pneumococcal infection in adults. Cochrane Database Syst Rev 2013;1:CD000422 10.1002/14651858.CD000422.pub3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kawakami K, Ohkusa Y, Kuroki R, et al. . Effectiveness of pneumococcal polysaccharide vaccine against pneumonia and cost analysis for the elderly who receive seasonal influenza vaccine in Japan. Vaccine 2010;28:7063–9. 10.1016/j.vaccine.2010.08.010 [DOI] [PubMed] [Google Scholar]
- 11.Maruyama T, Taguchi O, Niederman MS, et al. . Efficacy of 23-valent pneumococcal vaccine in preventing pneumonia and improving survival in nursing home residents: double blind, randomised and placebo controlled trial. BMJ 2010;340:c1004 10.1136/bmj.c1004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Suzuki M, Dhoubhadel BG, Ishifuji T, et al. . Adult Pneumonia Study Group-Japan (APSG-J). Serotype-specific effectiveness of 23-valent pneumococcal polysaccharide vaccine against pneumococcal pneumonia in adults aged 65 years or older: a multicentre, prospective, test-negative design study. Lancet Infect Dis 2017;17:313–21. 10.1016/S1473-3099(17)30049-X [DOI] [PubMed] [Google Scholar]
- 13.Ministry of Health, Labour and Welfare of Japan. Amendment of Code of Practice for Immunization (2014). No. 159, issued on 16-Jul-2014. http://www.mhlw.go.jp/file/06-Seisakujouhou-10900000-Kenkoukyoku/0000121144.pdf.
- 14. [The JRS guidelines for the management of community acquired pneumonia in adults]. Nihon Kokyuki Gakkai Zasshi 2007;Suppl(Suppl):2–85. [PubMed] [Google Scholar]
- 15.Miyashita N, Matsushima T, Oka M, et al. . The JRS guidelines for the management of community-acquired pneumonia in adults: an update and new recommendations. Intern Med 2006;45:419–28. 10.2169/internalmedicine.45.1691 [DOI] [PubMed] [Google Scholar]
- 16.Morrill HJ, Caffrey AR, Noh E, et al. . Epidemiology of pneumococcal disease in a national cohort of older adults. Infect Dis Ther 2014;3:19–33. 10.1007/s40121-014-0025-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Pelton SI, Shea KM, Farkouh RA, et al. . Rates of pneumonia among children and adults with chronic medical conditions in Germany. BMC Infect Dis 2015;15:470 10.1186/s12879-015-1162-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Weycker D, Farkouh RA, Strutton DR, et al. . Rates and costs of invasive pneumococcal disease and pneumonia in persons with underlying medical conditions. BMC Health Serv Res 2016;16:182 10.1186/s12913-016-1432-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Japan Medical Data Center. JMDC Claims Database. https://www.jmdc.co.jp/en/about/database.html.
- 20.Nakamura M. Utilization of MDV data and data quality control. Jpn J Pharmacoepidermiol 2016;21:23–5. [Google Scholar]
- 21.Hashikata H, Harada KH, Kagimura T, et al. . Usefulness of a large automated health records database in pharmacoepidemiology. Environ Health Prev Med 2011;16:313–9. 10.1007/s12199-010-0201-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Tanaka S, Seto K, Kawakami K. Pharmacoepidemiology in Japan: medical databases and research achievements. J Pharm Health Care Sci 2015;1:16 10.1186/s40780-015-0016-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Davis KL, Meyers J, Zhao Z, et al. . High-Risk Atherosclerotic Cardiovascular Disease in a Real-World Employed Japanese Population: Prevalence, Cardiovascular Event Rates, and Costs. J Atheroscler Thromb 2015;22:1287–304. 10.5551/jat.28852 [DOI] [PubMed] [Google Scholar]
- 24.Urushihara H, Taketsuna M, Liu Y, et al. . Increased risk of acute pancreatitis in patients with type 2 diabetes: an observational study using a Japanese hospital database. PLoS One 2012;7:e53224 10.1371/journal.pone.0053224 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Pelton SI, Weycker D, Farkouh RA, et al. . Risk of pneumococcal disease in children with chronic medical conditions in the era of pneumococcal conjugate vaccine. Clin Infect Dis 2014;59:615–23. 10.1093/cid/ciu348 [DOI] [PubMed] [Google Scholar]
- 26.Centers for Disease Control and Prevention (CDC). Use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine for adults with immunocompromising conditions: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep 2012;61:816–9. [PubMed] [Google Scholar]
- 27.Various Information of Medical Fee, operated by Ministry of Health, Labour and Welfare Japan. Injury name master. http://www.iryohoken.go.jp/shinryohoshu/searchMenu/doSearchInputBp.
- 28.Baxter R, Yee A, Aukes L, et al. . Risk of underlying chronic medical conditions for invasive pneumococcal disease in adults. Vaccine 2016;34:4293–7. 10.1016/j.vaccine.2016.07.003 [DOI] [PubMed] [Google Scholar]
- 29.Chiba N, Morozumi M, Shouji M, et al. . Invasive Pneumococcal Diseases Surveillance Study Group. Changes in capsule and drug resistance of Pneumococci after introduction of PCV7, Japan, 2010-2013. Emerg Infect Dis 2014;20:1132–9. 10.3201/eid2007.131485 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
bmjopen-2017-018553supp001.jpg (132.5KB, jpg)
bmjopen-2017-018553supp002.pdf (129.9KB, pdf)