

Abstract
Introduction:
Diabetes is progressive condition which requires various ways of treatment. Adequate therapy prescribed in the right time helps patient to postpone development of complications. Adherence to complicated therapy is challenge for both patients and HCPs and is subject of research in many disciplines. Improvement in communication between HCP and patients is very important in patient’s adherence to therapy.
Aim:
Aim of this research was to explore validity and reliability of modified SERVQUAL instrument in attempt to explore ways of motivating diabetic patient to accept prescribed insulin therapy.
Material and Methods:
We used modified SERVQUAL questionnaire as instrument in the research. It was necessary to check validity and reliability of the new modified instrument.
Results:
Results show that modified Servqual instrument has excellent reliability (α=0.908), so we could say that it measures precisely Expectations, Perceptions and Motivation at patients. Factor analysis (EFA method) with Varimax rotation extracted 4 factors which together explain 52.902% variance of the results on this subscale. Bifactorial solution could be seen on Scree-plot diagram (break at second factor).
Conclusion:
Results in this research show that modified Servqual instrument which is created in order to measure expectations and perceptions of the patients is valid and reliable. Reliability and validity are proven indeed in additional dimension which was created originally for this research - motivation to accept insulin therapy.
Keywords: SERVQUAL, insulin therapy, Diabetes mellitus type 2, Healthcare quality
1. INTRODUCTION
Diabetes is progressive condition which requires different ways of treatment depending on the stage of development. Adequate therapy prescribed in the right time helps patient to postpone development of complications which are expected to happen in the late stage. If diagnosed in time, Type 2 diabetes can be treated with modification in food, physical activity, stress control, oral therapy (i.e. metformin, sulphonylurea, DPP 4 inhibitors), but as time goes by more complex therapy will be a must. This therapy is called substitution therapy and could be incretin or insulin based. Although most of the doctors agree that initiating incretin or insulin therapy is efficient way of treatment many of them take this as a last option because their patients are refusing to accept and adhere to therapy which requires usage of needle. Additional moment in postponement of the therapy is lack of time which is crucial for education and helping patient to fight prejudices and fears connected with insulin (or needle) usage. Most of the prejudices and fears are result of lack of knowledge about diabetes as a condition or ways of living with diabetes (1).
All these issues put a big challenge in front of healthcare professional. How to motivate patient to accept prescribed therapy and adhere to it? At the same time motivating patient to accept the therapy becomes very important for the researchers in few scientific disciplines, medicine, psychology, pharmacy, health promotion and marketing which requires multidisciplinary approach. The concept of adherence, which indicates the degree to which a person follows the doctor’s advice, in terms of taking medication, observing a diet, or realizing a change in lifestyle is perceived as one of the main aspects to consider when dealing with diabetes, because this type of condition requires a high level of responsibility and activity from patients with respect to treatment. Some authors state that there are “patient-related and health care professional–related barriers to initiating insulin, some of which overlap” (2, 3, 4).
SERVQUAL provides a technology for measuring and managing service quality (SQ). Technology was first published in 1985. Since then its innovators Parasuraman, Zeithaml and Berry, have further developed, promulgated and promoted SERVQUAL through a series of publications (5, 6, 7, 8), SERVQUAL model is developed in order to analyze and improve the relationship between customer and service provider, in a way that knowing the gaps between perception and expectation of the service means making the relationship and communication smoother. It consists of 22 questions divided in five groups according to issues it is dealing with (i.e. Tangibility, Responsiveness, Reliability, Assurance and Empathy) SERVQUAL is intended to measure functional quality, not just technical, what is important, because, technical properties of various industries are different, but functional is similar for all service industries (6).
Objectives of this research were to investigate and explore following issues:
Modify SERVQUAL instrument according to specific situation in Bosnia and Herzegovina, to healthcare industry, revalidate the instrument and test it’s psychometric characteristics;
Explore possibility to use modified SERVQUAL instrument on patient’s motivation to accept insulin therapy.
2. MATERIALS AND METHODS
2.1. Quantitative Methods
Quantitative analysis was used as main method, all the concepts were reviewed by using the existing work in this field. We used SERVQUAL questionnaire as instrument in the research. This model has been in use since 1988 and is used in various service industries (6). Model is tested in healthcare industry, and satisfied validity and reliability requirements.
2.2. Questionnaire Preparation
Original instrument was modified so we can state we got new instrument and it was necessary to check validity and reliability of the new instrument:
First is the scale that is originally 7 degrees Likert scale, and was modified to 5 degrees. This has been used in research in this area (9, 10). Bigger scale is complicated for the most of people that should be questioned. This approach is recommended by Buttle (1996) who characterize 7 degrees Likert scale in SERVQUAL as flawed (11).
Second modification was modification of number of questions through dimensions and instrument in total. This modification was done in two steps. Standard SERVQUAL scale consists of 22 questions divided in 5 dimensions. Prior to analysis pilot research was conducted in order to increase validity and improve questionnaire as well as adapt it better to existing situation in Bosnia and Herzegovina. This approach was performed in the first study which used SERVQUAL in health. It resulted with shortening the questionnaire to 15 questions in 5 dimensions, out of original 22 questions (9). Researcher found three questions biased after translation so after first modification questionnaire had 18 questions.
Final number of questions is 13 through all five SERVQUAL dimensions (i.e. Tangibility, Responsiveness, Reliability, Assurance and Empathy).
Third modification was addition to existing scales (expectation and perception) which stated level of motivation to accept the therapy influenced by performed service. Validity was checked externally by the adequate sample, as well as internally, content validity by exploring participant’s knowledge and attitude and construct validity by demonstrating factor analysis. Reliability of the new instrument was tested via Cronbach’s alpha coefficient. This model is used in original calibration of SERVQUAL instrument.
Quantitative analysis was conducted by the method of surveying, using questionnaire, specially adapted and designed to cover all the important aspects. Survey was finally distributed to respondents: SERVQUAL covered patient’s (consumer’s) expectation, perception and motivation to accept insulin therapy. This questionnaire was filled by patients
2.3. Sample and Data Collection
Authors applied to obtain allowance from the authorities from clinical centers and health centers in Sarajevo and Tuzla, Clinical hospital Mostar and Cantonal Hospital Zenica, as well as Health Centers Mostar, Stari Grad Mostar and Zenica.
Population is urban and is connected to HCPs who are providing the service. Urban population is chosen because there is a huge difference between urban and rural population in the way of living, food, physical activity and level of stress. Sample size of patients was planned with confidence interval of 95%, acceptable margin of error is 5%, and response distribution 50 %.
Sample of patient’s was specifically set for the research. Patients’ with diabetes type 2 on insulin therapy age 45-55 years from four main centers in Federation of Bosnia and Herzegovina were included in the research. Questionnaires were distributed to 700 patients. Method of distribution was:
Via patient’s associations (Sarajevo and Zenica) 200;
Snowball method to patients who knew somebody from chosen population 150; and
Via HCPs in health centers who found patients from chosen population 350.
We received back 574 filled questionnaires, and after first check sample was reduced to 511 patients. Reasons for non-acceptance were:
Patients with type 1 diabetes; and
Inappropriate filling of questionnaire.
Final reduction was performed after box plot analysis which reduced sample to 491 patients with type 2 DM and that was set as final patient’s sample.
Sample of patients was set by non-random convenience method, with possible description of snowball sampling because specific population is very difficult to be found. Sample is reliable although is not random, because it is very close to total population. Data was collected at one point of time, meaning, survey was cross-sectional. Questionnaires were self-administered. Having in mind the problem of motivation which we plan to analyze population that is older than 55 but have experience of 10+ years on insulin therapy.
Distribution of the questionnaires for the patients went through Health Centers, each of the family medicine doctors distributed 2-5 questionnaires to patients. Family physicians or nurses helped in completing a questionnaire for each of up to 5 consecutive eligible patients (12). This way of surveying patients by family medicine doctors or nurses is common practice. Other way of distribution was through patients associations, specially in Zenica and Sarajevo.
All the surveys are filled in period February-May 2015. Data is collected by June 2015. Process of statistical analysis is completed by September of 2015.
3. RESULTS
We were exploring psychometric characteristics of the instrument which is modified from SERVQUAL instrument introduced by Parasuraman. Original instrument was reduced and modified in terms of adding new subscale for motivation to accept insulin therapy. Instrument consists of 39 questions, separated in 3 subscales with 13 identical questions each. First subscale measures expectations, second perceptions of experience and third motivation to accept prescribed therapy. Each subscale has 5 dimensions first 2 questions measure Tangibility, next 3 questions (3 to 5) measure Reliability, next 2 questions (6 and 7) measure Responsiveness, than 3 questions (8 to 10) measure Assurance, and last 3 questions (11 to 13) measure Empathy.
It is important to emphasize that this is new instrument because of huge redesign, so the results which are shown must be viewed and analyzed critically in order to get the best possible modification of instrument and improve motivation of patient to accept insulin therapy.
When we analyze psychometric characteristics of some instrument we have to show reliability and validity of the instrument.
Reliability of the instrument is capability of instrument to measure precisely in appropriate way construct we are measuring. Analysis that is most often used for proving reliability is internal consistency reliability measurement by Cronbach’s coefficient.
3.1. Reliability of Servqual for Patients – Motivation
It is expected that reliability inside dimensions could be questionable because of minimum quantity of questions. Reliability of subscale Motivation is acceptable (α=0.727), much better than reliability of its separated parts (dimensions). This shows that this subscale measures more accurately than its dimensions separately. Responsiveness dimension has questionable reliability and other dimensions have bad reliability (Table 1).
Table 1. Overview of reliability of dimensions and subscale Motivation.
| Dimension | Cronbachα | Description |
|---|---|---|
| Tangibility | 0.387 | Unacceptable |
| Reliability | 0.492 | Unacceptable |
| Responsiveness | 0.653 | Questionable |
| Assurance | 0.537 | Bad |
| Empathy | 0.496 | Unacceptable |
| Motivation | 0.727 | Acceptable |
3.2. Reliability of Servqual Instrument for Patients
Results show that Servqual instrument has excellent reliability (α=0.908), so we could say that it measures precisely Expectations, Perceptions and Motivation at patients. On the other hand, average value of inter-item correlations - 0.196 suggests weak relationship between 39 Servqual questions. Finally, reliability of the subscales is much better than reliability of dimensions inside subscales and reliability of modified SERVQUAL instrument is much better than those on subscales and could be marked as excellent.
When we look at subscales, Perception has excellent reliability, Expectation has good and Motivation acceptable reliability (Table 2).
Table 2. Reliability of Servqual instrument filled by patients.
| Cronbachα | Summary Item Statistics | ||||||
|---|---|---|---|---|---|---|---|
| Inter-Item Correlations | Mean | Minimum | Maximum | ||||
| 0.908 | 0.196 | -0.091 | 0.654 | ||||
| Items | Corr. Item-Total Correl. | Items | Corr. Item-Total Correl. | ||||
| exp_1 | 0.469 | perc _8 | 0.572 | ||||
| exp _2 | 0.386 | perc _9 | 0.591 | ||||
| exp _3 | 0.482 | perc _10 | 0.571 | ||||
| exp _4 | 0.508 | perc _11 | 0.602 | ||||
| exp _5 | 0.444 | perc _12 | 0.470 | ||||
| exp _6 | 0.412 | perc _13 | 0.610 | ||||
| exp _7 | 0.390 | motiv_1 | 0.433 | ||||
| exp _8 | 0.475 | motiv_2 | 0.219 | ||||
| exp _9 | 0.468 | motiv_3 | 0.328 | ||||
| exp _10 | 0.463 | motiv_4 | 0.265 | ||||
| exp _11 | 0.485 | motiv_5 | 0.297 | ||||
| exp_12 | 0.271 | motiv_6 | 0.184 | ||||
| exp _13 | 0.368 | motiv_7 | 0.229 | ||||
| perc_1 | 0.575 | motiv_8 | 0.251 | ||||
| perc _2 | 0.336 | motiv_9 | 0.332 | ||||
| perc _3 | 0.504 | motiv_10 | 0.314 | ||||
| perc _4 | 0.581 | motiv_11 | 0.251 | ||||
| perc _5 | 0.524 | motiv_12 | 0.241 | ||||
| perc _6 | 0.609 | motiv_13 | 0.314 | ||||
| perc _7 | 0.572 | ||||||
3.3. Validity of Servqual for Patients
Validity of the instrument is defined as capability of instrument to measure exactly what is created for to measure. When analyzing instrument’s validity we must be aware of three sorts of validity: 1) content validity, 2) construct validity which can be convergent and discriminant / divergent validity and 3) criterion validity.
Specific way of analyzing validity is factor analysis. There are two types of factor analysis - exploratory and confirmatory factor analysis. Exploratory factor analysis (EFA) is in line with basic theoretical setup of FA meaning it is exploring the structure that is behind the major set of variables. Confirmatory FA is testing and confirming if the measurements of the construct are in line or consistent with understanding the nature of that construct, meaning - does the construct has theoretical and practical sense? Basically the way of analysis is opposite. EFA is exploring the construct and CFA is confirming and accepting or rejecting the construct (13).
3.4. Validity of Servqual for Patients – Motivation
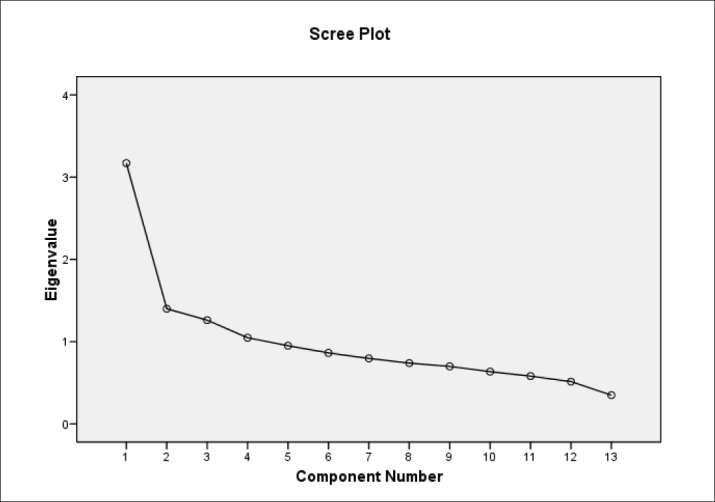
Factor analysis (EFA method) with Varimax rotation extracted 4 factors which together explain 52.902% variance of the results on this subscale. Bifactorial solution could be seen on Scree-plot diagram (break at second factor). Questions 6 to 8 (dimensions Responsiveness and part of Assurance) are grouped in the first factor, questions from 1 to 5 (dimensions Tangibility and Reliability) are grouped in the second factor. Questions from 11 to 13 (Empathy dimension) are grouped in third factor and Questions 9 and 10 (most of Assurance dimension) are grouped in fourth factor. (Figure 1)
Figure 1. Scree-plot Motivation subscale–patients.
3.5. Validity of Servqual Instrument Scale for Patients
Factor analysis of SERVQUAL instrument (EFA method) with Varimax rotation extracted 3 factors which together explain 39.195% variance of results. Four factors solution could be seen on Scree-plot diagram (break at fourth factor). Whole perception subscale with two questions from motivation subscale (15 questions total) are grouped in the first factor. Expectations subscale (13 questions) are grouped in the second factor. Rest of the Motivation subscale (11 questions) is grouped in the third factor. According to this we could call three factors by dimensions respectively.
This suggests that construct of SERVQUAL instrument is valid.
Table 3. Overview of validity of subscales and Servqual instrument in total.
| Subscale | Factors | Dimensions | % explanation of results variance | |
|---|---|---|---|---|
| Expectations | 2 | 1 | Responsiveness, Assurance, Empathy | 49.374 |
| 2 | Tangibility, Reliability | |||
| Perception | 1 | 1 | Tangibility, Reliability, Responsiveness, Assurance, Empathy | 47.808 |
| Motivation | 4 | 1 | Responsiveness and part of Assurance | 52.902 |
| 2 | Tangibility and Reliability | |||
| 3 | Empathy | |||
| 4 | Bigger part of Assurance | |||
| Servqual TOTAL | 3 | 1 | Perception | 39.195 |
| 2 | Expectations | |||
| 3 | Motivation | |||
4. DISCUSSION
We can say that SERVQUAL instrument with subscales has generally good psychometric characteristics in explaining the phenomena it is created for. Reliability of SERVQUAL subscales is much better than of dimensions most likely because of number of questions. When we look at subscales, Perception has excellent reliability, Expectation has good and Motivation acceptable reliability.
Reliability of modified SERVQUAL instrument is much better than those on subscales and could be marked as excellent. Inside the subscales has the lowest reliability of motivation in comparison to other subscales. Generally, when explaining validity of SERVQUAL instrument and it’s subscales we can say that subscales of SERVQUAL instrument show one to fourth factor’s solution with explanation of results variance of almost 53%. But since each of the subscales consists of 5 dimensions we could expect multifactorial solutions. If we have in mind the fact that variance is explained approximately 50% we could state that subscales of SERVQUAL instrument are relatively valid in what they are constructed to measure. Nevertheless, according to EFA setup, this percentage of variance explanation could be perceived as successful. Motivation subscale explains the phenomenon the best, than expectations and perception scale which is the weakest in explaining motivation of the patient to accept the therapy. SERVQUAL instrument shows three factor solution as it was expected. Percentage of variance explanation on the instrument is lower than the one at subscales so we can state that SERVQUAL measures expectations, perceptions and motivations less than the subscales. SERVQUAL instrument in total measures better perception, expectations and the least motivation.
We can conclude that SERVQUAL instrument with the subscales has relatively good psychometric characteristics in exploring phenomena it is constructed for, with the fact that, inside the subscales, measuring motivation to accept the therapy has the weakest reliability and strongest validity compared to other subscales. We can conclude that :
Looking from the patient’s perspective SERVQUAL instrument with the subscales has generally relatively good psychometric characteristics;
Inside the subscales instrument has the weakest reliability and the strongest validity in exploring patient’s motivation in comparison to other subscales; and
After performing planned research and all the analysis we can conclude that SERVQUAL model could be used as a model in creating algorithm for conducting conversation with diabetic patient. Instrument which is modified from original according to set procedure is reliable and valid for analysis. Considering the fact that number of questions in the instrument is reduced because of lack of time which HCP has with the patient for conversation we can conclude that modified SERVQUAL instrument should be used in total because if it is divided in separate questions or dimensions or subscales, validity and reliability are lower. Motivation of the patient to adhere to insulin therapy can be analyzed with modified SERVQUAL instrument and we should make additional efforts to make the instrument even more precise.
The most important part is proven validity and reliability of Servqual scale in specific situation on specific population. Modified Servqual scale is valid and it is proven by choosing appropriate sample of all the participants in diabetic healthcare. This sample provided face validity. At the same time content validity is proven by using appropriate set of questions which are forming construct appropriate for planned analysis. Face and content validity fulfill theoretical translational validity. Empirical, criterion- related validity is proven by performing factor analysis. Factor analysis aggregated given set of items into set of factors which were based on bivariate analysis. Bivariate analysis calculated correlations between constructs. Higher correlation between items of same construct (convergent validity) and low correlations between items of different constructs (discriminant validity). All of the results had shown acceptable results which opened room for usage of modified Servqual in further research in this area. Reliability of the research is ensured by surveying people who are directly interested in the topic, who care about the topic and have experience to answer the questions. Internal consistency reliability is measured by Cronbach’s alpha reliability measure which estimated average inter-item correlation and item to total correlation.
CONCLUSION
Results in this research show that scale was reliable, specially at dimensions level. This is not only the case with original Servqual instrument which is created in order to measure expectations and perceptions of the patients, but reliability and validity are proven in additional dimension which was created originaly for this research - motivation to accept insulin therapy.
Funding:
This research did not receive any specific grant from funding profit, non-profit or public agencies
Authors contribution:
V.J. made substantial contribution to concept and design and interpretation of data, S.S. contributed in analysis N.C. revised manuscript and gave final approval of the version to be submitted. Dz.K. revised manuscript and gave final approval of the final version to be submitted.
Conflict of interest:
none declared.
REFERENCES
- 1.Aščić-Buturović B. Institut za NIR KCU Sarajevo; 2009. Predijabetes i dijabetes melitus tip 2. [Google Scholar]
- 2.Korytkowski M. When oral agents fail: practical barriers to starting insulin. International Journal of Obesity and Related Metabolic Disorders. 2002;26(3):18–24. doi: 10.1038/sj.ijo.0802173. [DOI] [PubMed] [Google Scholar]
- 3.Larme AC, Pugh JA. Evidence-Based Guidelines Meet the Real World: The case of diabetes care. Diabetes Care. 2001 Jan;24(10):1728–33. doi: 10.2337/diacare.24.10.1728. [DOI] [PubMed] [Google Scholar]
- 4.Brown JB, Harris SB, Webster-Bogaert S, Wetmore S, Faulds C, Stewart M. The role of patient, physician and systemic factors in the management of type 2 Diabetes mellitus. Family Practice. 2002;(19):344–9. doi: 10.1093/fampra/19.4.344. [DOI] [PubMed] [Google Scholar]
- 5.Parasuraman A, Zeithaml VA, Berry LL. A Conceptual Model of Service Quality and Its Implications for Future Research. Journal of Marketing. 1985;49(4):41. [Google Scholar]
- 6.Parasuraman A, Berry LL, Zeithaml VA. SERVQUAL: A Multiple-Item Scale For Measuring Consumer Perceptions of Service Quality. Journal of Retailing. 1988;64(1):12–40. [Google Scholar]
- 7.Parasuraman A, Berry L L, Zeithaml VA. Refinement and Reassessment of the SERVQUAL Scale. Journal of Retailing. 1991;67(4):420–50. [Google Scholar]
- 8.Parasuraman A, Zeithaml VA, Berry LL. Reassessment of Expectations as a Comparison Standard in Measuring Service Quality: Implications for Further Research. Journal of Marketing. 1994;58(1):111. [Google Scholar]
- 9.Babakus E, Mangold WG. Adapting the SERVQUAL scale to hospital services: an empirical investigation. Health Service Research. 1992;(26):767–86. [PMC free article] [PubMed] [Google Scholar]
- 10.Silvestro R. Applying gap analysis in the health service to inform the service improvement agenda. International Journal of Quality & Reliability Management. 2005;22(3):215–33. [Google Scholar]
- 11.Buttle F. SERVQUAL: review, critique, research agenda. European Journal of Marketing. 1996;30(1):8–32. [Google Scholar]
- 12.Harris SB, Kapor J, Lank CN, Willan AR, Houston T. Clinical inertia in patients with T2 DM requiring insulin in family practice. Canadian Family Physician. Le Médecin de famille Canadien. 2010;56:418–24. [PMC free article] [PubMed] [Google Scholar]
- 13.Rao CR, Chakraborty R. Amsterdam: North-Holland: 1991. Handbook of statistics. [Google Scholar]