

Abstract
Background
Malaria and helminths share the same geographical distribution in tropical Africa. Studies of the interaction of helminth and malaria co-infection in humans have been few and are mainly epidemiological, with little information on cellular immune responses. This study aimed to determine Cytokine profiles among patients co-infected with Plasmodium falciparum malaria and soil borne helminth attending Kampala International University Teaching Hospital (KIU).
Methods
A case control study of 240 patients were recruited at KIU teaching hospital. Patients with Plasmodium falciparum malaria were 55 (22.9%) and those with soil-borne helminths were 63 (26.3%). The controls were 89 (37.1%), while those co-infected with Plasmodium falciparum malaria and soil-borne helminths were 33 (13.8%). Cases were defined as having a positive blood smear for P. falciparum malaria, those with helminths or co-infections of the two. Negative controls were those with a negative blood smear for P. falciparum malaria and those with no stool parasitic infections. Patients presenting with signs and symptoms of malaria or those suspected of having helminths were recruited for the study. A panel of five cytokines (IFN-γ, TNF-α, IL-6, TGF-β and IL-10) were assayed from plasma samples in patients with and without Plasmodium falciparum malaria, patients with and without helminth, and then those co-infected with the two diseases diagnosis was done using thick blood smears stained with 10% Giemsa and stool examination was done following the Kato Katz technique following standard procedures.
Results
The prevalence of Plasmodium falciparum malaria by sex was 28 (11.7%) and 27 (11.3%) in male and female respectively. The overall prevalence of soil borne helminth was 26.3%, and among those harbouring helminths, 13.8% were co-infected with Plasmodium falciparum. Cytokine levels significantly differed across Plasmodium falciparum malaria, soil borne helminth infected patients and health controls for IFN-γ (P = 0.023), IL-10 (P = 0.008) and TGF-β (P = 0.0001). Cytokine levels significantly differed across Plasmodium falciparum malaria, soil borne helminth infected patients and patients co-infected with Plasmodium falciparum malaria and soil borne helminth for IL-10 (P = 0.004), IL-6 (P = 0.011) and TGF-β (P = 0.003).
Conclusion
An up-regulation of IFN-γ during Plasmodium falciparum malaria and an up-regulation of IL-10 and TGF-β in soil borne helminth infections was demonstrated. We demonstrate that co-infections of Plasmodium falciparum and soil borne helminth lead to an up-regulation of IL-10 and IL-6 and a down-regulation of TGF-β.
Trial registration No17/10-16
Keywords: Plasmodium falciparum malaria, Soil borne helminths, Th1 and Th2 cytokines, Co-infected
Background of this study
Malaria remains a global burden with approximately 584,000 deaths among an estimated 198 million cases annually [1]. The biggest disease burden is mainly encountered among children in sub-Saharan Africa [1, 2]. This scenario is further complicated by the overlapping distribution of parasitic diseases in the tropics [3, 4] among which malaria-helminths co-infections are common [3, 5, 6]. It is estimated that half a billion people in the developing world harbour one or multiple helminths [7]. Malaria and helminths co-infections are mainly driven by poverty, tropical environment, water bodies and poor control measures among others [8]. Compelling evidence from the few studies that have investigated the effect of malaria-helminths co-infections suggests that an interaction between the two diseases might influence the clinical outcome of the involved diseases. However, inconsistencies about the clinical outcome of these interactions on malaria are common, both protective and detrimental effects have been reported [9, 10]. It has been reported previously that helminths increase vulnerability to malaria [11, 12], increase malaria parasitemia [13, 14], with a subsequent increase in malaria disease severity [15, 16].
However, in other related studies no apparent effect of helminths co-infections on malaria risk or disease severity were observed [17–19]. On the contrary, in other studies concurrent helminths infections have been associated with low malaria incidence [20], decreased parasitemia [20, 21], protection from cerebral malaria [22], nephron protective effects [20–22], and a reduction in malaria disease severity [11, 20–24]. Although the underlying mechanisms responsible for these varying responses are not well characterized, compelling evidence suggests that host inflammatory cytokines might be key players.
Malaria infections are generally characterized by a T helper 1 (Th1) response predominated by a number of pro-inflammatory cytokines with a gradual shift to Th2 response as the disease progresses [25, 26]. Pro-inflammatory cytokines like IFN-γ and TNF-α have been demonstrated to play critical roles early in the infection [27, 28]. Conversely, if pro-inflammatory cytokines are not regulated by counter inflammatory cytokines like IL-10 and TGF-β, the resulting pathology is exacerbated [29]. On the other hand, helminths infections are characterized by a strong Th2 immune response [30, 31] dominated by an up-regulation of counter inflammatory cytokines like IL-10 and TGF-β [32, 33]. Therefore, it is likely that during poly-parasitism if the counter balance between the Th1 and Th2 immune responses is not achieved, the clinical course of involved diseases might be altered. It’s proposed that host cytokines might be partly involved in driving the clinical outcome of malaria-helminths co-infections. However, literature on how these interactions influence the host cytokine profiles is still scarce with the few available studies reporting contradictory findings [29]. With such inconsistences, the questions as to whether co-infections impact on malaria incidence, clinical outcome and disease severity have not been conclusively addressed. Furthermore, although cytokine responses have been extensively described in P. falciparum and soil borne helminth infection separately [34], few studies have looked at systemic cytokine level concentration in co-infection of malaria and soil borne helminth parasites. We therefore, determined Cytokine profiles (IFN-γ, TNF-α, IL-6, TGF-β and IL-10) associated with Plasmodium falciparum malaria and soil borne helminth co-infections among patients attending Kampala International University Teaching Hospital in Uganda.
Methods
Study design
A case–control study was conducted at Kampala International University Teaching Hospital Out Patients Department (OPD) in Bushenyi district. Cases were defined as having a positive blood smear for P. falciparum malaria, those with helminths or those co-infected with both diseases. Negative controls were those with a negative blood smear for P. falciparum malaria and those with no stool parasitic infections. Patients presenting with signs and symptoms of malaria or those suspected of having helminths were recruited for the study. From each patient and control, 5 ml of venous blood was collected into EDTA vacutainers. Malaria diagnosis and parasite quantification was done using Giemsa stained thin and thick blood smears [35]. Stool examination was done following the Kato Katz technique [36] and worm burden categorized following WHO guidelines [37]. For statistical analyses, cases were categorized as those with malaria or helminths alone and those co-infected with both malaria and helminths, these were compared with health controls.
Upon recruitment into the study, a detailed clinical history was sought from each patient. Physical examination of patients was performed by a medical office. Data recorded on the clinical form included the patient’s demographic characteristics, clinical presentation, and perceived onset of illness. Children with other stool parasitic infections, those on anti-helminthic and malarial treatment were excluded from the study.
Collection of blood samples
For immunological assays, 5 ml blood were collected from each patient in EDTA vacutainers and centrifuged for 10 min at 3000g using an Eppendorf centrifuge. Plasma was subsequently aliquoted and stored at − 20 °C in the hospital laboratory refrigerator until further analysis. Samples were later transported in an ice cold box to immunology and molecular biology laboratory at the College of Veterinary Medicine, Animal Resources and Biosecurity (COVAB), Makerere University for cytokine assay analysis.
Blood smear for malaria diagnosis
Upon recruitment, P. falciparum diagnosis was done using thin and thick blood smears stained with 10% Giemsa. Parasite evaluation was done by microscopic examination of 200 fields at 100× magnification and parasite density expressed as number of parasites/µl [35].
Cytokine assays
Panels of both pro-inflammatory and counter inflammatory cytokines (IFN-, TNF-, TGF-β, IL-6, IL-10,) were assayed from plasma samples using solid phase sandwich enzyme-linked immunosorbent assay (Bio-Rad, UK) assay following manufacturer’s instructions as previously described [38]. All assays were done in triplicate. Values of cytokine concentrations were extrapolated from standard curves obtained from recombinant cytokine standards using Graph Pad version 6 statistical software.
Stool collection and evaluation
Stool samples were collected in dry leaky proof plastic bottles and approximately 3 g were used. Stool examination was done following the Kato Katz technique [36] and worm burden categorized following WHO guidelines [37].
Statistical analyses
All data were anonymized prior to analysis using Graph Pad Prism version 6.0. All numerical variables was summarized using mean and standard error of the mean (SEM). Before analysis of cytokine data, deviation from normality was tested using D’Agostino-Pearson normality test. Because none of the cytokines presented a normal distribution, data were presented as medians. Comparisons between groups were done using Kruskal–Wallis non parametric test followed by Dunn’s post-test at a significant level (P < 0.05).
Results
Patient’s characteristics
In this study a total of 240 patients were recruited. The mean age of patients was 7.6 ± 3.0 years with a sex ratio of 1.1 (male: female). Patients with Plasmodium falciparum malaria were 55 (22.9%) and those with soil-borne helminths were 63 (26.3%). The controls were 89 (37.1%), while those co-infected with Plasmodium falciparum malaria and soil-borne helminths were 33 (13.8%) as shown in Table 1. The intensity of Plasmodium falciparum malaria by sex was 28 (11.7%) and 27 (11.3%) in male and female respectively. Severe Plasmodium falciparum was detected in only 4 (4.5%) patients as compared to those with moderate 8 (9.1%) and low parasite intensity 76 (86.4%). Plasmodium falciparum intensity according to sex was 42 (47.7%), 3 (3.4%) and 4 (4.5%) for low, moderate and severe respectively in males and 34 (38.6%), 5 (5.7%) and 0 (0.0%) for low, moderate and severe respectively in females.
Table 1.
Patient’s baseline characteristics
| Male | Female | Total | P value | |
|---|---|---|---|---|
| Soil-borne helminths | 30 (12.5%) | 33 (13.8%) | 63 (26.3%) | 0.539 |
| Ascaris lumbricoides | 38 (39.6%) | 34 (35.4%) | 72 (75.0%) | |
| Hookworms (Ancylostoma duodenale and Necator americanus) | 13 (13.5%) | 7 (7.3%) | 20 (20.8%) | |
| Trichuris trichiura | 0 (0%) | 0 (0%) | 0 (0%) | |
| Mixed infections (Ascaris lumbricoides + Hookworms) | 0 (0%) | 4 (4.2%) | 4 (4.2%) | |
| Plasmodium falciparum parasitaemia | 28 (11.7%) | 27 (11.3%) | 55 (22.9%) | 0.362 |
| Low | 42 (47.7%) | 34 (38.6%) | 76 (86.4%) | |
| Moderate | 3 (3.4%) | 5 (5.7%) | 8 (9.1%) | |
| Severe | 4 (4.5%) | 0 (0.0%) | 4 (4.5%) | |
| Co-infections | 21 (8.8%) | 12 (5.0%) | 33 (13.8%) | 0.479 |
| Ascaris lumbricoides + Plasmodium falciparum | 15 (42.3%) | 11 (36.5%) | 26 (78.8%) | |
| Hookworms + Plasmodium falciparum | 6 (14.3%) | 1 (6.9%) | 7 (21.2%) |
Low (1–10 parasites per 100 thick film fields), Moderate (11–100 parasites per 100 thick film fields), Severe (1–10 parasites per each thick film field)
Prevalent soil-borne helminths
The overall prevalence of soil-borne helminths was 63 (26.3%). Among those harbouring helminths, 33 (13.8%) were co-infected with Plasmodium falciparum. The most prevalent soil-borne helminths observed was Ascaris lumbricoides, 72 (75.0%) followed by hookworms, 20 (20.8%). Mixed infection were only of Ascaris lumbricoides and hookworms with a prevalence 4 (4.2%). No Trichuris trichiura infections were observed in the study population. Among the helminths co-infections, Ascaris lumbricoides had the highest prevalence 26 (78.8%) as compared to hookworms 7 (21.2%). No significant differences were observed in soil-borne helminths across sex (P > 0.05, Table 1).
Cytokine expression in Plasmodium falciparum malaria and soil-borne helminths
In order to identify cytokines that are associated with either Plasmodium falciparum malaria or soil borne helminth infections, cytokines from each group of patients were compared with health controls. The results showed that cytokine levels significantly differed across groups for IFN-γ (P = 0.023, Fig. 1a), IL-10 (P = 0.008, Fig. 1b) and TGF-β (P = 0.0001, Fig. 1c). No Significant differences were observed for TNF-α (P = 0.368, Fig. 1d) and IL-6 (P = 0.329, Fig. 1e).
Fig. 1.
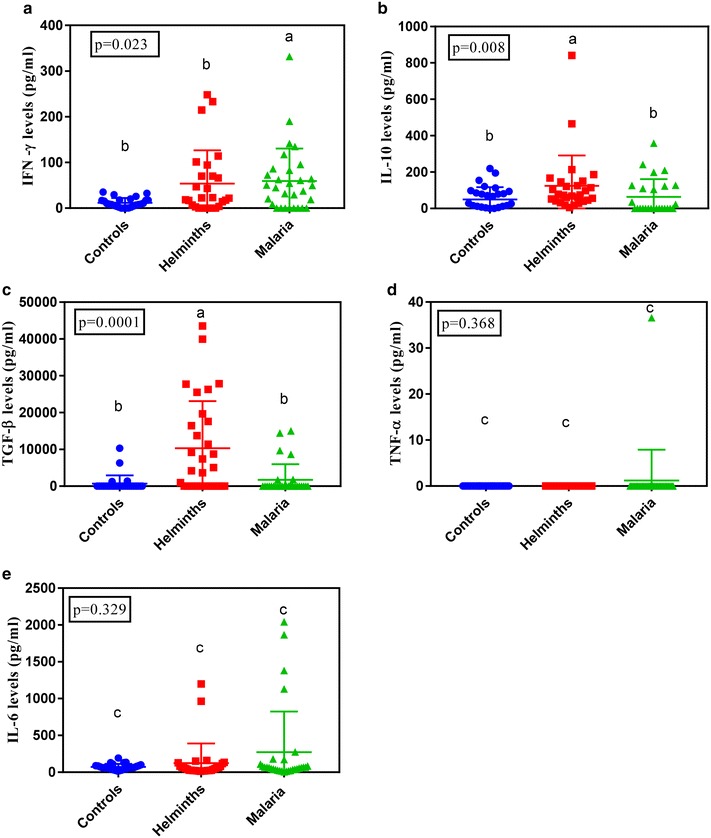
Plasma cytokine profiles in Plasmodium falciparum malaria cases, soil borne helminths and normal controls for IFN-γ (a), IL-10 (b), TGF-β (c), TNF-α (d) and IL-6 (e). Graphs show median level with interquartile range. Letters above the bars indicate significant difference between the groups (Dunn’s post-test, P ≤ 0.05)
When median plasma IFN-γ, IL-10 and TGF-β levels were compared across groups, the results showed that Plasmodium falciparum malaria infected individual expressed significantly higher (P < 0.05) levels of IFN-γ (47.7 pg/ml) as compared to health controls (8.8 pg/ml) and soil borne helminths infected individuals (22.8 pg/ml, Fig. 1a). When IL-10 levels were similarly compared soil borne helminths infected individuals expressed higher levels of IL-10 (73.86 pg/ml) as compared to Plasmodium falciparum malaria (33.64 pg/ml) and healthy individuals (26.09 pg/ml, Fig. 1b). When median plasma cytokine levels of TGF-β were compared across groups, the results showed that soil borne helminths infected individuals showed higher levels (P < 0.05) of TGF-β (2338 pg/ml) as compared to Plasmodium falciparum malaria infected individuals (772 pg/ml) and healthy controls (424.6 pg/ml, Fig. 1c). No significant differences across groups were noted for TNF-α and IL-6 cytokines levels (Fig. 1d, e respectively).
Cytokine expression in Plasmodium falciparum malaria and soil-borne helminths co-infection
In order to find the effect of harbouring both soil-borne helminths and Plasmodium falciparum malaria concurrently, cytokine levels for co-infected individuals were compared with those with either Plasmodium falciparum malaria or soil-borne helminths alone. Results showed that cytokine levels significantly differed across groups for IL-10 (P = 0.004, Fig. 2a), IL-6 (P = 0.011, Fig. 2b) and TGF-β (P = 0.003, Fig. 2c). No Significant differences were observed for IFN-γ (P = 0.347, Fig. 2d) and TNF-α (P = 0.167, Fig. 2e).
Fig. 2.
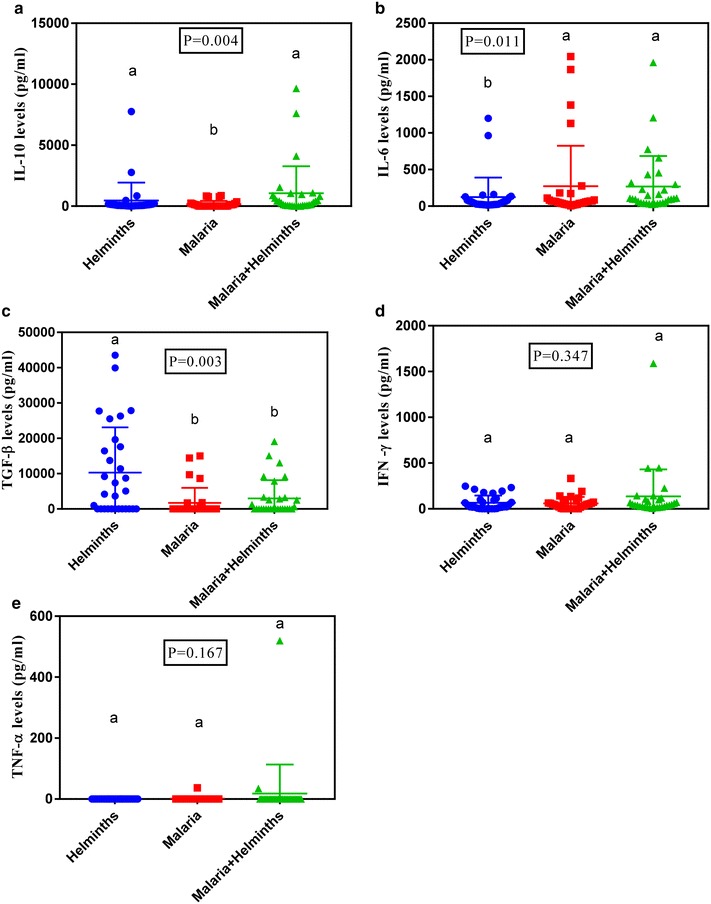
Plasma cytokine profiles in Plasmodium falciparum malaria cases, soil borne helminths and co-infections for IL-10 (a), IL-6 (b), TGF-β (c), IFN-γ (d) and TNF-α (e). Graphs show median level with interquartile range. Letters above the bars indicate significant difference between the groups (Dunn’s post-test, P ≤ 0.05)
When median plasma cytokine levels were compared across groups, the results showed that co-infected individuals expressed significantly (P < 0.05) higher levels of IL-10 (304 pg/ml) as compared to Plasmodium falciparum malaria infected individuals (11.57 pg/ml) and soil borne helminths infected individuals (77.01 pg/ml, Fig. 2a). When median plasma cytokine levels of IL-6 were compared across groups, the results showed that co-infected individuals showed higher (P < 0.05) levels of IL-6 (100.9 pg/ml) as compared to Plasmodium falciparum malaria infected individuals (63.7 pg/ml) and soil borne helminths infected individuals (45.37 pg/ml, Fig. 2b). Similarly, when TGF-β levels were similarly compared soil borne helminths infected individuals expressed higher (P < 0.05) levels of TGF-β (2338 pg/ml) as compared to Plasmodium falciparum malaria (772.7 pg/ml) and co-infected individuals (939.2 pg/ml, Fig. 2c). No significant differences across groups were noted for IFN-γ and TNF-α cytokines levels (Fig. 2d, e respectively).
Discussion
The over prevalence of soil borne helminth was (26.3%). This is in range with what has been reported previously in Uganda [39], Tanzania [40] and Ethiopia [4]. Prevalence studies of soil borne helminths since 2009 have indicated that of Ascaris lumbricoides, and the hookworm species are common infections in Bushenyi district among the soil borne helminths [39]. This is in agreement with our finding were Ascaris lumbricoides had the highest prevalence (75.0%) followed by hook worms (20.8%). In this study no Trichuris trichiura infections were detected, similarly to what was observed by Agwu et al. [39] in Bushenyi district. In this study, the Plasmodium falciparum malaria prevalence was (22.9%) lower than that reported in previous studies in Uganda 27% [2]. This could probably be because of the difference in the sample size. However, our findings compare well with the earlier report from southwest Uganda [19] that reported a prevalence of 23%. Results from this study are in range with a previous study by Shapiro et al. [19] who reported a prevalence of 15% among malaria helminth co-infected individuals in Uganda, 14% was reported in Zambia [35, 41] and 13% was reported in Kenya (Rutagwera et al. [6]). However this is not in range with a similar study done in Tanzania where they reported a prevalence among malaria helminth co-infected to be 26% [6]. Among the helminths co-infections, Ascaris lumbricoides had the highest prevalence (78.8%) and results from this study are in range with other studies done elsewhere in Madagascar which reported that among the helminths co-infections, Ascaris lumbricoides had the highest prevalence of 77% [14]. In our study, Plasmodium falciparum malaria infected individual expressed significantly higher levels of IFN-γ (47.7 pg/ml) as compared to health controls (8.8 pg/ml) and soil borne helminths infected individuals (22.8 pg/ml). This is in agreement with a study done in south East Asia and elsewhere which reported that Plasmodium falciparum malaria expressed higher IFN-γ levels (Doolan et al. [27]; Luty et al. [42]). These higher levels of IFN-γ have been associated with protective role of the cytokine against P. falciparum malaria [27, 35]. This effect has been attributed to the monocyte-macrophage activating capacity of IFN-γ, with rapid killing of the malarial blood-stage parasites by reactive oxygen and nitrogen intermediates [43, 44]. Also animal models of malaria have been associated with increased production of IFN-γ which has been associated with a favourable outcome of the disease [26]. Soil borne helminths infected individuals expressed higher levels of IL-10 (73.86 pg/ml) as compared to Plasmodium falciparum malaria (33.64 pg/ml) and healthy individuals (26.09 pg/ml). This is probably because IL-10 is a key anti-inflammatory cytokine protective against helminth infections that cause inflammation [45]. Also soil borne helminths infected individuals expressed the highest levels of TGF-β (2338 pg/ml) as compared to Plasmodium falciparum malaria infected individuals (772 pg/ml) and healthy controls (424.6 pg/ml). This is probably because TGF-β has been attributed to wound healing of the intestinal mucosa during tissue repair caused by helminths in the gut [32, 46]. TNF-α and IL-6 levels showed no significant difference across groups and this is in agreement with previous studies done by Franca and colleagues that reported that TNF-α and IL-6 cytokines are not associated with Plasmodium falciparum malaria and soil borne helminths infected individuals [47]. This is probably because the TNF-α is a key cytokine in cerebral malaria [48] and probably the patients we examined that time none had cerebral malaria. Also the higher levels of IL-10 and TGF-β expressed in soil borne helminths infected individuals could have down regulated the production of TNF-α levels [30, 49]. Lack of significant difference across groups in IL-6 could probably be because the IL-6 is not involved in modulation of the disease both in Plasmodium falciparum malaria infected individuals and soil borne helminths infected individuals. Co-infected individuals expressed significantly higher levels of IL-10 (304 pg/ml) as compared to Plasmodium falciparum malaria infected individuals (11.57 pg/ml) and soil borne helminths infected individuals (77.01 pg/ml). Results from this study are in agreement with a previous study by Hartgers who reported high expression of IL-10 in co-infected individuals [50]. Up regulation of IL-10 in co-infections is probably indicative that co-infected individuals don’t lose the protective role of the IL-10 against soil borne helminths during infection. This is in agreement with the role of gut helminth in modulation of TH2 cytokine like responses that lead to worm expulsion [51, 52]. Co-infected individuals expressed higher levels of IL-6 (100.9 pg/ml) as compared to Plasmodium falciparum malaria infected individuals (63.7 pg/ml) and soil borne helminths infected individuals (45.37 pg/ml). This is because IL-6 has been shown to possess both pro and anti-inflammatory features [53, 54]. Soil borne helminths infected individuals expressed higher levels of TGF-β (2338 pg/ml) as compared to Plasmodium falciparum malaria (772.7 pg/ml) and co-infected individuals (939.2 pg/ml).This down regulation of TGF-β in co-infections is indicative that co-infected individuals lose the protective role of TGF-β against soil borne helminths during infection. IFN-γ and TNF-α levels showed no significance across groups. This is probably because the higher levels of IL-10 in co-infections and soil borne helminths down regulates IFN-γ by supressing T cells from producing IFN-γ hence the decrease [24, 44]. Also TGF-β may down regulates production of TNF-α in soil borne helminths [33]. And lastly TNF-α is probably not involved in modulation of malaria, soil borne helminth and co-infections of both diseases.
Conclusion
In conclusion, our study demonstrates an up-regulation of IFN-γ during Plasmodium falciparum malaria and an up-regulation of IL-10 and TGF-β during soil borne helminth infections. We further show an up-regulation of IL-10 and IL-6 during co-infections of Plasmodium falciparum and soil borne helminth infections and a down-regulation of TGF-β during co-infections of Plasmodium falciparum and soil borne helminth infections. However, how these cytokines may influence the clinical outcome of the diseases involved calls for further investigations.
Authors’ contributions
BR coordinated the study and participated in its design, CDK performed the statistical analysis and WJ contributed in the research design. MDC helped in writing. All authors read and approved the final manuscript.
Acknowledgements
The laboratory analysis was carried out in the Immunology and Molecular Biology laboratory at the College of Veterinary Medicine, Animal Resources and Biosecurity (COVAB), Makerere University. I sincerely acknowledge the advice, guidance and assistance I received from Ms. Ann Kitibwa.
Competing interests
The authors declare that they are no competing interests.
Availability of data and materials
The data sets used and/or analysed during the current study are fully available from the corresponding author on reasonable request.
Consent for publication
Not applicable.
Ethics approval and consent to participate
Ethical approval was sought from the Institutional Review Board (IRB) at Mbarara University of Science and Technology (Reference Number: MUREC1/7). Final research approval was provided by the Ethical Committee on Human research under the National Council for Science and Technology. In all cases, patients recruited in the study were provided with written and verbal information about the project objectives so as to guide informed consent. For children, approval was sought from the parents or legal guardian, and were possible children were also asked to assent.
Funding
The study did not have any external funding. Costs regarding laboratory tests were paid for by internal investigator funds (Kampala International University, Western Campus).
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Abbreviations
- µl
micro litre
- H2SO4
hydrogen Sulphuric Acid
- HCL
hydrochloric acid
- IFN
interferon
- Ig
immuno globulin
- IL
interleukin
- KIU-TH
Kampala International University Teaching Hospital
- NAOH
sodium hydroxide
- nm
nano meter
- OD
optical density
- P
Plasmodium
- PBS
phosphate buffered saline
- RT
room temperature
- SBH
soil-borne helminths
- TGF-β
transforming growth factor Beta
- Th
T helper
- TNF-α
tumor necrosis factor alpha
Contributor Information
Richard Bwanika, Email: bwanikarichardatkiu@gmail.com.
Charles D. Kato, Email: katodrago@yahoo.com
Johnson Welishe, Email: johnwelishe@yahoo.com.
Daniel C. Mwandah, Email: danielchanskiu@gmail.com
References
- 1.World Health Organization (WHO 2014) World malaria report 2013. Geneva: World Health Organization; 2014. [Google Scholar]
- 2.World Health Organization (WHO 2013) The World malaria report 2013. Geneva: World Health Organization; 2013. [Google Scholar]
- 3.Hay SI, Okiro EA, Gething PW, Patil AP, Tatem AJ, Guerra CA. Estimating the global clinical burden of Plasmodium falciparum malaria in 2007. PLoS Med. 2010;7:750. doi: 10.1371/journal.pmed.1000290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Petney TN, Andrews RH. Multi parasite communities in animals and humans: frequency, structure and pathogenic significance. Int J Parasitol. 1998;28:377–393. doi: 10.1016/S0020-7519(97)00189-6. [DOI] [PubMed] [Google Scholar]
- 5.Kinung’hi SM, Magnussen P, Kaatano G, Kishamawe C, Vennervald BJ. Malaria and helminth co-infections in school and preschool children: a cross-sectional study in Magu district, north-western Tanzania. PLoS ONE. 2014;5:236–285. doi: 10.1371/journal.pone.0086510. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Rutagwera DG, Tylleskär T. Co-infection with malaria, hookworm and schistosomiasis among school children in Zambezi: a school-based rapid survey. Med J Zambia. 2014;39:18–23. [Google Scholar]
- 7.Pullan RL, Smith JL, Jasrasaria R, Brooker SJ. Global numbers of infection and disease burden of soil transmitted helminth infections in 2010. Parasites Vectors. 2014;7:37. doi: 10.1186/1756-3305-7-37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Bundy D, Medley G. Immuno-epidemiology of human geo helminthiasis: ecological and immunological determinants of worm burden. Parasitology. 1992;104:S105–S119. doi: 10.1017/S0031182000075284. [DOI] [PubMed] [Google Scholar]
- 9.Nacher M, Gay F, Singhasivanon P, Krudsood S, Treeprasertsuk S, Mazier D. Ascaris lumbricoides infection is associated with protection from cerebral malaria. Parasite Immunol. 2000;22:107–113. doi: 10.1046/j.1365-3024.2000.00284.x. [DOI] [PubMed] [Google Scholar]
- 10.Spiegel A, Tall A, Raphenon G, Trape JF, Druilhe P. Increased frequency of malaria attacks in subjects co-infected by intestinal worms and Plasmodium falciparum malaria. Trans R Soc Trop Med Hyg. 2003;97:198–199. doi: 10.1016/S0035-9203(03)90117-9. [DOI] [PubMed] [Google Scholar]
- 11.Degarege A, Legesse M, Medhin G, Animut A, Erko B. Malaria and related outcomes in patients with intestinal helminths: a cross-sectional study. BMC Infect Dis. 2012;12:291. doi: 10.1186/1471-2334-12-291. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Nacher M, Singhasivanon P, Yimsamran S, Manibunyong W, Thanyavanich N, Wuthisen P. Intestinal helminth infections are associated with increased incidence of Plasmodium falciparum malaria in Thailand. J Parasitol. 2002;88:55–58. doi: 10.1645/0022-3395(2002)088[0055:IHIAAW]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 13.Nkuo-Akenji TK, Chi PC, Cho JF, Ndamukong KK, Sumbele I. Malaria and helminth co-infection in children living in a malaria endemic setting of mount Cameroon and predictors of anemia. J Parasitol. 2006;92:1191–1195. doi: 10.1645/GE-895R.1. [DOI] [PubMed] [Google Scholar]
- 14.Brutus L, Watier L, Hanitrasoamampionona V, Razanatsoarilala H, Cot M. Confirmation of the protective effect of Ascaris lumbricoides on Plasmodium falciparum infection: results of a randomized trial in Madagascar. Am J Trop Med Hyg. 2007;77(6):1091–1095. [PubMed] [Google Scholar]
- 15.Sangweme DT, Midzi N, Zinyowera-Mutapuri S, Mduluza T, Diener-West M, Kumar N. Impact of schistosome infection on Plasmodium falciparum malariometric indices and immune correlates in school age children in Burma Valley, Zimbabwe. Med J Zambia. 2010;2:369–389. doi: 10.1371/journal.pntd.0000882. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Degarege A, Animut A, Legesse M, Erko B. Malaria and helminth co-infections in outpatients of Alaba Kulito Health Center, southern Ethiopia: a cross sectional study. BMC Res Notes. 2010;3:143. doi: 10.1186/1756-0500-3-143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Yatich NJ, Jolly PE, Funkhouser E, Agbenyega T, Rayner JC, Ehiri JE. The effect of malaria and intestinal helminth coinfection on birth outcomes in Kumasi, Ghana. Am J Trop Med Hyg. 2010;82:28–34. doi: 10.4269/ajtmh.2010.09-0165. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Abanyie FA, McCracken C, Kirwan P, Molloy SF, Asaolu SO, Holland CV. Ascaris co-infection does not alter malaria-induced anaemia in a cohort of Nigerian preschool children. Malar J. 2013;12(1):1. doi: 10.1186/1475-2875-12-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Shapiro AE, Tukahebwa EM, Kasten J, Clarke SE, Magnussen P, Olsen A. Epidemiology of helminth infections and their relationship to clinical malaria in southwest Uganda. Trans R Soc Trop Med Hyg. 2005;99:18–24. doi: 10.1016/j.trstmh.2004.02.006. [DOI] [PubMed] [Google Scholar]
- 20.Lyke KE, Dicko A, Dabo A, Sangare L, Kone A, Coulibaly D. Association of Schistosoma haematobium infection with protection against acute Plasmodium falciparum malaria in Malian children. Am J Trop Med Hyg. 2005;73:1124–1130. [PMC free article] [PubMed] [Google Scholar]
- 21.Lemaitre M, Watier L, Briand V, Garcia A, Le Hesran JY, Cot M. Coinfection with Plasmodium falciparum and Schistosoma haematobium: additional evidence of the protective effect of Schistosomiasis on malaria in Senegalese children. Am J Trop Med Hyg. 2014;90:329–334. doi: 10.4269/ajtmh.12-0431. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Nacher M, Singhasivanon P, Silachamroon U, Treeprasertsuk S, Vannaphan S, Traore B. Helminth infections are associated with protection from malaria-related acute renal failure and jaundice in Thailand. Am J Trop Med Hyg. 2001;65:834–836. doi: 10.4269/ajtmh.2001.65.834. [DOI] [PubMed] [Google Scholar]
- 23.Dolo H, Coulibaly YI, Dembele B, Konate S, Coulibaly SY, Doumbia SS. Filariasis attenuates anaemia and pro inflammatory responses associated with clinical malaria: a matched prospective study in children and young adults. PLoS Negl Trop Dis. 2012;6:e1890. doi: 10.1371/journal.pntd.0001890. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Righetti AA, Glinz D, Adiossan LG, Koua AYG, Niamké S, Hurrell RF. Interactions and potential implications of Plasmodium falciparum-hookworm co infection in different age groups in south-central Côte d’Ivoire. Parasites Vectors. 2012;12:52. doi: 10.1371/journal.pntd.0001889. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Artavanis-Tsakonas K, Tongren J, Riley E. The war between the malaria parasite and the immune system: immunity, immuno regulation and immunopathology. Clin Exp Immunol. 2003;133:145–152. doi: 10.1046/j.1365-2249.2003.02174.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Riley E, Wahl S, Perkins D, Schofield L. Regulating immunity to malaria. Parasite Immunol. 2006;28:35–49. doi: 10.1111/j.1365-3024.2006.00775.x. [DOI] [PubMed] [Google Scholar]
- 27.Doolan DL, Dobaño C, Baird JK. Acquired immunity to malaria. Clin Microbiol Rev. 2009;22:13–36. doi: 10.1128/CMR.00025-08. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Su Z, Segura M, Morgan K, Loredo-Osti JC, Stevenson MM. Impairment of protective immunity to blood-stage malaria by concurrent nematode infection. Infect Immun. 2005;73:3531–3539. doi: 10.1128/IAI.73.6.3531-3539.2005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Day NP, Hien TT, Schollaardt T, Loc PP, Chuong LV, Chau TT, Mai NT, Phu NH, Sinh DX, White NJ, Ho M. The prognostic and pathophysiologic role of pro- and anti-inflammatory cytokines in severe malaria. J Infect Dis. 1999;180:1288–1297. doi: 10.1086/315016. [DOI] [PubMed] [Google Scholar]
- 30.Figueiredo CA, Barreto ML, Rodrigues LC, Cooper PJ, Silva NB, Amorim LD. Chronic intestinal helminth infections are associated with immune hyporesponsiveness and induction of a regulatory network. Infect Immun. 2010;78:3160–3167. doi: 10.1128/IAI.01228-09. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Turner JD, Faulkner H, Kamgno J, Cormont F, Van Snick J, Else KJ. Th2 cytokines are associated with reduced worm burdens in a human intestinal helminth infection. J Infect Dis. 2003;188:1768–1775. doi: 10.1086/379370. [DOI] [PubMed] [Google Scholar]
- 32.Turner JD, Jackson JA, Faulkner H, Behnke J, Else KJ, Kamgno J. Intensity of intestinal infection with multiple worm species is related to regulatory cytokine output and immune hyporesponsiveness. J Infect Dis. 2008;197:1204–1212. doi: 10.1086/586717. [DOI] [PubMed] [Google Scholar]
- 33.Wammes LJ, Hamid F, Wiria AE, De Gier B, Sartono E, Maizels RM. Regulatory T cells in human geohelminth infection suppress immune responses to BCG and Plasmodium falciparum. Eur J Immunol. 2010;40:437–442. doi: 10.1002/eji.200939699. [DOI] [PubMed] [Google Scholar]
- 34.Allen JE, Maizels RM. Diversity and dialogue in immunity to helminths. Nat Rev Immunol. 2011;11:375–388. doi: 10.1038/nri2992. [DOI] [PubMed] [Google Scholar]
- 35.Cheesebrough M. Medical laboratory manual for tropical countries. Cambridge: Tropical Health Technology Publications and Butterworth-Heinemann; 2002. [Google Scholar]
- 36.Sánchez-Arcila JC, Perce-da-Silva DD, Vasconcelos MP, Rodrigues-da-Silva RN, Pereira VA, Aprígio CJ. Intestinal parasites coinfection does not alter plasma cytokines profile elicited in acute malaria in subjects from endemic area of Brazil. Mediat Inflamm. 2014;20:14. doi: 10.1155/2014/857245. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.World Health Organization . Bench aids for the diagnosis of intestinal parasites. Geneva: World Health Organisation; 1994. [Google Scholar]
- 38.Kato CD, Alibu VP, Nanteza A, Mugasa CM, Matovu E. Interleukin (IL)-6 and IL-10 are up regulated in late stage Trypanosoma brucei rhodesiense sleeping sickness. PLoS Negl Trop Dis. 2015;10:e0118370. doi: 10.1371/journal.pntd.0003835. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Agwu E, Tanayen G, Moazzam ML. Four-year health-point surveillance of human gastro-intestinal parasites among patients attending a clinic in Bushenyi, Uganda. Spec Parasites Pathog J SPPJ. 2015;1(1):0001–0006. [Google Scholar]
- 40.Mulu A, Legesse M, Erko B, Belyhun Y, Nugussie D, Shimelis T. Epidemiological and clinical correlates of malaria-helminth co-infections in Southern Ethiopia. Malar J. 2013;12:227. doi: 10.1186/1475-2875-12-227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Florey LS, King CH, Van Dyke MK, Muchiri EM, Mungai PL, Zimmerman PA. Partnering parasites: evidence of synergism between heavy Schistosoma haematobium and Plasmodium species infections in Kenyan children. PLoS Negl Trop Dis. 2012;6:e1723. doi: 10.1371/journal.pntd.0001723. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Luty AJ, Lell B, Schmidt-Ott R, Lehman LG, Luckner D, Greve B, Matousek P, Herbich K, Schmid D, Migot-Nabias F, Deloron P, Nussenzweig RS, Kremsner PG. Interferon-gamma responses are associated with resistance to reinfection with Plasmodium falciparum in young African children. J Infect Dis. 1999;179:980–988. doi: 10.1086/314689. [DOI] [PubMed] [Google Scholar]
- 43.Taylor-Robinson AW, Looker M. Sensitivity of malaria parasites to nitric oxide at low oxygen tensions. Lancet. 2013;351:1630. doi: 10.1016/S0140-6736(05)77685-6. [DOI] [PubMed] [Google Scholar]
- 44.Winkler S, Willheim M, Baier K, Schmid D, Aichelburg A, Graninger W, Kremsner PG. Reciprocal regulation of Th1- and Th2-cytokine-producing T cells during clearance of parasitemia in Plasmodium falciparum malaria. Infect Immun. 1998;66:6040–6044. doi: 10.1128/iai.66.12.6040-6044.1998. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.O’Garra A, Vieira P. Regulatory T cells and mechanisms of immune System control. Nat Med. 2004;10:801–805. doi: 10.1038/nm0804-801. [DOI] [PubMed] [Google Scholar]
- 46.Kulkarni AB, Letterio T, Thyagarajan JJ. Functions of cytokines within the TGF-beta superfamily as determined from transgenic and gene knock out studies in mice. Curr Mol Med. 2002;2:303–327. doi: 10.2174/1566524024605699. [DOI] [PubMed] [Google Scholar]
- 47.Hartgers FC, Obeng BB, Kruize YC, Dijkhuis A, McCall M, Sauerwein RW, Luty AJ, Boakye DA, Yazdanbakhsh M. Responses to malarial antigens are altered in helminth-infected children. J Infect Dis. 2009;78:760–769. doi: 10.1086/598687. [DOI] [PubMed] [Google Scholar]
- 48.Clark IA, Rockett KA. The cytokine theory of human cerebral malaria. Parasitol Today. 1994;10:410–412. doi: 10.1016/0169-4758(94)90237-2. [DOI] [PubMed] [Google Scholar]
- 49.Ho M, Sexton MM, Tongtawe P, Looareesuwan S, Suntharasamai P, Webster HK. Endogenous interleukin-10 modulates proinflammatory response in Plasmodium falciparum malaria. J Infect Dis. 1998;172:838–844. doi: 10.1093/infdis/172.3.838. [DOI] [Google Scholar]
- 50.Hartgers FC, Yazdanbakhsh M. Co-infection of helminths and malaria: modulation of the immune responses to malaria. Parasite Immunol. 2006;10:497–506. doi: 10.1111/j.1365-3024.2006.00901.x. [DOI] [PubMed] [Google Scholar]
- 51.Cliffe LJ, Humphreys NE, Lane TE, Potten CS, Booth C, Grencis RK. Accelerated intestinal epithelial cell turnover: a new mechanism of parasite expulsion. Science. 2005;308:1463–1465. doi: 10.1126/science.1108661. [DOI] [PubMed] [Google Scholar]
- 52.McDermott JR, Bartram RE, Knight PA, Miller HR, Garrod DR, Grencis RK. Mast cells disrupt epithelial barrier function during enteric nematode infection. Proc Natl Acad Sci USA. 2003;100:7761–7766. doi: 10.1073/pnas.1231488100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Penkowa, Polderman AM, Schulz-Key H, Soboslay PT. Prenatal immune priming with helminth infections: parasite-specific cellular reactivity and Th1 and Th2 cytokine responses in neonates. Trans R Soc Trop Med Hyg. 2003;55:732–739. doi: 10.1034/j.1398-9995.2000.00477.x. [DOI] [PubMed] [Google Scholar]
- 54.S Rose-John, Tall A, Raphenon G, Trape JF, Druilhe P. Increased frequency of malaria attacks in subjects co-infected by intestinal worms and Plasmodium falciparum malaria. Trans R Soc Trop Med Hyg. 2012;97:198–199. doi: 10.1016/s0035-9203(03)90117-9. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data sets used and/or analysed during the current study are fully available from the corresponding author on reasonable request.