

Abstract
Background:
Females are at an increased risk of sustaining noncontact knee ligament injuries as compared with their male counterparts. The kinetics that load the anterior cruciate ligament (ACL) are still under dispute in the literature.
Purpose/Hypothesis:
The purpose of this study was to determine whether there are differences in knee kinetics between the sexes that lead to greater ACL strain in females when similar external loads are applied during a simulated drop vertical jump landing task. It was hypothesized that female limbs would demonstrate significant differences in knee abduction moment that predispose females to ACL injury when compared with males.
Study Design:
Controlled laboratory study.
Methods:
Motion analysis data of 67 athletes who performed a drop vertical jump were collected. The kinematic and kinetic data were used to categorize tertiles of relative risk, and these values were input into a cadaveric impact simulator to assess ligamentous loads during the simulated landing task. Uni- and multiaxial load cells and differential variable reluctance transducer strain sensors were utilized to collect kinetic data and maximum ACL strain for analysis. Conditions of external loads applied to the cadaveric limbs were systematically varied and randomized. Data were analyzed with 2-way repeated-measures analysis of variance and the Fisher exact test.
Results:
Five kinetic parameters were evaluated. Of the 5 kinetic variables, only knee abduction moment (KAM) demonstrated significant differences in females as compared with males (F 1,136 = 4.398, P = .038). When normalized to height and weight, this difference between males and females increased in significance (F 1,136 = 7.155, P = .008). Compared with males, females exhibited a 10.3-N·m increased knee abduction torque at 66 milliseconds postimpact and a 22.3-N·m increased abduction torque at 100 milliseconds postimpact. For loading condition, the condition of “maximum ACL strain” demonstrated a maximum difference of 54.3-N·m increased abduction torque and 74.5-N·m increased abduction torque at 66 milliseconds postimpact.
Conclusion:
Under the tested conditions, increased external loads led to increased medial knee translation force, knee abduction moment, and external knee moment. Females exhibited greater forces and moments at the knee, especially at KAM, when loaded in similar conditions. As these KAM loads are associated with increased load and strain on the ACL, the sex-based differences observed in the present study may account for a portion of the underlying mechanics that predispose females to ACL injury as compared with males in a controlled simulated athletic task.
Clinical Relevance:
KAM increases strain to the ACL under clinically representative loading. Additionally, this work establishes the biomechanical characteristics of knee loading between sexes.
Keywords: anterior cruciate ligament (ACL), kinetics, injury, cadaveric, simulation, dynamic knee valgus
Anterior cruciate ligament (ACL) injuries are common knee-related injuries, with worldwide annual estimates of >2 million.32 The majority of ACL injuries occur with participation in sports that include cutting, pivoting, and landing.30 Participation in sports and incidence of sport injuries have increased among females, and exercise-related musculoskeletal injuries are more prevalent in females than in males.22,40 In addition, females have a 4- to 6-fold increased risk of ACL injury when compared with their male counterparts.1,12,25,30,35 In the United States, annual estimates of surgery and rehabilitation costs associated with female ACL injuries total $646 million.17,20 These factors result in a near-epidemic health issue for female athletes.19
Injury of the ACL is generally noncontact in nature, with estimates of a noncontact mechanism of injury near 75%.10,27,28,35 These findings indicate that ACL injuries are likely influenced by faulty biomechanical factors and poor neuromuscular control, which can be addressed with preventive biomechanical and neuromuscular strategies. To optimize preventive programs and lower the individual and societal burden of these injuries, especially for females, it is essential to establish the underlying mechanics that contribute to excessive loads that lead to ligament failure.3,11 The specific mechanisms that preload the ACL for injury are still under dispute, and the mechanisms may be different between sexes.30,42 Previous work has demonstrated that sex differences exist for proximal control of the knee joint, kinematics, stiffness, and recruitment strategies.23,26,41 However, insufficient cadaveric work has been performed to analyze (1) the kinetics that occur at the knee during landings that induce maximum ACL strain and ACL ruptures and (2) the sex differences in these variables. These studies are necessary to understand the forces and moments at the knee that lead to increased load on the ACL. Improved knowledge of the kinetics at the knee will allow for improved prevention strategies. Prevention is essential for reduction of the health burden associated with ACL injury and its debilitating sequelae,6 which include lower activity levels, contralateral ACL injury, and early-onset osteoarthritis.36 This information will enhance injury prevention, rehabilitation, and return-to-sport criteria37 and provide the framework for individualized medicine.
This study was designed to determine whether there are differences in knee kinetics between the sexes when similar external loads are applied that lead to greater ACL strain in females during landing deceleration movements. It was hypothesized that female limbs would demonstrate significant differences in knee forces and moments, especially with frontal plane knee abduction, that predispose females to ACL injury as compared with males.
Methods
Lower extremity cadaveric specimens (n = 45) were obtained (Anatomy Gifts Registry) according to predetermined inclusion criteria: age 18 to ≤50 years, no evidence of significant trauma or surgery to lower extremity, no extensive bed rest (defined as >1 month), and no evidence of extended chemotherapy (defined as >4 weeks). Specimens were not acquired if they had systemic infection, if they had a cartilaginous disease (other than typical of regular aging), and if cause of death would have induced significant trauma to the lower extremity. Specimens were dissected and prepared according to specifications outlined in a recent methodology study.4 Of the 45 available specimens (22 male, 23 female), 6 were excluded from final analysis owing to poor data quality from equipment failure (eg, nonbiomechanical damage to ACL from sensor), mechanical weakness attributed to specimen preparation (eg, tibial fixture screw cause of tibial fracture), or a pre-evaluation nonfunctional ACL determined by a board-certified orthopaedic surgeon (A.J.K.). Data analyses were therefore performed on 39 specimens (mean ± SD: age, 41.5 ± 8.4 years; mass, 85.7 ± 25.6 kg; 19 male, 20 female).
In Vivo Input Data for Physiologic Impact
Volunteers consented to participate in this study according to guidelines of the institutional review board of Mayo Clinic. Three-dimensional motion analysis (Raptor 12; Motion Analysis Corp) of the drop vertical jump (DVJ) task was performed with 67 healthy athletic participants. Kinematic and kinetic variables were calculated with inverse dynamics and customized software (MATLAB, v 2016a [The MathWorks Inc]; Visual3D, v 6 [C-Motion Inc]) to determine tertiles of injury risk (low, medium, high) in 3 degrees of knee dynamics: knee abduction moment (KAM), anterior tibial shear (ATS), and internal tibial rotation (ITR). These calculated forces and moments were utilized across the tertiles of risk in a randomized order as inputs into the applied external loads for impact testing (Table 1).4
TABLE 1.
Load Magnitudes Based on In Vivo Population Percentagea
| Percentage | KAM, N·m | ITR, N·m | ATS, N |
|---|---|---|---|
| 0 | 1.7 | 1.0 | 47 |
| 33 | 13.5 | 9.7 | 64 |
| 67 | 26.8 | 18.6 | 80 |
| 100 | 57.3 | 53.7 | 196 |
aATS, anterior tibial shear; ITR, internal tibial rotation; KAM, knee abduction moment.
Cadaveric Impactor
A custom-designed cadaveric impactor was utilized to simulate DVJs in the lower extremities of athletes (Figure 1).4 Pneumatic cylinders applied the designated knee forces/moments calculated from the in vivo participants and applied muscular forces to the quadriceps and hamstring tendons at a 1:1 ratio. The designated forces and torques were applied to the tibia prior to the release of a gravity-driven drop sled of 0.5 body weight (34 kg) from a height of 31 cm. Single- and 6-axis load cells recorded the vertical ground reaction force (vGRF) and forces and moments at the knee, respectively. The data of the 6-axis load cell were transformed to record forces and moments at the knee joint center. In addition, two 3-mm differential variable reluctance transducers (LORD MicroStrain Inc) were implanted into the midsubstance of the medial collateral ligament across the joint line and the distal third of the anteromedial bundle of the ACL, respectively, to measure ligament strain during simulation.5,24,31
Figure 1.
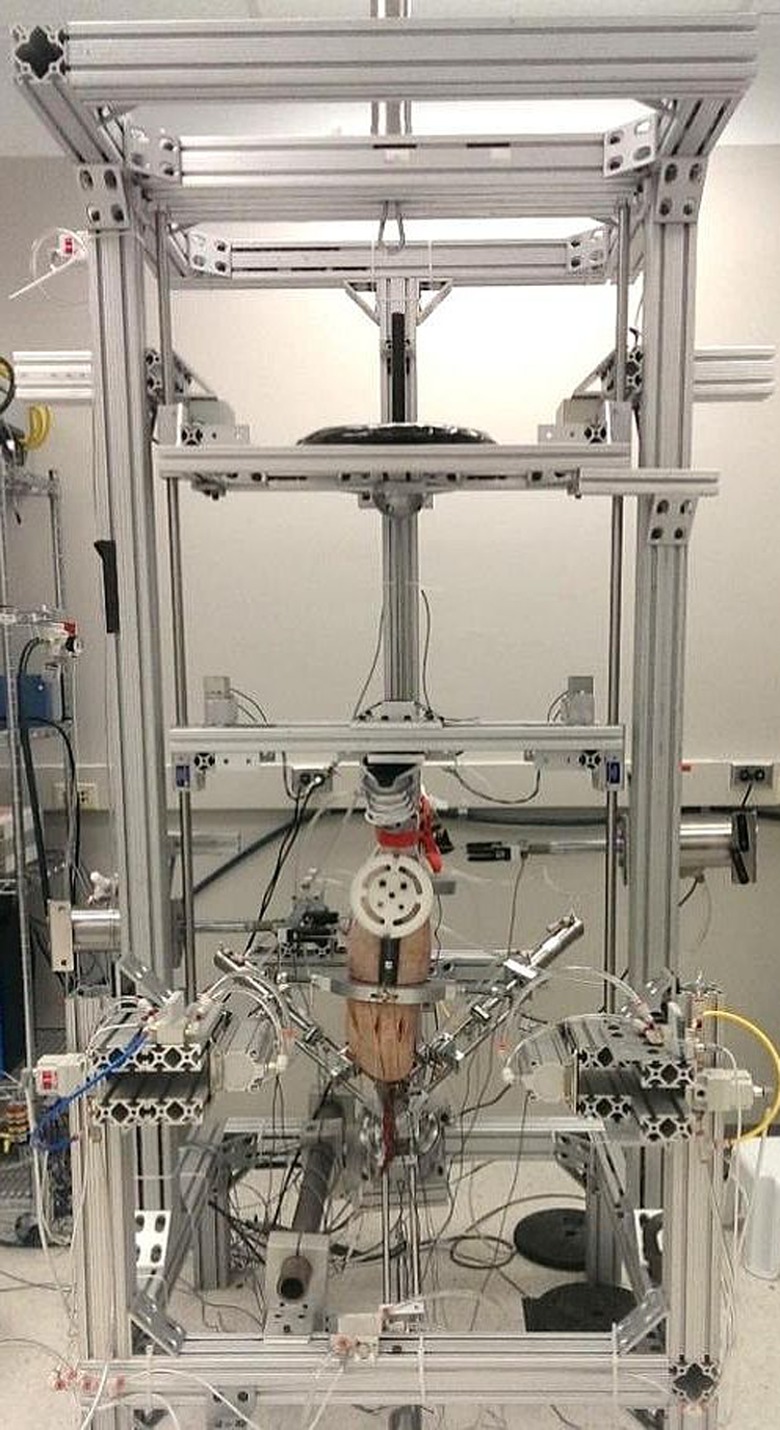
Custom-designed cadaveric impact simulator. The simulator applies external loads via programmatically controlled pneumatic cylinders and supplies a gravity-driven sled with customizable height and weight.
All limbs were oriented in the impactor at 25° to the vertical sagittal plane. A knee flexion angle of 25° was used, as it is representative of initial contact (IC) knee orientation in young athletes landing from a drop height of 31 cm.2 The long axis of the tibia was then aligned with the axis of the impact in the frontal and sagittal planes.
Impactor data were collected from load cells and differential variable reluctance transducers at 10 kHz with custom-designed software (LabVIEW 2015; National Instruments). During data collection, the software triggered the pneumatic cylinders for external loading/unloading and the electromagnet release of the drop sled to deliver the impact. All data were filtered with a 12-Hz low-pass fourth-order Butterworth filter and then postprocessed with LabVIEW and MATLAB.
Statistical Analysis
Four conditions were sampled for this study: (1) 0% KAM, 0% ATS, 0% ITR (00_00_00); (2) 67% KAM, 67% ATS, 67% ITR (67_67_67); (3) the condition in which each specimen experienced maximum ACL strain (ACL maximum); and (4) the condition prior to ACL failure (prefailure). Thus, with the latter 2 conditions, the amount of KAM, ATS, and ITR can vary across each specimen. The 00_00_00 trial was selected for baseline considerations without external loads, and the 67_67_67 trial was selected for its potential to load the knee with considerable levels of forces and moments in all 3 planes. These conditions were all selected to analyze 6-axis load cell force and moment data in which the ACL is subjected to significant strain. The reason to exclude the actual rupture trial was because of the potential confound that the data of the 6-axis load cell may not have recorded the responses of a joint under ACL strain but, rather, the responses of the tissues after ACL rupture. All kinetic variables were analyzed with raw values and normalized to (1) body weight (newtons) for forces and (2) body weight (newtons) and height (meters) for moments. Five kinetic variables were analyzed in this experiment: (1) anterior/posterior knee translation, (2) medial/lateral knee translation, (3) knee compression/distraction, (4) internal/external knee moment, and (5) abduction/adduction knee moment. As knee flexion/extension was restrained at 25° in the sagittal plane, flexion/extension moments of the knee were not able to be properly analyzed.
Statistical analyses were performed with JMP (v 12; SAS Institute) with utilization of 2-way repeated-measures analysis of variance (ANOVA) and Fisher exact test. For all 2-way repeated-measures ANOVA, we compared sex (male, female) by load (00_00_00, 67_67_67, ACL maximum, prefailure) and the interaction of sex × load. Statistical significance was set at P < .05.
Results
Specimen demographics were similar across sexes for age, body mass index, limb side, and dominant limb. There were expected anthropometric significant differences of increased body mass and height in male specimens (Table 2). Although the male specimens had significantly increased mass and height than female specimens, the sexes were equivalent in terms of body mass index (Table 2).
TABLE 2.
Specimen Demographics by Sexa
| Male (n = 19) | Female (n = 20) | P Value | |
|---|---|---|---|
| Age, y | 43.1 ± 7.7 | 40.0 ± 9.0 | .249 |
| Mass, kg | 95.4 ± 19.3 | 76.5 ± 27.8 | .019 |
| Height, cm | 181.7 ± 5.4 | 165.4 ± 7.5 | <.001 |
| Body mass index | 29.1 ± 6.5 | 27.7 ± 9.6 | .612 |
| Limb side, left:right, n | 8:11 | 11:9 | .527 |
| Dominant limb, left:right, n | 5:14 | 3:17 | .451 |
aValues are reported as mean ± SD unless otherwise noted. Age of specimens ranged from 24 to 52 years. Bolding indicates statistically significant between-group difference (P < .05).
Vertical Ground Reaction Force
For vGRF at maximum, minimum, IC, and 33, 66, and 100 milliseconds, sex (F 1,136 = 3.506, P = .064), load (F 3,136 = 0.009, P = .999), and the interaction of sex × load (F 3,136 = 0.260, P = .854) were not significant.
Ligament Strain
Males had a maximum ACL strain of 13.2% ± 8.1%, and females had a maximum ACL strain of 16.7% ± 8.3%. There was no significant difference between ligament strains (P = .184).
Knee Abduction/Adduction Moments
For knee abduction/adduction torque at maximum, minimum, IC, and 33, 66, and 100 milliseconds, sex was a significant factor (F 1,136 = 4.398, P = .038), as was load (F 3,136 = 39.093, P < .001), but the interaction of sex × load was not significant (F 3,136 = 2.515, P = .061). Compared with males, females exhibited 10.3-N·m increased abduction torque at the knee at 66 milliseconds postimpact and 22.3-N·m increased abduction torque at 100 milliseconds postimpact (Table 3). As for loading condition, the “ACL maximum” condition demonstrated a maximum difference of 54.3-N·m increased abduction torque and 74.5-N·m increased abduction torque at 66 milliseconds postimpact. With normalized values, sex was again significant (F 1,136 = 7.155, P = .008), as was load (F 3,136 = 31.651, P < .001), but the interaction of sex × load was again not significant (F 3,136 = 1.700, P = .170). For females, with inclusion of only knee abduction values, normalized values of KAM at maximum were 52% greater than males (Figure 2).
TABLE 3.
Raw Values of Knee Abduction Moment Between Sexes Across Timea
| Abduction/Adduction Moment, N·m, Mean ± SD | ||||||
|---|---|---|---|---|---|---|
| Sex | IC | 33 ms | 66 ms | 100 ms | Minimum | Maximum |
| Male | –3.8 ± 16.5 | 7.3 ± 46.5 | 24.6 ± 67.5 | –10.4 ± 51.4 | –69.0 ± 22.3 | 79.7 ± 47.9 |
| Female | 3.3 ± 21.1 | 7.8 ± 50.2 | 34.9 ± 61.4 | 11.9 ± 44.5 | –56.8 ± 20.9 | 84.5 ± 47.3 |
aPositive values denote knee abduction; negative values denote knee adduction. IC, initial contact.
Figure 2.

Normalized knee abduction/adduction moments at various time points. Females demonstrated an increased level of knee abduction moment as compared with males. F, female; IC, initial contact; M, male.
Internal/External Knee Rotation Moments
For knee internal/external rotation, load was a significant factor at maximum, minimum, IC, and 33, 66, and 100 milliseconds (F 3,136 = 34.906, P < .001), but sex (F 1,136 = 1.968, P = .163) and the interaction of sex × load (F 3,136 = 0.794, P = .499) lacked significance. With normalized values, significance remained the same for load (F 3,136 = 31.328, P < .001), sex (F 1,136 = 2.538, P = .114), and the interaction of sex × load (F 3,136 = 0.349, P = .790). The “ACL maximum” condition demonstrated increased external rotation at 66 milliseconds and maximum value when compared with the other load conditions.
Anterior/Posterior Knee Translational Forces
Sex was a significant factor for anterior/posterior knee translational force at maximum, minimum, IC, and 33, 66, and 100 milliseconds (F 1,136 = 64.411, P < .001); load was also a significant factor (F 3,136 = 3.194, P = .026), but there was no significant interaction of sex × load (F 3,136 = 0.956, P = .416). However, with normalized values, 2-way repeated-measures ANOVA demonstrated no significance for sex (F 1,136 = 3.333, P = .070), load (F 3,136 = 1.922, P = .129), and the interaction of sex × load (F 3,136 = 0.241, P = .867).
Lateral/Medial Knee Translational Forces
Sex was a significant factor for lateral/medial knee translational forces at maximum, minimum, IC, and 33, 66, and 100 milliseconds (F 1,136 = 26.960, P < .001); load was also a significant factor (F 3,136 = 19.242, P < .001), as was the interaction of sex × load (F 3,136 = 4.825, P = .003). However, once normalization was applied, the significance was eliminated for sex (F 1,136 = 1.966, P = .163) and the interaction of sex × load (F 3,136 = 1.973, P = .121). Significance of load was maintained (F 3,136 = 15.629, P < .001) with demonstration of increased medial translational force in the “ACL maximum” and “prefailure” conditions (Figure 3).
Figure 3.
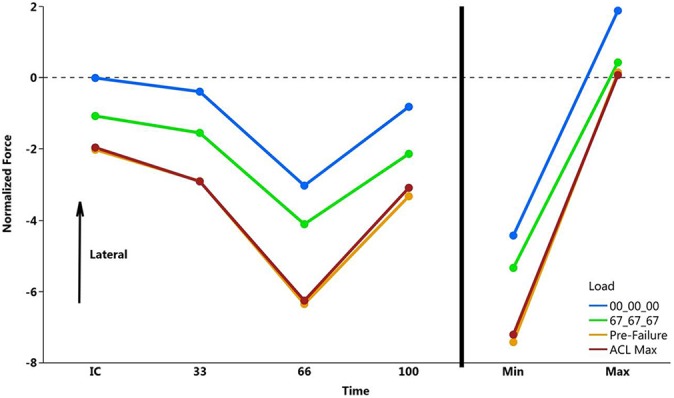
Normalized lateral/medial knee translational force at various time points. Positive values denote knee lateral translation; negative values denote medial translation. Prefailure and ACL maximum external load conditions demonstrated similar characteristics and significant medial knee translational force as compared with 00_00_00 (0% knee abduction moment, 0% anterior tibial shear, 0% internal tibial rotation) and 67_67_67 (67% knee abduction moment, 67% anterior tibial shear, 67% internal tibial rotation). ACL, anterior cruciate ligament.
Knee Distraction/Compression Forces
Sex was a significant factor for knee distraction/compression forces at maximum, minimum, IC, and 33, 66, and 100 milliseconds (F 1,136 = 28.417, P < .001); load was also a significant factor (F 3,136 = 2.713, P = .047). The interaction of sex × load was not significant (F 3,136 = 0.419, P = .740). However, with normalized values, sex was not a significant factor (F 1,136 = 2.249, P = .136), nor was load (F 3,136 = 1.808, P = .149) or the interaction of sex × load (F 3,136 = 0.119, P = .949).
Discussion
This study investigated the 3-dimensional kinetics of the intact human knee with simulated in vivo calculated external loads. To our knowledge, this is the first study to measure the 3-dimensional intact knee forces and moments with a simulated landing for sex-specific differentiation. Specific to load condition, there were significant differences across all 5 kinetic variables examined. As males and females had significant differences of height and mass (Table 2), it was imperative to normalize the 6-axis load cell data to attain proper comparisons of forces and moments. Once normalization was applied, only medial knee translational force, external rotation moment, and abduction moment remained significant relative to the magnitude of external load applied to the joint (Table 4). ATS, ITR, and KAM contribute to ACL load and strain.3,11,29,30
TABLE 4.
P Values of Each Knee Kinetic Parameter in the Raw and Normalized Conditionsa
| Rotation | Translation | ||||
|---|---|---|---|---|---|
| Abduction/Adduction | Internal/External | Anterior/Posterior | Lateral/Medial | Distraction/Compression | |
| Raw | |||||
| Sex | .038 | .163 | <.001 | <.001 | <.001 |
| Load | <.001 | <.001 | .026 | <.001 | .047 |
| Sex × load | .061 | .499 | .416 | .003 | .740 |
| Normalized | |||||
| Sex | .008 | .114 | .070 | .163 | .136 |
| Load | <.001 | <.001 | .129 | <.001 | .149 |
| Sex × load | .170 | .790 | .867 | .121 | .949 |
aBolding indicates statistically significant variable (P < .05).
After normalization, there were no significant differences between sexes for anterior/posterior knee translational force, medial/lateral knee translational force, knee distraction/compression force, or knee internal/external rotation moment. This demonstrates that both sexes encounter equal loading of the knee along these specific vectors and planes when adjusted for between-sex variability in height and mass. However, prior to and after normalization of the data, females demonstrated significant increases of KAM as compared with males at similar time points across the impact trial (100-millisecond duration) (Table 3 and Figure 2). Adolescent females produce larger magnitudes of out-of-plane moments than do males when landing from a jump.19 Therefore, the current investigation exemplifies that biomechanical behaviors representative of the female population during landing are likely to place a disproportionately larger strain on the ACL than that of males. In addition, these data support current methods of ACL risk stratification that are largely based on the magnitude of KAM.17 This significant increase of KAM kinetics demonstrates that KAM is a major contributor to ACL failure.15,19,39
Across all 5 kinetic variables analyzed, there was no significance of the interaction between sex and load (sex × load). This demonstrates that external loads and sex do not have a compounding effect on the outcomes of knee kinetic loading; rather, these variables act independently. Consequently, from the data presented, females will experience higher KAM with similar loading conditions as compared with males, which potentially predispose females to increased risk of ACL injury.
The vGRF was consistent across all load condition trials. Statistical comparison of vGRF demonstrated no significant difference between sexes with minimum values, maximum values, at IC, or at 33, 66, or 100 milliseconds postcontact. This is important to the nature of this study, as significant differences in vGRF could increase forces/moments at the knee and consequently induce more strain on the ACL. Consistency of the vGRF across trials demonstrates that biomechanical mechanisms other than vGRF (ie, dynamic knee valgus) influence resultant forces and moments at the knee that act to induce ACL injury. Although previous studies have demonstrated that females land with increased valgus,12,21,27 these studies did not specifically analyze the forces/moments at the knee joint with controlled input prior to ACL rupture. In this study, there was no neuromuscular control that could have contributed to induced valgus in females. Therefore, this study demonstrates that independent of neuromuscular control, females experience increased KAM from a drop landing.
It has been suggested that the increased incidence of female ACL injury as compared with males is due to inherent biomechanical differences between the sexes, such as musculoskeletal alignment, muscle anatomy/physiology, and passive joint compliance.7,18,33,38 Additionally, the injury disparity may be due to movement organization of descending input from cortical and subcortical regions,9 which may be mediated by hormonal concentration differences.8 As previously stated, this study did not allow for any neuromuscular control and could not take hormonal effects into account. However, the study does demonstrate that musculoskeletal alignment, viscoelastic properties of the myotendinous and ligamentous structure, and passive joint compliance are all potential factors that cause the higher prevalence of ACL injury in females.
Of particular interest in this study, ATS was not significantly different between sexes, although it is the primary motion of restraint of the ACL. While the ACL is a primary restraint for anterior knee translation, the ACL is also critical for stability for ITR and KAM. It is currently unclear why the “ACL maximum” condition exhibited external rotation at 66 milliseconds postimpact and at maximum value as compared with the other load conditions. This disparity will be explored in future work. The data reported here provide explanation to previous findings that female athletes often demonstrate a predominately coronal plane strategy of dynamic knee motion.16 Owing to the statistically significant level of increased KAM for females, the data evoke an even greater emphasis on young female athletes and their clinical and coaching staff to seek preventive neuromuscular training to avert potential ACL injury,11,13,14 especially for athletes involved in sports that involve landing, jumping, cutting, and pivoting. By participation in preventive neuromuscular training protocols, these young female athletes can avert a serious knee injury that carries burdensome sequelae of inactivity, future knee injury, and osteoarthritis.36 Future research should evaluate the effect of targeted preventive neuromuscular training and their effects on reducing the sex disparity that exists, with emphasis on frontal knee mechanics.
The cadaveric impactor used in this study utilized a dynamic, multiplanar knee injury simulation that is highly relevant to loading observed in typical sport maneuvers of landing, cutting, and pivoting.34 Consequently, the impactor induced physiologically relevant forces and moments encountered by athletes during such maneuvers. This work contributes to the scientific literature that KAM increases strain to the ACL under clinically representative loading. Additionally, this work further establishes the biomechanical characteristics of knee loading between sexes.
This study was limited by the inability to analyze flexion/extension knee moments and compare these with 3-dimensional motion capture data, as previously done for DVJ landings. The current protocol was designed with knowledge of this limitation because we wanted to know the effect of landing “stiff,” with poor biomechanics, at a common landing angle of 25° of knee flexion.2,30 Future studies will allow for free range of motion in the sagittal plan to determine the important kinetics that occurs during DVJ tasks. Additionally, this study was limited to cadaveric specimens with a mean age above that most common to ACL injury. However, this model included an age inclusion criterion of 18 to ≤50 years, with a mean age of 41.5 years, to more accurately reflect the data observed in the ACL-injured population. Although living tissue can heal and respond to external loads, the cadaveric specimens utilized were limited to 1 freeze-thaw cycle to preserve tissue quality and were simulated with external loads determined from in vivo DVJs. Moreover, the pneumatic loading allowed for rapid loading/unloading of the external loads and thus preserved native properties of the viscoelastic structures analyzed.
Conclusion
Under the tested conditions, increased external loads led to increased medial knee translation force, KAM, and external rotation knee moment. Compared with males, females exhibit greater forces and moments at the knee, especially regarding KAM, when loaded in similar conditions. As these kinetics are associated with increased load and strain on the ACL, the sex differences observed in the present study demonstrate a portion of the underlying mechanics that predispose females to ACL injury as compared with males in a controlled simulated athletic task.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: Funding for this study was received from the National Institute of Arthritis and Musculoskeletal and Skin Diseases (R01AR056259 and R01AR055563 to T.E.H., L30AR070273 to N.D.S., T32AR056950 to C.N.) and from the National Institute of Child Health and Human Development (K12HD065987 to N.D.S.). A.J.K. is a paid consultant for Arthrex and DePuy Orthopaedics, receives royalties for meniscus repair from Arthrex, and serves on the medical board of trustees of the Musculoskeletal Transplant Foundation.
Ethical approval for this study was waived by the Mayo Clinic Institutional Review Board (application 15-005819).
References
- 1. Arendt EA, Agel J, Dick R. Anterior cruciate ligament injury patterns among collegiate men and women. J Athl Train. 1999;34(2):86–92. [PMC free article] [PubMed] [Google Scholar]
- 2. Bates NA, Ford KR, Myer GD, Hewett TE. Kinetic and kinematic differences between first and second landings of a drop vertical jump task: implications for injury risk assessments? Clin Biomech (Bristol, Avon). 2013;28(4):459–466. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Bates NA, Myer GD, Shearn JT, Hewett TE. Anterior cruciate ligament biomechanics during robotic and mechanical simulations of physiologic and clinical motion tasks: a systematic review and meta-analysis. Clin Biomech (Bristol, Avon). 2015;30(1):1–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Bates NA, Schilaty ND, Nagelli CV, Krych AJ, Hewett TE. Novel mechanical impact simulator designed to generate clinically relevant anterior cruciate ligament ruptures. Clin Biomech (Bristol, Avon). 2017;44:36–44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Beynnon B, Howe JG, Pope MH, Johnson RJ, Fleming BC. The measurement of anterior cruciate ligament strain in vivo. Int Orthop. 1992;16(1):1–12. [DOI] [PubMed] [Google Scholar]
- 6. Blackburn JT, Norcross MF, Padua DA. Influences of hamstring stiffness and strength on anterior knee joint stability. Clin Biomech (Bristol, Avon). 2011;26(3):278–283. [DOI] [PubMed] [Google Scholar]
- 7. Cammarata ML, Dhaher YY. Evidence of gender-specific motor templates to resist valgus loading at the knee. Muscle Nerve. 2010;41(5):614–623. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Field EF, Pellis SM. The brain as the engine of sex differences in the organization of movement in rats. Arch Sex Behav. 2008;37(1):30–42. [DOI] [PubMed] [Google Scholar]
- 9. Ford KR, Myer GD, Schmitt LC, Uhl TL, Hewett TE. Preferential quadriceps activation in female athletes with incremental increases in landing intensity. J Appl Biomech. 2011;27(3):215–222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Griffin LY, Agel J, Albohm MJ, et al. Noncontact anterior cruciate ligament injuries: risk factors and prevention strategies. J Am Acad Orthop Surg. 2008;8(3):141–150. [DOI] [PubMed] [Google Scholar]
- 11. Hewett TE, Bates NA. Preventive biomechanics. Am J Sports Med. 2017;45(11):2654–2664. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Hewett TE, Ford KR, Hoogenboom BJ, Myer GD. Understanding and preventing ACL injuries: current biomechanical and epidemiologic considerations—update 2010. N Am J Sports Phys Ther. 2010;5(4):234–251. [PMC free article] [PubMed] [Google Scholar]
- 13. Hewett TE, Ford KR, Myer GD. Anterior cruciate ligament injuries in female athletes: part 2, a meta-analysis of neuromuscular interventions aimed at injury prevention. Am J Sports Med. 2006;34(3):490–498. [DOI] [PubMed] [Google Scholar]
- 14. Hewett TE, Ford KR, Xu YY, Khoury J, Myer GD. Effectiveness of neuromuscular training based on the neuromuscular risk profile. Am J Sports Med. 2017;45(9):2142–2147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Hewett TE, Ford KR, Xu YY, Khoury J, Myer GD. Utilization of ACL injury biomechanical and neuromuscular risk profile analysis to determine the effectiveness of neuromuscular training. Am J Sports Med. 2016;44(12):3146–3151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Hewett TE, Myer GD, Ford KR. Anterior cruciate ligament injuries in female athletes: part 1, mechanisms and risk factors. Am J Sports Med. 2006;34(2):299–311. [DOI] [PubMed] [Google Scholar]
- 17. Hewett TE, Myer GD, Ford KR, et al. Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: a prospective study. Am J Sports Med. 2005;33(4):492–501. [DOI] [PubMed] [Google Scholar]
- 18. Hewett TE, Myer GD, Ford KR, Paterno MV, Quatman CE. Mechanisms, prediction, and prevention of ACL injuries: cut risk with three sharpened and validated tools. J Orthop Res. 2016;34(11):1843–1855. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Hewett TE, Myer GD, Kiefer AW, Ford KR. Longitudinal increases in knee abduction moments in females during adolescent growth. Med Sci Sports Exerc. 2015;47(12):2579–2585. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Hewett TE, Torg JS, Boden BP. Video analysis of trunk and knee motion during non-contact anterior cruciate ligament injury in female athletes: lateral trunk and knee abduction motion are combined components of the injury mechanism. Br J Sports Med. 2009;43(6):417–422. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Joseph MF, Rahl M, Sheehan J, et al. Timing of lower extremity frontal plane motion differs between female and male athletes during a landing task. Am J Sports Med. 2011;39(7):1517–1521. [DOI] [PubMed] [Google Scholar]
- 22. Karakaya İÇ, Karakaya MG. Proprioception and gender In: Kaya D, ed. Proprioception: The Forgotten Sixth Sense. Foster City, CA: OMICS Group eBooks; 2014:3–12. [Google Scholar]
- 23. Kim J, Jung J, Reyes JL, et al. Gender differences in leg stiffness and stiffness recruitment strategy during two-legged hopping. J Mot Behav. 2005;37(2):111–125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Levine JW, Kiapour AM, Quatman CE, et al. Clinically relevant injury patterns after an anterior cruciate ligament injury provide insight into injury mechanisms. Am J Sports Med. 2012;41(2):385–395. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Mall NA, Chalmers PN, Moric M, et al. Incidence and trends of anterior cruciate ligament reconstruction in the United States. Am J Sports Med. 2014;42(10):2363–2370. [DOI] [PubMed] [Google Scholar]
- 26. Mendiguchia J, Ford KR, Quatman CE, Alentorn-Geli E, Hewett TE. Sex differences in proximal control of the knee joint. Sports Med. 2011;41(7):541–557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Myer GD, Ford KR, Hewett TE. The effects of gender on quadriceps muscle activation strategies during a maneuver that mimics a high ACL injury risk position. J Electromyogr Kinesiol. 2005;15(2):181–189. [DOI] [PubMed] [Google Scholar]
- 28. Myer GD, Ford KR, Khoury J, Succop P, Hewett TE. Biomechanics laboratory-based prediction algorithm to identify female athletes with high knee loads that increase risk of ACL injury. Br J Sports Med. 2011;45(4):245–252. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Nesbitt RJ, Herfat ST, Boguszewski DV, Engel AJ, Galloway MT, Shearn JT. Primary and secondary restraints of human and ovine knees for simulated in vivo gait kinematics. J Biomech. 2014;47(9):2022–2027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Quatman CE, Hewett TE. The anterior cruciate ligament injury controversy: is “valgus collapse” a sex-specific mechanism? Br J Sports Med. 2009;43(5):328–335. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Quatman CE, Kiapour AM, Demetropoulos CK, et al. Preferential loading of the ACL compared with the MCL during landing: a novel in sim approach yields the multiplanar mechanism of dynamic valgus during ACL injuries. Am J Sports Med. 2014;42(1):177–186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Renström PA. Eight clinical conundrums relating to anterior cruciate ligament (ACL) injury in sport: recent evidence and a personal reflection. Br J Sports Med. 2013;47(6):367–372. [DOI] [PubMed] [Google Scholar]
- 33. Sbriccoli P, Solomonow M, Zhou B-H, Lu Y, Sellards R. Neuromuscular response to cyclic loading of the anterior cruciate ligament. Am J Sports Med. 2005;33(4):543–551. [DOI] [PubMed] [Google Scholar]
- 34. Schilaty ND, Bates NA, Hewett TE. Letter to the editor: effect of sagittal plane mechanics on ACL strain during jump landing. J Orthop Res. 2017;35(6):1171–1172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Schilaty ND, Bates NA, Sanders TL, Krych AJ, Stuart MJ, Hewett TE. Incidence of second anterior cruciate ligament tears (1990-2000) and associate factors by geographic locale. Am J Sports Med. 2017;45(7):1567–1573. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Schilaty ND, Nagelli CV, Bates NA, et al. Incidence of second anterior cruciate ligament tears and identification of associated risk factors from 2001 to 2010 using a geographic database. Orthop J Sports Med. 2017;5(8):2325967117724196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Schilaty ND, Nagelli CV, Hewett TE. Use of objective neurocognitive measures to assess the psychological states that influence return to sport following injury. Sports Med. 2015;46(3):299–303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Shultz SJ, Schmitz RJ, Benjaminse A, Chaudhari AM, Collins M, Padua DA. ACL research retreat VI: an update on ACL injury risk and prevention. J Athl Train. 2012;47(5):591–603. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Stasi SD, Myer GD, Hewett TE. Neuromuscular training to target deficits associated with second anterior cruciate ligament injury. J Orthop Sports Phys Ther. 2013;43(11):777–792, A1–A11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Wang D, De Vito G, Ditroilo M, Fong DTP, Delahunt E. A comparison of muscle stiffness and musculoarticular stiffness of the knee joint in young athletic males and females. J Electromyogr Kinesiol. 2015;25(3):495–500. [DOI] [PubMed] [Google Scholar]
- 41. Wang I, Wang S, Wang L. Sex differences in lower extremity stiffness and kinematics alterations during double-legged drop landings with changes in drop height. Sports Biomech. 2015;14(4):404–412. [DOI] [PubMed] [Google Scholar]
- 42. Yu B, Garrett WE. Mechanisms of non-contact ACL injuries. Br J Sports Med. 2007;41(suppl 1):I47–I51. [DOI] [PMC free article] [PubMed] [Google Scholar]