

Abstract
Objective:
To evaluate whether multidetector CT with low-dose radiation (low-dose CT) of joints can be useful when evaluating fractures.
Methods:
Our study included CT scans of 398 patients, 103 shoulder cases, 109 wrist cases, 98 pelvis cases and 88 ankle cases. There were 191 females and 207 males. The low-dose CTs were performed using identical voltage and parameters with the exception of decreased (half of standard dose) tube current. Low-dose and standard-dose images were compared with regards to objective image quality, subjective evaluation of image quality and diagnostic performance for the fractures.
Results:
There was no significant difference of image noise between standard-dose CT and low-dose CT in every joint (p > 0.05). Each mean value of subjective score did not show significant difference according to the dosage of the CT scan. There were no statistically significant differences in the sensitivity (96–100%), specificity (95.2–100%) or accuracy (97.9–100%) between standard-dose CT and low-dose CT (p values, 0.1336–1.000).
Conclusion:
The evaluation of extremities for fractures using low-dose CT can reduce radiation exposure by about 50% compared with standard-dose CT without affecting image quality or diagnostic performance.
Advances in knowledge:
Low-dose CT of the extremities (shoulder, pelvis, ankle and wrist) can reduce radiation dose by about 50% compared with standard-dose CT and does not significantly affect image quality or diagnostic performance in fracture detection.
INTRODUCTION
Fractures are common injuries easily diagnosed using plain radiography. The use of multidetector CT (MDCT) has become more common for diagnosis and treatment decision-making in complex or indistinct fractures.1–4 MDCT is particularly useful for musculoskeletal imaging due to its accuracy, speed and minimal patient manipulation.5 The increased organ radiation doses corresponding to CT study are harmful to patients although the musculoskeletal system tolerates radiation better than other internal organs.6 Although bones are minimally affected by radiation, the marrow found within bones is the most radiosensitive organ in the body. Although the use of MDCT has increased since its development, many clinicians order CT scans without considering radiation exposure. Many recent studies have focused on reducing radiation exposure in skeletal CT.5–11 The aim of this study was to evaluate whether MDCT with low-dose radiation (low-dose CT, tube current is 50% of standard dose CT) can be useful when evaluating fractures. Thus, we compared the diagnostic accuracy of low-dose and standard-dose CT.
METHODS AND MATERIALS
Case selection
We retrospectively evaluated CT scans of 427 patients who visited our hospital with musculoskeletal complaints after trauma who underwent CT imaging (standard dose or low dose) of the shoulder, wrist, pelvis or ankle between January 2014 and May 2015. The patients who visited our hospital from January 2014 to September 2014 underwent standard dose CT and who from October 2014 to May 2015 underwent low dose CT. We excluded 29 patients who had pain due to other causes, such as systemic diseases involving the musculoskeletal system, tumorous conditions or infectious diseases. Our study included CT scans of 398 patients, 103 shoulder cases, 109 wrist cases, 98 pelvis cases and 88 ankle cases. There were 191 females and 207 males (mean age: 51.5 years, range: 3–93 years) included in the study. These patients were classified as fracture group and no-fracture group based on physical examination and clinical manifestations. The final diagnosis was made through following results: Apparent positive findings on plain radiography (89 cases), positive MRI findings (bone marrow edema in the equivalent bone, 10 cases), physical examination (tenderness and swelling at the equivalent bone, 99 cases) and surgical findings (209 cases). Our study population is summarized in Table 1. This study was approved by our hospital institutional ethics review board, and the requirement for informed consent was waived because of the retrospective nature of the study.
Table 1.
Selected cases of our study
| Location | Dose | Number of patients | Sex (M/F) | Age (years, mean/median) | Patients with fracture | Total fracture number |
|---|---|---|---|---|---|---|
| Shoulder | Standard-dose CT scan | 52 | 32/20 | 53/53 | 32 | 41 |
| Low-dose CT scan | 51 | 28/23 | 50/53 | 43 | 65 | |
| Pelvis | Standard-dose CT scan | 47 | 20/27 | 63/69 | 26 | 39 |
| Low-dose CT scan | 51 | 20/31 | 66/75 | 33 | 54 | |
| Ankle | Standard-dose CT scan | 43 | 26/17 | 38/33 | 25 | 38 |
| Low-dose CT scan | 45 | 23/22 | 45/41 | 38 | 78 | |
| Wrist | Standard-dose CT scan | 58 | 28/30 | 46/52 | 46 | 55 |
| Low-dose CT scan | 51 | 30/21 | 47/52 | 42 | 60 | |
| Total | Standard-dose CT scan | 200 | 27/24 | 50/52 | 129 | 173 |
| Low-dose CT scan | 198 | 25/24 | 52/55 | 156 | 257 |
Image acquisition
A 64-MDCT scanner (Brilliance 40, Philips Medical Systems, Cleveland, OH) was used for all CT scans. The scanning conditions (tube voltage and currents) for each group are shown in Table 2. Table speed was 31.3 mms−1 (except 48.5 mms−1 for the pelvis). For the low-dose studies, CTs were performed using identical kilo-voltage and parameters, but used decreased tube current (half dose). We used small focal spot size (0.6 × 0.7 mm) to acquire high resolution image. The field-of-view was adapted to the sectional area of each joint of the patients. The bone algorithm was used for image reconstruction. The reconstruction was done with filtered back projection. Sections were reconstructed with a 2-mm slice thickness at 2-mm intervals. Volume CT dose indices (CTDIvol) and dose length product (DLP) were automatically recorded. Effective doses (ED, mSv) were calculated based on dose and scan length.
Table 2.
CT parameters of each group
| Body part | Dose group | Tube voltage (kV) | Tube current (mA) | Collimation (mm) | Pitch | Rotation time (s) | Thickness (mm) | Scan length (cm) |
|---|---|---|---|---|---|---|---|---|
| Shoulder | Standard | 120 | 200 | 64 × 0.625 | 0.609 | 0.5 | 2 | 32 |
| Low | 120 | 100 | 64 × 0.625 | 0.609 | 0.5 | 2 | 32 | |
| Pelvis | Standard | 120 | 200 | 64 × 0.625 | 0.609 | 0.5 | 2 | 32 |
| Low | 120 | 100 | 64 × 0.625 | 0.609 | 0.5 | 2 | 32 | |
| Ankle | Standard | 120 | 150 | 64 × 0.625 | 0.391 | 0.5 | 2 | 32 |
| Low | 120 | 75 | 64 × 0.625 | 0.391 | 0.5 | 2 | 32 | |
| Wrist | Standard | 120 | 150 | 64 × 0.625 | 0.391 | 0.5 | 2 | 16 |
| Low | 120 | 75 | 64 × 0.625 | 0.391 | 0.5 | 2 | 16 |
Image analysis
CT images were assessed based on objective image quality, subjective evaluation of the image quality and the diagnostic performance for the fracture. First, a region of interest (ROI) was placed within the medullary portion of the bone to measure the standard deviation (SD) in the Hounsfield unit.5 The diameter of the ROI was 1 cm (Figure 1). The ROIs were located at the epiphysis of the humeral head of the shoulder joint, the epiphysis of the femoral head of the hip joint, the epiphysis of the distal tibia of the ankle joint and the epiphysis of the distal radius of the wrist joint based on coronal view. The measurement of the SD was performed by two radiologists in consensus. Subjective evaluations of the image quality were performed independently by two musculoskeletal radiologists with 14 and 8 years of experience, respectively, who were blinded to clinical information and radiologic reports. First, they evaluated the quality of the image using the following subjective 5-point scoring system from 0 to 4:4 (excellent image quality) = clear image and uniformity in particle size of CT pixel, 3 (good image quality) = clear image and comparative uniformity in particle size, 2 (moderate image quality) = general image and not uniform in particle size, not interfering with diagnostic quality, anatomic structures can be clearly demonstrated, 1 (poor image quality) = unclear image and coarse particle size, anatomic structures are ambiguous, interfering with diagnostic quality, 0 (very poor image quality) = unclear image, coarse particle size, anatomic structures are ambiguous, impossible to diagnose.12 Second, they reported the presence of a fracture, location of the fracture and number of fracture fragments (Figures 2–4).
Figure 1.
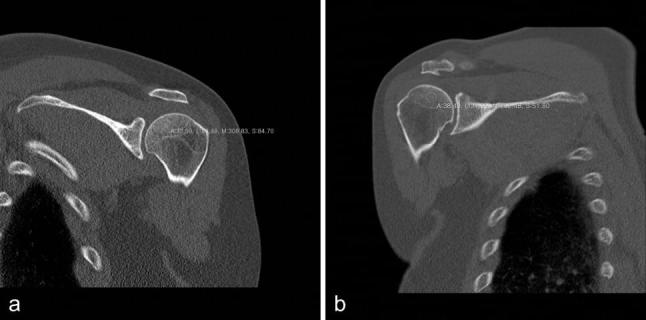
Measurement of standard deviation in Hounsfield units. (a) A 49-year-old female who complained of left shoulder pain for 3 months. She had tenderness at the shoulder joint on physical examination, limited movement and no abnormal findings on plain radiography. A region of interest was placed within the medullary portion of the epiphysis of the humerus (circle). Standard CT did not reveal a fracture. The scores of image quality were 4 by both interpreters. (b) A 54-year-old female with right shoulder pain after being struck by a car. She had tenderness at the joint on physical examination, limited movement and no abnormal findings on plain radiography. An ROI was placed within the medullary portion of the epiphysis of the humerus (circle). Low-dose CT image did not reveal a fracture. The scores of image quality were 3 by both interpreters.
Figure 2.

A 52-year-old female with bilateral hip pain for 3 months. She showed tenderness and positive Patrick’s test bilaterally.(a) Plain radiography of the pelvis does not show apparent fracture line.(b) Coronal reconstruction image of standard-dose pelvic bone CT shows faint irregular lines on both femoral heads, suggesting insufficiency fractures (arrows). Initial diagnosis missed these lesions.(c) Fat suppressed T2 weighted coronal image [Repetition Time (TR)/Echo Time (TE) = 3200, 40 ms] showing subchondral insufficiency fractures in both femoral heads (arrows).
Figure 4.
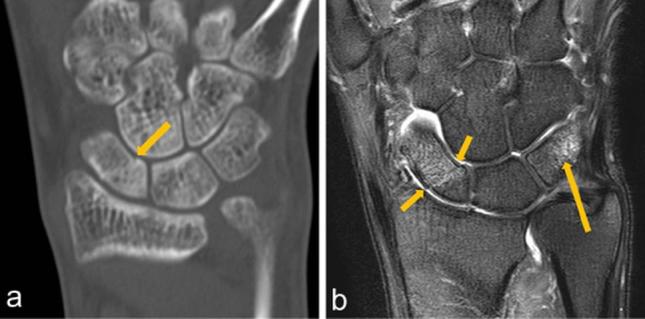
A 37-year-old male with left hand pain after a fall. He had tenderness and swelling of the hand. (a) Coronal image of low-dose CT scan showing faint cortical disruption (arrow) in the proximal scaphoid. This fracture was misdiagnosed as normal by one of interpreters. (b) Immediate follow-up MRI. Coronal T2 weighted fat-suppressed image (TR/TE, 4000 ms/90 ms) at the same portion revealed fracture lines and combined bone marrow edema (small arrows). Bone marrow edema was also evident in the triquetrum (long arrow). No apparent fracture line was seen on the CT even in the second evaluation.
Figure 3.
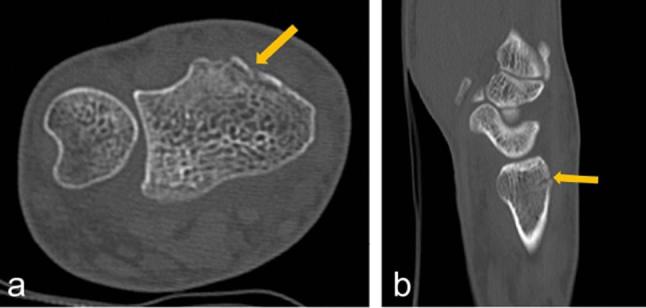
A 45-year-old male with right wrist pain after a fall. He had tenderness, swelling of the joint and limited movement. Plain radiography did not show definite fracture lines. (a) Axial image of standard-dose CT scan showing faint cortical disruption (arrow). (b) Sagittal reconstructed image showing cortical disruption (arrow). The patient was diagnosed with an avulsion fracture of the distal radius clinically and radiologically.
Statistical analysis
We compared the mean values of the SD, DLP, ED and image quality scores of standard-dose CT with low-dose CT using the Mann-Whitney U test (Table 3). Inter-reader agreement of the image quality score was analysed using an intraclass correlation coefficient (ICC). ICC values greater than 0.75 suggest excellent agreement, 0.40–0.75 are considered fair to good agreement, and values less than 0.40 are considered poor agreement.13 To compare the diagnostic performance of standard-dose and low-dose CT, the sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV) and accuracy for diagnosing fracture were calculated. Reference standards were made based on clinically confirmed diagnoses. Diagnostic performance was analysed with Chi-square test. Statistical analyses were performed using statistical software PASW version 18.0 (IBM, Armonk, NY). If p-value calculated was below 0.05 the result was considered as statistically significant.
Table 3.
Image noise (standard deviation of HU), DLP, effective dose and subjective image quality score according to anatomic location
| Location | Dose | Imagenoise | DLPa | Effective dose (mSvb) | Image quality (score, reader 1) | Image quality (score, reader 2) |
|---|---|---|---|---|---|---|
| Shoulder | Standard dose | 62.7 (±15) | 404 (±167) | 5.8 (±2.3) | 3.69 (±0.5) | 3.71 (±0.5) |
| Low dose | 64.1 (±18) | 199 (±78) | 2.9 (±1.1) | 3.78 (±0.4) | 3.78 (±0.4) | |
| p value | 0.77 | <0.001 | <0.001 | 0.37 | 0.40 | |
| Pelvis | Standard dose | 73.4 (±22) | 492 (±190) | 7.4 (±2.9) | 3.78 (±0.4) | 3.77 (±0.4) |
| Low dose | 69.2 (±23) | 247 (±59) | 3.9 (±1.6) | 3.76 (±0.5) | 3.82 (±0.4) | |
| p value | 0.41 | <0.001 | <0.001 | 0.93 | 0.48 | |
| Ankle | Standard dose | 94.1 (±29) | 229 (±90) | 1.4 (±0.5) | 3.60 (±0.5) | 3.65 (±0.5) |
| Low dose | 81.6 (±24) | 136 (±46) | 0.8 (±0.3) | 3.60 (±0.7) | 3.64 (±0.6) | |
| p value | 0.45 | <0.001 | <0.001 | 0.73 | 0.94 | |
| Wrist | Standard dose | 78.0 (±27) | 202 (±31) | 1.2 (±0.2) | 3.86 (±0.5) | 3.88 (±0.4) |
| Low dose | 67.7 (±27) | 116 (±10) | 0.7 (±0.1) | 3.80 (±0.5) | 3.75 (±0.5) | |
| p value | 0.40 | <0.001 | <0.001 | 0.21 | 0.08 |
Note: Data in parentheses are standard deviations.
DLP, dose length product; HU, Hounsfield unit.
DAP, Dose area product
mSv, milli-Sievert
RESULT
200 patients were scanned using the standard-dose protocol and another 198 patients were scanned with the low-dose protocol. 285 patients had fractures and there were a total of 430 fractures. The prevalence of fracture in our study was 71.6%. Among them, there were 106 shoulder fractures (75 patients), 93 pelvis fractures (59 patients), 116 ankle fractures (63 patients) and 115 wrist fractures (88 patients). The percentages of fracture according to the anatomic location were as follows: shoulder 72.8%, pelvis 60.2%, ankle 71.6% and wrist 80.7%. In the standard-dose group, the percentages of fractures of shoulder, pelvis, ankle and wrist were 61.5%, 55.3%, 58.1% and 79.3%, respectively, and in the low-dose group, the percentages were 84.3%, 64.7%, 84.4% and 82.4%, respectively. The mean DLP and ED values among the standard-dose CT group were significantly higher than those of the low-dose CT group according to the anatomic location (42–50%, Table 3). There was no significant difference of image noise between standard-dose and low-dose CT in every joint (p > 0.05, Table 3). Mean subjective values of image quality ranged from 3.6 to 3.82 and no significant difference was seen in relation to the dosage of the CT scan. The ICCs for measuring subjective image quality between readers showed excellent agreement except for wrist joint scans (fair-to-good agreement, Table 4). The diagnostic performance of each scan was evaluated based on sensitivity, specificity, PPV, NPV and accuracy (Table 5). Sensitivity ranged from 96 to 100%, specificity from 95.2 to 100%, PPV and NPV from 96.9 to 100% and accuracy ranged from 85.7 to 100%. Reader 1 missed a single fracture on standard-dose pelvis CT and reader 2 missed one pelvic fracture (on standard-dose CT), two wrist fractures (one on standard-dose CT and one on low-dose CT) and one ankle fracture (on low-dose CT). There were no statistically significant differences in the sensitivity, specificity or accuracy between standard-dose CT and low-dose CT (p values, 0.1336–1.000, Table 5).
Table 4.
Intraclass correlation coefficients of score for image quality
| Anatomic location | Intraclass correlation | 95% confidence interval | p-value |
|---|---|---|---|
| Shoulder | 0.784 | 0.697–0.849 | <0.001 |
| Pelvis | 0.830 | 0.757–0.883 | <0.001 |
| Ankle | 0.862 | 0.797–0.907 | <0.001 |
| Wrist | 0.537 | 0.387–0.659 | <0.001 |
Table 5.
Diagnostic performance according to anatomic location
| Location | Reader | Sensitivity | Specificity | PPV | NPV | Accuracy |
|---|---|---|---|---|---|---|
| Shoulder standard dose | Reader 1 | 100% | 95.2% | 96.9% | 100% | 98.1% |
| Reader 2 | 100% | 95.2% | 96.9% | 100% | 98.1% | |
| Shoulder low dose | Reader 1 | 100% | 100% | 100% | 100% | 100% |
| Reader 2 | 100% | 100% | 100% | 100% | 100% | |
| p value | 1.000 | 0.5354 | 0.2483 | 1.000 | 0.3250 | |
| 1.000 | 0.5354 | 0.2483 | 1.000 | 0.3250 | ||
| Pelvis standard dose | Reader 1 | 96.0% | 100% | 100% | 95.7% | 97.9% |
| Reader 2 | 96.0% | 100% | 100% | 95.7% | 97.9% | |
| Pelvis low dose | Reader 1 | 100% | 100% | 100% | 100% | 100% |
| Reader 2 | 100% | 100% | 100% | 100% | 100% | |
| p value | 0.2506 | 1.000 | 1.000 | 0.3790 | 0.3008 | |
| 0.2506 | 1.000 | 1.000 | 0.3790 | 0.3008 | ||
| Ankle standard dose | Reader 1 | 100% | 100% | 100% | 100% | 100% |
| Reader 2 | 100% | 100% | 100% | 100% | 100% | |
| Ankle low dose | Reader 1 | 100% | 100% | 100% | 100% | 100% |
| Reader 2 | 97.5% | 100% | 100% | 87.5% | 97.8% | |
| p value | 1.000 | 1.000 | 1.000 | 1.000 | 1.000 | |
| 0.4202 | 1.000 | 1.000 | 0.1336 | 0.3308 | ||
| Wrist standard dose | Reader 1 | 100% | 100% | 100% | 100% | 100% |
| Reader 2 | 95.5% | 100% | 100% | 85.7% | 96.4% | |
| Wrist low dose | Reader 1 | 100% | 88.9% | 97.7% | 100% | 98.0% |
| Reader 2 | 100% | 100% | 100% | 100% | 100% | |
| p value | 1.000 | 0.2485 | 0.3145 | 1.000 | 0.2899 | |
| 0.1667 | 1.000 | 1.000 | 0.2456 | 0.1733 |
NPV, negative predictive value; PPV, positive predictive value.
DISCUSSION
Medical decisions are made by considering the wellbeing of a patient and evaluating potential benefits and risks (such as radiation hazard). Many studies have evaluated low-dose CT in an attempt to decrease patient radiation exposure without loss of diagnostic performance. A recent study of patients undergoing workup for acute appendicitis found that low-dose non-enhanced CT with coronal reformation had sufficient diagnostic performance to be used as the first-line imaging modality.14 Wang et al12 reported that when conducting an MDCT scan for orbital trauma, images acquired using 100 mA tube current (the conventional dose is 300 mA) met the clinical diagnostic requirements, resulting in decreased patient radiation exposure. With regard to extremity imaging, Moritz et al15 demonstrated that ultra-low-dose CT (up to 11 mA) showed sufficient diagnostic performance for fractures, despite the significant radiation reduction. In this study, we used tube current half of standard dose CT and compared scan image quality and diagnostic performance between standard-dose and low-dose CT. Image noise was decreased in low-dose CT with the exception of the shoulder joint images (Table 3). In a study of cervical spinal trauma, Mulkens et al5 reported that low-dose CT increased image noise; however, the increased noise did not affect subjective image quality. We also found no significant difference in subjective image quality between the two imaging methods. The ICC of image quality score for wrist was lower than those for other locations. After reviewing raw data for image quality score of the wrist we found that three cases showed marked different scores (2 points). Whereas, only one case showed the difference of 2 in the image quality score in shoulder and pelvis, respectively and no case showed the difference of 2 in the image quality score in ankle. It is not certain why two readers made different scoring. With regards to the diagnostic performance of low-dose CT, dose reduction did not affect its diagnostic performance for fracture detection, although a single ankle fracture was missed on low-dose CT by reader 2 (Table 5). However, a total of four fractures were missed in the standard-dose CT group. Missed fracture cases were thus presumed to be too faint to perceive even on standard-dose CT (Figure 2). We think that the difficulties associated with diagnosing fractures are associated with characteristics of the fracture itself rather than simply CT image quality. It is likely that the image quality of CT scans can be affected, not only mechanical factors, such as mAs or kVp, but also by biological factors, like bone density or soft tissue thickness. Therefore, individualization of the radiation dose for optimization of image quality and minimization of radiation risk could be beneficial for both patients and radiologists.
Our study had some limitations. First, the analysis was performed retrospectively. Second, some cases were not confirmed surgically; patients were carefully diagnosed based on thorough physical examination and symptoms. The third limitation was that this study did not include micro-fracture cases, which are challenging to diagnose on CT scan.
In conclusion, low-dose CT of the extremities (shoulder, pelvis, ankle and wrist) can reduce radiation dose by about 50% compared with standard-dose CT and does not significantly affect image quality or diagnostic performance in fracture detection.
Contributor Information
Jung Woo Yi, Email: yijw8282@gmail.com.
Hee Jin Park, Email: parkhiji@gmail.com.
So Yeon Lee, Email: capella27@gmail.com.
Myung Ho Rho, Email: rmh96@dreamwiz.com.
Hyun Pyo Hong, Email: summersonrad@naver.com.
Yoon Jung Choi, Email: yoonchoi99@gmail.com.
Mi Sung Kim, Email: misung70@gmail.com.
References
- 1.Lubovsky O, Liebergall M, Mattan Y, Weil Y, Mosheiff R. Early diagnosis of occult hip fractures MRI versus CT scan. Injury 2005; 36: 788–92.https://doi.org/10.1016/j.injury.2005.01.024 [DOI] [PubMed] [Google Scholar]
- 2.Gill SK, Smith J, Fox R, Chesser TJS. Investigation of Occult hip fractures: the use of CT and MRI. Scientific World J 2013; 2013: 1–4.https://doi.org/10.1155/2013/830319 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Markhardt BK, Gross JM, Monu JU. Schatzker classification of tibial plateau fractures: use of CT and MR imaging improves assessment. Radiographics 2009; 29: 585–97.https://doi.org/10.1148/rg.292085078 [DOI] [PubMed] [Google Scholar]
- 4.Dodd A, Oddone Paolucci E, Korley R. The effect of three-dimensional computed tomography reconstructions on preoperative planning of tibial plateau fractures: a case-control series. BMC Musculoskelet Disord 2015; 16: 144.https://doi.org/10.1186/s12891-015-0608-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Mulkens TH, Marchal P, Daineffe S, Salgado R, Bellinck P, te Rijdt B, et al. Comparison of low-dose with standard-dose multidetector CT in cervical spine trauma. AJNR Am J Neuroradiol 2007; 28: 1444–50.https://doi.org/10.3174/ajnr.A0608 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Brenner DJ, Hall EJ. Computed tomography--an increasing source of radiation exposure. N Engl J Med 2007; 357: 2277–84.https://doi.org/10.1056/NEJMra072149 [DOI] [PubMed] [Google Scholar]
- 7.Diederichs CG, Engelke WG, Richter B, Hermann KP, Oestmann JW. Must radiation dose for CT of the Maxilla and mandible be higher than that for conventional panoramic radiography? AJNR Am J Neuroradiol 1996; 17: 1758–60. [PMC free article] [PubMed] [Google Scholar]
- 8.Dammert S, Funke M, Merten HA, Obernauer S, Grabbe E. Multislice helical CT (MSCT) for mid-facial trauma: optimization of parameters for scanning and reconstruction. Rofo 2002; 174: 874–9.https://doi.org/10.1055/s-2002-32682 [DOI] [PubMed] [Google Scholar]
- 9.Bohy P, de Maertelaer de V, Roquigny A, Keyzer C, Tack D, Gevenois PA. Multidetector CT in patients suspected of having lumbar disk herniation: comparison of standard-dose and simulated low-dose techniques. Radiology 2007; 244: 524–31.https://doi.org/10.1148/radiol.2442060606 [DOI] [PubMed] [Google Scholar]
- 10.Connor SE, Arscott T, Berry J, Greene L, O'Gorman R. Precision and accuracy of low-dose CT protocols in the evaluation of skull landmarks. Dentomaxillofac Radiol 2007; 36: 270–6.https://doi.org/10.1259/dmfr/90016954 [DOI] [PubMed] [Google Scholar]
- 11.Lutz J, Jäger V, Hempel MJ, Srivastav S, Reiser M, Jäger L. Delineation of temporal bone anatomy: feasibility of low-dose 64-row CT in regard to image quality. Eur Radiol 2007; 17: 2638–45.https://doi.org/10.1007/s00330-007-0578-1 [DOI] [PubMed] [Google Scholar]
- 12.Wang JW, Tang C, Pan BR. Data analysis of low dose multislice helical CT scan in orbital trauma. Int J Ophthalmol 2012; 5: 366–9.https://doi.org/10.3980/j.issn.2222-3959.2012.03.22 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Rosner B. Fundamentals of biostatistics. Belmont, CA: Duxbury Press; 2005. [Google Scholar]
- 14.Yun SJ, Kim HC, Yang DM, Kim SW, Rhee SJ, Shin JS, et al. Diagnostic usefulness of Low-Dose Nonenhanced Computed tomography with Coronal reformations in patients with suspected Acute appendicitis: a comparison with Standard-Dose computed tomography. J Comput Assist Tomogr 2016; 40: 485–92.https://doi.org/10.1097/RCT.0000000000000381 [DOI] [PubMed] [Google Scholar]
- 15.Moritz JD, Hoffmann B, Sehr D, Keil K, Eggerking J, Groth G, et al. Evaluation of ultra-low dose CT in the diagnosis of pediatric-like fractures using an experimental animal study. Korean J Radiol 2012; 13: 165–73.https://doi.org/10.3348/kjr.2012.13.2.165 [DOI] [PMC free article] [PubMed] [Google Scholar]