

Abstract
Despite efforts to operationalize the nicotine dependence syndrome among adolescents, little is known regarding the relative severity of dependence symptoms assessed by different measures. The current study utilized a nonparametric item response model to assess the unidimensionality of the nicotine dependence construct and relative severity of dependence symptoms characterized by the Hooked on Nicotine Checklist (HONC) and the modified Fagerström Questionnaire (mFTQ) in a sample of 109 adolescent smokers (58% female) participating in a prospective investigation of smoking self-change efforts. It was hypothesized that symptoms assessed by the HONC would be associated with lower levels of nicotine dependence severity than symptoms assessed with the mFTQ. Results indicated that HONC and mFTQ items could be linked to a single latent construct. Most HONC items captured variability at the lower range and mFTQ items made discriminations at the middle and higher end of the dependence severity continuum. Findings suggest the HONC and mFTQ may provide complementary information in assessing nicotine dependence levels in adolescent regular smokers and have implications for symptoms expression in youth.
Keywords: Adolescents, nicotine dependence symptoms, symptoms expression, item-response modeling
1. Introduction
Adolescent smoking remains a major public health problem given the persistence of this behavior into adulthood. Progression to levels of smoking associated with symptoms of nicotine dependence have been reported to occur within weeks of onset of occasional smoking in youth (DiFranza et al. 2000, 2002). In concert with seminal reviews highlighting the dearth of gold standard assessments and clear conceptualization of nicotine dependence among adolescents (Colby, Tiffany, Shiffman, & Niaura, R.S., 2000a,b; Shadel, Shiffman, Niaura, Nichter, & Abrams, 2000), several measures have been revised or developed with the intention of better characterizing the youth nicotine dependence syndrome (e.g., mFTQ (Prokhorov, Pallonen, Fava, Ding, & Niaura, 1996); NDSS (Clark et al., 2005); ANDI (Cohen, Kelly, & Myers, 2002); HONC (DiFranza et al., 2002)). With few exceptions (Strong, Brown, Ramsey & Myers, 2003; Strong et al., 2007), there has been limited examination of the extent to which such measures may work in conjunction to assess overlapping or varied levels of a common nicotine dependence syndrome. Better understanding of the interrelationships among different nicotine dependence measures can increase understanding of the ordering of symptom development and which symptoms may be most relevant to the expected levels of nicotine dependence in a given sample of youth (Shadel et al., 2000).
Efforts to determine which among the multiple measures of nicotine dependence in youth may be considered ‘superior’ to another in its psychometric properties has typically relied on classical test theory estimates, such as internal consistency or test-retest reliability (e.g., Wellman, Pbert, & DiFranza, 2006a; Wellman et al., 2006b), and correlational approaches to examine convergent validity across measures (e.g., Cohen et al., 2002; Kandel et al., 2005). Studies investigating the convergence of nicotine dependence measures among adolescents have focused primarily on the two most widely used measures of nicotine dependence, the mFTQ (Prokhorov et al., 1996) and assessments derived from DSM-IV dependence criteria (Cohen et al., 2002; Kandel et al., 2005). Findings vary but have generally indicated low concordance across these measures, which may reflect that different aspects of dependence are measured by the mFTQ versus DSM-IV-based criteria (Hughes et al., 2004; Kandel et al., 2005). However, traditional correlational approaches may provide inconsistent results from direct comparison of the same measures across samples with divergent levels of nicotine dependence. Further, use of summary statistics (e.g., internal consistency reliability estimates) provides an evaluation of measure reliability reflecting average performance across all levels of dependence, rather than illustrating where on the continuum the measure performs best. These limitations have resulted in a move toward methods based on item-response theory (IRT; c.f. Lord, 1980; Rasch, 1960) to compare the relative severity and overlap of nicotine dependence measures by separating items from the scales and linking them together using a latent measurement model (e.g., Orlando, Sherbourne, & Thissen, 2000). Methods based on IRT provide a means of establishing a common metric across disparate scales and provide a method for direct comparison of all individual symptoms to a common latent construct of nicotine dependence.
The few studies to date that have utilized IRT models to examine the relative severity of nicotine dependence symptoms among youth (Strong et al., 2003, 2007) provide important information for where along an underlying nicotine dependence continuum specific symptoms might be observed. In an initial study, Strong and colleagues (2007) demonstrated that the mFTQ and DSM-IV based criteria could be organized along the same single latent nicotine dependence syndrome among adolescent smokers. Results suggested that behavioral and cognitive symptoms of dependence (e.g., smoking more after unable to smoke, want to cut down but could not) occurred in the lowest range of nicotine dependence; core physiological symptoms (e.g., smoking within 30 minutes of waking) were in the middle range of nicotine dependence severity; and symptoms reflecting organization of behavior around smoking (e.g., missing school because of smoking) and more severe physical dependence (e.g., smoking more in the first two hours of the day) were observed at the highest end of the continuum. In particular, physiological symptoms assessed by the mFTQ captured variation in nicotine dependence from the middle to upper end of the severity continuum, while a number of the more cognitive and behavioral DSM-IV criteria captured variability below the least severe symptom of the mFTQ. Given the increasing numbers of nicotine dependence measures developed for youth, it would be useful to continue to examine how particular symptoms are relevant to specific levels of nicotine dependence and the extent to which recently developed and more established measures provide unique information about the nature of nicotine dependence in youth (Colby et al. 2000b; Shadel et al., 2000).
The Hooked on Nicotine Checklist (HONC; DiFranza et al., 2002) is one recently developed measure proposed to assess the onset of nicotine dependence among adolescents, based on a concept of ‘loss of autonomy’ over tobacco use. The first 6 items on the HONC represent primarily cognitive and behavioral aspects of dependence, while the remaining 4 items inquire about withdrawal symptoms when trying to stop smoking or being unable to smoke. The HONC total score has been found to correlate with maximum smoking quantity and frequency, duration of tobacco use, age at first use (DiFranza et al., 2002; Wellman et al., 2006b) and smoking behavior at 6 and 12-months following assessment (Wellman et al., 2006b) among adolescents. Although published data on the dimensionality of the HONC among adolescents is limited, a factor analysis of the HONC among youth who had ever used tobacco produced a primary factor accounting for 66% of the total variance (DiFranza et al., 2002). Additionally, a factor analysis of the HONC in a large sample of adult smokers indicated it was primarily unidimensional (Wellman et al., 2006a).
We identified only two studies in the published literature that examined the concordance of the full HONC scale with another measure of nicotine dependence among youth. Wellman et al. (2006b) indicated a relatively strong relationship (r=.83) between the HONC and the mFTQ while O’Loughlin and colleagues (2002) found youth who endorsed one symptom on the HONC to have a higher mean Stanford Dependence Index score (a modified version of the mFTQ) than those youth who endorsed no symptoms on the HONC (O’Loughlin, Kishchuk, DiFranza & Paradis, 2002). However, the HONC has not been previously evaluated concurrently with the mFTQ to identify which symptoms are associated with relatively lower or higher levels of nicotine dependence.
The HONC was designed to be developmentally sensitive to the onset of nicotine dependence (DiFranza et al., 2002) and thus would be expected to capture variability at the lower end of dependence continuum. Endorsement of at least one HONC item is relatively high in samples with limited smoking experience. For example, in a study of youth, 50% of occasional smokers and 100% of current smokers endorsed at least one HONC item (Wheeler, Fletcher, Wellman, & DiFranza, 2004), indicating the relatively low threshold for endorsing a given item on this measure. However, variability in the rates of endorsement across specific HONC items, particularly among youth with a very low level of tobacco exposure (DiFranza et al., 2007), suggests the measure’s potential to capture variations in lower levels of nicotine dependence. Conversely, the mFTQ, originally derived from an adult model of dependence, validated on more heavily smoking adolescents (Prokhorov et al., 1996) and focused on physiological dependence symptoms, would be expected to capture variability in a more severe end of a nicotine dependence syndrome (Kandel et al., 2005; Strong et al., 2007). The addition of low level symptoms of dependence severity from the HONC such as ‘ever feeling’ a desire for a cigarette might complement the mFTQ by adding potential symptoms below levels assessed by the mFTQ. Further, anchoring concepts such as ‘loss of autonomy’ or items describing ‘feeling hooked’ on nicotine in the context of established measures’ thresholds will better place those categorized as dependent by each HONC and mFTQ method.
1.1 Current Study
The aim of the current study was to examine the extent to which symptoms on the HONC and the mFTQ could be disaggregated from the respective measures and linked concurrently to a unidimensional latent nicotine dependence construct among a sample of adolescent established smokers. Thus we examined the relative severity of symptoms measured by the HONC and the mFTQ. We purposefully chose a sample of adolescents with established smoking experience to ensure the middle and upper ranges of nicotine dependence are represented as well as to examine the utility of the HONC items in adolescents with more than minimal smoking exposure. It is expected that the majority of symptoms assessed by the HONC, which tend to cover more global lifetime experiences of cognitive symptoms (e.g., have you ever felt like you really needed a cigarette?) and that have been previously identified as relatively low severity behavioral symptoms (e.g., difficulty cutting down or quitting) will be observed at a lower level of severity of a nicotine dependence syndrome (Brandon, Herzog, Irvin & Gwaltney, 2004; Kandel et al., 2005). In contrast, it was expected that the behavioral and physical symptoms measured with the mFTQ, will capture variability in the middle to upper ends of a latent nicotine dependence continuum in youth (Prokhorov et al., 2000; Strong et al., 2007).
2. Methods
2.1 Procedure
This study employed baseline data from a sample of 14 to 18 year old adolescent smokers (N = 109) participating in a longitudinal study of adolescent smoking cessation self-change. Data were collected through a combination of in-person structured interviews and self-report questionnaires. One hundred and nine adolescents were recruited from four high schools in metropolitan San Diego. Criteria for subject inclusion in the present study were: 1) 14-18 years of age and 2) having smoked a cigarette in the prior 30 days. Participants were recruited for the study with a combination of passive (e.g., advertisements on campuses) and active (e.g., presenting the study during homerooms) recruitment methods. Informed consent (assent for minors under age 18) was obtained from parents and adolescent participants. So as to maintain confidentiality, parents were not informed of their child’s smoking status during the consent procedure. As an incentive for participation, each participant received a $25 gift certificate for participation in the baseline assessment.
The included participants were on average 16.8 years of age (SD = 1.1; range 14.3 - 18.8), 58% (n = 63) were females, and 71% were White, 10% Hispanic, 6% Asian-American, 12% of Mixed background (primarily White & Hispanic) and 1% of other ethnicity. See Table 1 for sample smoking history and correlations with nicotine dependence measures.
Table 1.
Sample Smoking Characteristics and correlations with mFTQ and HONC scale scores.
| Smoking Characteristics | HONC total score | mFTQ total score | |
|---|---|---|---|
| Length of smoking history in years (M(SD)) | 3.63 (1.89) | .19a | .16 |
| Established smokers - smoked 100 cigarettes in lifetime (%) | 95.4 | ||
| Past 30-day cigarettes per smoking day (M(SD)) | 6.03 (5.48) | .51b | .65b |
| Daily smokers (%) | 40.4 | .48b | .47b |
| Lifetime quit attempts (% yes) | 68.8 | .21a | .01 |
| HONC total score (M(SD)) | 6.02 (3.30) | NA | NA |
| mFTQ total score (M(SD)) | 4.00 (2.01) | .53b | NA |
p<.05
p<.01
2.2 Measures
2.2.1 Smoking Characteristics. Teen Smoking Questionnaire (TSQ; Myers, Brown, & Kelly, 2000)
The TSQ is a semi-structured interview that assesses smoking history (e.g., age at smoking initiation, lifetime cessation efforts), from which smoking characteristics and history of the present sample were obtained. The Time-line Follow-back procedure (TLFB; Sobell & Sobell, 1992) was employed to gather information regarding cigarette and other tobacco product quantity and frequency of use during the 90-day interval preceding the baseline interview. Information was collected using a calendar format to provide temporal cues (e.g., holidays) to assist in recall. The TLFB has been shown to have good reliability and validity with adolescent smokers (Lewis-Esquerre et al., 2005). Baseline 30-day cigarette smoking quantity/frequency (QF) was computed as the average number of cigarettes smoked per smoking day across the 30 days prior to baseline.
2.2.2 Modified Fagerström Tolerance Questionnaire (mFTQ; Prokhorov et al., 1996)
The 7-item mFTQ, for which initial reliability and validity have been demonstrated with adolescent smokers (Prokhorov et al., 1996; Prokhorov, Koehly, Pallonen, & Hudmon, 1998) was employed as one measure of nicotine dependence. The mFTQ was administered via in-person interview as part of the TSQ (Myers et al., 2000). The mFTQ was derived from the original Fagerström Tolerance Questionnaire (Fagerström, 1978), a measure designed to assess physiological tolerance to nicotine. Previous psychometric analyses have supported the mFTQ as measuring a unidimensional construct (Prokhorov et al., 1996; Prokhorov et al., 2000) that correlates with smoking frequency, number of cigarettes per day, and salivary cotinine (Prokhorov et al., 1996, 2000). Internal consistency estimates from previous studies for the mFTQ have ranged from 0.71 to 0.75 (Prokhorov et al., 1996, 2000). The coefficient alpha in the current sample was 0.62.
2.2.3 Hooked on Nicotine Checklist (HONC; DiFranza, et al., 2002)
In the present study, the HONC was completed by self-report. The 10-item dichotomously scored HONC was originally developed to assess nicotine dependence as conceptualized through a blend of self-medication theory, negative reinforcement theory, and incentive sensitization theory (DiFranza et al., 2002). Previous research has indicated a unidimensional structure to the HONC (DiFranza et al., 2002), and evidence exists for the measure’s concurrent and predictive validity (e.g., DiFranza et al., 2002; Wellman et al., 2006). Internal consistencies of the HONC from previous studies of adolescents with a variety of smoking behavior range from .90 (O’Loughlin, Tarasuk, DiFranza, & Paradis, 2002) to .94 (DiFranza et al., 2002). Scoring of the HONC has consisted of two methods: 1) total scale score as an indicator of level of nicotine dependence, and 2) endorsement of at least one item as an indicator of “loss of autonomy” over tobacco use (DiFranza et al., 2002; Wheeler et al., 2004). The coefficient alpha in the current sample was .89. Notably, 95.5% of the current sample endorsed at least one item on the HONC.
3. Data Analyses
3.1 Unidimensionality of the HONC & mFTQ
Prior to evaluating individual item response probabilities, we evaluated the assumption that items of the HONC and mFTQ collectively measure a single, latent “nicotine dependence” construct (Panter & Reeve, 2002). Although strict unidimensionality is not assumed (c.f. Stout, 1987), we evaluated whether the first factor was significantly larger than subsequently extracted factors. Because items are dichotomously scored on the HONC and were dichotomized for the mFTQ based on previous IRT analysis of this measure in adolescent smokers (Strong et al., 2007), exploratory factor analysis (EFA) was conducted in Mplus (Muthen & Muthen, 1998-2001) using the Robust Weighted Least Squares method of factor extraction. Eigenvalues, the ratio of the first to second eigenvalues, and the interpretability of additional factors were used to determine the strength of the primary factor (Fabrigar, Wegener, MacCullum, & Strahan, 1999; Floyd & Widaman, 1995). The cutoff for determining whether or not an item substantively contributed to a primary factor was set at a loading of 0.3 (Floyd & Widaman, 1995).
3.2 Item Response Models
Several IRT models exist for the analysis of psychometric properties of self-report measures that use dichotomous response formats. IRT methods provide a means of scaling both items and persons along a theorized underlying latent continuum (Panter & Reeve, 2002) and allow individual symptoms from different measures to be placed on a common metric for comparison. Methods based on item response theory have been successfully used to model the relative severity of DSM-IV and mFTQ symptoms to a latent nicotine dependence construct among adolescent heavy smokers (Strong et al., 2007). IRT methods allow examination of how the probability of choosing each option for each HONC and mFTQ item vary in relation to individual levels of nicotine involvement. We examined these response probabilities by constructing option characteristic curves (OCCs) for each item. OCCs allow for both the inspection of item performance and the examination of how particular item contents are endorsed differently across the continuum of nicotine dependence. IRT models differ primarily in the method of estimating the OCCs.
To examine item characteristics, we used a nonparametric kernel-smoothing method and software (TestGraf) developed by Ramsay (2000). These methods have been used previously in a paper on the DSM-IV nicotine dependence and modified Fagerstrom Tolerance Questionnaire (mFTQ) symptoms in adolescent heavy smokers with comorbid psychopathology (Strong, Brown, Ramsey, & Myers, 2003) as well as in several papers on scales for measuring depression (Santor & Coyne, 1997, 2001; Santor, Zuroff, Ramsay, Cervantes, & Palacios, 1995) and depression-related cognitions (Beevers, Strong, Meyer, Pilkonis, & Miller, 2007). We chose not to use a parametric models for the OCCs because, although mFTQ symptoms have been previously analyzed with a parametric (Rasch) model (Strong et al., 2007), we had no a priori reasons to expect a particular form for response distributions among HONC items and wanted to allow for OCCs with nonmonotonic functions to be revealed. Compared to parametric IRT models, nonparametric IRT models do not impose a specific form on the item response function, can be used with relatively small sample sizes as in the present study, and can estimate item characteristics more easily (Meijer & Baneke, 2004). Individuals are ranked according to total scores across the mFTQ and the HONC, and these ranks are then converted to standard normal scores. OCCs are then constructed across a specified number of evaluation points within these standard normal scores by using a nonparametric smoothing kernel (Ramsay, 1991). This approach estimates OCC at each evaluation point by using a local average, a method that gives observations increased influence in determining the estimated OCC values if they fall closer to the specific evaluation point. This method is particularly useful when the relationship between response probabilities and nicotine dependence operates asymmetrically.
4. Results
4.1 Unidimensionality
We conducted exploratory factor analysis with Robust Weighted Least Squares method of factor extraction of the seven symptoms of the mFTQ and the ten symptoms of the HONC. Results supported a primary dimension that was substantially larger than subsequent factors. The first factor accounted for 55% of the common variance, with the second and third factors extracted accounting for 9.8% and 8.4% of the variance, respectively. The first eigenvalue was 9.27, which was substantially larger than the eigenvalues of the second and third factors (1.67 and 1.42). Generally, factors with eigenvalues of less than two units will have modest impact on a measure with multiple items because such a dimension would have less than the strength of two items. All items had loadings greater than .30 on the primary factor except for the mFTQ item ‘how soon after waking’ which had a loading of .27. However, this item was retained for further inspection due to prior findings that it mapped a nonoverlapping region of the nicotine dependence continuum as measured by the mFTQ in a sample of youth (Strong et al., 2003).
4.2 Item Response Analysis
In linking the 17 items on a common dimension, TESTGRAF was used first to analyze all items simultaneously. From this initial analysis, TESTGRAF was then used to compute a score for each adolescent using maximum likelihood estimation, conditional on the item characteristic curves computed in the initial step. These scores were used to anchor subsequent analysis of the 10 HONC items and 7 mFTQ items, respectively. By anchoring the score for each adolescent, the computation of estimates for the item characteristic curves will be generated using the same level of reliability in the trait estimates across HONC and mFTQ analyses1.
Using the estimates obtained from the IRT analyses, we examined item characteristic curves (ICCs) for adolescents in the present sample to assess each item’s overall ability to discriminate among the levels of nicotine dependence (see Figure 1). ICCs were constructed by plotting the expected item score (0 = absent, 1 = present) across maximum likelihood estimates of dependence levels generated during initial analyses with all 17 items. Figure 1 displays the ICCs for all 17 items. The dichotomous format of the HONC items and dichotomized format of the mFTQ items allows items to be characterized by ICCs alone; thus option characteristic curves (OCCs) are not presented. In figure 1, each symptom is estimated as more likely to be present than absent when the ICC crosses the midpoint (.50) of the y-axis. Effective items were expected to have ascending sloped curves reflecting that individuals with higher expected total scores were increasingly likely to agree to statements reflecting increasing levels of nicotine dependence.2
Figure 1.
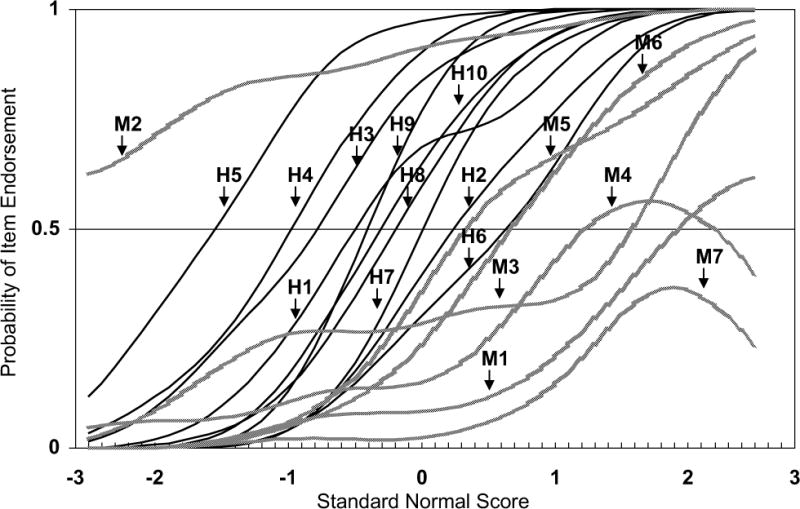
Item characteristic curves for the HONC and the mFTQ
Note: Item characteristic curves are labeled according to the measure to which they correspond (H= HONC; M=mFTQ) and to the item number (HONC items 1-10; mFTQ items 1-7).
4.3 Ability of mFTQ and HONC items to discriminate among levels of nicotine dependence
Three of the mFTQ items demonstrated adequate discrimination in the present sample: “how soon after waking” (item 3), “difficulty to refrain” (item 5), and “smoke if ill in bed” (item 6). Thus, as the estimated level of nicotine dependence increased, the likelihood of endorsing each of these items generally increased as expected. Similar to previous IRT analyses of the mFTQ in adolescent smokers (Strong et al., 2003, 2007), the “inhale” item (item 2) demonstrated poor discrimination, with the ICC remaining relatively flat across the estimated levels of nicotine dependence. In the present sample, a few of the mFTQ items also only discriminated at the higher end of the nicotine dependence continuum. Both “which hate to give up” (item 4) and “smoke more in first two hours” (item 7) demonstrated little discrimination until approximately the 90th and 69th percentiles, respectively, at which time the probability of endorsing these items quickly increased. However, the downward sloping of both items at the highest end of the nicotine dependence continuum suggests that there were likely fewer adolescents in the present sample at the highest range of dependence, and thus less data defining the curve location. Surprisingly, “cigarettes per day” (mFTQ item 1) also demonstrated little discrimination until the 98th percentile in this sample of youth.
After rank-ordering adolescents in the present study, we found that as estimated levels of nicotine dependence increased, the probability of each HONC item being endorsed as present also increased for the majority of the HONC items (see Figure 1). HONC items “smoke now because hard to quit” (item 2), “felt addicted” (item 3), “strong cravings” (item 4), “felt like really needed a cigarette” (item 5), “smoke in places” (item 6), “when quit, become more irritable” (item 8), and “when quit, become more nervous, restless, and anxious” (item 10) all appeared to perform similarly, as indicated by the relatively equal levels of discrimination across their respective ICCs. HONC items 7 and 9 (“when quit hard to concentrate” and “when quit, had strong urges”, respectively) had ICCs that were slightly more discriminating than the other HONC items. Finally, HONC item 1, “ever tried to quit but couldn’t” appeared to be more discriminating in the lower range of nicotine dependence but relatively less discriminating through the middle to higher range of estimated nicotine dependence. It is possible that the compound nature of this item in which a “no” response could either indicate that the adolescent “never tried to quit at all” or that the adolescent “tried to quit and was successful at one point” could influence how youth are responding to it at varying levels of nicotine dependence.
4.4 Relative severity of mFTQ and HONC symptoms
As can be seen in Figure 1, with the exception of the mFTQ “inhale” item, the majority of the mFTQ items capture variation at the more severe end of the nicotine dependence continuum. Specifically, all items on the mFTQ except for the “inhale” item discriminated above the 65th percentile, indicating that the measure captured no variation in the less severe end of a nicotine dependence construct. In contrast, and consistent with expectations, the HONC items tend to be relatively less severe, discriminating mostly through the middle range of the estimated nicotine dependence continuum. However, few items were found to discriminate in the lower range of dependence. In terms of coverage of the nicotine dependence continuum, items from the HONC were better targeted to the levels of dependence observed in this sample, but provided little information about the highest or lowest levels of dependence severity. This is exemplified by the majority of HONC items making discriminations between the 18th and 50th percentile and no HONC item discriminating above the 75th percentile. There was also significant overlap of items along the continuum, suggesting that a number of items did not map unique regions of the dependence continuum. For example, six HONC items discriminated between approximately the 25th and 50th percentile (items 3, 9, 1, 10, 8, and 7), yet only two items discriminated below the 25th percentile. As expected, HONC item 5 (ever felt like you really needed a cigarette) represented the item with the lowest severity yet interestingly covered a unique region of the dependence continuum. Although mFTQ items discriminated at the most severe end of the continuum, no items provided coverage between the 75th and 90th percentile, with only three mFTQ items (items 4, 3, and 1) discriminating above the 90th percentile. HONC items 1 and 9 as well as HONC item 6 and mFTQ item 6, discriminated at the exact same point along the nicotine dependence continuum and thus were completely redundant in terms of information provided.
4.5 Test Reliability
The combined HONC & mFTQ was maximally reliable in the second quartile with reliability estimates ranging from .75 to .77 from the 25th to the 50th percentile. Reliability estimates steadily decreased from .75 to .67 between the 25th and 5th percentile and slightly more rapidly decreased from .75 to .59 from the 50th to the 95th percentiles. See Figure 2.
Figure 2.
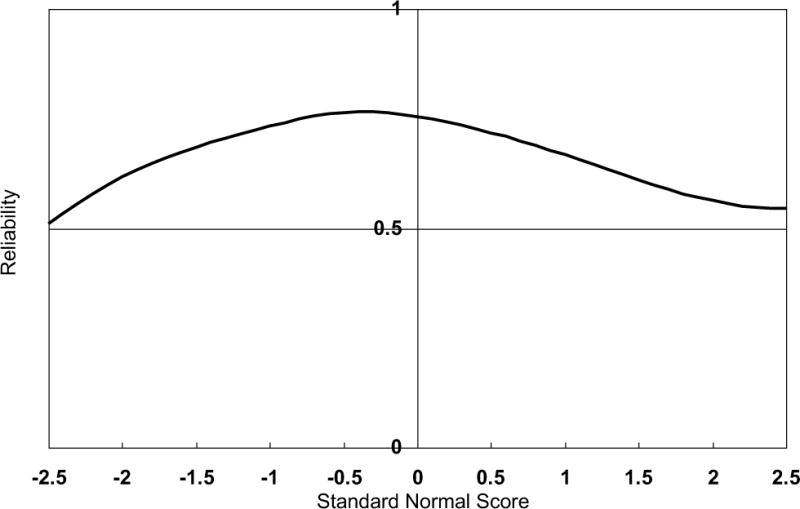
Test reliability of the combined HONC and mFTQ
5. Discussion
The present study was designed to examine the extent to which symptoms assessed by the HONC and mFTQ could be disaggregated from their respective measures and linked to a common underlying nicotine dependence syndrome. Nonparametric IRT analyses supported the ability to link symptoms of both measures to a unidimensional latent construct in a sample of adolescents established smokers. Consistent with expectations, results also suggested that HONC and mFTQ symptoms represented complementary indicators of nicotine dependence severity with relatively minimal overlap across the two measures. Three of the seven symptoms of the mFTQ provided adequate discrimination across the nicotine dependence construct in the current sample, with discriminations occurring at the middle to higher end of the severity continuum. Alternatively, seven of the ten HONC indicators provided adequate, although relatively equivalent and overlapping discriminations through the middle range of nicotine dependence with minimal coverage at the lower or higher ends of a severity continuum. Items of the HONC were generally better-matched to the nicotine dependence severity of the current sample than those of the mFTQ. However, findings suggest clear room for improving our coverage of all levels of a nicotine dependence syndrome in adolescent regular smokers.
Symptom expression as a function of level of dependence was relatively consistent with expectations. More general cognitive and behavioral symptoms were observed at lower levels of severity, while core physiological symptoms corresponded with the mid to upper range of severity. In particular, relative ordering of the mFTQ item severities in the current sample was equivalent to those identified with Rasch analyses (Strong et al., 2007), with the exception of “smoking if ill in bed” which was a relatively lower severity item in the current sample than in Strong et al. (2007). In the present study, all mFTQ items captured information at greater levels of nicotine dependence severity than items on the HONC, with the exception of the HONC item “difficult to refrain from smoking in places” which is equivalent in content to the mFTQ item “hard to keep from smoking in places.” Make point 3 about HONC6 & mFTQ5 overlap here? HONC items inquiring about “ever” experiencing certain cognitive symptoms such as needing a cigarette, cravings, and feeling addicted captured the lowest level of severity as expected given the more global nature of and greater temporal period covered by these items. In particular these items were endorsed by more than 72% of the current sample although only “needing a cigarette” captured information in a unique area of the nicotine dependence continuum. HONC items inquire about quit experiences as well as withdrawal symptoms (e.g., nervousness, difficulty concentrating) by cueing the adolescent to respond to the items in the scenario where he or she was trying to stop smoking or was unable to smoke for a period of time. These contextualized inquiries about the expected effects of interrupting smoking captured information at a greater level of severity than the more global cognitive symptoms (e.g., ever felt like needed a cigarette, ever felt addicted) but of less severity than the report of experienced physical symptoms assessed by the mFTQ. Such findings are consistent with previous studies in which withdrawal symptoms were observed at the middle range of a dependence continuum youth (Strong et al., 2003, 2007) and further speak to the importance of framing questions so that they link adolescent experiences with smoking to specific situations and behaviors (MacPherson, Myers, & Johnson, 2006; Mermelstein et al., 2002).
Although these initial findings are supportive of the measurement properties of the HONC, one potential concern is the authors’ suggested use of positive endorsement of any single item on the HONC as indicative of a ‘loss of autonomy’ over tobacco use (DiFranza et al., 2002). This approach presumes that all items of the HONC are of equal severity in assessing an underlying nicotine dependence syndrome. However, our present analyses indicate some variability in the range of dependence severity across specific HONC symptoms. For example, ‘ever really felt a need for a cigarette’, ‘tried to quit but couldn’t,’ and ‘smoke now because it is hard to quit’ mapped to different levels of dependence severity in the current sample. If these results hold, this single-item threshold includes teens who report many more severe symptoms, such as physiological dependence, but labels them similarly to youth with very low levels of dependence, such as those who report at minimum that they ever felt they really needed a cigarette, the lowest severity HONC item in the present study. Thus, a significant amount of information may be lost when grouping those with only the lowest levels of dependence with youth who report many symptoms.
While HONC and mFTQ symptoms may capture variability at complementary areas of the nicotine dependence continuum, substantial redundancy among items was observed. This finding suggests the need for identifying items that will improve coverage of the adolescent nicotine dependence construct. For example, in the present sample few items provided discriminations at the most and least severe ends of the dependence continuum, with the majority of symptoms representing the middle range of dependence severity. Reducing redundancy among symptoms used to measure dependence can thus increase the efficiency of assessing this construct. Further evaluation of symptom expression based on various measures of nicotine dependence will improve our ability to adequately and efficiently capture a commonly defined nicotine dependence continuum in youth.
4.1 Limitations
There are limitations in the present study worth noting. The current sample was relatively small and homogenous, in that the majority were established smokers with a substantial percentage of daily smokers. The relatively small size of the sample may have impacted the reliability of the correlation coefficients used to estimate the factor analytic model in the current study (Tabachnick & Fidell, 2001). Also, it remains unknown if differences in administration of the two dependence measures affected rank ordering of individuals or item discriminations. Despite this concern we were able to link items from both measures to a single latent continuum. These considerations, along with the preliminary nature of thestudy, the present findings should be replicated in larger samples of youth with a wider range of smoking experience. Future studies should also attempt to replicate our current findings with parametric models. We chose a nonparametric IRT model because we had no a priori assumptions regarding the shapes of the item characteristic curves of the HONC items. However, our findings suggest potential fit of the HONC items to a parametric model. Given that previous studies have fit a parametric model to mFTQ symptoms in youth (Strong et al., 2007), linking both measures to common latent continuum with such a model is a logical next step.
4.2 Conclusion
To our knowledge this is the first study to examine concurrently the relative severity of nicotine dependence symptoms assessed by the HONC and the mFTQ in a sample of adolescents. By placing these measures on a common metric, we were able to assess the construct of nicotine dependence using symptoms disaggregated from two commonly used scales. The current study contributes to the growing literature indicating cognitively mediated and behavioral regulatory symptoms are particularly relevant to lower to mid levels of nicotine dependence with core physiological symptoms and organization of behavior around smoking occurring at mid to higher levels of dependence among youth (DiFranza et al., 2007; Kandel et al., 2005; Strong et al., 2007). Additionally, our findings suggest that both the mFTQ and HONC provide complementary information about nicotine dependence in a sample of regular smoking youth. As such, more efficient assessment of the dependence construct could be achieved by removing redundant items both within and across measures while simultaneously incorporating new items or items from other measures to more adequately characterize the full continuum of dependence in adolescence (Sledjeski et al., 2007). As both empirical (e.g., Strong et al., 2007) and conceptual (e.g., Tiffany et al., 2004) arguments are increasingly made for a dimensional approach to the assessment of nicotine dependence in youth, continued examination of the unique information provided by items from more established and recently developed measures will improve our understanding of the development of nicotine dependence in this vulnerable group.
Table 2.
Item characteristics: Endorsement, Severity Parameters, Percentile of Discrimination
| Measure | Item | % endorsed | Pseudo severity | Percentile |
|---|---|---|---|---|
| mFTQ2 | Do you inhale? | 89.0 | NA | NA |
| HONC5 | Have you ever felt like you really needed a cigarette? | 87.2 | −1.5 | 6.7 |
| HONC4 | Do you ever have strong cravings to smoke? | 78.0 | −0.9 | 18.4 |
| HONC3 | Have you ever felt like you were addicted to tobacco? | 72.5 | −0.7 | 24.2 |
| HONC9a | Did you feel a strong need or urge to smoke? | 63.3 | −0.4 | 34.5 |
| HONC1 | Have you ever tried to quit but couldn’t? | 59.6 | −0.4 | 34.5 |
| HONC10a | Did you feel nervous, restless or anxious because you couldn’t smoke? | 58.7 | −0.4 | 38.2 |
| HONC8a | Did you feel more irritable? | 56.0 | −0.1 | 46.0 |
| HONC7a | Did you find it hard to concentrate? | 49.5 | 0.1 | 54.0 |
| HONC2 | Do you smoke now because it is really hard to quit? | 41.3 | 0.3 | 61.8 |
| mFTQ5 | Do find it difficult to refrain from smoking in places where it is forbidden? | 37.6 | 0.4 | 65.5 |
| HONC6 | Is it hard to keep from smoking in places where you are not supposed to, like school? | 35.8 | 0.7 | 75.8 |
| mFTQ6 | Do you smoke if you are so ill that you are in bed? | 32.1 | 0.7 | 75.8 |
| mFTQ3 | How soon after you wake up do you smoke first cigarette? | 32.1 | 1.6 | 94.5 |
| mFTQ4 | Which cigarette would you hate to give up? | 22.0 | 1.3 | 90.3 |
| mFTQ1 | How many cigarettes a day do you smoke? (16-25) | 14.7 | 2.0 | 97.7 |
| mFTQ7 | Do you smoke more during the first 2 hours? | 8.3 | 0.5 | 69.1 |
Indicates HONC items that are prefaced by: “When you tried to stop smoking or have not used tobacco for a while”
Acknowledgments
This research was supported by Tobacco Related Disease Research Program Grant # 10IT-0280 and National Institute on Drug Abuse Grant # T32 DA016184. We extend our appreciation to the staff of the high schools involved and to our research assistants.
Footnotes
Utilization of a rest score from all 17 items when analyzing items of each measure provides an iterated analysis using maximum likelihood weights that weigh option choices by taking into account the overall quality of the item in terms of the information it provides about the underlying latent construct (theta), how informative each item option is within an item, and where along theta the options and items are most informative (Ramsay, 2001). These procedures are recommended by Ramsey (2001) to provide better estimates of the underlying trait level.
Because HONC item 6 and mFTQ item 5 overlap almost entirely in terms of their content (i.e., both inquire about difficulty in refraining from smoking in places where it is restricted), it is possible that any discriminating effect of either item could be confounded by their collective weight. Thus, all analyses were re-conducted without each of these items, respectively. In the analyses without the overlapping items, no meaningful differences emerged in item discriminations for the other remaining items (i.e., no values changed more than .1 units) and the relative order of item thresholds did not change when HONC6 or mFTQ5 were excluded. Additionally, as utilization of the rest score from the initial analysis of the full 17 items improves estimation of the underlying dependence syndrome in the subsequent analyses, …
References
- Beevers CG, Strong DR, Meyer B, Pilkonis PA, Miller IW. Efficiently assessing negative cognition in depression: An item response theory analysis of the Dysfunctional Attitude Scale. Psychological Assessment. 2007;19(2):199–209. doi: 10.1037/1040-3590.19.2.199. [DOI] [PubMed] [Google Scholar]
- Brandon TH, Herzog TA, Irvin JE, Gwaltney CJ. Cognitive and social learning models of drug dependence: Implications for assessment of tobacco dependence in adolescents. Addiction. 2004;99(Supp. 1):51–77. doi: 10.1111/j.1360-0443.2004.00737.x. [DOI] [PubMed] [Google Scholar]
- Clark DB, Wood DS, Martin CS, Cornelius JR, Lynch KG, Shiffman S. Multidimensional assessment of nicotine dependence in adolescents. Drug and Alcohol Dependence. 2005;77:235–242. doi: 10.1016/j.drugalcdep.2004.08.019. [DOI] [PubMed] [Google Scholar]
- Cohen LM, Myers MG, Kelly JF. Assessment of nicotine dependence among substance abusing adolescent smokers: A comparison of the DSM-IV criteria and the modified Fagerström Tolerance Questionnaire. Journal of Psychopathology and Behavioral Assessment. 2002;24:225–233. [Google Scholar]
- Colby SM, Tiffany ST, Shiffman S, Niaura RS. Are adolescent smokers dependent on nicotine? A review of the evidence. Drug and Alcohol Dependence. 2000a;59(Suppl 1):S83–S95. doi: 10.1016/s0376-8716(99)00166-0. [DOI] [PubMed] [Google Scholar]
- Colby SM, Tiffany ST, Shiffman S, Niaura RS. Measuring nicotine dependence among youth: A review of available approaches and instruments. Drug and Alcohol Dependence. 2000b;59(Suppl. 1):S23–S39. doi: 10.1016/s0376-8716(99)00163-5. [DOI] [PubMed] [Google Scholar]
- DiFranza JR, Rigotti NA, McNeill AD, Ockene JK, Savageau JA, St Cyr D, Coleman M. Initial symptoms of nicotine dependence in adolescents. Tobacco Control. 2000;9:313–319. doi: 10.1136/tc.9.3.313. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DiFranza JR, Savageau JA, Rigotti NA, Fletcher K, Ockene JK, McNeill AD, Coleman M, Wood C. Development of symptoms of tobacco dependence in youths: 30 month follow up data from the DANDY study. Tobacco Control. 2002;11:228–235. doi: 10.1136/tc.11.3.228. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DiFranza JR, Savageau JA, Fletcher K, O’Loughlin J, Pbert L, Ockene JK, McNeill AD, Hazelton J, Friedman K, Dussault G, Wood C, Wellman RJ. Symptoms of tobacco dependence after brief intermittent use: the Development and Assessment of Nicotine Dependence in Youth-2 study. Archives of Pediatric and Adolescent Medicine. 2007;161(7):704–710. doi: 10.1001/archpedi.161.7.704. [DOI] [PubMed] [Google Scholar]
- Fabrigar LR, Wegener DT, MacCullum RC, Strahan EJ. Evaluating the use of exploratory factor analysis in psychological research. Psychological Methods. 1999;4(3):272–299. [Google Scholar]
- Fagerström KO. Measuring degree of physical dependence to tobacco smoking with reference to individualization of treatment. Addictive Behaviors. 1978;3:235–241. doi: 10.1016/0306-4603(78)90024-2. [DOI] [PubMed] [Google Scholar]
- Floyd FJ, Widaman KF. Factor analysis in the development and refinement of clinical assessment instruments. Psychological Assessment. 1995;7(3):286–299. [Google Scholar]
- Hughes JR, Oliveto AH, Riggs R, Kenny M, Liguori A, Pillitteri JL, MacLaughlin MA. Concordance of different measures of nicotine dependence: two pilot studies. Addictive Behaviors. 2004;29:1527–1539. doi: 10.1016/j.addbeh.2004.02.031. [DOI] [PubMed] [Google Scholar]
- Kandel DB, Schaffran C, Griesler P, Samuolis J, Davies M, Galanti R. On the measurement of nicotine dependence in adolescence: Comparisons of the mFTQ and DSM-IV-based scale. Journal of Pediatric Psychology. 2005;27:1–14. doi: 10.1093/jpepsy/jsi027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lewis-Esquerre JM, Colby SM, Tevyaw TO, Eaton CA, Kahler CW, Monti PM. Validation of the timeline follow-back in the assessment of adolescent smoking. Drug and Alcohol Dependence. 2005;79:33–43. doi: 10.1016/j.drugalcdep.2004.12.007. [DOI] [PubMed] [Google Scholar]
- Lord F. Applications of item response theory to practical testing problems. Hillsdale, NJ: Erlbaum; 1980. [Google Scholar]
- MacPherson L, Myers MG, Johnson M. Adolescent definitions of change in smoking behavior: An investigation. Nicotine & Tobacco Research. 2006;8(5):683–687. doi: 10.1080/14622200600910827. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meijer RR, Baneke JJ. Analyzing psychopathology items: A case for nonparametric item response theory modeling. Psychological Assessment. 2004;9(3):354–368. doi: 10.1037/1082-989X.9.3.354. [DOI] [PubMed] [Google Scholar]
- Mermelstein R, Colby SM, Patten C, Prokhorov A, Brown R, Myers M, Adelman W, Hudmon K, McDonald P. Methodological issues in measuring treatment outcome in adolescent smoking cessation studies. Nicotine & Tobacco Research. 2002;4:395–403. doi: 10.1080/1462220021000018470. [DOI] [PubMed] [Google Scholar]
- Muthén LK, Muthén BO. Mplus user’s guide. Los Angeles, CA: Muthén and Muthén; 1998–2001. [Google Scholar]
- Myers MG, Brown SA, Kelly JF. A smoking intervention for substance abusing adolescents: Outcomes, predictors of cessation attempts, and post-treatment substance use. Journal of Child and Adolescent Substance Abuse. 2000;9:77–81. [Google Scholar]
- O’Loughlin J, Kishchuk N, DiFranza J, Paradis G. Reliability of selected measures of nicotine dependence among adolescents. Annals of Epidemiology. 2002;12(5):353–362. doi: 10.1016/s1047-2797(01)00312-x. [DOI] [PubMed] [Google Scholar]
- Orlando M, Sherbourne CD, Thissen D. Summed-score linking using item response theory: Application to depression measurement. Psychological Assessment. 2000;12(3):354–359. doi: 10.1037//1040-3590.12.3.354. [DOI] [PubMed] [Google Scholar]
- Panter AT, Reeve BD. Assessing tobacco beliefs among youth using item response theory models. Drug and Alcohol Dependence. 2002;68(Suppl. 1):S21–S39. doi: 10.1016/s0376-8716(02)00213-2. [DOI] [PubMed] [Google Scholar]
- Prokhorov AV, Pallonen UE, Fava JL, Ding L, Niaura R. Measuring nicotine dependence among high-risk adolescent smokers. Addictive Behaviors. 1996;21:117–127. doi: 10.1016/0306-4603(96)00048-2. [DOI] [PubMed] [Google Scholar]
- Prokhorov AV, Koehly LM, Pallonen UE, Hudmon KS. Adolescent nicotine dependence measured by the modified Fagerstrom Tolerance Questionnaire at two time points. Journal of Child and Adolescent Substance Abuse. 1998;7:35–47. [Google Scholar]
- Prokhorov AV, De Moor C, Pallonen UE, Hudmon KS, Koehly L, Hu S. Validation of the modified Fagerström Tolerance Questionnaire with salivary cotinine among adolescents. Addictive Behaviors. 2000;25:429–433. doi: 10.1016/s0306-4603(98)00132-4. [DOI] [PubMed] [Google Scholar]
- Ramsay JO. Kernel-smoothing approaches to nonparametric item characteristic curve estimation. Psychometrika. 1991;56:611–630. [Google Scholar]
- Ramsay JO. Testgraf98: A program for the graphical analysis of multiple choice test and questionnaire data (windows version) 2001 Retrieved July 12, 2006, from http://www.psych.mcgill.ca/faculty/ramsay/TestGraf.html.
- Rasch G. Probabilistic models for some intelligence and attainment tests. Copenhagen: Denmark’s Paedagogiske Institut; 1960. [Google Scholar]
- Santor DA, Zuroff DC, Ramsay JO, Cervantes P, Palacios J. Examining scale discriminability in the BDI and CES-D as a function of depressive severity. Psychological Assessment. 1995;7:131–139. [Google Scholar]
- Santor DA, Coyne JC. Shortening the CES-D to improve its ability to detect cases of depression. Psychological Assessment. 1997;9:233. [Google Scholar]
- Santor DA, Coyne JC. Evaluating the continuity of symptomatology between depressed and nondepressed individuals. Journal of Abnormal Psychology. 2001;110:216. doi: 10.1037//0021-843x.110.2.216. [DOI] [PubMed] [Google Scholar]
- Shadel WG, Shiffman S, Niaura R, Nichter M, Abrams DB. Current models of nicotine dependence: What is known and what is needed to advance understanding of tobacco etiology among youth. Drug and Alcohol Dependence. 2000;59:S9–S21. doi: 10.1016/s0376-8716(99)00162-3. [DOI] [PubMed] [Google Scholar]
- Sledjeski EM, Dierker LC, Costello D, Shiffman S, Donny E, Flay BR. Predictive validity of four nicotine dependence measures in a college sample. Drug and Alcohol Dependence. 2007;87:10–19. doi: 10.1016/j.drugalcdep.2006.07.005. [DOI] [PubMed] [Google Scholar]
- Sobell LC, Sobell MB. Time-line follow-back: A technique for assessing self-reported alcohol consumption. In: Litten RZ, Allen JP, editors. Measuring Alcohol Consumption: Psychosocial and Biochemical Methods. Pergamon Press; Totowa, NJ: 1992. pp. 73–98. [Google Scholar]
- Stout WF. A nonparametric approach for assessing latent trait unidimensionality. Psychometrika. 1987;52:589–617. [Google Scholar]
- Strong DR, Brown RA, Ramsey SE, Myers MG. Nicotine dependence measures among adolescents with psychiatric disorders: Evaluating symptom expression as a function of dependence severity. Nicotine & Tobacco Research. 2003;5:735–746. doi: 10.1080/1462220031000158609. [DOI] [PubMed] [Google Scholar]
- Strong DR, Kahler CW, Abrantes AM, MacPherson L, Myers MG, Ramsey SE, Brown RA. Nicotine dependence symptoms among adolescents with psychiatric disorders: Using a Rasch model to evaluate symptom expression across time. Nicotine and Tobacco Research. 2007;9(5):557–569. doi: 10.1080/14622200701239563. [DOI] [PubMed] [Google Scholar]
- Tabachnick BG, Fidell LS. Using multivariate statistics. Fourth. Allyn and Bacon; Boston, Massachusetts: 2001. [Google Scholar]
- Tiffany ST, Conklin CA, Shiffman S, Clayton RR. What can dependence theories tell us about assessing the emergence of tobacco dependence? Addiction. 2004;99(Suppl. 1):78–86. doi: 10.1111/j.1360-0443.2004.00734.x. [DOI] [PubMed] [Google Scholar]
- Wellman RJ, DiFranza JR, Pbert L. A comparison of the psychometric properties of the hooked on nicotine checklist and the modified Fagerstrom tolerance questionnaire. Addictive Behaviors. 2006a;31(3):486–495. doi: 10.1016/j.addbeh.2005.05.031. [DOI] [PubMed] [Google Scholar]
- Wellman RJ, Savageau JA, Godiwala S, Savageau N, Friedman K, Hazelton J, DiFranza JR. A comparison of the Hooked on Nicotine Checklist and the Fagerstrom Test for Nicotine Dependence in adult smokers. Nicotine and Tobacco Research. 2006b;8(4):575–580. doi: 10.1080/14622200600789965. [DOI] [PubMed] [Google Scholar]
- Wheeler KC, Fletcher KE, Wellman RJ, DiFranza JR. Screening adolescents for nicotine dependence: The Hooked on Nicotine Checklist. Journal of Adolescent Health. 2004;35(3):225–230. doi: 10.1016/j.jadohealth.2003.10.004. [DOI] [PubMed] [Google Scholar]