

Abstract
Background
Lower extremity movement compensations following transtibial amputation are well-documented and are likely influenced by trunk posture and movement. However, the biomechanical compensations of the trunk and lower extremities, especially during high-demand tasks such as step ascent and descent, remain unclear.
Methods
Kinematic and kinetic data were collected during step ascent and descent tasks for three groups of individuals: diabetic/transtibial amputation, diabetic, and healthy. An ANCOVA was used to compare peak trunk, hip and knee joint angles and moments in the sagittal and frontal planes between groups. Paired t-tests were used to compare peak joint angles and moments between amputated and intact limbs of the diabetic/transtibial amputation group.
Findings
During step ascent and descent, the transtibial amputation group exhibited greater trunk forward flexion and lateral flexion compared to the other two groups (P<0.016), which resulted in greater low back moments and asymmetric loading patterns in the lower extremity joints. The diabetic group exhibited similar knee joint loading patterns compared to the amputation group (P<0.016), during step descent.
Interpretation
This study highlights the biomechanical compensations of the trunk and lower extremities in individuals with dysvascular transtibial amputation, by identifying low back, hip, and knee joint moment patterns unique to transtibial amputation during stepping tasks. In addition, the results suggest that some movement compensations may be confounded by the presence of diabetes and precede limb amputation. The increased and asymmetrical loading patterns identified may predispose individuals with transtibial amputation to the development of secondary pain conditions, such as low back pain or osteoarthritis.
Keywords: dysvascular amputation, diabetes, biomechanics, stairs
1. Introduction
Transtibial amputation (TTA) occurs in many cases for people with non-healing and/or infected wounds related to complex dysvascular pathologies, which often include severe Diabetes Mellitus (DM). Following dysvascular amputation, nearly 50% of individuals do not achieve community ambulation (Davies and Datta, 2003) and the majority of individuals report difficulty with higher demand tasks, such as step ambulation (de Laat et al., 2013). In addition, 40-50% of individuals with unilateral TTA suffer from disabling comorbidities, such as low back pain (LBP), (Ehde et al., 2001) which further compromise function and mobility, ultimately having a negative impact on quality of life (Pell et al., 1993).
In order to maintain mobility after TTA, individuals must adopt movement compensations to account for the loss of ankle function in the amputated limb (e.g. increased hip and decreased knee extensor moments on the amputated limb) (Sagawa et al., 2011). These compensatory movements may contribute to poor ambulatory outcomes and the development of secondary pain conditions (e.g., LBP and osteoarthritis (OA)) (Morgenroth et al., 2012). While numerous studies have documented movement compensations in individuals with unilateral TTA during level-ground gait (Prinsen et al., 2011; Sagawa et al., 2011; Soares et al., 2009), there is a paucity of studies that have investigated movement compensations during high-demand tasks such as step ascent and descent. Additionally, most studies investigating movement compensations in individuals with TTA have included study samples with a variety of amputation etiologies (e.g. traumatic, tumoral, or congenital) and frequently only compare to healthy individuals. Individuals with DM who have not undergone TTA also exhibit movement compensations during mobility tasks (Brown et al., 2016; Sawacha et al., 2009), indicating that the presence of DM may further confound mobility after TTA. Combining amputation etiologies and only comparing to healthy individuals limits the ability to accurately describe movement compensations in individuals with dysvascular TTA and identify compensations above and beyond the presence of DM.
Stepping up and down are commonly encountered in daily living and place an increased mechanical demand on the musculoskeletal system compared to level-ground gait (Nadeau et al., 2003; Reeves et al., 2008). During step ascent and descent, individuals with TTA exhibit a hip dominant strategy consisting of increased hip extension moments and decreased knee extension moments which is in contrast to healthy individuals who typically utilize a knee dominant strategy (Alimusaj et al., 2009; Powers et al., 1997; Schmalz et al., 2007; Yack et al., 1999). Reduced knee loading by individuals with TTA may be an attempt to minimize mechanical demand on the amputated limb in order to enhance stability due to knee extensor weakness (Powers et al., 1996). Increased hip loading on the side of the amputation likely serves to compensate for the knee and ankle by aiding in forward progression of the body (Powers et al., 1997; Schmalz et al., 2007). In contrast to the amputated limb, during step ascent and descent with the intact limb, knee extension moments exceed those of healthy individuals while hip extension moments are similar to healthy individuals (Alimusaj et al., 2009; Schmalz et al., 2007). These results indicate that during step ascent and descent, individuals with TTA exhibit asymmetric loading patterns between limbs which are likely amplified compared to less complex tasks such as level walking and may predispose individuals with TTA to development of OA in lower extremity joints (Morgenroth et al., 2012).
Despite the apparent interaction between trunk and lower extremity movement compensations, few studies have investigated regional interdependence by examining both trunk and lower extremity kinematics and kinetics during high-demand tasks in individuals with TTA. Movement compensations in the lower extremities of individuals with TTA are likely accompanied by both sagittal and frontal plane compensations at the trunk due to regional interdependence (Gillet et al., 2003). For example, during level-ground gait, individuals with TTA exhibit reductions in amputated limb hip abduction and knee adduction moments, which is accompanied by increased frontal plane lateral trunk flexion over the amputated limb during stance phase (Compensated Trendelenburg pattern) (Rueda et al., 2013). Such movement compensations of the trunk may aid in increasing stability and achieving forward progression, but can result in increased loading and muscular demand at the low back (Hendershot and Wolf, 2014, 2015a; Hendershot and Wolf, 2015b), which may predispose individuals with TTA to an increased risk of LBP (Kumar, 2001).
The purpose of this study was to identify biomechanical compensations of the trunk, hip, and knee during step ascent and step descent tasks in individuals with DM and TTA (TTA group) compared to two groups: 1) individuals with DM without TTA (DM group) and 2) healthy individuals (HC group) of similar age. We hypothesized that the TTA group would exhibit altered and asymmetrical motion and moments at the trunk, hip, and knee during step ascent and descent compared to HC and that the differences would be greater compared to the HC group than the DM group.
2. Methods
2.1 Participants
Three groups of participants were enrolled in this study: TTA (n=9), DM (n=10), and HC (n=11) (Table 1). Eligibility for all groups included a body mass index (BMI) less than 40 and an age between 50-85 years. Both the DM and TTA groups had a clinical diagnosis of type II diabetes. Individuals were included in the TTA group if they had a unilateral TTA in the previous one to three years and were able to walk with a prosthesis for four minutes without rest. The HC had no history of LBP. Individuals were excluded from all groups if they had uncontrolled diabetes, cardiovascular, orthopaedic, neurologic condition, or wounds/ulcers that limited function, or if their TTA was traumatic or cancer-related. The study protocol was approved by the [blinded for review] Institutional Review Board and prior to participation all participants signed a written, informed consent form.
Table 1.
Comparison of mean (SD) baseline demographics and anthropometrics between groups. TTA, Transtibial amputation with diabetes group; DM, Diabetes group; HC, healthy cohort.
| Characteristic | TTA | DM | HC |
|---|---|---|---|
| n | 9 | 10 | 11 |
| Age (year) | 56.9 (4.6) | 63.5 (8.3) | 59.7 (7.0) |
| Body Mass (kg) | 94.7 (13.4) | 96.1 (20.1) | 84.8 (10.3) |
| Body Height (m) | 1.79 (0.1) | 1.79 (0.1) | 1.81 (0.04) |
| Self-selected Gait Speed (m/s) | 0.97 (0.1) | 1.01 (0.2) | 1.37 (0.2) |
2.2 Instrumentation and Procedures
Participants were instrumented with 63 reflective markers placed on the head, trunk, pelvis, and bilateral upper and lower extremities (Figure 1). The pelvis was digitally marked using a spring-loaded digitizing pointer (C-Motion, Inc., Germantown, MD, USA). The trunk was modelled as a single rigid segment in accordance with the ISB recommendations using the C7, T10, bilateral acromia and sternal markers (Figure 1) (Wu et al., 2005). Distally, the trunk was connected in the model to the pelvis at the L5/S1 joint. Three-dimensional kinematic data were collected using eight infrared cameras (Vicon, Centennial, CO, USA) sampling at 100Hz and synchronized with two embedded force plates (Bertec, Columbus, OH, USA) sampling at 2000Hz. For step ascent, participants stood on an embedded force plate and stepped onto a step (60cm × 40cm × 20cm) placed over an adjacent force plate. For step descent, participants began on the step and stepped down onto the embedded force plate. The TTA group was instructed to lead the first three trials of step ascent with their intact limb and step descent with their amputated limb, as this is the pattern that is typically emphasized during rehabilitation. The DM and HC groups lead the first three trials of both tasks with their right limb followed by their left limb. A total of three trials leading with each limb were performed and averaged for group comparisons.
Figure 1.
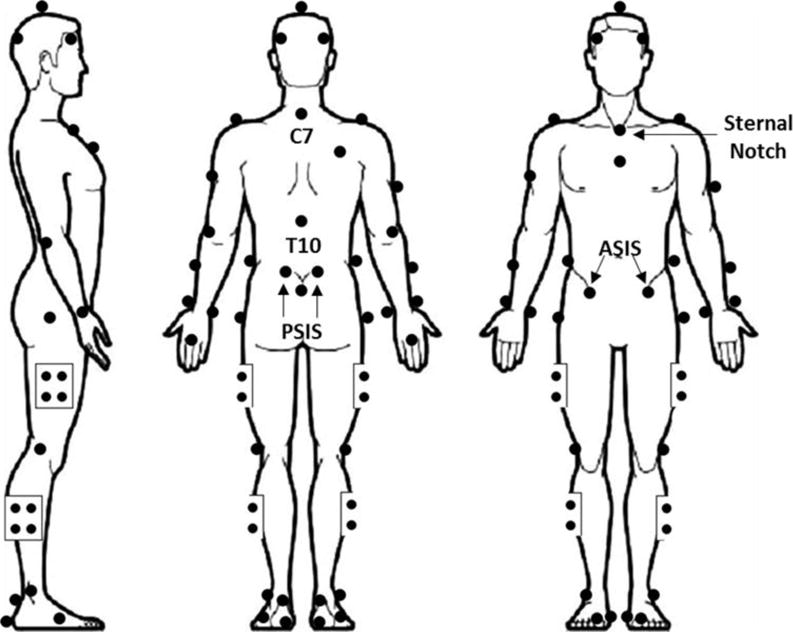
Full-body marker set used to collect kinematic data.
Kinematic and kinetic data were low-pass filtered with a 4th-order Butterworth filter with a cutoff of 6Hz and 20Hz, respectively. A 15-segment, subject-specific model was created using Visual 3D (C-Motion, Inc. Germantown, MD, USA) with intact segment masses and inertial properties being estimated as previously described by Dempster and Hanavan. The mass, center of mass, and inertial properties of the prosthetic shank and foot for the TTA group were determined using a reaction board technique and oscillation method, as previously described.(Smith et al., 2014) Individuals in the TTA group wore their own prosthesis consisting of a total contact carbon fiber socket, dynamic elastic response foot, and either pin (n=6) or sleeve (n=3) suspension. Hip and ankle joint centers were calculated in Visual 3D from a static calibration in an anatomically neutral pose and knee joint centers were calculated using a functional joint center approach (Schwartz and Rozumalski, 2005). Joint angles were determined using an X–Y–Z Cardan sequence with the hip and knee joint angles being defined as the thigh relative to the pelvis and shank relative to the thigh, respectively. Trunk segment angles were defined relative to the laboratory coordinate system. Low back, hip, and knee moments were calculated using an inverse dynamics approach.
2.3 Data Analysis
The limb in contact with the step was analyzed for both tasks. For the step ascent task, the period of interest was from weight acceptance on the step through single limb support (Zachazewski et al., 1993). For the step descent task, the period of interest was from single limb support on the step through controlled lowering to the floor (Zachazewski et al., 1993). The data were time normalized to 100% of single limb support for step ascent and step descent cycles. Peak joint angles and moments during each task were identified and averaged across three trials for each limb and used in the analysis. In the sagittal plane, peak knee, hip, and trunk flexion angles and peak knee, hip, and low back extension moments were the dependent variables. In the frontal plane, peak knee and hip adduction angles and trunk lateral flexion angle, as well as peak knee adduction and hip abduction moments and peak low back lateral bend moments were the dependent variables. The right and left limb kinematic and kinetic variables for the DM and HC groups were averaged for analysis after no meaningful difference was observed between limbs for either task. Kinematic and non-normalized kinetic data for each limb were compared between groups using an ANCOVA controlling for body mass index (BMI)(Curran-Everett, 2013). The level of significance was set a priori at α = 0.05. Where statistically significant differences by group were identified we performed Bonferroni adjusted pairwise comparisons (adjusted α = 0.016). Within the TTA group, paired t-tests were used to compare between limb differences (amputated vs. intact limb). All inferential statistics were performed using SPSS v 22.0 (IBM Corp, Armonk, NY).
3. Results
There were no differences between groups on any of the descriptors (Table 1). The TTA group were all K-2 level ambulators, reported using their prosthesis daily, and were able to ambulate without the use of an assistive device. Three participants in the TTA were not able complete the step descent task and were not included in the final analysis of that task.
3.1 Step Ascent Kinematics
In the sagittal plane, the trunk remained flexed forward throughout the step ascent for all groups (Figure 2A). Peak trunk flexion was bilaterally similar in the TTA group [amputated limb=31.8 (7.2)°; intact limb= 31.4 (7.5)°; P=0.80]. The TTA group exhibited greater trunk flexion than the HC group [21.6 (8.6)°, P=0.0017 for the amputated limb; P=0.02 for the intact limb], but not the DM group [27.11 (7.6)°, P=0.63 for the amputated limb; P=0.77 for the intact limb]. In the TTA group, peak hip flexion angle was greater (P=0.03) on the amputated limb [68.6 (12.6)°] than the intact limb [63.2 (8.7)°]. Sagittal plane hip excursions were greater in the HC group [41.5 (3.3)°] than the TTA group [amputated limb= 35.9 (4.6)°, P=0.017] and DM group [34.3 (4.0)°, P = 0.002]. Sagittal plane knee excursions were greater bilaterally in the TTA group [amputated limb = 49.0 (4.2)°, P= 0.001; intact limb = 49.1 (6.6)°, P=0.003] than the DM limb [41.0 (5.4)°].
Figure 2.
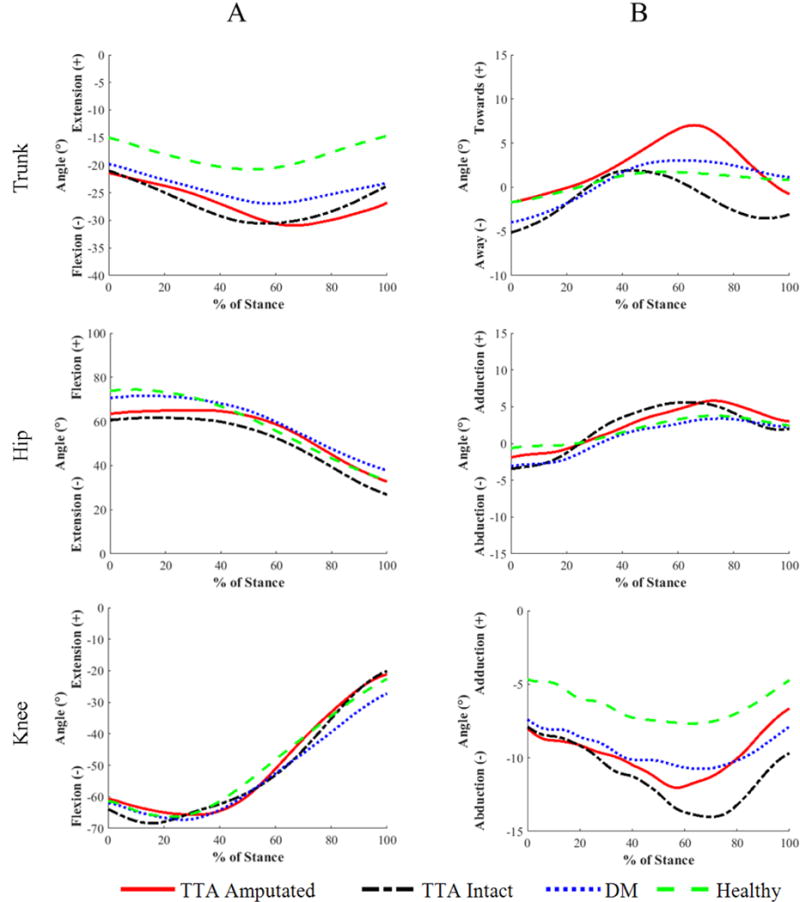
(A)Sagittal plane joint angles and (B) frontal plane joint angles during stance phase of step ascent.
In the frontal plane, the trunk tended to lean towards the stance limb for all groups (Figure 2B). In the TTA group, peak lateral trunk flexion tended to be greater (P=0.02) on the amputated limb [7.9 (3.9)°] than the intact limb [3.9 (3.9)°] during step ascent on the amputated limb. The TTA group exhibited greater peak lateral trunk flexion toward the amputated limb than the DM group [3.6 (2.1)°, P=0.001] and HC group [2.2 (1.4)°, P<0.001]. Trunk lateral excursions in the TTA group were larger on the amputated limb [12.4 (4.7)°] than the DM group [7.5 (2.6)°, P=0.005] and HC group [4.0 (2.9)°, P<0.001]. Additionally, trunk lateral excursions on the intact limb of the TTA group [10.9 (3.6)°] were larger than the HC group (P<0.001). Hip frontal plane motion was greater in the TTA group on the intact limb [11.5 (3.6)°] than both the DM group [7.2 (2.5)°, P=0.004] and HC group [6.4 (2.6)°, P=0.002].
3.2 Step Ascent Kinetics
The TTA group generated larger peak low back extension moments on the amputated limb than the DM (P=0.003) and HC groups (P=0.001) (Table 2). The TTA group generated larger peak hip extension moments on the amputated limb than the DM and HC groups (P<0.001). The TTA group also generated larger peak hip extension moments on the intact limb than the HC group (P=0.013), but not the DM group (P=0.03). Peak knee extension moments were asymmetrical between the amputated and intact limbs of the TTA group (P<0.001). The TTA group generated smaller peak knee extension moments on the amputated limb than both the DM and HC groups (P<0.001). Additionally, the TTA group generated larger peak knee extension moments on intact limb than the DM group (P=0.005), but not the HC group (P=0.29).
Table 2.
Comparison of mean (SD) peak internal moments (Nm/kg*m) during single limb support (SLS) phase on each limb for step ascent between groups and between limbs within each group. TTA, Transtibial amputation with diabetes group; DM, Diabetes group; HC, healthy cohort.
| TTA Amputated n=9 |
TTA Intact n=9 |
DM n=10 |
HC n=10 |
|
|---|---|---|---|---|
| Low Back | ||||
| Extension | −0.58 (0.11) *† | −0.51 (0.11) | −0.41 (0.11) | −0.34 (0.11) |
| Timing (%SLS) | 59.8 (9.6) | 49.9 (13.2) | 56.5 (8.2) | 49.4 (5.7) |
| Lateral Bend | 0.18 (0.08) *† | 0.09 (0.08) | 0.10 (0.04) | 0.08(0.04) |
| Timing (%SLS) | 68.1 (8.3) | 72.9 (21.3) | 71.1 (11.3) | 69.9 (19.6) |
| Hip | ||||
| Extension | −0.80 (0.15) *† | −0.71 (0.17) * | −0.55 (0.12) | −0.50 (0.10) |
| Timing (%SLS) | 59.4 (10.9) | 48.7 (15.3) | 52.4 (8.8) | 43 (6.6) |
| Abduction | −0.33 (0.09) § | −0.53 (0.12) *† | −0.35 (0.09) | −0.38 (0.04) |
| Timing (%SLS) | 85 (12.5) | 68.2 (15.4) | 81.7 (8.5) | 71.2 (11.4) |
| Knee | ||||
| Extension | 0.26 (0.08) *†§ | 0.74 (0.10) † | 0.56 (0.15) | 0.68 (0.06) |
| Timing (%SLS) | 60.1 (24.3) | 55.4 (9.3) | 57.3 (9.7) | 50 (5.7) |
| Adduction | 0.04 (0.03) | 0.05 (0.04) | 0.07 (0.06) | 0.07 (0.06) |
| Timing (%SLS) | 64.1 (24.3) | 51.6 (20.4) | 57.9 (10.4) | 46.1 (23.5) |
Note: Results of post hoc analyses are indicated by the following symbols:
Significant difference vs. HC
Significant difference vs. DM
Significant difference between TTA Amputated vs. TTA Intact
In the frontal plane, the TTA group generated larger peak low back lateral bend moments on the amputated limb than both the DM (P=0.007) and HC (P=0.003) groups. Peak hip abduction moments were asymmetrical between amputated and intact limbs in the TTA group (P<0.01). Peak hip abduction moments on the intact limb in the TTA group were greater than both the DM (P<0.001) and HC groups (P=0.003).
3.3 Step Descent Kinematics
In the sagittal plane, the TTA group exhibited greater hip excursions on the amputated limb [22.6 (5.5)°] than both the DM [16.7 (2.4)°, P=0.013] and HC [16.2 (4.5)°, P=0.003] groups during step descent (Figure 3A). Hip excursions on the TTA group intact limb [21.7 (6.7)°] were greater than the HC group (P=0.01) but not the DM group (P=0.16). Peak knee flexion angle was greater (P=0.04) on the TTA group amputated limb [108.7 (8.6)°] than the intact limb [99.7 (6.5)°].
Figure 3.
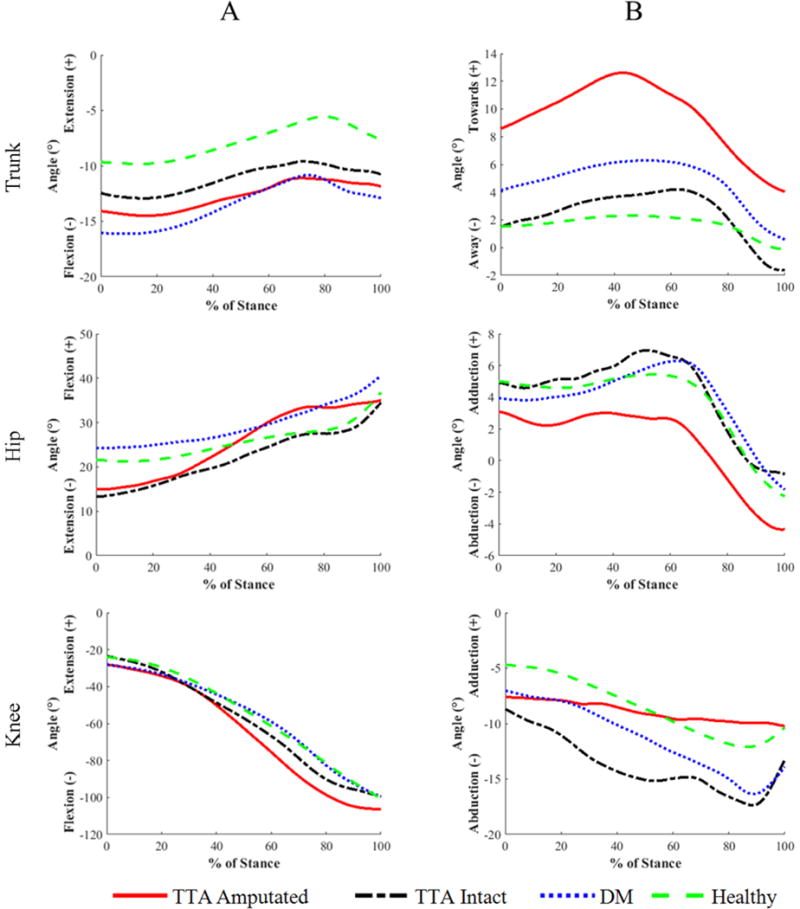
(A) Sagittal plane joint angles and (B) frontal plane joint angles during stance phase of step descent.
In the frontal plane, the trunk tended to lean over the stance limb for all groups during step descent (Figure 3B). The TTA group exhibited asymmetrical peak lateral trunk flexion angles between the amputated [12.8 (5.3)°] and intact [5.2 (4.1)°, P=0.04] limbs. On the amputated limb, the TTA group exhibited greater peak lateral trunk flexion angles than both the DM [6.6 (5.3)°, P=0.01) and HC [3.0 (1.9)°, P<0.001] groups. Lateral trunk excursions were bilaterally similar (P=0.35) in the TTA group. On the amputated limb, the TTA group exhibited greater lateral trunk excursions [9.0 (4.6)°] than the HC group [3.2 (1.9)°, P=0.013], but not the DM group (P=0.15). The TTA group exhibited smaller amputated limb knee excursions [6.5 (3.2)°] than the intact limb [13.1 (3.4)°, P=0.05].
3.4 Step Descent Kinetics
The mean joint moments during stance phase of step descent for each group are presented in Table 3. In the sagittal plane, the TTA group generated greater (P=0.03) low back extension moments on the amputated limb than the intact limb (Table 3). The TTA group generated smaller knee extension moments on the amputated limb than the intact limb (P<0.01) and HC group (P=0.007). Greater knee extension moments were generated on the intact limb than the DM group (P=0.013).
Table 3.
Comparison of mean (SD) peak internal moments (Nm/kg*m) during single limb support (SLS) phase on each limb for step descent between groups and between limbs within each group. TTA, Transtibial amputation with diabetes group; DM, Diabetes group; HC, healthy cohort.
| TTA Amputated n=9 |
TTA Intact n=9 |
DM n=10 |
HC n=10 |
|
|---|---|---|---|---|
| Low Back | ||||
| Extension | −0.13 (0.14) § | −0.02 (0.07) | −0.01 (0.18) | 0.08 (0.13) |
| Timing (%SLS) | 68.7 (28.6) | 80.8 (32.2) | 64.2 (30.9) | 80.3 (31.6) |
| Lateral Bend | 0.24 (0.13) *† | 0.16 (0.08) | 0.15 (0.04) | 0.10 (0.07) |
| Timing (%SLS) | 38.5 (23.9) | 49.3 (26.2) | 54.7(7) | 53.7 (7.1) |
| Hip | ||||
| Extension | −0.30 (0.08) § | −0.15 (0.07) | −0.22 (0.17) | −0.17 (0.15) |
| Timing (%SLS) | 24.3 (31.1) | 0.2 (0.4) | 5.5 (11.8) | 1.5 (2.5) |
| Abduction | −0.34 (0.11) | −0.44 (0.13) | −0.43 (0.07) | −0.44 (0.06) |
| Timing (%SLS) | 50.2 (54.6) | 43.5 (33.8) | 20.2 (25.11) | 8.7 (19.6) |
| Knee | ||||
| Extension | 0.49 (0.12)*§ | 0.88 (0.18) † | 0.67 (0.16) | 0.76 (0.15) |
| Timing (%SLS) | 59.7 (14) | 64.8 (9.6) | 63.6 (6.5) | 69.8 (4) |
| Adduction | 0.03 (0.03) †§ | 0.20 (0.08) * | 0.13 (0.07) | 0.10 (0.07) |
| Timing (%SLS) | 35 (29.6) | 58.2 (11.9) | 64.6 (6.4) | 62.8 (10.2) |
Note: Results of post hoc analyses are indicated by the following symbols:
Significant difference vs. HC
Significant difference vs. DM
Significant difference between TTA Amputated vs. TTA Intact
In the frontal plane, low back lateral bend moments were bilaterally similar in the TTA group (P=0.23). On the amputated limb, the TTA group generated greater low back lateral bend moments than both the DM (P=0.013) and HC (P=0.001) groups (Table 3). Peak knee adduction moments were asymmetrical between the amputated limb than the intact limb (P<0.01). On the amputated limb, the TTA group generated smaller knee adduction moments than the DM group (P=0.008). Additionally, on the intact limb, the TTA group generated greater knee adduction moments than the HC group (P=0.01, Table 3).
4. Discussion
The purpose of this study was to investigate trunk and lower extremity movement compensations during step ascent and descent in individuals with DM and TTA. Previous studies have primarily focused on compensations in the lower extremities (Alimusaj et al., 2009; Schmalz et al., 2007); however, given the influence the trunk can have on lower extremity loading (Gillet et al., 2003) and the high prevalence of LBP in individuals with TTA (Ehde et al., 2001) it is important to understand the compensations that are occurring more proximally. Our results highlight the regional interdependence between the lower extremity joints and the trunk in response to the lack of ankle motion and function in the amputated limb.
During both stepping tasks, individuals with TTA exhibited asymmetrical and excessive trunk motion, which was accompanied by altered joint moments in the low back and lower extremities compared to individuals with DM and healthy individuals. On the amputated limb, the limited range of motion available at the ankle likely contributed to many of the movement compensations observed at the knee, hip, and low back as well as to the preferential loading of the intact limb. The results of this study have implications for addressing the biomechanical pathogenesis of secondary pain conditions such as LBP and lower extremity OA in individuals with DM and TTA. Furthermore, it appears that similar changes to the TTA group occur in the DM group, but to a lesser degree.
4.1 Step Ascent
4.1.1 Sagittal Plane
In the present study, the TTA group exhibited excessive forward trunk flexion compared to the DM and HC groups, which resulted in low back extension moments that were over 35% higher than what has been reported in individuals with TTA during level ground walking (Hendershot and Wolf, 2014). Forward trunk flexion shifts the trunk center of mass anteriorly, thereby placing a greater loading demand on the low back extensor muscles. Ascending a step is generally considered to be a higher-demand task than level-ground walking, as it requires larger ranges of joint motion and peak joint moments to move the body upwards and forwards (Nadeau et al., 2003; Reeves et al., 2008).
The excessive forward trunk lean exhibited by the TTA group may help to facilitate the use of a hip dominant strategy when stepping onto the amputated limb (Alimusaj et al., 2009; Schmalz et al., 2007; Yack et al., 1999). This strategy may be an attempt to reduce the loading demand on the knee extensors (quadriceps avoidance pattern). By flexing the trunk forward, the center of mass is shifted away from the hip joint and closer to the knee joint, which increases and decreases the demand for producing extension moments at the hip and knee, respectively. The TTA group produced a significantly greater hip extension moment and reduced knee extension moment when stepping onto the amputated limb which is consistent with a hip dominant strategy, and has been previously described in individuals with TTA during step ascent (Alimusaj et al., 2009; Schmalz et al., 2007; Yack et al., 1999). Conversely, when stepping up with the intact limb, the TTA group generated a knee extension moment similar to the HC group, which resulted in asymmetrical knee loading between the amputated and intact limbs. Preferential loading of the intact limb has been reported during step ascent in individuals with TTA (Barnett et al., 2014; Schmalz et al., 2007) and has been implicated in the development of OA (Morgenroth et al., 2012).
4.1.2 Frontal Plane
In the frontal plane, the TTA group exhibited asymmetrical trunk motion consisting of a larger lateral trunk flexion angle toward the amputated limb. The exaggerated lateral trunk flexion angle when stepping onto the amputated limb likely contributed to the reduced hip abductor moment observed in amputated limb relative to the intact limb. Clinically, this movement pattern is known as a compensated Trendelenburg and has been previously identified during level-ground walking in individuals with TTA (Hendershot and Wolf, 2014; Rueda et al., 2013). A compensated Trendelenburg pattern is commonly employed to improve pelvic stability in the presence of hip abductor weakness. While this compensation may be effective for maintaining mediolateral pelvic stability, the current results indicate that it increases the low back loading, as evidenced by low back lateral bend moments that were two times larger than the intact limb and the DM and HC groups. Contrary to the amputated limb, the TTA group produced hip abduction moments when stepping onto the intact limb that were approximately 30% greater than the DM and HC groups. This finding indicates the use of a “hip-hike” strategy by the TTA group, which has been previously observed during level-ground walking (Michaud et al., 2000) to ensure that the amputated limb clears the step.
4.2 Step Descent
4.2.1 Sagittal Plane
During step descent, the TTA group exhibited low back extension moments that were five times higher when stepping onto the intact limb compared to the amputated limb. A higher low back extension moment was produced when stepping down onto the intact limb, despite no significant difference in trunk forward flexion angle between limbs in the TTA group. One possible explanation for this finding is a lack of dorsiflexion in the trailing amputated limb preventing optimal alignment of the ground reaction force relative to the low back joints. While the trunk was flexed forward on both limbs, the ability to dorsiflex the intact ankle more than the prosthetic ankle allows the trunk and pelvis to progress anteriorly over the foot, thus reducing the moment arm between the low back and the ground reaction force.
Similar to step ascent, the TTA group exhibited a larger hip extension moments compared to stepping onto the amputated limb. Additionally, the TTA group produced significantly lower knee extension moments on the amputated limb compared to both the intact limb and the HC group. Step descent requires large knee extension moments to be produced for controlled lowering of the body (Mcfadyen and Winter, 1988). It is possible that the TTA group is attempting to reduce the loading demand on the amputated limb knee joint in the presence of knee extensor weakness. Although not measured in the present study, knee extensor weakness is prevalent in individuals with TTA (Powers et al., 1996).
When using the intact limb to lower the body from the step, the TTA group generated significantly greater knee extension moments than the DM group. Additionally, knee extension moments generated in the amputated limb of the TTA group were not significantly different from the DM group. Reduced knee extension moments during step descent in individuals with DM have been previously reported (Brown et al., 2016). These results indicate that the shift away from the typical knee dominant strategy towards a hip dominant strategy during step ambulation in individuals with DM and TTA may precede the amputation.
4.2.2 Frontal Plane
The TTA group exhibited a greater lateral trunk flexion angle over the amputated limb than the intact limb, which resulted in greater low back lateral bend moments when stepping onto the intact limb compared to the DM and HC groups. Interestingly, when supported by the amputated limb and stepping onto the intact limb, the TTA group exhibited larger lateral trunk lean and subsequent low back lateral bend moment during step descent compared to ascent. Maintaining mediolateral stability during step descent is important for controlled lowering of the body in order to prevent falls. The greater frontal plane trunk motion and low back moment during step descent indicates that individuals with TTA may have more difficulty maintaining pelvic stability due to weakness in the hip abductors (Powers et al., 1996) and controlling the body’s center of mass in the mediolateral direction than during step ascent.
At the knee joint, the TTA group produced a larger adduction moment and a greater peak abduction angle in the intact limb compared to the amputated limb. One possible explanation for this finding is that the lateral trunk lean towards the amputated limb reduced the frontal plane loading demand at the knee joint. Additionally, the socket fit or suspension system (sleeve vs. pin/lock) of the prosthesis could have affected frontal plane movement and loading of the knee joint.
4.3 Limitations
While the present study focused on the stance limb on the step, the trailing push off limb (step ascent) and leading landing limb (step descent) also contribute to movement and loading patterns. Examination of the push-off and landing limbs in individuals with TTA, in terms of loading and loading rates warrants further investigation. Second, participants in the TTA group had undergone TTA that was dysvascular in nature, thereby limiting generalizability of these findings to individuals with TTA of other etiologies such as trauma or cancer. Third, step negotiation was a highly difficult task for participants in the TTA group to perform and as such we limited performance of the stepping tasks to three trials per limb, per task (12 total trials). Limiting the number of repetitions to three did not allow assessment of within subject variability, which warrant further investigation. Finally, while none of the participants in the TTA group had complaints of acute LBP during the testing sessions, history of LBP, which could potentially influence movement, was not recorded in these individuals.
5. Conclusion
During step ascent and descent, individuals with DM and TTA exhibited asymmetrical and excessive trunk motion, which was accompanied by asymmetrical loading of the low back and lower extremity joints. These movement compensations may contribute to the pathogenesis of secondary pain conditions such as LBP and OA in individuals with DM and TTA. In addition to increasing functional mobility and independence following TTA, rehabilitation interventions are needed to reduce excessive low back loading demands and emphasize use of hip abductor and knee extensor strength in the amputated limb during step negotiation. Some movement compensations in the TTA group were also observed in the DM group, indicating that the presence of DM may further confound movement after TTA. Therefore, individuals with DM without amputation may also benefit from interventions aimed at improving movement quality and step ascent and descent performance.
Highlights.
Movement compensations after amputation occur in both the lower limbs and trunk.
Individuals with transtibial amputation exhibit excessive trunk motion.
Altered low back and lower extremity loading accompany excessive trunk motion.
There is biomechanical interdependence in trunk and lower limb compensations.
Acknowledgments
This work was supported by the National Institues of Health (K12-HD05593) and pilot funding from the University of Denver Knoebel Institue for Healthy Aging. The authors would like to acknowledge the contributions of Dr. Victor Cheuy, PhD in assisting with data reduction.
The study protocol was approved by the Colorado Multiple Institutional Review Board (#14-0770).
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
All authors were involved in this study and the preparation of this manuscript. The material in this manuscript has not been submitted for publication elsewhere.
References
- Alimusaj M, Fradet L, Braatz F, Gerner HJ, Wolf SI. Kinematics and kinetics with an adaptive ankle foot system during stair ambulation of transtibial amputees. Gait Posture. 2009;30:356–363. doi: 10.1016/j.gaitpost.2009.06.009. [DOI] [PubMed] [Google Scholar]
- Barnett CT, Polman RCJ, Vanicek N. Longitudinal changes in transtibial amputee gait characteristics when negotiating a change in surface height during continuous gait. Clin Biomech. 2014;29:787–793. doi: 10.1016/j.clinbiomech.2014.05.012. [DOI] [PubMed] [Google Scholar]
- Brown SJ, Handsaker JC, Maganaris CN, Bowling FL, Boulton AJ, Reeves ND. Altered joint moment strategy during stair walking in diabetes patients with and without peripheral neuropathy. Gait Posture. 2016;46:188–193. doi: 10.1016/j.gaitpost.2016.03.007. [DOI] [PubMed] [Google Scholar]
- Curran-Everett D. Explorations in statistics: the analysis of ratios and normalized data. Adv Physiol Educ. 2013;37:213–219. doi: 10.1152/advan.00053.2013. [DOI] [PubMed] [Google Scholar]
- Davies B, Datta D. Mobility outcome following unilateral lower limb amputation. Prosthet Orthot Int. 2003;27:186–190. doi: 10.1080/03093640308726681. [DOI] [PubMed] [Google Scholar]
- de Laat FA, Rommers GM, Dijkstra PU, Geertzen JH, Roorda LD. Climbing Stairs After Outpatient Rehabilitation for a Lower-Limb Amputation. Arch Phys Med Rehab. 2013;94:1573–1579. doi: 10.1016/j.apmr.2013.01.020. [DOI] [PubMed] [Google Scholar]
- Ehde DM, Smith DG, Czerniecki JM, Campbell KM, Malchow DM, Robinson RLR. Back pain as a secondary disability in persons with lower limb amputations. Arch Phys Med Rehab. 2001;82:731–734. doi: 10.1053/apmr.2001.21962. [DOI] [PubMed] [Google Scholar]
- Gillet A, Duboy J, Barbier F, Armand S, Jeddi R, Lepoutre FX, Allard P. Contribution of accelerated body masses to able-bodied gait. Am J Phys Med Rehab. 2003;82:101–109. doi: 10.1097/00002060-200302000-00004. [DOI] [PubMed] [Google Scholar]
- Hendershot BD, Wolf EJ. Three-dimensional joint reaction forces and moments at the low back during over-ground walking in persons with unilateral lower-extremity amputation. Clin Biomech. 2014;29:235–242. doi: 10.1016/j.clinbiomech.2013.12.005. [DOI] [PubMed] [Google Scholar]
- Hendershot BD, Wolf EJ. Persons with unilateral transfemoral amputation have altered lumbosacral kinetics during sitting and standing movements. Gait Posture. 2015a;42:204–209. doi: 10.1016/j.gaitpost.2015.05.011. [DOI] [PubMed] [Google Scholar]
- Hendershot BD, Wolf IJ. Mediolateral Joint Powers at the Low Back Among Persons With Unilateral Transfemoral Amputation. Arch Phys Med Rehab. 2015b;96:154–157. doi: 10.1016/j.apmr.2014.07.402. [DOI] [PubMed] [Google Scholar]
- Kumar S. Theories of musculoskeletal injury causation. Ergonomics. 2001;44:17–47. doi: 10.1080/00140130120716. [DOI] [PubMed] [Google Scholar]
- Mcfadyen BJ, Winter DA. An Integrated Biomechanical Analysis of Normal Stair Ascent and Descent. J Biomech. 1988;21:733–744. doi: 10.1016/0021-9290(88)90282-5. [DOI] [PubMed] [Google Scholar]
- Michaud SB, Gard SA, Childress DS. A preliminary investigation of pelvic obliquity patterns during gait in persons with transtibial and transfemoral amputation. J Rehabil Res Dev. 2000;37:1–10. [PubMed] [Google Scholar]
- Morgenroth DC, Gellhorn AC, Suri P. Osteoarthritis in the disabled population: a mechanical perspective. PM & R: the journal of injury, function, and rehabilitation. 2012;4:S20–27. doi: 10.1016/j.pmrj.2012.01.003. [DOI] [PubMed] [Google Scholar]
- Nadeau S, McFadyen BJ, Malouin F. Frontal and sagittal plane analyses of the stair climbing task in healthy adults aged over 40 years: what are the challenges compared to level walking? Clin Biomech. 2003;18:950–959. doi: 10.1016/s0268-0033(03)00179-7. [DOI] [PubMed] [Google Scholar]
- Pell JP, Donnan PT, Fowkes FGR, Ruckley CV. Quality-of-Life Following Lower-Limb Amputation for Peripheral Arterial-Disease. Eur J Vascular Surg. 1993;7:448–451. doi: 10.1016/s0950-821x(05)80265-8. [DOI] [PubMed] [Google Scholar]
- Powers CM, Boyd LA, Fontaine CA, Perry J. The influence of lower-extremity muscle force on gait characteristics in individuals with below-knee amputations secondary to vascular disease. Phys Ther. 1996;76:369–377. doi: 10.1093/ptj/76.4.369. [DOI] [PubMed] [Google Scholar]
- Powers CM, Boyd LA, Torburn L, Perry J. Stair ambulation in persons with transtibial amputation: An analysis of the Seattle LightFoot(TM) J Rehabil Res Dev. 1997;34:9–18. [PubMed] [Google Scholar]
- Prinsen EC, Nederhand MJ, Rietman JS. Adaptation Strategies of the Lower Extremities of Patients With a Transtibial or Transfemoral Amputation During Level Walking: A Systematic Review. Arch Phys Med Rehab. 2011;92:1311–1325. doi: 10.1016/j.apmr.2011.01.017. [DOI] [PubMed] [Google Scholar]
- Reeves ND, Spanjaard M, Mohagheghi AA, Baltzopoulos V, Maganaris CN. The demands of stair descent relative to maximum capacities in elderly and young adults. Journal of electromyography and kinesiology: official journal of the International Society of Electrophysiological Kinesiology. 2008;18:218–227. doi: 10.1016/j.jelekin.2007.06.003. [DOI] [PubMed] [Google Scholar]
- Rueda FM, Diego IMA, Sanchez AM, Tejada MC, Montero FMR, Page JCM. Knee and hip internal moments and upper-body kinematics in the frontal plane in unilateral transtibial amputees. Gait Posture. 2013;37:436–439. doi: 10.1016/j.gaitpost.2012.08.019. [DOI] [PubMed] [Google Scholar]
- Sagawa Y, Turcot K, Armand S, Thevenon A, Vuillerme N, Watelain E. Biomechanics and physiological parameters during gait in lower-limb amputees: A systematic review. Gait Posture. 2011;33:511–526. doi: 10.1016/j.gaitpost.2011.02.003. [DOI] [PubMed] [Google Scholar]
- Sawacha Z, Gabriella G, Cristoferi G, Guiotto A, Avogaro A, Cobelli C. Diabetic gait and posture abnormalities: a biomechanical investigation through three dimensional gait analysis. Clin Biomech. 2009;24:722–728. doi: 10.1016/j.clinbiomech.2009.07.007. [DOI] [PubMed] [Google Scholar]
- Schmalz T, Blumentritt S, Marx B. Biomechanical analysis of stair ambulation in lower limb amputees. Gait Posture. 2007;25:267–278. doi: 10.1016/j.gaitpost.2006.04.008. [DOI] [PubMed] [Google Scholar]
- Schwartz MH, Rozumalski A. A new method for estimating joint parameters from motion data. J Biomech. 2005;38:107–116. doi: 10.1016/j.jbiomech.2004.03.009. [DOI] [PubMed] [Google Scholar]
- Smith JD, Ferris AE, Heise GD, Hinrichs RN, Martin PE. Oscillation and reaction board techniques for estimating inertial properties of a below-knee prosthesis. Journal of visualized experiments: JoVE. 2014 doi: 10.3791/50977. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Soares ASOD, Yamaguti EY, Mochizuki L, Amadio AC, Serrao JC. Biomechanical parameters of gait among transtibial amputees: a review. Sao Paulo Medical Journal. 2009;127:302–309. doi: 10.1590/S1516-31802009000500010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wu G, van der Helm FCT, Veeger HEJ, Makhsous M, Van Roy P, Anglin C, Nagels J, Karduna AR, McQuade K, Wang XG, Werner FW, Buchholz B. ISB recommendation on definitions of joint coordinate systems of various joints for the reporting of human joint motion – Part II: shoulder, elbow, wrist and hand. J Biomech. 2005;38:981–992. doi: 10.1016/j.jbiomech.2004.05.042. [DOI] [PubMed] [Google Scholar]
- Yack HJ, Nielsen DH, Shurr DG. Kinetic Patterns During Stair Ascent in Patients with Transtibial Amputations Using Three Different Prostheses. Journal of Prosthetics and Orthotics. 1999;11:57–62. [Google Scholar]
- Zachazewski JE, Riley PO, Krebs DE. Biomechanical analysis of body mass transfer during stair ascent and descent of healthy subjects. J Rehabil Res Dev. 1993;30:412–422. [PubMed] [Google Scholar]