

Abstract
Background
Coeliac disease might affect school performance due to its effect on cognitive performance and related health consequences that might increase school absenteeism. The aim of this study was to investigate whether children with coeliac disease performed differently on completion of ninth grade in school compared with children without coeliac disease.
Methods
Analysis was performed on a population of 445 669 children born in Sweden between 1991 and 1994 of whom 1767 were diagnosed with coeliac disease. School performance at ninth grade was the outcome and coeliac disease was the exposure. Other covariates included sex, Apgar score at 5 min, small for gestational age, year of birth, family type, parental education and income.
Results
There was no association between coeliac disease and school performance at ninth grade (adjusted coefficient −2.4, 95% CI 5.1 to 0.4). A weak association was established between late coeliac diagnosis and higher grades, but this disappeared after adjusting for parent socioeconomic conditions. Being small for gestational age affected performance negatively (adjusted coefficient −6.9, 95% CI 8.0 to 5.7). Grade scores were significantly lower in children living with a single parent (adjusted coefficient −20.6, 95% CI 20.9 to 20.2), compared with those with married/cohabiting parents. A positive association was found between scores at ninth grade and parental education and income.
Conclusion
Coeliac disease diagnosis during childhood is not associated with poor school performance at ninth grade.
Keywords: achievement, celiac, disease, education, grades, income, performance and school
What is already known on this topic?
Childhood chronic diseases are associated with increased risk of low school performance.
Adulthood coeliac disease is associated with low cognitive ability.
Coeliac disease is associated with several health consequences that may increase school absenteeism.
What this study adds?
Childhood coeliac disease is not associated with school performance at ninth grade.
A weak association was found between late coeliac disease diagnosis and high grades, but this disappeared after adjusting for socioeconomic conditions.
The study confirms an association between low school performance and living in a single parent household, low parental education and low parental income.
Introduction
Current evidence suggests a link between health and educational achievements, even though this does not necessarily imply causation.1 2 Research on childhood health and school performance has shown that low birth weight has a negative impact on children’s intellectual capacity3–5 as well as school achievements.6 7 Currie and Hyson point out that there are relatively few studies on the effect of health after birth and school performance due to a lack of suitable data.3 However, the few existing studies suggest such a relationship for several chronic diseases such as diabetes, sickle cell anaemia, seizure disorders, asthma and obesity.2 8 9
Coeliac disease is a chronic disorder occurring after birth, but often during childhood.10 Previously coeliac disease was considered rare, but it is now quite common, with an increasing occurrence in many populations. On average the prevalence is estimated to be about 1%, but considerably higher in some countries, with up to 3% in some population segments.11 Coeliac disease has a multifactorial aetiology, with genetics and gluten as necessary factors, but other environmental factors have been implicated.12–16 We have been unable to find any published studies on coeliac disease and school achievement. However, a few available closely related studies have investigated the effect of coeliac disease on adult intellectual ability and cognitive impairment.17–21
Coeliac disease has systemic effects, it mainly affects the gastrointestinal tract with enteropathy resulting in malabsorption. Today there is only one effective treatment, which is a lifelong strict gluten-free diet, and dietary compliance is challenging. Left untreated, the disease can give a wide range of health consequences such as failure to thrive, nausea/vomiting, diarrhoea or obstipation, anaemia and fatigue.22–24 Many of these health problems can decrease school attendance and contribute to low school performance.
Several studies have shown coeliac disease to negatively influence the cognitive performance and intellectual ability of adult patients.17–21 In the USA, lower cognitive ability among the elderly with coeliac disease has been indicated.17 To our knowledge, no studies to date have looked at coeliac disease in relation to cognitive performance, intellectual ability or school performance in the child population.
Our hypothesis is that childhood coeliac disease negatively affects school performance at ninth grade. Performance at ninth grade is a good measure for overall school performance as these scores are used in determining transition into higher secondary school and as such are important for the entire educational trajectories. Thus, in our study we assessed school performance at ninth grade and how this differs between children with coeliac disease and those without, while adjusting for relevant health, demographic and socioeconomic factors.
Methods
Study population and data availability
The study population consisted of all children born in Sweden between 1991 and 1994. Selection of this birth cohort was based on data availability. It is from 1991 that most cases were reported to the Swedish National Childhood Celiac Disease Register with a personal identity number, a requirement for linkage of registers. Since data were only available up to 2010, majority of these children had only completed ninth grade as the highest level of education.
A total of 506 357 children were identified, of whom 60 688 were excluded either as they were born outside Sweden and therefore lacked health data from birth, or because they lacked data on ninth grade scores (figure 1). A total of 445 669 children were included in the analysis, of whom 1767 had coeliac disease diagnosed, as shown in figure 1.
Figure 1.
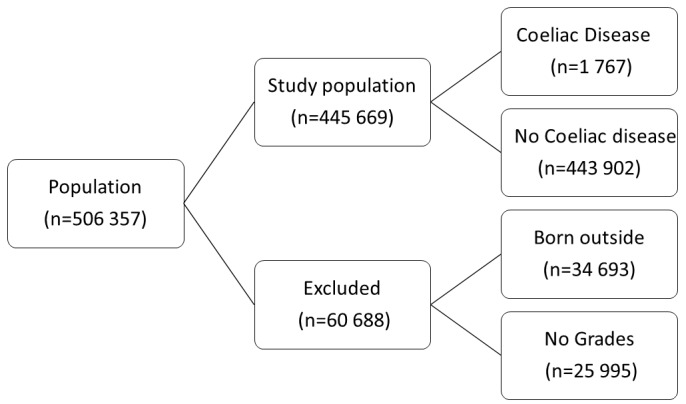
Selection of the study population.
Data were made available through the Swedish Initiative for Research on Microdata in the Medical and Social Sciences (Umeå SIMSAM Lab) hosting data up to 2010.25 This is a comprehensive database with selected data from Statistics Sweden, the National Board of Health and Welfare, and the Swedish National Childhood Celiac Disease Incidence Register.26 Statistics Sweden performed data linkage using personal identity numbers, but before delivery to us the data were anonymised.27
Statistics Sweden’s Longitudinal Integration Database for Health Insurance and Labour Market (LISA database) provided information on the total population, parents’ education and income, and the Swedish National Agency for Education’s Pupil Register provided data on school grades. The National Board of Health and Welfare provided data on perinatal events through its Medical Birth Register.
Outcome
Grade scores on completion of the ninth year of compulsory school education were the outcome of interest. Compulsory school education is from first to ninth grades and each grade is equivalent to 1 year of schooling. A national examination is administered in the ninth year and final grade scores are calculated as the sum of the 16 best subject grades in the final year using grading points. The grading points offer a summary of performance during the final compulsory school year, with grades ranging from 0 to 320 points. For every subject, students are assigned a grade ranging from 0 to 20, where 0 represents failure, 10 is E, 12 is D, 15 is C, 17.5 is B and 20 is A. The lowest obtainable score on all subjects is 0, implying that one has scored 0 in all the tested subjects, while the highest is 320, implying that one has scored 20 in all 16 subjects.
Independent variable: coeliac disease cases
A total of 1767 children with coeliac disease were identified from all the 47 paediatric units in the country by accessing the Swedish National Childhood Celiac Disease Incidence Register.26 Ascertainment of coeliac disease status was based on the 1990 diagnostic criteria by ESPGHAN (the European Society for Paediatric Gastroenterology, Hepatology and Nutrition). This implies that coeliac disease is ascertained by a biopsy assessment of the small intestinal mucosa showing an enteropathy on a gluten-containing diet, followed by a clinical improvement after a change to a gluten-free diet. Child age at the coeliac disease diagnosis was given for the age intervals 0–5 years, 6–12 years and 13–15 years (15.9 years); in a subanalysis the youngest group was compared with the older groups.
Covariates: other characteristics
Variables were selected if they had been previously suggested to be associated with both health and school achievements. For child characteristics we included the following: sex, small for gestational age, Apgar score at 5 min (a measure of the newborn’s physical condition 5 min after birth) and year of birth. Sex was grouped into female and male, and there were no missing data. Apgar score at 5 min was categorised according to established criteria into low if the score was <7 and normal if the score was within the range of 7–10. Data were missing for 7%. Small for gestational age was precategorised into two groups (yes and no) according to the Swedish weight-based growth standards. Children are classified as small for gestational age if birth weight is 2 SD below the mean at a certain pregnancy length and not small for gestational age if otherwise. Data were missing for 9%. Year of birth ranged from 1991 to 1994, and this information was available for all children.
We included parental characteristics that previous studies have considered to be strongly associated with school performance and educational attainment.28–30 Initially, we planned to include maternal and paternal educational levels as two separate variables, but due to a strong correlation categorisation was based on the highest education of the mother or the father. This variable was divided into four groups: compulsory education (reference), upper secondary education, <2 years of university education and ≥2 years of university education. Maternal and paternal disposable income at the child’s completion of ninth grade (per 100 SEK) was categorised into tertiles. The groups were labelled low (reference), middle and high (information was missing for fathers’ income for 4% and mother’s income for 2%). Type of family was categorised into two groups: married/cohabiting and single for all those living alone, that is, widows, widowers, divorced, separated and never married.
Statistical analysis
The multiple linear regression procedure was used to assess how well coeliac disease predicted ninth grade scores. Other studied covariates were added step-by-step to assess any confounding, and this was done by running four models separately. Model 1 consisted of a coeliac disease status alone. In model 2, the child’s demographic factors were added (sex, year of birth). In model 3, child’s health factors (Apgar score and small for gestational age) were added. In model 4, family type, parental education, and mother and father’s income were added. In a separate analysis that only included coeliac disease cases, we checked whether age at diagnosis of coeliac disease affected the performance at ninth grade. In this analysis, the first model (model 1C) only included age at diagnosis of the disease; however, thereafter the models were built stepwise (models 2C–4C) as in the previous analyses. A statistically significant association was defined as having 95% CIs that did not include 0, corresponding to p<0.05. Statistics were calculated using SPSS V.24.0 2000.
Ethical consideration
This study was approved by the Research Ethics Committee of the Umeå University. Subject information was anonymised by Statistics Sweden prior to the analyses.
Result
During this follow-up period, the mean age for completion of ninth grade was 16 years and the mean grade score for this population was 207 (SD=66). Additional basic descriptive statistics are shown in table 1.
Table 1.
The study population with mean scores at ninth grade completion (with SDs) given for each child and parental characteristics, for coeliac disease and non-coeliac disease children
| Characteristics | Mean grades (SD) | Coeliac disease (n=1767) | Non-coeliac disease (n=443 902) | Total number |
| Sex | ||||
| Male | 198 (62.5) | 651 | 226 963 | 227 614 |
| Female | 220 (64.8) | 1116 | 216 939 | 218 055 |
| Apgar score at 5 min | ||||
| 7–10 | 209 (64.5) | 1733 | 431 895 | 433 628 |
| <7 | 206 (64.8) | 12 | 3290 | 3302 |
| Small for gestational age | ||||
| No | 209 (64.6) | 1659 | 431 895 | 418 598 |
| Yes | 198 (67.1) | 38 | 3290 | 10 096 |
| Age at diagnosis (years) | ||||
| 0–5 | 208 (63.3) | 671 | 0 | 671 |
| 6–12 | 211 (66.5) | 806 | 0 | 806 |
| 13–15 | 220 (62.1) | 290 | 0 | 290 |
| Year of birth | ||||
| 1991 | 207 (64.6) | 402 | 115 529 | 115 931 |
| 1992 | 209 (64.7) | 451 | 114 225 | 114 676 |
| 1993 | 209 (64.8) | 598 | 109 377 | 109 975 |
| 1994 | 210 (64.3) | 316 | 104 771 | 105 087 |
| Type of family | ||||
| Married/cohabiting | 216 (60.1) | 1268 | 312 771 | 314 039 |
| Single | 190 (70.7) | 498 | 130 856 | 131 354 |
| Parental education | ||||
| Compulsory | 163 (71.5) | 35 | 15 225 | 15 260 |
| Upper secondary | 191 (63.1) | 848 | 209 505 | 210 353 |
| <2 years university | 219 (58.9) | 143 | 33 735 | 33 878 |
| ≥2 years university | 231 (58.5) | 741 | 185 437 | 186 178 |
| Mother’s income | ||||
| Low | 198 (66.4) | 503 | 136 877 | 137 380 |
| Middle | 206 (62.2) | 607 | 149 267 | 149 874 |
| High | 223 (62.1) | 634 | 150 327 | 150 961 |
| Father’s income | ||||
| Low | 192 (68.6) | 429 | 131 453 | 131 882 |
| Middle | 206 (60.1) | 653 | 146 966 | 147 619 |
| High | 229 (57.9) | 622 | 149 310 | 149 932 |
Child characteristics and school performance
We found no significant association between coeliac disease and school performance at ninth grade (table 2). In these birth cohorts (1991–1994), girls performed better than boys at ninth grade. Using the 1991 birth cohort as a reference, a noticeable annual drop in grades was seen for later cohorts. Apgar score showed no significant association with school grades while being born small for gestational age appeared to negatively impact children’s performance. Notably, children with coeliac disease diagnosed at 13–15 years of age performed better in ninth grade compared with children diagnosed earlier in life; however, this relationship disappeared after adjusting for parental characteristics (table 3).
Table 2.
Impact of coeliac disease on school achievement at ninth grade completion, taking child and parental characteristics into account
| Child and parental characteristics | Model 1 | Model 2 | Model 3 | Model 4 | |||||
| b | 95% CI | b | 95% CI | b | 95% CI | b | 95% CI | ||
| Coeliac disease status | No | Ref | Ref | Ref | Ref | ||||
| Yes | 2.8 | –0.2 to 5.8 | –0.5 | −3.5 to 2.5 | −0.6 | −3.7 to 2.4 | −2.4 | −5.1 to 0.4 | |
| Sex | Male | Ref | Ref | Ref | |||||
| Female | 22.4** | 21.9 to 22.7 | 22.5** | 22.1 to 22.9 | 22.5** | 22.2 to 22.9 | |||
| Year of birth | 1991 | Ref | Ref | Ref | |||||
| 1992 | 2.1** | 1.5 to 2.6 | 1.9** | 1.5 to 2.5 | −0.6* | −1.1 to −0.1 | |||
| 1993 | 2.9** | 2.5 to 3.5 | 2.9** | 2.4 to 3.5 | −1.4** | −1.9 to −0.9 | |||
| 1994 | 3.1** | 2.6 to 3.6 | 2.9** | 2.4 to 3.5 | −2.5** | −2.9 to −1.9 | |||
| Apgar score at 5 min | 7–10 | Ref | Ref | ||||||
| <7 | −1.8 | −4.1 to 0.5 | −1.0 | −3.1 to 1.1 | |||||
| Small for gestational age | No | Ref | Ref | ||||||
| Yes | −10.8** | −12.0 to −9.5 | −6.9** | −8.0 to −5.7 | |||||
| Family type | Married/cohabiting | Ref | |||||||
| Single | −20.6** | −20.9 to −20.2 | |||||||
| Parental education | ≤9 years schooling | Ref | |||||||
| Upper secondary | 21.5** | 20.5 to 22.5 | |||||||
| University <2 years | 42.5** | 41.3 to 43.6 | |||||||
| University ≥2 years | 52.5** | 51.5 to 53.5 | |||||||
| Mother’s income | Low | Ref | |||||||
| Middle | 5.5** | 5.0 to 5.9 | |||||||
| High | 15.4** | 14.9 to 15.8 | |||||||
| Father’s income | Low | Ref | |||||||
| Middle | 9.3** | 8.8 to 9.7 | |||||||
| High | 22.1** | 21.6 to 22.5 | |||||||
Model 1 contains only coeliac disease status, model 2 contains coeliac disease status plus children’s demographic characteristics, model 3 contains model 2 plus children’s health characteristics, and model 4 contains model 3 plus parental characteristic.
Ordinary least squares regression, b=unstandardised coefficients, n=445 669.
*p<0.05; **p<0.001.
Table 3.
Impact of age at diagnosis of coeliac disease on school achievement at ninth grade completion, taking child and parental characteristics into account
| Child and parental characteristics | Model 1C | Model 2C | Model 3C | Model 4C | |||||
| b | 95% CI | b | 95% CI | b | 95% CI | b | 95% CI | ||
| Age at diagnosis (years) | 0–12 | Ref | Ref | Ref | Ref | ||||
| 13–15 | 9.9* | 1.8 to 18.1 | 10.5* | 2.3 to 18.6 | 11.6* | 3.3 to 19.9 | 7.1 | −0.2 to 14.8 | |
| Sex | Male | Ref | Ref | Ref | |||||
| Female | 22.1** | 15.9 to 28.3 | 21.3** | 14.9 to 27.6 | 22.9** | 17.5 to 28.6 | |||
| Year of birth | 1991 | Ref | Ref | Ref | |||||
| 1992 | −4.6 | −13.2 to 3.9 | −3.9 | −12.7 to 4.9 | −7.3 | −13.8 to 2.0 | |||
| 1993 | 5.5 | −2.6 to 13.6 | 5.8 | −2.5 to 14.1 | 0.1 | −6.2 to 8.7 | |||
| 1994 | 3.1 | −6.3 to 12.5 | 2.8 | −6.8 to 12.0 | −1.3 | −9.4 to 7.2 | |||
| Apgar score at 5 min | 7–10 | Ref | Ref | ||||||
| <7 | 11.2 | −26.8 to 49.2 | 15.1 | −20.8 to 45.5 | |||||
| Small for gestational age | No | Ref | Ref | ||||||
| Yes | −14.8 | −35.7 to 6.1 | −9.4 | −26.7 to 8.9 | |||||
| Family type | Married/cohabiting | Ref | |||||||
| Single | −22.4** | −28.0 to −15.7 | |||||||
| Mothers’ education | ≤9 years schooling | Ref | |||||||
| Upper secondary | 23.1** | 10.0 to 31.7 | |||||||
| University <2 years | 46.2** | 27.8 to 61.2 | |||||||
| University ≥2 years | 45.3** | 31.6 to 54.7 | |||||||
| Mother’s income | Low | Ref | |||||||
| Middle | 6.4 | 1.2 to 14.8 | |||||||
| High | 12.8* | 6.2 to 20.2 | |||||||
| Father’s education | ≤9 years schooling | Ref | |||||||
| Upper secondary | 15.1** | 7.2 to 22.9 | |||||||
| University <2 years | 31.9** | 19.4 to 43.4 | |||||||
| University >2 years | 32.0** | 21.6 to 41.0 | |||||||
| Father’s income | Low | Ref | |||||||
| Middle | 8.6** | 2.3 to 16.0 | |||||||
| High | 17.7** | 11.1 to 25.8 | |||||||
Model 1C contains age at diagnosis, model 2C contains age at diagnosis plus children’s demographic characteristics, model 3C contains model 2 plus children’s health characteristics, and model 4C contains model 3 plus parental characteristics.
Ordinary least squares regression, b=unstandardised coefficients, n=1767.
*p<0.05; **p<0.001.
Parental characteristics and school performance
Living in a household with an unmarried/non-cohabiting parent was significantly associated with poorer performance at ninth grade compared with living in a household of married/cohabiting parents. Scores at ninth grade were also significantly associated with parental education and income; the higher the levels of parental education and income, the higher the grade scores on completion of the ninth grade. For all interaction terms included, we found no statistically significant association and thus these results are not shown.
Discussion
From existing research, we know that health is important for academic performance and eventual educational attainment. What we did not know was whether coeliac disease influences school performance. Based on findings from this study, coeliac disease is not significantly associated with grade scores on completion of the ninth grade. However, being small for gestational age, being born after 1991 and living in a single parent household were all strongly associated with low performance. In contrast, high performance at ninth grade was predicted by being female and having parents with high education and income.
Coeliac disease and school performance
The absence of an association between coeliac disease and school performance is probably due to early coeliac disease diagnosis and adherence to a gluten-free diet. This study hypothesised that celiac disease may affect school performance based on evidence from earlier studies showing a link between coeliac disease and cognitive performance. However, these earlier studies were performed on adult populations, whereas cases in the present study were diagnosed between 0 and 15 years of age. It may be that the negative effect of coeliac disease is only evident following long exposure to gluten such as in individuals with a delayed diagnosis. Hu et al showed the impact of coeliac disease on cognitive performance to be more pronounced in the elderly.17 Similarly, Hadjivassiliou et al reported that the onset of symptoms of cognitive dysfunction occurred on average at 53 years of age among patients with gluten ataxia.21 Casella et al confirmed that poor cognitive performance was pronounced in patients diagnosed with coeliac disease during adulthood.18 Additionally, it is plausible that our cases adhere to the recommended strict gluten-free diet and thus are living a relatively normal life following early diagnosis. Even though we did not include data on nutrition, the earlier study from this population reported an 82% gluten-free diet compliance rate.31 Interestingly, age at diagnosis did not appear to play a significant role. Children diagnosed after 13 years of age tended to perform better. However, this could be due to a socioeconomic bias, as this relationship disappeared when we controlled for resources, that is, parental education and income.
Other child characteristics and school performance
The finding that children born small for gestational age performed poorly at ninth grade compared with others is in line with previous studies.32 The mechanism underlying pregnancy length at birth and performance at ninth grade is likely to be multifactorial; it has been suggested that preterm children have an increased risk of delayed development, cognitive impairments, learning disabilities, behavioural problems and emotional problems, among other issues.33 These factors negatively impact school performance. Our findings on decreasing school performance in birth cohorts over time and better performance among girls are also in line with earlier studies.34 This study does not explain why there is decrease in performance at ninth grade in the recent years or as to why girls outperform boys, further research is needed.
Parental conditions and school performance
We reported that school performance at ninth grade was positively associated with parental income and education. This finding confirms a well-documented association between socioeconomic status and academic achievement.35 Parental income reflects the economic and social resources available to the child, and parental education was linked to both parental income and levels of engagement in the child’s education.36 Low performance was significantly higher in children living with non-married/non-cohabiting parents, and similar observations have been shown by earlier studies.37 This negative effect has previously been attributed to detrimental stress arising from parental conflict following divorce/separation, the meagre economic resources typical in most one-parent homes and time pressures on single parents making them less able to participate in the child’s schooling.37 38
Conclusion
In conclusion, coeliac disease diagnosed during childhood in Sweden is not associated with poor school performance at ninth grade.
Acknowledgments
The Umeå SIMSAM Lab data infrastructure used in this study was developed with support from the Swedish Research Council and by strategic funds from Umeå University.
Footnotes
Contributors: MS and KN were responsible for the conceptualisation of the study, supervised the analysis process and offered quality control of both data and the final study results. AI provided clinical insights and interpretation of the study variables and the research findings. FN performed the statistical analyses and wrote the manuscript. All authors contributed to the selection of the studied variables, choice of study design, interpretation of study findings, and revision of the manuscript, and have approved the submitted version of the manuscript.
Funding: The research has been supported by grants from the Swedish Science Council (Dnr: 2014-1992) and Markus and Marianne Wallenbergs fund (Dnr: 2014.0154).
Competing interests: None declared.
Ethics approval: Swedish Ethical Review Board.
Provenance and peer review: Not commissioned; externally peer reviewed.
Data sharing statement: All data for this study are available through the Umeå SIMSAM Lab. More data similar to the one used in this study can be obtained from Statistics Sweden and the Swedish National Board of Health and Welfare upon request and ethical clearance.
References
- 1. Brown JO, Grubb SB, Wicker TE, et al. Health variables and school achievement. J Sch Health 1985;55:21–3. 10.1111/j.1746-1561.1985.tb04068.x [DOI] [PubMed] [Google Scholar]
- 2. Forrest CB, Bevans KB, Riley AW, et al. Health and school outcomes during children’s transition into adolescence. J Adolesc Health 2013;52:186–94. 10.1016/j.jadohealth.2012.06.019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Currie J, Hyson R. Is the impact of Health Shocks cushioned by socioeconomic status? the case of low birthweight. Am Econ Rev 1999;89:245–50. 10.1257/aer.89.2.245 [DOI] [Google Scholar]
- 4. Bergvall N, Iliadou A, Tuvemo T, et al. Birth characteristics and risk of low intellectual performance in early adulthood: are the associations confounded by socioeconomic factors in adolescence or familial effects? Pediatrics 2006;117:714–21. 10.1542/peds.2005-0735 [DOI] [PubMed] [Google Scholar]
- 5. Torche F, Echevarría G. The effect of birthweight on childhood cognitive development in a middle-income country. Int J Epidemiol 2011;40:1008–18. 10.1093/ije/dyr030 [DOI] [PubMed] [Google Scholar]
- 6. Ross G, Lipper EG, Auld PA, et al. Educational status and school-related abilities of very low birth weight premature children. Pediatrics 1991;88:1125–34. [PubMed] [Google Scholar]
- 7. Saigal S, Szatmari P, Rosenbaum P, et al. Cognitive abilities and school performance of extremely low birth weight children and matched term control children at age 8 years: a regional study. J Pediatr 1991;118:751–60. 10.1016/S0022-3476(05)80043-5 [DOI] [PubMed] [Google Scholar]
- 8. Taras H, Potts-Datema W. Chronic health conditions and student performance at school. J Sch Health 2005;75:255–66. 10.1111/j.1746-1561.2005.00034.x [DOI] [PubMed] [Google Scholar]
- 9. Crump C, Rivera D, London R, et al. Chronic health conditions and school performance among children and youth. Ann Epidemiol 2013;23:179–84. 10.1016/j.annepidem.2013.01.001 [DOI] [PubMed] [Google Scholar]
- 10. Green PH, Jabri B. Coeliac disease. Lancet 2003;362:383–91. 10.1016/S0140-6736(03)14027-5 [DOI] [PubMed] [Google Scholar]
- 11. Myléus A, Ivarsson A, Webb C, et al. Celiac disease revealed in 3% of swedish 12-year-olds born during an epidemic. J Pediatr Gastroenterol Nutr 2009;49:170–6. 10.1097/MPG.0b013e31818c52cc [DOI] [PubMed] [Google Scholar]
- 12. Namatovu F, Olsson C, Lindkvist M, et al. Maternal and perinatal conditions and the risk of developing celiac disease during childhood. BMC Pediatr 2016;16:1–10. 10.1186/s12887-016-0613-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Namatovu F, Sandström O, Olsson C, et al. Celiac disease risk varies between birth cohorts, generating hypotheses about causality: evidence from 36 years of population-based follow-up. BMC Gastroenterol 2014;14:59 10.1186/1471-230X-14-59 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Namatovu F, Strömgren M, Ivarsson A, et al. Neighborhood conditions and celiac disease risk among children in Sweden. Scand J Public Health 2014;42:572–80. 10.1177/1403494814550173 [DOI] [PubMed] [Google Scholar]
- 15. Namatovu F, Lindkvist M, Olsson C, et al. Season and region of birth as risk factors for coeliac disease a key to the aetiology? Arch Dis Child 2016;101:1114–8. 10.1136/archdischild-2015-310122 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Roberts SE, Williams JG, Meddings D, et al. Perinatal risk factors and coeliac disease in children and young adults: a record linkage study. Aliment Pharmacol Ther 2009;29:222–31. 10.1111/j.1365-2036.2008.03871.x [DOI] [PubMed] [Google Scholar]
- 17. Hu WT, Murray JA, Greenaway MC, et al. Cognitive impairment and celiac disease. Arch Neurol 2006;63:1440–6. 10.1001/archneur.63.10.1440 [DOI] [PubMed] [Google Scholar]
- 18. Casella S, Zanini B, Lanzarotto F, et al. Cognitive performance is impaired in coeliac patients on gluten free diet: a case-control study in patients older than 65 years of age. Dig Liver Dis 2012;44:729–35. 10.1016/j.dld.2012.03.008 [DOI] [PubMed] [Google Scholar]
- 19. Lichtwark IT, Newnham ED, Robinson SR, et al. Cognitive impairment in coeliac disease improves on a gluten-free diet and correlates with histological and serological indices of disease severity. Aliment Pharmacol Ther 2014;40:160–70. 10.1111/apt.12809 [DOI] [PubMed] [Google Scholar]
- 20. Hallert C, Aström J. Intellectual ability of adults after lifelong intestinal malabsorption due to coeliac disease. J Neurol Neurosurg Psychiatry 1983;46:87–9. 10.1136/jnnp.46.1.87 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Hadjivassiliou M, Sanders DS, Grünewald RA, et al. Gluten sensitivity: from gut to brain. Lancet Neurol 2010;9:318–30. 10.1016/S1474-4422(09)70290-X [DOI] [PubMed] [Google Scholar]
- 22. Kurppa K, Collin P, Sievänen H, et al. Gastrointestinal symptoms, quality of life and bone mineral density in mild enteropathic coeliac disease: a prospective clinical trial. Scand J Gastroenterol 2010;45:305–14. 10.3109/00365520903555879 [DOI] [PubMed] [Google Scholar]
- 23. Kurien M, Barratt SM, Sanders DS. Functional gastrointestinal disorders and coeliac disease in adults - negative impact on quality of life. Aliment Pharmacol Ther 2011;34:1044–5. 10.1111/j.1365-2036.2011.04831.x [DOI] [PubMed] [Google Scholar]
- 24. Mukherjee R, Kelly CP, Leffler DA. Gastrointestinal Cancer in celiac disease: "the first days are the hardest days, don’t you worry anymore?". Clin Gastroenterol Hepatol 2012;10:4–6. 10.1016/j.cgh.2011.09.028 [DOI] [PubMed] [Google Scholar]
- 25. Lindgren U, Nilsson K, de Luna X, et al. Data Resource Profile: Swedish Microdata Research from Childhood into Lifelong Health and Welfare (Umeå SIMSAM Lab). Int J Epidemiol 2016;45:dyv358 10.1093/ije/dyv358 [DOI] [PubMed] [Google Scholar]
- 26. Ivarsson A, Persson LA, Nyström L, et al. Epidemic of coeliac disease in Swedish children. Acta Paediatr 2000;89:165–71. 10.1111/j.1651-2227.2000.tb01210.x [DOI] [PubMed] [Google Scholar]
- 27. Ludvigsson JF, Otterblad-Olausson P, Pettersson BU, et al. The swedish personal identity number: possibilities and pitfalls in healthcare and medical research. Eur J Epidemiol 2009;24:659–67. 10.1007/s10654-009-9350-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Evans GW, Schamberg MA. Childhood poverty, chronic stress, and adult working memory. Proc Natl Acad Sci U S A 2009;106:6545–9. 10.1073/pnas.0811910106 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Murnane RJ. Improving the education of children living in poverty. Future Child 2007;17:161–82. 10.1353/foc.2007.0019 [DOI] [PubMed] [Google Scholar]
- 30. Chen E, Martin AD, Matthews KA. Trajectories of socioeconomic status across children’s lifetime predict health. Pediatrics 2007;120:e297–e303. 10.1542/peds.2006-3098 [DOI] [PubMed] [Google Scholar]
- 31. Webb C, Myléus A, Norström F, et al. High adherence to a gluten-free diet in adolescents with screening-detected celiac disease. J Pediatr Gastroenterol Nutr 2015;60:54–9. 10.1097/MPG.0000000000000571 [DOI] [PubMed] [Google Scholar]
- 32. Noble KG, Fifer WP, Rauh VA, et al. Academic achievement varies with gestational age among children born at term. Pediatrics 2012;130:e257–e264. 10.1542/peds.2011-2157 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Stjernqvist K, Svenningsen NW. Ten-year follow-up of children born before 29 gestational weeks: health, cognitive development, behaviour and school achievement. Acta Paediatr 1999;88:557–62. 10.1111/j.1651-2227.1999.tb00175.x [DOI] [PubMed] [Google Scholar]
- 34. Blanchenay P, Burns T, Köster F. Shifting Responsibilities-20 Years of Education Devolution in Sweden. Sweden: OECD Publishing. [Google Scholar]
- 35. Sirin SR, Status S. Socioeconomic status and Academic Achievement: a Meta-Analytic Review of Research. Rev Educ Res 2005;75:417–53. 10.3102/00346543075003417 [DOI] [Google Scholar]
- 36. Szumski G, Karwowski M. School achievement of children with intellectual disability: the role of socioeconomic status, placement, and parents' engagement. Res Dev Disabil 2012;33:1615–25. 10.1016/j.ridd.2012.03.030 [DOI] [PubMed] [Google Scholar]
- 37. Amato PR. Children of divorce in the 1990s: an update of the Amato and Keith (1991) meta-analysis. J Fam Psychol 2001;15:355–70. 10.1037/0893-3200.15.3.355 [DOI] [PubMed] [Google Scholar]
- 38. Sl P, Dronkers J, Hampden‐Thompson G, et al. Family Policies and Children’s School Achievement in Single- Versus Two-Parent Families. Journal of Marriage and Family 2003;65:681–99. [Google Scholar]