

Abstract
Background
Submitral left ventricular aneurysm is a rarely reported cardiac abnormality that is encountered commonly among blacks. So far, only one case has been reported from Ethiopia and East Africa.Our aim is to report an interesting and rare case that we encountered at St. Paul's Hospital Millennium Medical College.
Methods
In April 2017, a 25-year-old patient havingsubmitral left ventricular aneurysm with New York Heart Association (NYHA) class IV heart failure and mild left ventricular systolic dysfunctionreceived medical treatment at our institution. She had severe mitral regurgitation and aneurysmal thrombus. The diagnosis was easily made using GE Vivid E9 transthoracic echocardiography. She was given drugs for management of heart failure and anticoagulation.
Results
Our patient was discharged with a stable condition, and she had no early mortality. At 3 months' follow-up,shehad clinical improvement with NYHA class II heart failure, slight improvement of left ventricular systolic function, and resolution of the left ventricular thrombus. However, there waspersistent severe mitral regurgitation and aneurysm.
Conclusion
Submitral left ventricular aneurysm is a rare cardiac abnormality. Diagnosis can be easily made with echocardiography. Surgery is the definitive treatment. However, it is not currently available in the country and patients cannot afford treatment abroad.
Keywords: Ethiopia, heart failure, submitral aneurysm, thrombus
Introduction
Submitral left ventricle aneurysm is a rare cardiovascular disorder worldwide, but is mainly reported from West and South Africa (1). It is also more frequently reported from the Indian subcontinent (2). Among the various causes, congenital outpouching of the left ventricular wall adjacent to the posterior leaflet of the mitral valve is the commonly reportedpresentation (3). Other less frequently associated causes are: Takayasu's arteritis, rheumatic fever, tuberculosis, infective endocarditis, ischemic heart disease, and vascular tumors. There are also other reported cases with nounderlying cause identified. Although submitral aneurysm was predominantly reported in blacks of African origin, it was also identified in other races(2). In this article, we describe the clinical presentation, diagnostic work-up and existing treatments provided for a rarely reported case of submitral aneurysm in Ethiopia. We will also discuss the case and briefly review the current literature.
Case
A 25-year-old Ethiopian girl presented to the Emergency Department of St. Paul's Hospital Millennium Medical College, Addis Ababa, with a history of progressive dyspnea, orthopnea, paroxysmal nocturnal dyspnea, palpitation, and easy fatigabilityof two weeks duration. She had no history of fever, loss of appetite, weight loss or sweating. There was no history of hypertension, diabetes mellitus, dyslipidemia, kidney disease, smokingor any cardiac illness in the family.
On general examination, she was acutely sick-looking, and had blood pressure of 90/60 mmHg and regular heart rate of 96 beats per minute. On respiratory examination, there was bilateral fine crepitation and reduced air entry on both the lower one-third lung fields. The cardiovascular evaluation revealed elevated jugular venous pressure,displaced apical impulse, soft S1, and grade 4/6holo-systolic murmur at the apex that radiated to the left axilla. There was also grade 2 pan-systolic murmur at the left lower sternal border which increased in intensity during inspiration.
Laboratory examination showed white cell count 13,500/ µL, hemoglobin 12.5 g/dl, and ESR 15mm/1sthr. Liver, renal and thyroid function tests were normal. Abdominal ultrasound study was also normal. Chest x-ray showed cardiomegaly, grade 2 pulmonary edema, and bilateral pleural effusion. Electrocardiogram showed normal sinus rhythm and trans-thoracic echocardiogram revealed 4.0 cm by 3.9 cm single submitral aneurysm (Figure 1 (A and B) and Figure 2) on the posterolateral wall of the left ventricle. The patient also had severe eccentric mitral valve regurgitationand dilated left atrium and left ventricle. There was also mild left ventricular systolic dysfunction with an ejection fraction of about 40%, organized thrombus inside the aneurysm and mild tricuspid regurgitation (Figure 3 (A and B)). Due to lack of other diagnostic facilities and definitive surgical treatment in the country, the patient was managed with furosemide, enalapril, metoprolol, and warfarin. Moreover, she could not afford treatment abroad. After three months of medical management with the above medications, she had improvement of heart failure symptoms and resolution of the left ventricular thrombus. However, there was persistent severe mitral regurgitation and submitral aneurysm.
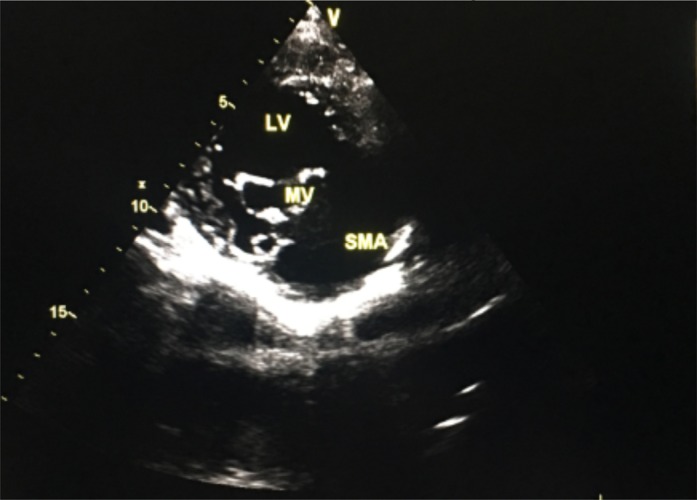
Figure 1.

Parasternal long axis (A), apical 4-chamber (B) views of submitral aneurysm
RA: right atrium, RV: right ventricle, LA: left atrium, LV: left ventricle, SMA: submitral aneurysm, PML: posterior mitral leaflet, AML: anterior mitral leaflet, AOV: aortic valv
Figure 2.
Parasternal short axis view of submitral aneurysm
Figure 3.

Apical 4-chamber view showing; (A) mitral regurgitation, tricuspid regurgitation (TR) and thrombus in the aneurysm at initial diagnosis (B) mitral regurgitation after three months
SMA: Submitral aneurysm, LV: left ventricle, MR: mitral regurgitation, TR: tricuspid regurgitation, L: vena contracta of mitral regurgitation
Discussion
Submitral aneurysm is commonly defined as an outpouching of the left ventricular wall invariably occurring adjacent to the posterior mitral leaflet (1). The posterior leaflet of the mitral valve is attached to the left ventricular myocardium through an annular ring. A weakness or disruption of this musculo-fibrous union results in the occurrence of a submitral aneurysm below the mitral leaflet (2). The etiology of submitral aneurysm remains uncertain, even though believed to be due to a congenital developmental defect (1). It is more frequently seen among blacks indicating a possible genetic predisposition (2).
Clinical symptoms arise as a result of secondary mitral valvular regurgitation in most cases due to loss of leaflet coaptation or occasionally from compression of cardiac structures by the aneurysmal saccausing chest pain, or the patient can be asymptomatic for many years (3). Most cases present with symptoms and signs of acute or chronic heart failure and cardiogenic shock and less commonly with acute coronary symptoms, left ventricular thrombus, arrhythmias or systemic embolization (4). Our case presented with progressive symptoms of congestive heart failure, severe mitral regurgitation, and aneurysmal thrombus indicating advanced stage of disease.
In the diagnosis of a submitral aneurysm, the electrocardiogram (ECG) and chest radiogram studies are frequently nonspecific. The frequently reported ECG findings are normal sinus rhythm, sinus tachycardia, supraventricular tachycardia, atrial fibrillation, low voltage, left ventricular hypertrophy, signs of ischemia, and non-specific ST-segment and T-wave changes. The chest radiography findings are variable degrees of cardiomegaly with or without pulmonary congestion and calcified bulge on the left heart. Before the advent of echocardiography, cardiac catheterization and angio-ventriculography were necessary to characterize the aneurysm (4). Nowadays, echocardiography can effectively diagnose and characterize submitral aneurysm using its various modalities; 2D, 3D, color Doppler, contrast and transesophageal echocardiography. Transthoracic echocardiography can clearly delineate aneurysmal dilatation in submitral location behind the posterior leaflet of the mitral valve, communicating with the left ventricular cavity through one or more necks (1). Current multi-detector cardiac CT and cardiac MRI studies have greatly improved the detailed description of a submitral aneurysm and detection of associated calcifications, thrombus formation and coronary artery compression (4). Our case had aneurysm behind the posterior mitral leaflet with a single neck and thrombus in the aneurysm and mildly depressed left ventricular systolic function.
The initial medical management of patients with a submitral aneurysm is stabilization with diuretics, afterload reducing agents and anti-coagulation to prevent thromboembolism. The definitive management is surgical treatment with aneurysmal repair or patch. If there is associated significant mitral regurgitation, either mitral valve repairor mitral valve replacement is warranted (5). Our patient needed definitive treatment with both aneurysmal repair and mitral valve repair. However, this modality of treatment is not currently available in Ethiopia. Thus, the patient has been on conservative managementwith drugs for heart failure and anticoagulation. After three months of follow-up, she is now in New York Heart Association class II, mild improvement of left ventricular systolic function with ejection fraction of 45%, and resolution of the left ventricular aneurysmal thrombus.
In conclusion, submitral aneurysm is a rare cardiovascular abnormality in Ethiopia and East Africa. However, it should be suspected in a young patient with significant mitral valve regurgitation, and echocardiography is essential for its diagnosis and the definitive management remains surgical correction.
Acknowledgement
We would like to thank our patient for giving us permission to report her medical information.
References
- 1.Morais H. Submitral Aneurysm: An Echocardiography Study in a Tertiary Center in Angola. J ClinExpCardiolog. 2014;5:290. [Google Scholar]
- 2.Baruah DK, Naresh Kumar PV, Reddy GSP, Ramesh Babu V. Submitral aneurysm of the left ventricle. Indian Heart Journal. 2012;6401:77–79. doi: 10.1016/S0019-4832(12)60015-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Simpson Leo, Michael DJ, Raymond FS. Perforated Submitral Left Ventricular Aneurysm Resulting in Severe Mitral Annular Regurgitation. Tex Heart Inst J. 2006;33:492–494. [PMC free article] [PubMed] [Google Scholar]
- 4.Peters Ferande, Khandheria Bijoy K, et al. Out of Africa: congenital submitral aneurysm with extrinsic compression of the left anterior descending and circumflex arteries. Circulation. 2013;128:1925–1926. doi: 10.1161/CIRCULATIONAHA.112.000275. [DOI] [PubMed] [Google Scholar]
- 5.Clive SL, Graham EV, Michael MWP. Thrombus within a submitral left ventricular aneurysm: diagnosis on cross sectional echocardiography. Br Heart J. 1991;66:179–181. doi: 10.1136/hrt.66.2.179. [DOI] [PMC free article] [PubMed] [Google Scholar]