

Abstract
Electronic cigarettes (“e-cigs”) have recently gained in popularity, but their health risks, including dependence potential are unclear. This study analyzed the adult database from the Wave 1 Population Assessment of Tobacco and Health (PATH) Study, a nationally representative survey of tobacco use in the United States, to assess the relative level of dependence among adult, exclusive everyday users of e-cigarettes and cigarettes.
Of the total 32,320 observations from the Wave 1 PATH adult database, 3586 (5.9%, weighted) were eligible for our analysis population. Among those who met the eligibility criteria, 156 (4.6%) were exclusive e-cig users, and 3430 (95.4%) were exclusive cigarette smokers. Our results show that e-cig users reported a significantly longer time-to-first-use of the day after waking (measured in minutes) compared to cigarette smokers after adjusting for confounders (adjusted Geometric Mean [95% Confidence Limits (CL)]: 29.2 [24.4–34.9] vs. 20.0 [18.7, 21.5]). In addition, cigarette smokers were significantly more likely to consider themselves addicted (Adj. Odds Ratio [95% CL]: 6.9 [4.5–10.7]); have strong cravings (2.9 [1.9–4.2]); find it difficult in the past 12 months to refrain from using their product in places where it was prohibited (6.4 [2.9–14.3]); and feel like they really needed to use their product (3.9 [2.4–6.4]).
These results are consistent with previous studies, in finding that exclusive daily e-cigarette users are less dependent on their respective product than comparable cigarette smokers.
Keywords: e-cigarettes, electronic cigarettes, cigarettes, inhaled nicotine device, addiction, dependence, nicotine, adults, tobacco, smoking
INTRODUCTION
Tobacco smoking is the leading preventable cause of premature morbidity and mortality in the U.S. (1) and cessation offers immediate and sustained improvement in health and quality of life (2). Over the past 10 years, a new inhaled nicotine device, popularly referred to as an electronic cigarette (“e-cig”) has become increasingly popular around the world (3–5), particularly in the United States where more than 79% of adults are currently aware of e-cigarettes and 3.7% are using one on a regular basis (6). Current everyday or some-day e-cigarette use is most prevalent among current cigarette smokers (15.9%) and recent former smokers (22.0%) and is very uncommon among adults who have never smoked cigarettes (0.4%) (6–8). E-cigarettes are battery-powered devices that heat and vaporize a liquid mixture (e-liquid), typically containing a vehicle such as propylene glycol and/or vegetable glycerin, and often but not always nicotine and/or flavorings, to produce an aerosol that is inhaled by the user (9, 10).
As of 2016, there were more than 250 brands of e-cigs on the United States market alone, with sales of approximately $3.5 billion (11). Per the recent Surgeon General’s report (12), as of 2015 e-cig use on one or more of the past 30 days among middle school students, high school students, young adults (18–24 years of age) and adults (aged 25 or older) are 5.3%, 16.0%, 13.6% and 5.7%, respectively; and the prevalence of e-cig use among young adults more than doubled from 2013 to 2014 (12). In May 2016, the FDA ruled that e-cigs, among other products, are subject to regulation. The new regulation prohibits marketing and sale of e-cigarettes to minors (under age 18), and restricts marketing and selling of e-cigs in many ways (13).
Despite the steady decline in cigarette smoking among adults and adolescents (14), the emergence of new tobacco products such as e-cigs has brought new uncertainties about the likely public health impact (9, 15–17). Studies have yielded mixed results regarding the effects of e-cigs on smoking cessation (18–21). In addition, electronic cigarettes are generally perceived as a less harmful alternative for smokers because rather than burning tobacco (22), liquids containing nicotine and flavorings are heated and vaporized. On the other hand, numerous studies have raised concerns that e-cigs may have more appeal to non-tobacco users who might otherwise not be attracted to the use of tobacco products (9, 15–17). Like any new product entering the mainstream and gaining popularity, there is still a lack of knowledge about e-cigs. The recent Surgeon General’s report states that there is a lack of knowledge about the harmfulness of e-cigs and that “strategic, comprehensive research is critical to identify and characterize the potential health risks from e-cigarette use” (12).
One important aspect of health consequences of a tobacco or nicotine delivery product is their tendency to result in dependence. Dependence, also referred to as addiction, is characterized by a perceived loss of control, including compulsive use and a difficulty abstaining. The present study aims to assess nicotine dependence among e-cig users in comparison with dependence among a comparable group of traditional tobacco cigarette smokers. Previous studies have utilized convenience samples recruited via internet surveys to compare dependence on e-cigs with that of cigarettes (23–25) and nicotine gum (23). Etter & Eissenberg concluded that e-cigs were less addictive than tobacco cigarettes and may be less addictive than nicotine gum. Farsalinos et al (24) reported that among 111 former-smoking current e-cig users, participants currently had a longer time-to-first-use of the day and rated themselves as less dependent on e-cigs relative to their prior cigarette use.
Foulds et. al. (25) studied self-reported dependence in a large sample (n=3,609) of current exclusive e-cig users who had successfully quit cigarette smoking. Having assessed their e-cig dependence using the 10-item Penn State (PS) Electronic Cigarette Dependence Index, these scores were retrospectively compared with those on the Penn State Cigarette Dependence Index. The current e-cig users reported less dependence on e-cigs than on their cigarettes prior to switching. However, despite the large sample size, there are potential limitations in that study. For example, recall bias could be of particular concern in reference to retrospective dependence measures on a product they claim to no longer use. In addition, the study sample was a volunteer convenience sample recruited online, and could have attracted individuals with a more positive view of e-cigs relative to cigarettes.
One previous study examined dependence symptoms in participants drawn from a large representative sample in the United States(26). They examined the 2012–13 National Adult Tobacco Survey and found that exclusive daily e-cigarette users reported significantly fewer symptoms of dependence than exclusive daily cigarette smokers.
The aim of our study is to compare dependence among e-cig users and cigarette smokers. The Population Assessment of Tobacco and Health (PATH) database provides the opportunity to assess dependence in exclusive e-cig users and cigarette smokers using a nationally representative sample. We chose to study exclusive product users in order to prevent any contamination of other product use with regard to survey responses pertaining to nicotine dependence.
METHODS
Data Source
The PATH Study is a national longitudinal study of tobacco use among youth and adults designed for use in evaluating the health effects on people in the United States (27). The first wave of data consists of baseline information for the study population. Continued follow-up data will become available as the consortium collects subsequent waves of data in future years. PATH Study data collection involves a rigorous, multi-layered sampling and weighting scheme to ensure that data are representative nationwide (28).
Ascertainment of Study Population
Our study focused on the adult population of the PATH database contained in the Wave 1 Adult Interview [September 12, 2013 to December 14, 2014] (28). The PATH Study classifies study participants into various types of tobacco users according to algorithms of responses to relevant survey questions. These are referred to as derived variables that already exist in the study’s Public-Use Files. Given that these classifications have already been ‘pre-defined’ by the PATH survey construction, these derived variables were heavily involved in defining our analysis population of interest. Not only were these algorithms used to categorize all participants interviewed in the PATH Study, but they were also used to determine and delegate which participants were routed to each survey question. This allowed for comprehensive data collection while minimizing the burden of participation on the subjects.
As previously mentioned, we focused on the dependence of e-cig and cigarette users, whose use of each product is exclusive, daily, established and current. To isolate these exclusive users, we excluded any past 30-day users of e-cigarettes and cigarettes who were classified as past 30-day, current established, or current experimental users of any other tobacco product.
Of particular interest to our analysis were participants’ responses to items within the Nicotine Dependence questionnaire (29). Because use within the past 12 months was not originally involved in the criteria defining our analysis population, further exclusions were necessary for the cigarette cohort in order to capture the responses that pertained only to their cigarette use. By design, if a participant reported using other products within the last 12 months, the survey was built to capture responses solely pertaining to the use of e-cigarettes; therefore this further refinement was not needed for the e-cig cohort.
To further delineate the dependence responses for the cigarette cohort and ensure that they were responding to this section with respect to their addiction to cigarettes only, we needed to further remove those classified as a Former Established Past 12 Months User of any other tobacco product. A more comprehensive summary of our analysis population and eligibility criteria is depicted in Figure 1, providing the hierarchical unweighted frequencies of each layer of criteria used to isolate these cohorts of interest. In total, 3586 unweighted (5.9% weighted) observations were eligible for our analysis population. Of these, 156 (4.6% weighted) were exclusive e-cigarette users, and 3430 (95.4% weighted) were exclusive cigarette smokers.
Figure 1. Flowchart: derivation of the study population.
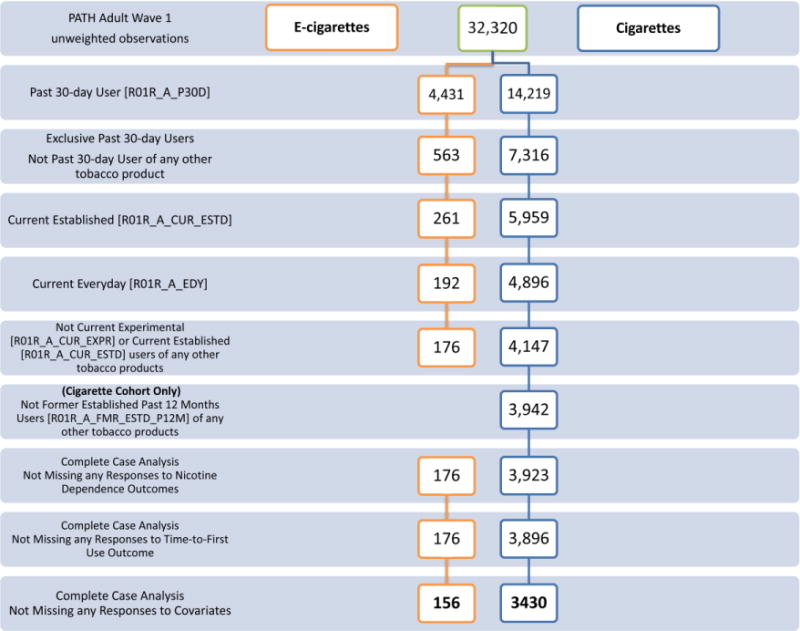
* Please note that the PATH adult survey intentionally oversampled tobacco users, young adults and black persons. While performing weighted analyses accounts for this, the unweighted observation frequencies presented in this figure are solely used for illustration purposes and are not meant to be interpreted as representative proportions.
Interestingly, of the 156 (unweighted) e-cigarette users, 151 (96.3% weighted) reported that the e-cig they used most of the time was rechargeable, 124 (76.5% weighted) reported that they were able to refill their e-cigarette or e-cigarette cartridges with e-liquid, and 150 (95.8% weighted) reported using e-cigarettes that usually contained nicotine. Of the 151 that used rechargeable e-cigarettes most of the time, 52 (37.9% weighted) reported that their e-cigarettes used cartridges.
Outcomes and covariates
The PATH nicotine dependence survey includes a number of questions relating to dependence, withdrawal and quit attempts. Most of these items used a numerical, ordinal response scale from 1 to 5, with anchors for the endpoints but no labels for intermediary levels, making interpretation difficult. We therefore selected four universally interpretable items with direct relevance to dependence with clear yes/no response options. Also of interest as a proxy for assessing dependence is the self-reported time-to-first-use (measured in minutes), as it has a very strong track record as a predictor of quitting difficulty. The four survey response questions are listed below:
“Do you consider yourself addicted to cigarettes/e-cigarettes?”
“Do you ever have strong cravings to smoke cigarettes/use e-cigarettes?”
“In the past 12 months, did you find it difficult to keep from smoking cigarettes/using e-cigarettes in places where it was prohibited?”
“Have you ever felt like you really needed to smoke cigarettes/use e-cigarettes?”
In order to account for potential confounders in our analysis, we considered the following covariates: Race/Ethnicity [Non-Hispanic White; Hispanic Blacks/Other Races]; Education [Less Than High School; High School Graduate/GED; Post-Secondary Education]; Age [18–24; 25–34; 35–44; 45–54; 55–64; 65–74; 75+]; Sex [Male; Female]; Poverty Status [Below Poverty Level; At or Above Poverty Level] (29).
For time-to-first-use of the day, we consider the addition of another covariate that accounts for rules about smoking a combustible tobacco product/using non-combustible tobacco products inside the home, which had the following possible options:
Not allowed anywhere or at any time inside the home
Allowed in some places or at some times inside the home
Allowed anywhere and at any time inside the home
Data analysis
SAS Version 9.4 (SAS Institute, Cary, NC, USA) SURVEY Procedures were used in all analyses to account for the complex sampling design and weighting of the observations in the PATH Study. The replicate weights provided within the PATH database were used to obtain accurate variance estimations using Fay’s Method of Balanced Repeated Replication (BRR), with the Fay coefficient specified at the value of 0.30, as recommended by the PATH Study (29). Rao-Scott Chi-Square tests were performed to evaluate the association of the binary group (e-cigarette vs. cigarette) variable with all binary and categorical variables. Binary logistic regression models, as implemented by PROC SURVEYLOGISTIC, were used to assess both the unadjusted and adjusted group effect on each of the binary nicotine dependence outcomes, while PROC SURVEYREG was used to fit unadjusted and adjusted linear regression models of the continuous time-to-first-use of the day variable. A natural log transformation of this response was needed in order to meet the normality assumption.
We compared the distributions of time-to-first-use (in minutes) in two ways. We categorized this continuous variable according to the Fagerstrom Test for Nicotine Dependence cut points (30), and also analyzed it continuously. A significance level of 0.05 was used for all analyses.
RESULTS
The unweighted frequencies and weighted percentages for demographic characteristics are presented in Table 1. The two cohorts are similar in age and gender distributions, and the e-cig group is comprised of more non-Hispanic whites than the cigarette group (84.8% vs. 74.0%). Most of the e-cigarette users have received some sort of post-secondary education (57.1%), while most of the cigarette smokers have not (59.3%). In addition, more than one-third of cigarette smokers (35.0%) are below poverty level in comparison to less than one-sixth (14.6%) of e-cig users. Notably, the majority of e-cigarette users live in a place that allows the use of their product anywhere and at any time inside their home (61.9%), compared to only 26.5% of the cigarette smokers. Almost halfof the cigarette smokers are not allowed to smoke anywhere or at any time inside the home (47.8%). This will likely have a confounding effect on their time-to-first-use of the day, as those who are allowed to use the product in the home have greater opportunity to use their product sooner after awakening.
Table 1.
Demographics by Group
| E-cigarette Users N=156 |
Cigarette Smokers N=3430 |
|
|---|---|---|
|
| ||
| Age | ||
| 18–24 | 11 (3.6) | 341 (5.8) |
| 25–34 | 39 (27.5) | 688 (19.9) |
| 35–44 | 29 (16.8) | 681 (19.7) |
| 45–54 | 39 (24.4) | 794 (24.5) |
| 55–64 | 27 (18.9) | 609 (19.5) |
| 65–74 | 8 (6.1) | 249 (8.2) |
| 75+ | 3 (2.6) | 68 (2.4) |
|
| ||
| Gender | ||
| Male | 70 (46.7) | 1475 (46.8) |
| Female | 86 (53.3) | 1955 (53.2) |
|
| ||
| Race/Ethnicity* | ||
| Non-Hispanic White | 129 (84.8) | 2446 (74.0) |
| Hispanic Blacks/Other Races | 27 (15.2) | 984 (26.0) |
|
| ||
| Education* | ||
| Less Than High school | 12 (8.2) | 605 (16.5) |
| High school Graduate/GED | 47 (34.6) | 1346 (42.9) |
| Beyond High School (Post-Secondary) | 97 (57.1) | 1479 (40.7) |
|
| ||
| 2-Level Poverty Status* | ||
| Below poverty level | 24 (14.6) | 1304 (35.0) |
| At or above poverty level | 132 (85.4) | 2126 (65.0) |
|
| ||
| Home Smoking Rules Inside the Home* | ||
| Not allowed anywhere/at any time | 34 (21.0) | 1617 (47.8) |
| Allowed in some places/at some times | 26 (17.1) | 893 (25.7) |
| Allowed anywhere/at any time | 96 (61.9) | 920 (26.5) |
Unweighted frequency (Weighted Column Percent)
P < 0.01 (Rao-Scott Chi-Square Test).
For all qualitative measures of nicotine dependence, e-cig users consistently reported lower dependence on their product than cigarette smokers (Table 2). In particular, compared with cigarette smokers, fewer e-cig users considered themselves addicted (77.2% vs. 94.0%); had strong cravings (72.8% vs. 86.9%); found it difficult to keep from using (5.6% vs. 28.6%); and felt like they really need to use (71.5% vs. 88.5%). When assessing dependence with an established quantitative measurement using time-to-first-use of the day, 15.1% of e-cig users reported first use within 5 minutes of waking compared to 24.0% of cigarette smokers.
Table 2.
Nicotine Dependence Outcomes by Group
| E-cigarette Users N=156 |
Cigarette Smokers N=3430 |
|
|---|---|---|
|
| ||
| Do you consider yourself addicted to cigarettes/e-cigarettes?* | ||
| No | 38 (22.8) | 204 (6.0) |
| Yes | 118 (77.2) | 3226 (94.0) |
|
| ||
| Do you ever have strong cravings to smoke cigarettes/use e-cigarettes?* | ||
| No | 46 (27.2) | 437 (13.1) |
| Yes | 110 (72.8) | 2993 (86.9) |
|
| ||
| In the past 12 months, did you find it difficult to keep from smoking cigarettes/using e-cigarettes in places where it was prohibited?* | ||
| No | 148 (94.4) | 2449 (71.4) |
| Yes | 8 (5.6) | 981 (28.6) |
|
| ||
| Have you ever felt like you really needed to smoke cigarettes/use e-cigarettes?* | ||
| No | 43 (28.5) | 379 (11.6) |
| Yes | 113 (71.5) | 3051 (88.5) |
|
| ||
| Time-to-First-Use | ||
| Within 5 Minutes | 21 (15.1) | 825 (24.0) |
| 6–30 Minutes | 77 (49.4) | 1541 (44.7) |
| 31–60 Minutes | 39 (24.6) | 643 (19.2) |
| > 60 Minutes | 19 (10.9) | 421 (12.1) |
Unweighted frequency (Weighted Column Percent)
P < 0.0001 (Rao-Scott Chi-Square test).
Unadjusted regression analyses showed consistent results with those reported above. Cigarette smokers reported significantly higher dependence on their product than e-cig users (Table 3). After adjusting for age, gender, race/ethnicity, education and poverty level, the group effect remained statistically significant. Specifically, cigarette smokers were significantly more likely to consider themselves addicted (Adj. OR [95% CL]: 6.92 [4.46–10.73]); to have strong cravings (2.85 [1.92–4.23]); in the past 12 months, to find it difficult to keep from using their product in places where it was prohibited (6.39 [2.85–14.32]); and to feel like they really needed to use their product (3.89 [2.36–6.40]). Moreover, the group effect on time-to-first use became larger after adjusting for the aforementioned covariates in addition to rules of smoking inside the home. Cigarette smokers had significantly shorter time-to-first-use compared to e-cig users (Adj. GM [95% CL]: 20.03 [18.66–21.49] vs. 29.16 [24.39–34.87]).
Table 3.
Regression Analysis Results for Nicotine Dependence Questions
| Unadjusted | Adjusted | |
|---|---|---|
| Outcome3 | OR (95% CL) | OR (95% CL)1 |
| Do you consider yourself addicted to cigarettes/e-cigarettes? | 4.63 (3.05, 7.02) | 6.92 (4.46, 10.73) |
| Do you ever have strong cravings to smoke cigarettes/use e-cigarettes? | 2.48 (1.66, 3.70) | 2.85 (1.92, 4.23) |
| In the past 12 months, did you find it difficult to keep from smoking cigarettes/using e-cigarettes in places where it was prohibited? | 6.80 (3.08, 15.04) | 6.39 (2.85, 14.32) |
| Have you ever felt like you really needed to smoke cigarettes/use e-cigarettes? | 3.06 (1.92, 4.86) | 3.89 (2.36, 6.40) |
| GM (95% CL) | GM (95% CL)2 | |
|
Time-to-first Use (minutes) E-Cigarette Users Cigarette Smokers |
23.46 (19.47, 28.27) 19.25 (18.25, 20.30) |
29.16 (24.39, 34.87) 20.03 (18.66, 21.49) |
Adjusting for Race/Ethnicity, Education, Age, Sex, and Poverty Status
Adjusting for Race/Ethnicity, Education, Age, Sex, Poverty Status and Smoking Rules in the Home
Modeling the probability of a ‘Yes’ response to the Nicotine Dependence questions
OR: Odds ratios reflect the relationship of cigarette smokers to e-cigarette users
GM: geometric mean, rough approximate of median
In the multivariable regression models, most of the covariates were significantly associated with the nicotine dependence outcomes. Specifically, race, age, and gender were significant covariates in modeling three nicotine dependence questions: “Do you consider yourself addicted to e-cigarettes/cigarettes?”, “Do you ever have strong cravings to use e-cigarettes/smoke cigarettes?”, and “Have you ever felt like you really needed to use e-cigarettes/smoke cigarettes?” Consistently, non-Hispanic whites and females were more likely to respond “Yes” to these survey questions. Additionally, compared to those in the oldest group (75 years or older), subjects in younger groups felt more nicotine dependent, with age group 35–44 being the strongest. Poverty status was significant when modeling “Do you consider yourself addicted to e-cigarettes/cigarettes?” with those at or above poverty level more likely to report “Yes.” Interestingly, poverty status was the only significant covariate when modeling “In the past 12 months, did you find it difficult to keep from using e-cigarettes/smoking cigarettes in places where it was prohibited?” with those below poverty level more likely to report “Yes.”
In the regression analysis of time-to-first-use, all covariates (race/ethnicity, education, age, poverty status, and additionally, home smoking rules) except for gender were significant in the model. Non-Hispanic Whites, those with less than a high school education, and those below poverty level used their products sooner after waking compared to Hispanic Blacks/Other races, those with post-secondary education, and those at or above poverty level, respectively. All younger age groups used their product sooner compared to those 75 years old or older with age groups 35–44 and 45–54 taking the shortest time-to-first-use. Additionally, less stringent home smoking rules are associated with shorter time-to-first-use of the product.
Discussion
The results from this study consistently showed that established, everyday exclusive e-cigarette users have lower nicotine dependence than established, everyday exclusive cigarette users, as supported by all five outcome variables that we used as markers of dependence. Considered as an extension to the work of Foulds et al (25), our study has shown that while there are differences between the reported dependence on each product, it is worth noting that the e-cig users’ reported dependence on their product is not negligible. Over three quarters of the e-cig users considered themselves addicted to e-cigs. The pattern of results is consistent with the known nicotine delivery of different types of e-cigarettes (lower), relative to tobacco cigarettes (31).
It should also be noted that in PATH Wave 1, while almost a quarter (23.8%) of adults who have ever tried a cigarette are currently daily cigarette smokers, under 7% (6.8%) of ever e-cig users are daily e-cig users (including both exclusive and dual-product e-cigarette users). This same difference in transfer to daily use occurs in young adults (ages 18–24), and is itself suggestive of differential dependence potential (27). This also means that in selecting comparable groups of exclusive daily users in order to compare ‘like-with-like’, we are in fact selecting the most extremely dependent subgroup of daily e-cig users to compare with cigarette smokers exhibiting a fairly common pattern of daily cigarette use. Of the 156 exclusive daily e-cigarette users eligible for our analytical cohort, 145 (92.9%) of them were former established cigarette smokers, 10 (6.7%) were former experimental cigarette users and 1 (0.4%) was a never cigarette user, who was also a never user of any other tobacco product.
Study limitations
Ideally, for this analysis, we would have liked to have compared the frequency of use per day between these two groups; however the units of measure for e-cigs and cigarettes were non-comparable within the PATH survey. In particular, for e-cig users, there are a wide variety of e-cig product characteristics such as refillable cartridges, disposables, e-liquid with varying concentrations of nicotine, flavors, etc. Each e-cig product type requires a different metric in evaluating this frequency of use, making a quantitative comparison between e-cigs and cigarettes impossible.
As shown in Figure 1, the vast majority of past 30-day e-cig users are dual or poly-product users, rather than exclusive users. While it may therefore be of interest to examine dependence among dual users, it becomes difficult to interpret and attribute dependence to a specific product in those using multiple nicotine delivery products.
In hopes of utilizing the length of time e-cig users and cigarette smokers have been using their products, we considered the PATH-derived ‘Age range when first started using every day’ variable. However, given that both age variables (at time of screening and when first started) are categorical, the duration of use for each respective product could not be reliably calculated or assessed. We were unable to adequately account for this use history in our analyses.
Conclusions
Our results are consistent with those of previous studies based on convenience samples (23–25), and the one previous study based on a representative national sample (26) in finding that established, everyday exclusive e-cig users report lower dependence than comparable cigarette users. Future studies should examine exposure biomarkers (e.g. cotinine) and assess the development of dependence on e-cigarettes over time and how this differs by device and liquid characteristics. The longitudinal design of the PATH Study will also facilitate study of the development of dependence on e-cigarettes over time.
Highlights.
E-cig users report less dependence on their product than cigarette smokers
Cig smokers are more likely to consider themselves addicted
To have strong cravings, and to feel like they really needed to use their product
Cig smokers found it more difficult not to use in places where prohibited
E-cig users report a longer time-to-first-use after waking
Acknowledgments
Funding
This work was supported in part by the National Institute on Drug Abuse of the NIH and the Center for Tobacco Products of the FDA (P50-DA-036107) (Liu, Wasserman, Foulds) and by the National Center for Advancing Translational Sciences, NIH, through Grant UL1 TR000127 (Kong). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH or the FDA.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Warren GW, Alberg AJ, Kraft AS, Cummings KM. The 2014 Surgeon General’s report: “The health consequences of smoking–50 years of progress”: a paradigm shift in cancer care. Cancer. 2014;120(13):1914–6. doi: 10.1002/cncr.28695. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Wu J, Sin DD. Improved patient outcome with smoking cessation: when is it too late? Int J Chron Obstruct Pulmon Dis. 2011;6:259–67. doi: 10.2147/COPD.S10771. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Gravely S, Fong GT, Cummings KM, Yan M, Quah AC, Borland R, et al. Awareness, trial, and current use of electronic cigarettes in 10 countries: Findings from the ITC project. International journal of environmental research and public health. 2014;11(11):11691–704. doi: 10.3390/ijerph111111691. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ayers JW, Ribisl KM, Brownstein JS. Tracking the Rise in Popularity of Electronic Nicotine Delivery Systems (Electronic Cigarettes) Using Search Query Surveillance. American Journal of Preventive Medicine. 2011;40(4):448–53. doi: 10.1016/j.amepre.2010.12.007. [DOI] [PubMed] [Google Scholar]
- 5.Adkison SE, O’Connor RJ, Bansal-Travers M, Hyland A, Borland R, Yong HH, et al. Electronic nicotine delivery systems: international tobacco control four-country survey. Am J Prev Med. 2013;44(3):207–15. doi: 10.1016/j.amepre.2012.10.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Schoenborn CA, Gindi RM. Electronic Cigarette Use Among Adults: United States, 2014. NCHS Data Brief. 2015;(217):1–8. [PubMed] [Google Scholar]
- 7.Mazurek GSAJBAKJM. Electronic Cigarette Use Among Working Adults — United States, 2014. MMWR Morb Mortal Wkly Rep 2016. 2016;65:557–61. doi: 10.15585/mmwr.mm6522a1. [DOI] [PubMed] [Google Scholar]
- 8.King BA, Patel R, Nguyen KH, Dube SR. Trends in awareness and use of electronic cigarettes among US adults, 2010–2013. Nicotine & tobacco research : official journal of the Society for Research on Nicotine and Tobacco. 2015;17(2):219–27. doi: 10.1093/ntr/ntu191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Primack BA, Soneji S, Stoolmiller M, Fine MJ, Sargent JD. Progression to Traditional Cigarette Smoking After Electronic Cigarette Use Among US Adolescents and Young Adults. JAMA pediatrics. 2015;169(11):1018–23. doi: 10.1001/jamapediatrics.2015.1742. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Walton KM, Abrams DB, Bailey WC, Clark D, Connolly GN, Djordjevic MV, et al. NIH electronic cigarette workshop: developing a research agenda. Nicotine & tobacco research : official journal of the Society for Research on Nicotine and Tobacco. 2015;17(2):259–69. doi: 10.1093/ntr/ntu214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Wells Fargo Securities. Nielsen WF. Tobacco “All Channel” Data Cig Pricing Remains Strong; E-Cig $ Sales Growth Re-Accelerates. Equity Research. 2015 [Google Scholar]
- 12.US Department of Health and Human Services. E-cigarette use among youth and young adults: a report of the surgeon general—executive summary. 2016 [Google Scholar]
- 13.Food, Drug Administration HHS. Deeming Tobacco Products To Be Subject to the Federal Food, Drug, and Cosmetic Act, as Amended by the Family Smoking Prevention and Tobacco Control Act; Restrictions on the Sale and Distribution of Tobacco Products and Required Warning Statements for Tobacco Products. Final rule. Fed Regist. 2016;81(90):28973–9106. [PubMed] [Google Scholar]
- 14.Syamlal G, Mazurek JM, Hendricks SA, Jamal A. Cigarette Smoking Trends Among U.S. Working Adult by Industry and Occupation: Findings From the 2004–2012 National Health Interview Survey. Nicotine & tobacco research : official journal of the Society for Research on Nicotine and Tobacco. 2015;17(5):599–606. doi: 10.1093/ntr/ntu185. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Barrington-Trimis JL, Urman R, Berhane K, Unger JB, Cruz TB, Pentz MA, et al. E-Cigarettes and Future Cigarette Use. Pediatrics. 2016;138(1) doi: 10.1542/peds.2016-0379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Leventhal AM, Strong DR, Kirkpatrick MG, Unger JB, Sussman S, Riggs NR, et al. Association of Electronic Cigarette Use With Initiation of Combustible Tobacco Product Smoking in Early Adolescence. Jama. 2015;314(7):700–7. doi: 10.1001/jama.2015.8950. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Unger JB, Soto DW, Leventhal A. E-cigarette use and subsequent cigarette and marijuana use among Hispanic young adults. Drug and alcohol dependence. 2016;163:261–4. doi: 10.1016/j.drugalcdep.2016.04.027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Biener L, Hargraves JL. A longitudinal study of electronic cigarette use among a population-based sample of adult smokers: association with smoking cessation and motivation to quit. Nicotine & tobacco research : official journal of the Society for Research on Nicotine and Tobacco. 2015;17(2):127–33. doi: 10.1093/ntr/ntu200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Brose LS, Hitchman SC, Brown J, West R, McNeill A. Is the use of electronic cigarettes while smoking associated with smoking cessation attempts, cessation and reduced cigarette consumption? A survey with a 1-year follow-up. Addiction (Abingdon, England) 2015;110(7):1160–8. doi: 10.1111/add.12917. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Delnevo CD, Giovenco DP, Steinberg MB, Villanti AC, Pearson JL, Niaura RS, et al. Patterns of Electronic Cigarette Use Among Adults in the United States. Nicotine & tobacco research : official journal of the Society for Research on Nicotine and Tobacco. 2016;18(5):715–9. doi: 10.1093/ntr/ntv237. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Pearson JL, Stanton CA, Cha S, Niaura RS, Luta G, Graham AL. E-Cigarettes and Smoking Cessation: Insights and Cautions From a Secondary Analysis of Data From a Study of Online Treatment-Seeking Smokers. Nicotine & tobacco research : official journal of the Society for Research on Nicotine and Tobacco. 2015;17(10):1219–27. doi: 10.1093/ntr/ntu269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Baeza-Loya S, Viswanath H, Carter A, Molfese DL, Velasquez KM, Baldwin PR, et al. Perceptions about e-cigarette safety may lead to e-smoking during pregnancy. Bulletin of the Menninger Clinic. 2014;78(3):243–52. doi: 10.1521/bumc.2014.78.3.243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Etter JF, Eissenberg T. Dependence levels in users of electronic cigarettes, nicotine gums and tobacco cigarettes. Drug and alcohol dependence. 2015;147:68–75. doi: 10.1016/j.drugalcdep.2014.12.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Farsalinos KE, Romagna G, Tsiapras D, Kyrzopoulos S, Voudris V. Evaluating nicotine levels selection and patterns of electronic cigarette use in a group of “vapers” who had achieved complete substitution of smoking. Subst Abuse. 2013;7:139–46. doi: 10.4137/SART.S12756. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Foulds J, Veldheer S, Yingst J, Hrabovsky S, Wilson SJ, Nichols TT, et al. Development of a questionnaire for assessing dependence on electronic cigarettes among a large sample of ex-smoking E-cigarette users. Nicotine & tobacco research : official journal of the Society for Research on Nicotine and Tobacco. 2015;17(2):186–92. doi: 10.1093/ntr/ntu204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Rostron BL, Schroeder MJ, Ambrose BK. Dependence symptoms and cessation intentions among US adult daily cigarette, cigar, and e-cigarette users, 2012–2013. BMC Public Health. 2016;16(1):814. doi: 10.1186/s12889-016-3510-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Kasza KA, Ambrose BK, Conway KP, Borek N, Taylor K, Goniewicz ML, et al. Tobacco-Product Use by Adults and Youths in the United States in 2013 and 2014. N Engl J Med. 2017;376(4):342–53. doi: 10.1056/NEJMsa1607538. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Hyland A, Ambrose BK, Conway KP, Borek N, Lambert E, Carusi C, et al. Design and methods of the Population Assessment of Tobacco and Health (PATH) Study. Tobacco control. 2016 doi: 10.1136/tobaccocontrol-2016-052934. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Inter-university Consortium for Political and Social Research. Population Assessment of Tobacco and Health (PATH) Study [United States] Public-Use Files Codebook for Wave 1: Adult Data. 2016 [Google Scholar]
- 30.Heatherton TF, Kozlowski LT, Frecker RC, Fagerstrom KO. The Fagerstrom Test for Nicotine Dependence: a revision of the Fagerstrom Tolerance Questionnaire. Br J Addict. 1991;86(9):1119–27. doi: 10.1111/j.1360-0443.1991.tb01879.x. [DOI] [PubMed] [Google Scholar]
- 31.Hajek P, Przulj D, Phillips A, Anderson R, McRobbie H. Nicotine delivery to users from cigarettes and from different types of e-cigarettes. Psychopharmacology (Berl) 2017;234(5):773–9. doi: 10.1007/s00213-016-4512-6. [DOI] [PMC free article] [PubMed] [Google Scholar]