

Abstract
Introduction:
The main objective of this case report is to demonstrate endoscopic calcaneoplasty (ECP) using two lateral portals.
Case Report:
The patient is middle-aged male aged 40 years, with higher basal metabolic index (BMI) and was diagnosed having a Haglund’s bump and was on conservative treatment for a period of over 6 months, with minimal relief. We did ECP with the patient in lateral decubitus position using two lateral portals instead of using one medial and one lateral portal, his American Orthopaedic Foot and Ankle Society score has improved from 64 to 98, and his Fowler-Philip angle is reduced from 71° to 45°.
Conclusion:
ECP using two lateral portals with patient in lateral position is comfortable for the patients with higher BMI and the surgical time can also be reduced. However, we need to perform more number of cases through this technique to conclude to the results. Endoscopic calcaneoplasty, two lateral portals, Haglund’s bump.
Learning Points for this Article.
Safe procedure for patients who are high risk for anaesthesia and with morbid obesity, where prone position is not possible.
Introduction
The common causes for the retrocalcaneal pain are the insertional tendinitis of Achilles tendon, Haglund’s syndrome, and retrocalcaneal bursitis [1, 2]. In 1928, the Swedish orthopedic surgeon, Patrick Haglund described Haglund’s syndrome as a painful osseous prominence of the posterosuperior corner of the calcaneus with large posterior palpable callus, and retrocalcaneal bursitis which was caused by rigid heel counters [3]. This is also known as “pump-bump”. The disorder is caused mechanically from abnormally high pressure between the posterosuperior corner of the calcaneus and the Achilles tendon, and the impingement of the retrocalcaneal bursa between the both leading to the inflammation of the bursa and not by the intrinsic disease of the tendon. Haglund disease is usually observed bilaterally, in the women in their second or third decade [4]. The diagnosis is made with typical history of pain for the initial few steps of walking after a period of rest, proper clinical examination and interpretation with radiographs [5] and ultrasonography (USG) if required. Other pathologies causing pain in the posterior heel should be clearly distinguished.
Tenderness caused by isolated sub-tendinous bursitis can best be isolated by palpation just anterior to both the medial and lateral edge of the distal Achilles tendon. Tenderness due to insertional Achilles tendinitis is located slightly more distal, where the Achilles tendon inserts onto the posterior calcaneus [5].
Surgical intervention is the treatment of choice for patients in whom conservative treatment has failed for over 6 months. Open and endoscopic are the two surgical methods. Classic endoscopic calcaneoplasty (ECP) uses one medial and a lateral portal with patient in prone position.
In this case report, we are going to discuss about the ECP using two lateral portals with patient in semi-prone or lateral decubitus position.
Case Report
The patient is a 40-year-old male patient with moderate obesity complaining of pain and swelling in the left retrocalcaneal region. X-ray and USG of ankle were taken and diagnosed having Haglund’s bump with retrocalcaneal bursitis, calcification in tendon is ruled out by USG. He was given 6 months of conservative treatment, but there was no improvement. His American Orthopaedic Foot and Ankle Society (AOFAS) score was 64 and Fowler- Philip angle is 71 (Fig. 1). Surgical intervention was planned.
Figure 1.

Pre-operative X-ray with calculated Fowler-Phillip angle for the left ankle showing 71°.
Surgical technique: The patient in spinal anesthesia is placed in lateral decubitus position. Tourniquet is placed in the thigh and the other limb is flexed at hip and knee so that it will not interfere with the procedure. The limb is scrubbed and draped, tourniquet inflated. Bony landmarks and the portals are marked.
With the ankle in the neutral position, a line was drawn from the tip of the lateral malleolus to the Achilles tendon, parallel to the foot sole. The posterolateral portal was situated just above the line, in front of the Achilles tendon (Fig. 2). A small vertical skin incision is given, blunt trocar was used to reach the retrocalcaneal space and is replaced with 30° 4 mm arthroscope (directing towards 1st web space).
Figure 2.
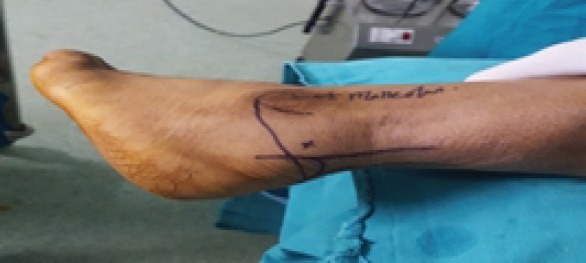
Limb positioning and marking ofposterolateral portal.
Then, an accessory lateral portal is created by giving a stab incision below the posterolateral portal using a needle as a guide so as to reach the posterolateral corner ofthe calcaneum. A stab incision is given, spread with mosquito forceps while entering the retrocalcaneal space. The bursa is shaved with a shaver tip facing away from the Achilles tendon. The medial and lateral corners of the Haglund’s bump are viewed after the bursa is shaved off. An osteotome is passed through the accessory lateral portal (Fig. 3) and the Haglund’s bump is removed and is confirmed on fluoroscopy and by plantar flexing the ankle to see whether the sufficient amount has been removed or not. The sharp edges are smoothened using an acromioniser (Fig. 4 and 5). The skin is closed using non-absorbable sutures, and pressure dressing is applied, tourniquet is released (Fig. 6).
Figure 3.

Intraoperative positioning of arthroscope through proximal posterolateral portal and osteotome through distal posterolateral portal.
Figure 4.

Fan-shaped insertion of Achilles tendon.
Figure 6.

Post-operative picture showing portals and sutures.
The patient started full ankle range of movements and weight-bearing as tolerated from the 1st post-operative day (P.O.D). He was discharged on the 2nd P.O.D after primary dressing and suture removal was done on the 12th P.O.D. Patient started full weight-bearing from the 13th P.O.D. His post-operative X-ray showed reduction in Fowler-Phillip angle from 71 to 45 (Fig. 7). We did not encounter any complications during intraoperative and post-operative follow-up period. He was followed on the 1st, 3rd, and 6 months postoperation and his AOFAS score improved from 64 to 98 at 6-month follow up. Patient is pleased as there was no swelling in the retrocalcaneal region with minimal scar tissue formation (Fig. 8) and early rehabilitation.
Figure 7.

Post-operative X-ray showing reduction in the Fowler-Phillip angle.
Figure 8.

3-month follow-up showing minimal scarring of the portals and decrease in the retrocalcaneal swelling.
Figure 5.

Excising the bump through distal posterolateral portal using an osteotome.
Discussion
Haglund’s syndrome is a common cause for retrocalcaneal heel pain. Biomechanical studies show an increasing pressure on the retrocalcaneal bursa during dorsiflexion of the foot and a decrease of the pressure in plantar flexion [6]. Symptoms often worsen when the person first initiates an activity after a period of rest. Tenderness due to insertional Achilles tendinitis is located slightly more distal, where the Achilles tendon inserts onto the posterior calcaneus. While in Haglund’s disease, tenderness is usually 3-4 cm proximal to the insertion of the Achilles tendon [5].
In the open procedure, the surgical goal is to achieve complete exposure of the retrocalcaneal space and to perform the resection of the bump without weakening the insertion of the Achilles tendon [7, 8]. The same goal can be achieved endoscopically. Following open surgery, various complications have been reported such as skin complications [7], hyperesthesia in the area of the scar [9], irritation of the scar [10], Achilles tendon lesions [11], weakness of the calcaneus after removing the posterosuperior bony prominence [12], persistent pain [13], and irritation of the whole heel [13]. Advantages of endoscopic technique over open surgeries are short recovery time, rapid return to work and sports, small incision, and good scar healing [4, 14].
Because endoscopic treatment for Haglund’s syndrome is a new procedure and experience is limited, modification of endoscopic techniques has continued to evolve, aiming to avoid complications and improve outcome. Wu et al., [15] in 2012 used three portal techniques for ECP for 23 patients and achieved good results. They used two lateral portals, proximal posterolateral (primary viewing), and distal posterolateral and one distal posteromedial portal (working portals). In our case, we made only proximal and distal posterolateral portals. Interchanging of portals was not required as we used an osteotome for excising the Haglund’s bump through distal posterolateral portal, thereby creating enough space for the shaver to reach posteromedial corner of the heel to excise the inflamed bursa if present. We achieved an excellent result using this technique. The operating time was only 20 min. However, we need to perform more number of cases through this technique to conclude to the results.
Conclusion
Using two lateral portals with patient in lateral decubitus position is comfortable and less time consuming for obese patients for ECP and can be a viable option for classic procedure using medial and lateral portals.
Clinical Message.
Normally, ECP is done in prone position using medial and lateral portals. However, in our case, the patient was obese with higher basal metabolic index (BMI). Prone position in such patients is a higher anesthesia risk and can create complications. Hence, placing these patients in lateral decubitus position can avoid such complications. We used two lateral portals instead of taking one medial and one lateral portal, as it is technically difficult to create medial portal in lateral decubitus position. Thus, it becomes advantageous to operate these patients in lateral decubitus position using two lateral portals and can be a good option in patients with central obesity, high BMI, as well as high-risk patients.
Biography
References
- 1.Clancy WG. Runners' injuries. Part two. evaluation and treatment of specific injuries. Am J Sports Med. 1980;8:287–9. doi: 10.1177/036354658000800415. [DOI] [PubMed] [Google Scholar]
- 2.Fiamengo SA, Warren RF, Marshall JL, Vigorita VT, Hersh A. Posterior heel pain associated with a calcaneal step and Achilles tendon calcification. Clin Orthop Relat Res. 1982;162:203–11. [PubMed] [Google Scholar]
- 3.Haglund P. Beitragzur klinik der Achilles tendon. Zeitschr Orthop Chir. 1928;49:49–58. [Google Scholar]
- 4.Jerosch J, Schunck J, Sokkar SH. Endoscopic calcaneoplasty (ECP) as a surgical treatment of haglund's syndrome. Knee Surg Sports Traumatol Arthrosc. 2007;15:927–34. doi: 10.1007/s00167-006-0279-3. [DOI] [PubMed] [Google Scholar]
- 5.Van Dijk CN, van Dyk CE, Scholten PE, Kort NP. Endoscopic calcaneoplasty. Foot Ankle Clin. 2006;2:439–46. doi: 10.1016/j.fcl.2006.02.004. [DOI] [PubMed] [Google Scholar]
- 6.Jerosch J. Endoscopic calcaneoplasty. Foot Ankle Clin. 2015;20:149–65. doi: 10.1016/j.fcl.2014.10.004. [DOI] [PubMed] [Google Scholar]
- 7.Pauker M, Katz K, Yosipovitch Z. Calcaneal osteotomy for haglund's disease. J Foot Surg. 1992;31:558–89. [PubMed] [Google Scholar]
- 8.Keck SW, Kelly PJ. Bursitis of the posterior part of the heel :Evaluation of surgical treatment of 18 patients. J Bone Joint Surg Am. 1965;47A:267–73. [PubMed] [Google Scholar]
- 9.Angermann P. Chronic retrocalcaneal bursitis treated by resection of the calcaneus. Foot Ankle. 1990;10:285–7. doi: 10.1177/107110079001000508. [DOI] [PubMed] [Google Scholar]
- 10.Leach RE, Dilorio E, Harney RA. Pathological hindfoot conditions in the athlete. Clin Orthop. 1983;177:116–21. [PubMed] [Google Scholar]
- 11.Le TA, Joseph PM. Common exostectomies of the rearfoot. Clin Podiatr Med Surg. 1991;8:601–23. [PubMed] [Google Scholar]
- 12.Periman MD. Enlargement of the entire posterior aspect of the calcaneus:Treatment with the Keck and Kelly calcaneal osteotomy. J Foot Surg. 1992;31:424–33. [PubMed] [Google Scholar]
- 13.Nesse E, Finsen V. Poor results after resection for haglund's heel. Analysis of 35 heels treated by arthroscopic removal ofbony spurs. Acta Orthop Scand. 1994;65:107–9. doi: 10.3109/17453679408993732. [DOI] [PubMed] [Google Scholar]
- 14.Jerosch J, Nasef NM. Endoscopic calcaneoplasty –Rationale, surgical technique, and early results:A preliminary report. Knee Surg Sports Traumatol Arthrosc. 2003;11:190–5. doi: 10.1007/s00167-003-0365-8. [DOI] [PubMed] [Google Scholar]
- 15.Wu Z, Hua Y, Li Y, Chen S. Endoscopic treatment of haglund's syndrome with a three portal technique. Int Orthop. 2012;36:1623–7. doi: 10.1007/s00264-012-1518-5. [DOI] [PMC free article] [PubMed] [Google Scholar]