

Abstract
Introduction
Before the advent of assisted reproductive technologies, the incidence of heterotopic pregnancy was estimated to be in 1 out of 30,000 pregnancies in the United States. With interstitial pregnancy comprising only 2.4% of ectopic pregnancies, spontaneous heterotopic interstitial pregnancies are exceedingly rare.
Case
A 27-year-old pregnant woman (gravida 3 para 1011) with a history of one prior term vaginal delivery and a spontaneous abortion in the first trimester presented to the emergency department with abdominal pain and a positive home pregnancy test. Transvaginal ultrasound confirmed heterotopic pregnancy and she underwent operative management, at which point a ruptured interstitial pregnancy was identified.
Conclusion
Heterotopic and interstitial pregnancies are rare and to see them together in a spontaneous pregnancy is virtually unique. The case report describes our management of this rarely seen condition.
Keywords: Heterotopic interstitial pregnancy
Highlights
-
•
Spontaneous heterotopic interstitial pregnancies are exceedingly rare.
-
•
We submit a unique surgical approach of cornual resection.
-
•
Stability of the patient may guide the management of the remaining intrauterine pregnancy.
1. Introduction
Heterotopic pregnancy was previously estimated to occur in 1 out of 30,000 pregnancies in the United States [1], but has been seen with increasing incidence in recent years due to growing use of assisted reproductive technologies with a more recent estimate of 1:3900 pregnancies [3]. Most often, heterotopic pregnancies are a combination of intrauterine and ectopic pregnancies [1,4]. The overwhelming majority of ectopic pregnancies occur within the fallopian tube, with interstitial pregnancies occurring in approximately 2.4% of all ectopic pregnancies [2]. As such, incidence of natural heterotopic interstitial pregnancy is exceedingly rare and can present unique challenges in management when compared more commonly seen fallopian ectopic pregnancy.
2. Patient Information
A 27-year-old G3 P1011 presented to our emergency department with one day of worsening left lower quadrant abdominal pain and a positive home pregnancy test. Upon arrival the patient was tachycardic with heart rate equal to 123 bpm and blood pressure of 88/40 mmHg. A qualitative beta-HCG test was repeated and was positive. Gynecology was consulted to evaluate the patient for a presumed ectopic pregnancy. A transvaginal ultrasound was performed which revealed a viable intrauterine pregnancy with cardiac activity at 9 weeks 0 day gestation based on crown-rump length (Fig. 1). An additional left-sided ectopic pregnancy mass contiguous with uterus, measuring 13.2 cm, was identified with unclear location (fallopian tube, interstitial, adnexal, or intra-ovarian). Cardiac activity was identified in the ectopic pregnancy with an estimated gestational age 9 weeks 1 day based on crown-rump length (Fig. 2). Additionally, probable blood products were noted in the left adnexa. Ultrasound was consistent with heterotopic pregnancy.
Fig. 1.

Fetal pole of intrauterine pregnancy, Twin A.
Fig. 2.
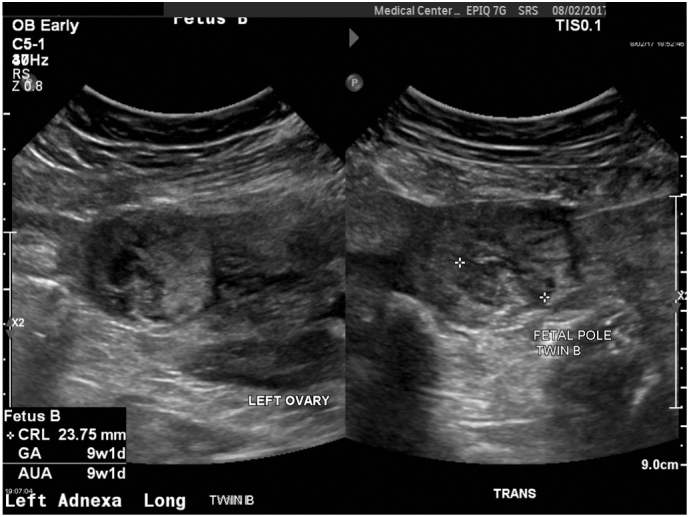
Left adnexa with Twin B Fetal Pole.
Diagnostic Assessment: This unstable patient was counseled on the emergent need for surgical intervention to remove the ectopic pregnancy, including the risk of potentially miscarrying the IUP or of even having to do more extensive surgery such as a hysterectomy. The patient was adamant that we try to do everything we could to save the intrauterine pregnancy. Given the acuity of this life threatening condition in an unstable patient, we had concerns that she would need time to process and grieve the loss of both pregnancies if a missed abortion did occur. We decided to stabilize her acute issues and give her time to process and grieve the loss of at least one embryo of this wanted twin pregnancy. The patient consented to surgical intervention to remove the ectopic pregnancy and was taken to the operating room.
Diagnostic laparoscopy was performed. Upon entry to the abdomen a large amount of blood was visualized, with a large 20 cm clot adherent to the uterus. A second and third trochar were placed to facilitate visualization of the ectopic mass. Blunt graspers were used to elevate the uterus and a left interstitial pregnancy was identified with continued active bleeding from the posterior aspect of the ectopic mass. The decision was then made to convert to laparotomy. The peritoneal cavity was accessed through Pfannenstiel incision. A 400 cm3 blood clot was evacuated and the interstitial pregnancy was identified, measuring approximately 4 cm in diameter. There was active bleeding from a 5 mm laceration on the posterior aspect of the cornua. A Heaney clamp was placed across the cornua and care was taken to place the clamp below the actual pregnancy (Fig. 3). The left tube was separated from the cornua using a hand held electrosurgical vessel sealing device. The device was then used to sequentially clamp, cauterize, and separate segments of the cornua from the uterus corpus until the pregnancy was entirely removed. With the Heaney clamp still in place, sequential figure of eight sutures were placed. With each suture, the Heaney clamp was slowly removed. Approximately eight sutures were placed, the clamp was removed and the area appeared completely hemostatic (Fig. 4). Attention was then turned to the amputated left fallopian tube. It appeared hemostatic with large varicosities extending along the length of the tube. It was decided to leave the tube in place due to high risk of bleeding from these large varicosities. Several pieces of absorbable hemostatic agent were placed along the area of the cornual resection and the area was observed for approximately 5 minutes to ensure complete hemostasis. The pelvis was freed of all blood and clot. The uterus was again inspected and noted to be hemostatic with normal anatomy on the right side and normal right and left ovary. The patient required transfusion of 3 units packed red blood cells during the case, but tolerated to procedure well and was transferred to the post anesthesia care unit in stable condition.
Fig. 3.

Interstitial pregnancy with Heaney clamp placed below pregnancy.
Fig. 4.

Uterus following resection of interstitial pregnancy.
We waited to perform the ultrasound to assess viability of the intrauterine pregnancy to accommodate stabilizing the patient so that she could be more involved in decision making. On admission, she was acutely ill and unstable, with her primary concern being trying to salvage the pregnancy. On post-operative day #1, a bedside ultrasound was performed to assess the remaining intra-uterine pregnancy and no cardiac activity was observed. We discussed this with the patient, and she decided not to pursue surgical evacuation of the uterus. We had concerns of a possibly increased risk of perforation through the area of the interstitial resection if we performed a dilation and curettage. If the patient had decided she wanted surgical intervention, we planned to perform ultrasound guidance of the procedure. Medical management with a prostaglandin was also discussed, but ultimately she decided to manage the spontaneous abortion expectantly. Rho(D) immune globulin was given due the patient's Rh negative status. The patient was discharged on postoperative day #2 with scheduled outpatient follow-up and weekly quantitative hCG.
Follow-up and Outcomes: One week after discharge the patient presented to our emergency department with incomplete abortion of the remaining intrauterine pregnancy. Products of conception were removed from the cervical os, and misoprostol was administered to facilitate passage of the remainder of the pregnancy. She was counseled to avoid pregnancy for six months to let her uterus heal, and that because the uterine incision went across the fundus, she would need a Cesarean section for any further deliveries.
3. Discussion
Unfortunately, when the patient arrived at our institution, we had concerns that she was incapable of understanding the emergent nature of her exact diagnosis due to her instability. She persisted in stating her desire to continue the pregnancy, even after being confronted with the probable high risk of need to return to surgery to complete evacuation of the uterus in the event of miscarriage of the intrauterine twin.
Ideally, assessment of the viability of the remaining pregnancy, and evacuation of the non-viable pregnancy would have occurred at time of laparotomy to decrease the risk of complications, and to prevent a possible return to the operating room. Guiding the dilation and curettage while the abdomen is open to avoid perforation of the uterine scar would have been ideal. This would be more possible in settings where patients are anticipated to have heterotopic pregnancies, such as populations undergoing in vitro fertilization.
Contributors
Joy Anderson M.D., Chase Patterson M.D., and April Riley D.O. were the equal and sole contributors.
Conflict of Interest
The authors declare that they have no conflict of interest.
Funding
No funding was sought or secured in relation to this case report.
Consent
Consent for publishing this patient's case was obtained both preoperatively, as well as after conclusion of her course of care.
Provenance and Peer Review
This case report was peer reviewed.
References
- 1.Reece E.A., Petrie R.H., Sirmans M.F., Finster M., Todd W.D. Combined intrauterine and extrauterine gestations: a review. Am. J. Obstet. Gynecol. 1983;146(3):323–330. doi: 10.1016/0002-9378(83)90755-x. [DOI] [PubMed] [Google Scholar]
- 2.Bouyer J., Coste J., Fernandez H., Pouly J.L., Job-spira N. Sites of ectopic pregnancy: a 10 year population-based study of 1800 cases. Hum. Reprod. 2002;17(12):3224–3230. doi: 10.1093/humrep/17.12.3224. [DOI] [PubMed] [Google Scholar]
- 3.Tal J., Haddad S., Gordon N., Timor-tritsch I. Heterotopic pregnancy after ovulation induction and assisted reproductive technologies: a literature review from 1971 to 1993. Fertil. Steril. 1996;66(1):1–12. doi: 10.1016/s0015-0282(16)58378-2. [DOI] [PubMed] [Google Scholar]
- 4.Pisarska M.D., Carson S.A. Incidence risk and factors for ectopic pregnancy. Clin. Obstet. Gynecol. 1999;42(1):2–8. doi: 10.1097/00003081-199903000-00004. [DOI] [PubMed] [Google Scholar]