

Abstract
Accessory scrotum and congenital perineal lipoma are unusual congenital anomalies. Congenital pulmonary airway malformation (CPAM) is a rare congenital disorder of the lung. There are five types of CPAM, each with a different clinical presentation and prognosis. The present report involves a case of type 2 CPAM associated with accessory scrotum and congenital perianal lipoma.
Keywords: Accessory scrotum, congenital lipoma, type 2 congenital pulmonary airway malformation
Introduction
Accessory scrotum is a rare condition. In fact, it is the least frequent congenital anomaly of the scrotum. To the best of our knowledge, only 43 cases have been reported in the English literature. Most of these cases were associated with adjacent lipoma. Isolate congenital perianal lipoma is, however, extremely rare.[1-3] None of the reported cases were associated with congenital pulmonary airway malformation (CPAM) type 2, a subtype of a rare congenital disorder of the lung.[4] Herein, we report a rare case of accessory scrotum and congenital perineal lipoma in association with CPAM.
Case Report
A 6-month-old baby boy, the product of a full-term pregnancy with a caesarean section was diagnosed with CPAM by antenatal ultrasound. The baby had an Apgar score of 8 and 7 at 1 and 5 min, respectively. He was admitted to the neonatal intensive care unit for observation and management. Physical examination showed a skin covered soft mass measuring 1.5 cm × 1.5 cm just above the anal orifice. The penis was of normal size and shape, with deficient skin ventrally, and both testicles were palpated in the scrotum. Hernia orifices were intact. Examination of other systems showed no abnormalities. Ultrasound of the abdomen and pelvis was within normal limits.
The patient was discharged after 3 days in fair condition. Computed tomography scan of the chest performed at 2 months, showed a large 7 cm × 5 cm × 3 cm lucent lesion in the left upper lobe that contained multiple cysts of variable sizes consistent with type 2 CPAM. At 6 months of age, the patient underwent elective surgery for left thoracotomy and upper lung lobectomy, perianal mass excision, and circumcision. The left upper lobe and the perianal mass were sent for histopathology.
Gross examination showed a lung lobe measuring 8 cm × 5 cm × 5 cm with multiple cysts ranging in size from 0.1 to 0.7 cm. The perianal mass consisted of skin covered polypoidal soft tissue measuring 2.5 cm × 2 cm × 2 cm with a small 1 cm protrusion covered by dark colored skin.
Histological examination of the formalin-fixed, paraffin-embedded, and hematoxylin and eosin-stained tissue sections of the lung showed numerous small cysts lined by benign bronchial epithelium. The intervening lung parenchyma showed mixed inflammatory infiltrate [Figure 1a and b]. The findings were consistent with CPAM type 2.
Figure 1.
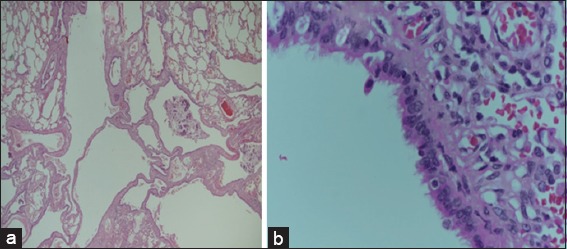
(a) The lung lobe shows multiple variable sized cysts (hematoxylin and eosin (H and E, ×20). (b) The cysts are lined by benign bronchial epithelium (H and E, ×20)
Sections from the perianal mass showed keratinized epidermis and dermis with underlying mature adipose tissue proliferation [Figure 2a], while sections from the protruding lesion showed keratinized epidermis with underlying bundles of smooth muscle in the dermis and subcutaneous tissue [Figure 2b]. These findings were consistent with congenital lipoma and accessory scrotum.
Figure 2.
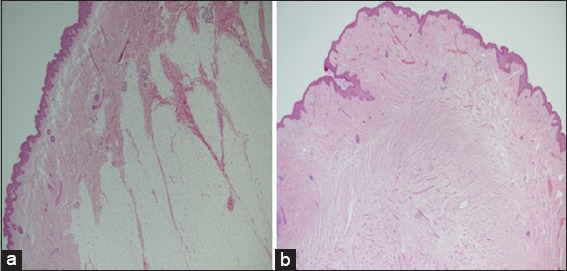
(a) The perianal mass shows keratinized epidermis, dermis, and with underlying mature adipose tissue proliferation (H and E, ×20). (b) The protruding lesion shows keratinized epidermis with underlying smooth muscle bundles (H and E, ×20)
The patient now is 14-month-old and doing well.
Accessory scrotum is the rarest of all congenital scrotal abnormalities. It is characterized by the presence of additional scrotal tissue without a testis, in addition to a normally developed scrotum. To the best of our knowledge, only 43 such cases have been reported, in the English literature.[1]
Lipoma is one of the most common benign neoplasms, for which, the average age of onset is the fourth decade of life. However, lipomas are very rare in neonates and perineal lipoma itself is very rare.[2] There is a high incidence of association between the presentation of accessory scrotum and adjacent subcutaneous tumors, and most cases are reported with lipomas followed by hematoma and lipoblastoma. Other urogenital and anorectal anomalies have also been reported in association with accessory scrotum.[1,3]
CPAM is characterized by the hamartomatous proliferation of terminal respiratory bronchioles forming a multicystic lung mass. The first description, by Ch’in and Tang in 1949,[4] utilized existent terminology for congenital cystic adenomatoid malformation.[4] Stocker suggested a new classification and renamed this group of malformations CPAM. There are five types of CPAM (0–4) with variable clinical presentations, prognoses, and microscopic findings.[5]
Although CPAM has been considered as a rare disease entity, at least one retrospective study has concluded that both the incidence of CPAM and its antenatal detection rate are rising.[4]
The type 2 CPAM that is associated with other congenital anomalies are seen more frequently than other types of CPAM and represents 10-15% of all CPAM cases. Macroscopically, a type -2 lesion contains multiple small cysts (0.5–2 cm). Microscopically, it shows small, relatively uniform cysts resembling bronchioles separated by normal alveoli. The cysts are lined by cuboid-to-columnar epithelium and have a thin fibromuscular wall.[5]
Association of the accessory scrotum and congenital perineal lipoma with a case of type 2 CPAM is unusual.
Conclusion
We herein report a rare case of accessory scrotum and congenital perineal lipoma in association with type 2 CPAM. It is very important to conduct a complete systemic physical examination that includes the urogenital and anorectal organs in patients with type 2 CPAM to exclude congenital anomalies.
References
- 1.Murase N, Uchida H, Hiramatsu K. Accessory scrotum with perineal lipoma diagnosed prenatally: Case report and review of the literature. Nagoya J Med Sci. 2015;77:501–6. [PMC free article] [PubMed] [Google Scholar]
- 2.Kim SH, Cho YH, Kim HY. Does this baby have a tail? A case of congenital isolated perineal lipoma presenting as human pseudo-tail. Ann Surg Treat Res. 2016;90:53–5. doi: 10.4174/astr.2016.90.1.53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Chatterjee S, Gajbhiye V, Nath S, Ghosh D, Chattopadhyay S, Das SK. Perineal accessory scrotum with congenital lipoma: A rare case report. Case Rep Pediatr. 2012;2012:757120. doi: 10.1155/2012/757120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Lau CT, Kan A, Shek N, Tam P, Wong KK. Is congenital pulmonary airway malformation really a rare disease? Result of a prospective registry with universal antenatal screening program. Pediatr Surg Int. 2017;33:105–8. doi: 10.1007/s00383-016-3991-1. [DOI] [PubMed] [Google Scholar]
- 5.Taştekın E, Usta U, Kaynar A, Ozdemır C, Yalçin O, Ozyilmaz F, et al. Congenital pulmonary airway malformation Type 2: A case report with review of the literature. Turk Patoloji Derg. 2016;32:200–4. doi: 10.5146/tjpath.2013.01208. [DOI] [PubMed] [Google Scholar]