

Abstract
Objectives:
The objectives were to determine whether employment-related factors had influence on physical and mental health outcomes among uninsured expatriates working in Saudi Arabia and to identify whether these factors act as facilitators or barriers to health.
Methods:
Cross-sectional face-to-face interviewsusing previously published methodswere conducted among a multistage stratified cluster sample of 1370 employees as their problemsin seeking health benefits have notbeen studied. Male expatriates working in different companies representing several trades in Riyadh were selected, for which tested questionnaires were administered to them.
Results:
Among 1370 uninsured expatriates, across various tested independent variables, age and income level were having most prominent influences on self-rated perceptions of physical and mental health. Uninsured expatriates with 60 plus age group have 71% more chances ofdeteriorating physical and mental health as compared to their younger age group uninsured expatriates. The expatriates earning less than SR 2000 had 68% more chances ofhaving poor physical and mental health as compared to their counterparts earning more than SR 6000, indicating more adverse outcomes among people in low-income categories. 74% of the expatriates having maximum education were found to have better physical and emotional outcomes than the less educated ones.
Conclusion:
The present study provides useful insights into the complex health-care system in Saudi Arabia and contributes to the exploration of health behaviors and the shaping of health perceptions among expatriates.
Keywords: Employment factors, uninsured expatriates, Saudi Arabia
Introduction
At present, the globalized world is characterized by demographic imbalances, with disparities leading to economic and political crises - both natural and human-made. One of the major outcomes of this phenomenon is the migration of human resources, which is pervasive and has become essential to compensate for demographic trends and skill shortages in some contexts and to provide assistance to sending communities through remittances. In the Gulf region, 48.1% of the total population of 50,759,763 are non-nationals or expatriates. Among the Gulf Cooperation Council countries, the Kingdom of Saudi Arabia has the highest percentage of expatriates, with the 2014 census stating that, of a total population of 30,770,775, 32.7% were expatriates.[1-3]
The health of expatriates populations is influenced by multifaceted connections between mental health and physical conditions. Recently, we have demonstrated that both personal and workplace characteristics are important factors influencing health insurance status.[4] The previous studies have also shown that economic and social drivers such as income, education, and social connectedness have a direct bearing on health.[5-8] Various studies conducted in other countries have suggested that certain health-related barriers influence the low socioeconomic status of expatriates, particularly their education, employment status, and general health-linked associations. The World Report on Migration highlights the fact that, worldwide, expatriate workers lack equal access to health care.[9-15] In addition, expatriates who are uninsured have worse health outcomes, delay seeking care, and receive less medical care.[2,16,17]
Saudi Arabia, as a developed nation with extensive employment opportunities, attracts a large number of expatriates from Asia. Saudi Arabia has attempted to restructure its private health-care system and reduce expatriate access to government resources through the provision of compulsory employment-based health insurance (CEBHI).[18-20] However, despite substantial developments such as the restructuring of the health-care system, access to this system, and the introduction of CEBHI, health care is still in its nascent stage in Saudi Arabia. Thus, knowledge about factors that are influential for determining health outcomes in this context is vital to provide inputs for the successful expansion of health care.
One of the key strengths of the present study was its focus on expatriates from Asian countries working in Saudi Arabia. The problems faced by this group in seeking health benefits had not previously been studied in depth, leaving this group of people with unequal health access because of their own growing problems unexamined. Previous work has also highlighted that expatriates represent an understudied population with regard to their health status.[19,20] Moreover, there is a distinct lack of evidence from population-based studies on the rates of access or unmet need for health services among uninsured expatriates working in Saudi Arabia.[19-22]
To date, there is no data-based information available on employment factors and their impact on the uninsured expatriates working in the kingdom. In the present study, we have tried to analyze some of the key employment factors associated with these uninsured expatriates and identify how such factors may act as facilitators or barriers to overall health status. This work is an extension of our recently published communication showing the influence of personal and workplace characteristics along with the development and extent of the insurance industry on health insurance status of insured expatriates.[4]
Notably, employment-related factors constitute one of the most important pillars of any successful health-care model. The majority of the expatriates come from developing nations have limited education and face additional problems because of multiple factors.[23-26] Gaining a better understanding of the factors associated with the healthcare of the ever-increasing number of expatriatess in the kingdom is an important area of research and will allow for the development of future strategies for a healthy expatriates society and for a strong, disease-free nation. The present study, which is the first of its type in this context, was carried out to gain an understanding of the links between employment-related characteristics and physical and mental health, health behavior, and disease status among uninsured expatriates working in Riyadh, Saudi Arabia.
Methods
Cross-sectional face-to-face interviews were conducted using employee population across varioustrade sectors used in the study. The sample stratification was based on business type, company size, and number of employees. Riyadh was selected because one-third of the expatriates in Saudi Arabia live in this region.[20,26] The sample was selected from the large pool of companies (population) registered in Riyadh, the capital of the Kingdom of Saudi Arabia.
The sample size was calculated using multistage cluster sampling method, where sampling fraction of 0.001911 was estimated and was used to predict the total number of sample employees per economic sector/companies. Companies were randomly selected from the Ministry of Labour database according to their size and economic sector. The SPSS software was used to conduct the randomization, with the companies’ identities hidden. All companies providing health-care-oriented services, such as hospitals, clinics (medical, clinical, or any other professional health-care clinics), optical shops, insurance companies, and pharmacies were excluded from the study. Female expatriates were also excluded from the sample because men dominate the expatriate workforce in the private sector. The sum total of all economic sectors ranging from agriculture to personnel services gave an appropriate sample size of 4575 expatriate employees, representing the expatriate population included under the study. The estimated sample population was then divided into insured and uninsured category. The current study included only uninsured expatriates where 1389 male expatriate employees were contacted, and 1370 responded to the study.
Using the sampling formula, estimated value of 664 was calculated to be a true measure of the population. To minimize chances of error with predicted 50% response rate, a sample size of 1370 uninsured expatriates was selected for our study which was double the estimated sample size value. The translated survey instrument had sufficiently acceptable content validity, test-retest, and inter-rater reliability. In case ofilliterate respondents, interviews were managed by specially trained research assistants who explained them the questions without any bias. All of the respondents were working in Saudi Arabia, and all were uninsured. Since the number of female expatriates was very low, representing only 1.7% of the expatriate population,[23] it would, therefore, have been very difficult to obtain a sufficient number of female participants, and hence, were not included in the study.
The present study was conducted from December 2014 to July 2016, and the data were collected from all of the companies immediately after the implementation of CEBHI. To test the outcomes, pre-tested questionnaires were administered to the expatriates working in different companies in trades including agriculture, mining, industry, construction, transportation, and financial services. The classification of economic sector/industry was based on the third revision of the International Standard Industrial Classification of all economic activities, which has been used to standardize the collection and reporting of statistics.[26]
Standard published methodologies were adopted in the current study. The employment factors included in the questionnaire were based on Andersen’s Behavior Model (1995) and included sections on parameters representing employment factors, namely, age, years of service, job category/designation, qualifications, and income.[4] These factors were classified as independent variables in this study. The employment-related factors gauged by work profile/nature of job, work experience, related qualifications, and income level are some of the most important parameters used to define key employment characteristics.[4] The outcome measures (dependent variables) for evaluating the physical and mental health of the examined working expatriates population were self-rated physical and mental health status, the presence of any chronic disease, smoking behavior, and proneness to depression.[26,27]
Self -rated health refers to survey questionnaire in which participants assess different dimensions of their own health and measured by question in which participants rate their health as excellent, very good, good, not good or poor with higher scores indicating poorer self- rated health. For the purpose of analysis, the scale was divided into 2 discrete categories of excellent to good and not good to poor. Descriptive statistics using frequencies and percentages were calculated from the data using SPSS software, version 22.0 was used, and the dependent variable was tabulated using the physical and mental health questionnaire modified from Agency for Healthcare Research and Quality, Medical Expenditure Panel Survey (AHRQ-MEPS) health questionnaire. Chi-square test was used to compare the categorical variables and t-tests for continuous variables with P < 0.05 was considered statistically significant.
Later, logistic regression was employed to assess the correlates for physical and mental health of the uninsured expatriates. The model included following factors and covariates: Age, income level, education level, duration of stay in KSA, job position, marital status, self-rated physical and emotional health, smoking behavior, tendency for depression, and presence ofany chronic disease. Odds ratio and the associated 95% confidence intervals for variables in the final model have beenreported, and all tests were two-sided with an alpha level of 0.05.
Results
General demographic and employability characteristics of the participants
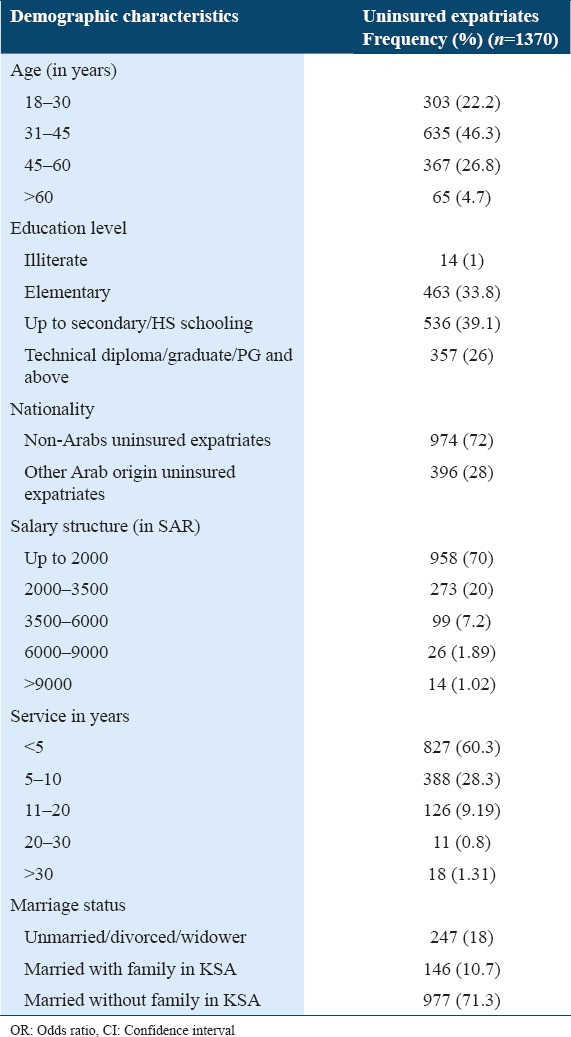
Of 1389 potential participants, 1370 responded to the questionnaire. Table 1 provides a demographic overview of the respondents. The average age of the sample was 36 years. The majority (51.79%) of the uninsured expatriate workers were aged 30–45 years and 22.2% were younger than 30 years. Most of the participants interviewed reported that they were from the Asian subcontinent (Bangladesh, India, and Pakistan). Egypt was the most commonly reported country of origin of uninsured expatriates from Arab countries (15.7%), followed by Yemen (4.6%) and other countries (8.7%) [Table 1]. Married respondents comprised 71.3% of the sample. Of the married respondents, most (89.3%) lived alone, without their families. In terms of educational qualifications, 80% were educated to the high school level, whereas 19% had professional diplomas/degrees or above. Turning to income, 70% had a monthly income of < 2000 SAR, 27.2% earned 2001–6000 SAR, and only 2.91% earned 6000 SAR or higher. Among the industrial sectors selected for drawing the sample of the expatriates population, the five most frequently reported areas were trade (30.48%), education (21%), social services (16.69%), water (16.25%), and power construction (15.52%).
Table 1.
Demographic employability characteristics of the uninsured expatriates working in Riyadh, KSA
Outcome measures: Self-rated physical and emotional health status, behavioral factors in terms of various employment factors of the uninsured expatriates
In the univariate analysis, the participant’s age and income were significant correlates of physical and mental health (P < 0.05). The other factors including education level, number of years of service, and marital status were found not be associated. In the present study, overall 76.5% among uninsured expatriates surveyed classified their health status as good to excellent, whereas 23.5% classified it as having not good to poor. Segregating the same in terms of age groups and the perception of good to excellent physical health was found to be more prominent among the younger age groups, with the percentage holding this perception declining as age increased. Vice versa, the percentage assessing their physical health as poor to fair increased as age increased. Significant difference was found between self-perceived of physical and mental health status among younger and older age group population.
In cross-tabulations of the uninsured expatriates’ perceptions of their health status with income level, the lowest perceptions of health were found maximum among those earning < 2000 SR as compared to those earning more than 2000 SR and above. Thus, as income increased, perceived health status outcomes also increased (Figure 1, P = 0.00*).
Figure 1.

Percentage of self-rated physical and mental health among uninsured expatriates (n = 1370): Stratified by age, years of service, job category, educational qualification, and income levels (P < 0.05) significance
However, the job category, number of years of service affects perceptions of one’s physical and emotional health status insignificantly. For example, while examining emotional health status by job category, for uninsured expatriates working in the specialist/technical category, trade and sales-related jobs, and those doing clerical work, an average of 4.7% reported not good to poor emotional health. This was higher than the same percentage for other categories, but the difference was insignificant.
In terms of behavioral characteristics likely to influence physical and mental health, after excluding cases with missing data, the presence of chronic disease, smoking behavior, and proneness to depression was investigated among the 1370 surveyed male expatriates. Highest numbers of expatriates suffering from chronic disease belonged to the two oldest age groups (over 60 years, 63%; and 45–60 years, 34.44%). For smoking behavior, the highest number of expatriates who smoked were aged over 60 years. In the younger age groups (<30 years), an average of 18% of the expatriates smoked.
In the evaluation of the relationship between income and the health behavior outcome measures (chronic disease, smoking and proneness to depression), income was not found to be correlated with the prevalence of chronic disease, as this relationship was statistically insignificant. Across all age groups, the prevalence of chronic disease was approximately 6.2%, and most respondents (94%) had no disease [Figure 2]. On analysis of the smoking behavior of the respondents in relation to income categories, in the present study, it was observed that about 30.77% of the respondents having income of 6000 to 9000 (SAR)smoked cigarettes, followed by 21.94 % of the expatriates who smoked and had earnings of 600 to 2000 (SAR). Turning to proneness to depression, unexpectedly, expatriates with an income level of 6000–9000 SAR were found to be more prone to depression (15.38%) compared with those in other income groups, though insignificant.
Figure 2.

Percentage of various behavioral outcome measure (smoking, chronic disease, and depression) among uninsured expatriates of various age groups
There was no significant relationship found between health-related behavior outcomes and higher or lower levels of job-related qualifications. In contrast, the reported prevalence of chronic disease increased with an increase in years of service. Similarly, examining smoking behavior by years of service, almost 30% of respondents with 20–30 years of service were smokers. Along the same lines, comparing proneness to depression by years of service revealed that the highest percentage of respondents who were prone to depression (14%) was observed among expatriates who had worked in Saudi Arabia for < 5 years.
We used regression analyses to examine the impact of various employment factors: Age, income, education, job category, and marital status on participants’ measures of physical and mental health. In preliminary testing, we found that the two measures - age and income – both contributed significantly to physical and mental status outcomes of the respondents, whereas other important employment variables including job/work position and education level did not vary significantly with measures of physical and mental health.
Uninsured expatriates with 60 plus age group had 71% (0.29, CI 95% 0.18–0.86) more chances of detiorating physical and mental health as compared to their younger age group uninsured expatriates. Thus, the odds of physical health decreased with each increased level of age and with an increased level of mental stress. The income levels of the uninsured expatriates were too found to have a significant influence on the physical and mental health status. The expatriates earning less than SR 2000 had 68% more chances of having poor physical and mental health as compared to their counterparts earning more than SR 6000 [Table 2].
Table 2.
Multivariate logistic regression for the correlates of physical and mental health (assessed using AHRQ-MEPS modified questionnaire) among 1370 expatriate workers

Discussion
The purpose of the present study was to understand the links between employment-related characteristics and physical and mental health, health-related behavior, and disease status among uninsured expatriates workers. One of the key differences between our study and earlier work is that we measured the influence of depression along with other covariates, namely, chronic disease and smoking, as well as overall perceptions of physical and mental health, among uninsured expatriate male workers. The study showed that a clear majority (72%) of these workers were of Asian origin. Understanding the key issues relevant to their health can have a significant impact on productivity and related factors, which can directly or indirectly influence the Saudi Arabian economy.[23,28]
Several similarities were observed between the sample used for the present study and the overall expatriate population in Saudi Arabia. The sample had a median age of 36 years and an average duration of stay in the kingdom of 12 years. Most of the expatriates surveyed (51.79%) were aged 30–45 years and 21.1% were aged < 30 years. Likewise, according to the Ministry of Labour in Saudi Arabia, the median age of expatriate workers in the country is 34 years.[26] Existing work has also revealed that insurance status varies by age. It has been found that young adults represented the largest percentage of Americans who were not covered by a health insurance plan.[29-32] A 2004 Joint Economic Committee study showed that young adults aged 18–24 were about 30% less likely to be insured, compared with the rest of the population, and the chances of being insured increased with age.[30] Similarly, in Carper and Beauregard’s MEP survey,[32] conducted in the United States in 2009, age was found to play a major role in whether a worker had health insurance. Young adults aged 19–23 years were at more risk of being uninsured than those in any other age group. In addition, this survey found that workers under the age of 45 years were significantly more likely to be uninsured all year than were older workers. These findings are well corroborated by the present study, where 68.5% of uninsured expatriates were under 45 years old.
The present study also found that perceptions of good-to-excellent physical and emotional health were more prominent among respondents in the younger age groups, with the percentage of respondents rating their health status at this level declining as age increased and was found to be a significant factor for physical and mental health. Our study revealed a strong relationship between age as an important determining factor for physical and mental health regardless of the job category, education, or years of service. The basis for these perceptions find support in the form of higher prevalence of chronic disease been reported by the expatriates as their age increased [Table 2]. The difference in chronic disease by age was statistically significant and is likely related to the fact that smoking was found to be more common among older individuals than among the younger respondents.
These findings are similar to those of Ahmad[33] on the prevalence and attitude toward cigarette smoking among Indian expatriates living in Jeddah, Saudi Arabia. In the study, it was found that the majority of smokers were of 41–50 years and had an increased risk of chronic disease. In terms of emotional health, a series of studies among the general population in Saudi Arabia reported that women and individuals older than 45 years are more prone to depression.[34,35] Similarly, positive physical and mental health were higher among those who reported to have better job categories; however, the variables lost their significance in the multivariate model. One key example to highlight this phenomena is the fact that professions such as teaching would require the person to be a graduate/postgraduate. However, irrespective of better job category, similar outcome measures were not evident and were inconsistent.
Our finding that people in older age groups reported worse emotional health than their younger counterparts may be related to the fact that although the vast majority of the study respondents were married, most lived alone without their families. These circumstances may have contributed to increasing depression as the expatriate worker’s age progressed. The desire and need for care and companionship might be felt more strongly as age advances and health begins to fail. These underlying behavioral factors might lead to more stress, with increased feelings of isolation likely resulting in increased smoking behavior as an emotional outlet. Our study also revealed that uninsured expatriates in older age groups were two-third times more prone to have poor physical and mental health outcomes as compared to their younger counterparts. Further investigation, which is currently underway, is needed to assess the associations between tobacco smoking and the subsequent risk of depressive symptoms and other behavioral characteristics which may influence outcomes more clearly.
The present study also found that the vast majority (74%) of the expatriates workers surveyed had high school-level education or less. This finding could be considered statistically significant, as it reveals that the majority of these workers were either unskilled with no education or worked as manual workers with a secondary level education. Our findings on education matched the information gained from the Ministry of Labour database,[26] and the International Monetary Fund has also reported that 85% of the expatriates in Saudi Arabia were employed in low-skilled jobs.[3]
The perception of good or excellent physical health was found to be associated with education level, with physical health improving as the level of education increases. Level of education is considered an important determinant of employment, and it is assumed that more educated people are more aware of their health. A low level of education can lead to low health literacy. In addition to significantly influencing the assessment of one’s own physical health, education may also equip people to cope better with stress and depression. This idea is supported by our findings indicating that respondents with more education had better physical and emotional outcomes compared with those with less education. Carper and Beauregard[32] also reported that educational attainment has a substantial impact on workers’ health insurance status. Lower levels of education were found to be associated with being uninsured all years among workers aged 19–64. Workers with less than a high school education were twice as likely as those with at least some college attendance to be uninsured all through the year.
Employment can have an ambivalent influence on health, as it is both an enabler and an impediment to health behavior. Income is important in determining one’s health status because it makes it possible to pay the high cost of health services. Better positions and higher remunerations improve health prospects among expatriates workers,[36] as well as being directly and indirectly correlated with health-seeking behavior.[37] For example, being employed with better salary packages has been found to increase financial capacity and integration into social support networks, both of which facilitate health-seeking behavior.
It is clearly evident from our findings that increases in salary levels could positively influence the self-rated assessment of both physical and emotional health. Our study revealed that income level of employees earning less than SR 2000 affects the health score significantly by about 68%, in comparison to employees earning better salaries. These findings are in agreement with a study conducted on Filipino Americans where it was found that lower pay scales can cause job-related stress, which are significantly associated with lower levels of some health-related behavior outcomes and can lead to depression and the development of chronic diseasesas well.[38] Correspondingly, our data showthat, as respondents’ monthly income increased, the status of their health improved which was found to be statistically significant.
Although expatriates earning 600–2000 SAR reported slightly less smoking behavior than those earning 6000–9000 SAR, a comparison of smoking across income groups indicates that the expatriate workers earning less (i.e., <2000 SAR) may consider smoking to be a means of relieving stress. This finding is consistent with previous work in other countries that have found a link between high smoking prevalence and low socioeconomic status.[37-39] In the past work that has directly examined various psychosocial dimensions, including proneness to depression, loneliness, homesickness, empathy, compassion, and care, smoking can be seen as a major emotional outlet, although it is also a precursor to chronic diseases.[34] Our finding that almost 30% of respondents with 20–30 years of service were smokers likely provides a partial explanation for the positive association found between years of service and chronic disease.
A number of previous studies have shown that difficulties with expatriates’ adjustment to their new environment and problems with mental health are more pronounced when there is a significant cultural difference between the home country and the host country. These problems are further aggravated when financial conditions are difficult.[36-41] Grant-Vallone and Ensher[42] have stated that expatriate workers experience worse mental health than native workers. Recently, Nadim et al. have reported that depression is considerably high among the migrant workers in KSA, high-stress level, and poor self-rated health being its significant correlates.[43]
Given these previous findings, the present study provides important and useful insights into the complex health-care system in Saudi Arabia that can be used to explore the key employment parameters influencing expatriate workers’ health behaviors and perceptions. These perceptions, along with health awareness, will be the vital drivers of a successful symbiotic relationship between the insured and the insurer. For many expatriates who have settled in a new country in search of a better life, health-seeking behavior is perceived as a lower priority in the face of multiple and simultaneous settlement needs.[25,42]
The present study was innovative in its assessment of the impact of the nature of employment on certain health outcomes and some health-related behaviors. Among all of the employment categories, expatriates in managerial positions had better health outcomes than did those in other job categories [Figure 1]. It is felt that expatriatess, working at clerical levels/positions probably, may not have perception of high values of self-worth/self-esteem and are under constant pressure from their bosses to manage tasks in a particular order. This might be an explanation for why workers in this job category rated their emotional health as fair to bad more commonly than those in other job categories. In contrast, those working at the managerial level or higher faced less stress and among those surveyed, 100% assessed their emotional health positively, although the nature of their jobs could still be stressful.
Several studies conducted in the Western world have also supported the finding of differences in health by type of job.[37,42] A study conducted in Spain compared job satisfaction among expatriate workers, repatriate workers, and domestic workers reportedthat the lower employment segment fared poorly in comparison with workers at the managerial level and that this impacted the health status of the lower-segment workers in a negative way.[44] Our findings confirm that, among the total sample of uninsured male expatriates, the predictors of employment are important determinants of health and are significant for the overall well-being of workers.
Limitations of the study
This study has several limitations. The study included only expatriate men; women and children were excluded from the study. Representing only 1.7% of the expatriate population,[39] the number of female expatriates working in the selected companies was very limited. Therefore, it would have been very difficult to obtain a sufficient number of female study participants to allow for a meaningful analysis of this group. In addition, this was a cross-sectional study, which may have increased bias with respect to the time ordering of events. Furthermore, the inclusion of self-reported data and any information bias has been included.
Conclusion
Our findings indicate that there are several important employment-related factors that can influence expatriate workers’ perceptions of their physical and mental health status, consequently impacting their health insurance levels. Specifically, these factors include age and income levels, which can affect the physical and mental status of the uninsured expatriate workers. Without health insurance, these expatriate workers may experience significant health and financial burdens related to these specific employment factors and can serious impact their overall health status. Therefore, we recommend further studies to investigate these employment factors, also examining accessibility and utilization of health services by uninsured expatriate workers. This kind of work would help in framing a health-care model that might be adopted worldwide.
Acknowledgments & Ethical Approval
This work was supported by the King Abdullah International Medical Research Centre under grant number RC09/084 upon the recommendation of the Research Committee following the review of the ethical aspects of the proposal by the Institutional Research Board.
Conflict of Interest
The authors do not have any conflicts of interest.
References
- 1.Baicker K, Taubman SL, Allen HL, Bernstein M, Gruber JH, Newhouse JP, et al. The oregon experiment-effects of medicaid on clinical outcomes. N Engl J Med. 2013;368:1713–22. doi: 10.1056/NEJMsa1212321. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Kronfoll NM. Access and barriers to health care delivery in arabcountries: A review. Eastern Mediterr Health J. 2012;18:1239–46. doi: 10.26719/2012.18.12.1239. [DOI] [PubMed] [Google Scholar]
- 3.International Monetary Fund (IMF) Report on GCC. Labour Markets. 2013 [Google Scholar]
- 4.Alkhamis A, Cosgrove P, Mohamed G, Hassan A. The personal and workplace characteristics of uninsured expatriate males in Saudi Arabia. BMC Health Serv Res. 2017;41:1–12. doi: 10.1186/s12913-017-1985-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Sommers BD, Baicker K, Epstein AM. Mortality and access to care among adults after state medicaid expansions. New Engl J Med. 2012;367:1025–34. doi: 10.1056/NEJMsa1202099. [DOI] [PubMed] [Google Scholar]
- 6.Sekhri N, Savedoff W. Private health insurance: Implications for developing countries. Bull WHO. 2005;83:8. [PMC free article] [PubMed] [Google Scholar]
- 7.Bassett MC, Kane VM. Review of the literature on voluntary private health insurance. In: Preker AS, Bassett MC, editors. Private Voluntary Health Insurance in Development Friend or Foe? Washington, DC: World Bank; 2007. p. 335. [Google Scholar]
- 8.Thomson S, Foubister T, Mossialos E. European Observatory on Health Systems and Policies. Copenhagen: WHO; 2009. Financing health care in the European union: Challenges and policy responses; p. 200. [Google Scholar]
- 9.Ministry of Labour. The Annual Statistical Book for One Year 2009. The Annual Report. Riyadh: Ministry of Labour; 2009. [Google Scholar]
- 10.Schoen C, Osborn R, Squires D, Doty MM. How health insurance design affects access to care and costs, by income, in eleven countries. Health Aff. 2010;29:2323–34. doi: 10.1377/hlthaff.2010.0862. [DOI] [PubMed] [Google Scholar]
- 11.Dorherty J. Expansion of the Private for Profit Health Sector in East and Southern Africa, in EQUINET, with UCT HEU and TARSC Policy No. 26. 2011 [Google Scholar]
- 12.Berkhout E, Oostingh H. Health Insurance in Low-Income Countries: Where is the Evidence that it Works? Joint NGO Briefing Paper No. 112. 2008 [Google Scholar]
- 13.Drechsler D, Jütting JP. Private Health Insurance in Low and Middle-Income Countries: Scope, Limitations, and Policy Responses. Paris: OECD Development Centre; 2005. p. 67. [Google Scholar]
- 14.Islam M. Health Systems Assessment Approach: A How-To Manual, U.S. Agency for International Development in Collaboration with Health Systems 20/20 Management Sciences for Health. Arlington, VA: USAID; 2007. [Google Scholar]
- 15.Smith PC. Provision of a public benefit package alongside private voluntary health insurance. In: Preker AS, Scheffler RM, Bassett MC, editors. Private Voluntary Health Insurance in Development Friend or Foe? Washington, DC: World Bank; 2007. pp. 147–67. [Google Scholar]
- 16.Alkhamis A. Health care system in Saudi Arabia: An overview. East Mediterr Health J. 2012;18:1078–9. doi: 10.26719/2012.18.10.1078. [DOI] [PubMed] [Google Scholar]
- 17.Alkhamis AA, Hassan A, Cosgrove P. Financing healthcare in Gulf cooperation council countries: A focus on Saudi Arabia. Int J Health Planning Manage. 2014;29:e64–82. doi: 10.1002/hpm.2213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Jeong HS, Niki R. Divergence in the development of public health insurance in Japan and the republic of Korea: A multiple-payer versus a single-payer system. Int Soc Secur Rev. 2012;65:51–73. [Google Scholar]
- 19.Naithani P. Challenges faced by expatriate workers in GCC countries. Int J Bus Manage. 2010;5:98–103. [Google Scholar]
- 20.The Council of Cooperative Health Insurance. Regulations for Cooperative Health Insurance System, Insurance. Riyadh: The Council of Cooperative Health Insurance; 2009. [Google Scholar]
- 21.Gallagher EB. Modernization and health reform in Saudi Arabia. In: Twaddle AC, editor. Health Care Reform Around the World. Ch. 4. London: Auburn House; 2002. pp. 181–97. [Google Scholar]
- 22.Alkhamis AA. Framing health policy in the context of Saudi Arabia. J Infect Public Health. 2016;9:3–6. doi: 10.1016/j.jiph.2015.11.002. [DOI] [PubMed] [Google Scholar]
- 23.Safi O. The challenges for Saudi Arabia healthcare system Indian. J Appl Res. 2016;6:231–3. [Google Scholar]
- 24.Kutner M, White S. Washington, DC: National Center for Education Statistics; 2006. The and Health Literacy of America’s Adults: Results from the 2003 National Assessment of Adult Literacy, NCES 2006-2483. [Google Scholar]
- 25.Levy H, Janke A. Health literacy and access to care. J Health Commun. 2016;21(Suppl 1):43–50. doi: 10.1080/10810730.2015.1131776. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Ministry of Labour. Saudi Labour Market Indicators, Riyadh Region. Riyadh: Ministry of Labour; 2009. p. 124. [Google Scholar]
- 27.Agency for Healthcare Research and Quality, Medical Expenditure Panel Survey-Healthcare Questionnaire. 2009. [Last accessed on 2016 Dec 1]. Available from: http://www.meps.ahrq.gov/mepsweb/survey.comp/survey.jsp .
- 28.McCormack L. Health insurance literacy of older adults. J Consum Aff. 2009;43:223–48. [Google Scholar]
- 29.United Nations Department of Economic and Social Affairs. World Population Prospects: The 2008 Revision in World Population Prospects: Population Division. New York: United Nations, Department of Economic and Social Affairs; 2008. p. 87. [Google Scholar]
- 30.Quinn K, Schoen C, Buatti L. On Their Own: Young Adults Living Without Health Insurance. 2000. [Last accessed on 2016 Nov 29]. Available from: http://www.commonwealthfund.org/usr_doc/quinn.safety in health care .
- 31.Short P. Counting and characterizing the uninsured. In: McGlaughlin C, editor. Health Policy and the Uninsured, Health Insurance Coverage in the United States 2013. Suppl 2. Vol. 22. Washington, DC: The Urban Institute Press; 2004. [Last accessed on 2016 Nov 29]. pp. 360–361. Available from: http://www.census.gov/InternMed . [Google Scholar]
- 32.Carper K, Beauregard K. Characteristics of Uninsured Workers: Estimates for the U.S. Civilian Noninstitutionalized Population 19-64 Years of Age Medical Expenditure Panel Survey No. 257. 2009:1–8. [Google Scholar]
- 33.Ahmad S. Prevalence and attitude of cigarette smoking among indian expatriates living in Jeddah, Kingdom of Saudi Arabia. J Int Oral Health. 2015;7:18–21. [PMC free article] [PubMed] [Google Scholar]
- 34.Joury AU, Al Atmi AA, Al Babtain SA, Alsharif M, Al Babtain NA, Mogbil AB, et al. Prevalence of depression and its association with socio-demographic characteristics among the general population. Int J Modern Altern Med Res. 2014;2:8–15. [Google Scholar]
- 35.Garnefski N, Teerds J, Kraaij V, Legerstee J, Kommer T. Cognitive emotion regulation strategies and depressive symptoms: Differences between males and females. Pers Individ Differ. 2004;36:267–76. [Google Scholar]
- 36.de Castro AB, Gee GC, Takeuchi DT. Job-related stress and chronic health conditions among filipino imexpatriatess. J Imexpatriates Minor Health. 2008;10:551–8. doi: 10.1007/s10903-008-9138-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Stewart MJ, Gillis A, Brosky G, Johnston G, Kirkland S, Leigh G, et al. Smoking among disadvantaged women: Causes and cessation. Can J Nurs Res. 1996;28:41–60. [PubMed] [Google Scholar]
- 38.Hill DJ, White VM, Scollo MM. Smoking behaviours of Australian adults in 1995: Trends and concerns. Med J Aust. 1998;168:209–13. doi: 10.5694/j.1326-5377.1998.tb140132.x. [DOI] [PubMed] [Google Scholar]
- 39.The Economist Intelligence Report. Health Care in Saudi Arabia. 2014. [Last accessed on 2016 Dec 20]. Available from: http://www.eiuperspectives.economist.com/healthcare/Saudi Arabia .
- 40.Health Insurance Coverage in the United States. [Last accessed on 2016 Dec 20];2013 22(Suppl 2):360–361. Available from: http://www.census.gov/InternMed . [Google Scholar]
- 41.Truman SD, Sharar DA, Pompe JC. The mental health status of expatriate versus U.S. Domestic workers: A comparative study. Int J Ment Health. 2011;40:3–18. [Google Scholar]
- 42.Grant-Vallone EJ, Ensher EA. An examination of work and personal life conflict, organizational support and employee health among international expatriates. Int J Intercult Relat. 2001;25:261–78. [Google Scholar]
- 43.Nadim W, Al Otaibi A, Al-Mohaimeed A, Ewid M, Sarhandi M, Saquib J, et al. Depression among migrant workers in Al-Qassim, Saudi Arabia. J Affect Disord. 2016;206:103–8. doi: 10.1016/j.jad.2016.07.037. [DOI] [PubMed] [Google Scholar]
- 44.Bonache J. Job Satisfaction among expatriates, repatriates and domestic employees: The perceived impact of international assignments on work related variables. BMC Health Res Serv. 2005;11:1–32. [Google Scholar]