

Abstract
Background and Aim.
Migraine is a common form of headache that affects patients quality of life negatively. In addition to pharmacologic treatment, there are a variety of nonpharmacologic treatments for migraine headache. In present study, we examined the effect of prayer on intensity of migraine pain.
Methods.
In a prospective, randomized, controlled trial from October 2013 to June 2014, this study has been conducted in Kerman, Iran. We randomly assigned 92 patients in 2 groups to receive either 40 mg of propranolol twice a day for 2 month (group “A”) or 40 mg of propranolol twice a day for 2 months with prayer (group “B”). At the beginning of study and 3 months after intervention, patients’ pain was measured using the visual analogue scale.
Results.
At the beginning of study and before intervention, the mean score of pain in patients in groups A and B were 5.7 ± 1.6 and 6.5 ± 1.9, respectively. According to results of independent t test, mean score of pain intensity at the beginning of study were similar between patients in 2 groups (P > .05). Three month after intervention, mean score of pain intensity decreased in patients in both groups. At this time, the mean scores of pain intensity were 5.4 ± 1.1 and 4.2 ± 2.3 in patients in groups A and B, respectively. This difference between groups was statistically significant (P < .001).
Conclusions.
The present study revealed that prayer can be used as a nonpharmacologic pain coping strategy in addition to pharmacologic intervention for this group of patients.
Keywords: complementary therapies, alternative therapies, pain intensity, migraine headache
The use of alternative medicine for illness is common among people in several countries with different religion and cultural background. A report of the National Center for Complementary and Alternative Medicine in 2002 showed that prayer for self (43%) and prayer for others (24.4%) are the 2 most commonly used alternative medicine practice in the United States.1
Use of prayer as an alternative treatment during time of illness received great attention by researchers in previous decade. In one study in this regard, Matthews et al2 examined the effects of intercessory prayer on patients with rheumatoid arthritis. Results of the study by Matthews et al2 showed that patients receiving in-person intercessory prayer showed significant overall improvement during 1-year follow-up. Matthews et al2 concluded that in-person intercessory prayer may be a useful adjunct to standard medical care for certain patients with rheumatoid arthritis. In the other study, Coleman et al3 examined the association of gender to use of prayer as a self-care strategy for managing the human immunodeficiency virua (HIV)-related symptoms of fatigue, nausea, depression, and anxiety among 448 African American men and women with HIV. Results of the study by Colemen et al3 showed that prayer is used as a self-care strategy by more 50% of the respondents for 3 of the 4 symptoms and is rated highly efficacious. In a randomized, blinded study, Olver and Dutney4 examined the effects of intercessory prayer on spiritual well-being in patients with cancer. Results of the study by Olver and Dutney4 showed that intercessory prayer significantly improved spiritual well-being in this group of patients.
The fourth leading cause of patients visits in the United States emergency departments are related to headache.5 Migraine is a common form of headache that remains an important public health problem.5–7 Recently Burch et al5 reported that 14.2% of the adults population in the United States suffers from some degree of migraine. In another study in this regard in the United States, Tepper8 reported that 8.7 million females and 2.6 million males suffer from migraine headache with moderate to severe disability. Pharmacologic therapies are the mainstay of migraine treatment. However, in recent years, some nonpharmacologic, alternative and complementary therapies, such as biofeedback, cognitive therapies, aerobic exercise, relaxation training, and acupuncture have been proposed for use in combination with pharmacologic therapies. In one study, Dittrich et al9 examined effects of aerobic exercise with relaxation on migraine patients’ level of pain. They reported that patients’ migraine pain intensity reduced significantly after implemented aerobic exercise with relaxation program.9
One of the most commonly used alternative medicine procedures that traditionally used by people both in relation to their own health and the health of others is prayer.10,11 The aim of this study was to examine the effect of prayer on intensity of pain in migraine patients.
Methods
This study is a double blind randomized controlled trial conducted from October 2013 to January 2014 in Kerman, Iran. This study has received permissions from deputy of research and also the ethics board of the Kerman University of Medical Sciences. Each patient was asked to fill in a written consent form (previously approved by ethics committees). In addition, all participants were promised that all data would remain anonymous, kept confidential, and be stored safely.
With regard to our pilot study and considering a power of 95% (beta) and P = .05% (alpha), the sample size would be 36 in each group (total 82).13 For increasing power of our finding we obtained 92 samples for present study. Samples were 92 patients suffering from migraine with and without aura according to the criteria of the International Headache Society12 (Table 1). Patients with other types of headache were excluded. Study patients were randomized into 2 groups to receive either 40 mg of propranolol twice a day for 2 months (group “A”) or 40 mg of propranolol twice a day for 2 months with prayer (group “B”) by the head nurse of the clinic, who chose the next serially numbered sealed opaque envelope containing a simple 1:1 randomization sequence. The head nurse were not aware of the study groups and aims in time randomization. The prayer group participated in an 8-week, weekly, intercessory prayer program with each session lasting 45 minutes. Pain reduction was measured at baseline and after 3 months, by registered nurses who were specialist in pain management and did not know which patients were in which groups (control or intervention), using a visual analogue scale. This scale has been used among Iranian patients and its reliability and validity have been confirmed by in previous studies in Iranian context.
Table 1.
International Headache Society Criteria for Migraine Used in the Present Study.
| A. At least 5 attacks fulfilling criteria below |
| B. Headache lasting 4 to 72 hours |
| 1. Unilateral location |
| 2. Pulsating quality |
| C. Headache characterized by at least 2 of the following |
| 3. Moderate or severe intensity (inhibits or prohibits daily activity) |
| 4. Aggravated by climbing stairs or similar routine physical activity |
| D. Headache accompanied by at least 1 of the following |
| 1. Nausea or vomiting, or both |
| 2. Photophobia and phonophobia |
A Kolmogorov-Smirnov test indicated that the data were sampled from a population with normal distribution. The data analysis was performed using SPSS (Statistical Package for the Social Sciences) version 17. A P value of less than .05 was considered as statistically significant. Descriptive statistics (expressed as mean and standard deviation), independent t test and paired t test were used.
Results
All patients who participate in present study were Muslim. Of the 92 patients, 82 were women. The mean age of all patients was 33.7 ± 10.3 years. Most patients were married (75%). The demographic characteristics including age, sex, level of education, and time of migraine diagnosis were similar in both groups of patients (P > .05) (Table 1) (Table 2).
Table 2.
Patients Demographic Characteristics.
| Items | Intervention | Control | P Value |
|---|---|---|---|
| Sex | >.05 | ||
| Male | 7 | 3 | |
| Female | 39 | 43 | |
| Marital status | >.05 | ||
| Single | 11 | 12 | |
| Married | 35 | 34 | |
| Level of education | >.05 | ||
| Diploma and lesser | 20 | 22 | |
| Postdiploma | 8 | 7 | |
| Graduate | 16 | 14 | |
| Postgraduate | 2 | 3 | |
| Age (years) | 34.2 ± 12.3 | 33.2 ± 7.8 | >.05 |
| Duration of disease (years) | 5.2 ± 5.1 | 4.7 ± 3.4 | >.05 |
| Pain score before study | 6.5 ± 1.9 | 5.7 ± 1.6 | >.05 |
At the beginning of study and before intervention, the mean score of pain in patients in groups A and B were 5.7 ± 1.6 and 6.5 ± 1.9, respectively. According to results of the independent t test, mean score of pain intensity at the beginning of study were similar between patients in 2 groups (P > .05). Three months after intervention, the mean score of pain intensity decreased in patients in both groups. In this time, the mean score of pain intensity were 5.4 ± 1.1 and 4.2 ± 2.3 in patients in groups A and B, respectively. This difference between groups was statistically significant (P < .001) (Figure 1).
Figure 1.
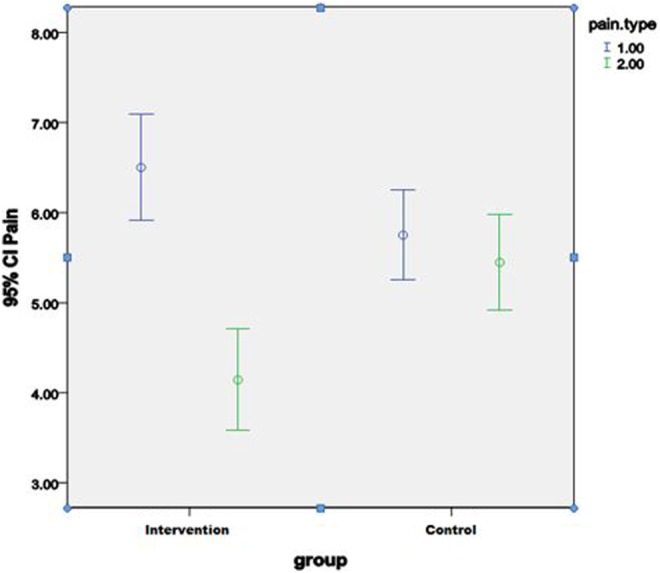
Pain score in patients before and after the intervention.
Discussion
In addition to pharmacologic treatment, there are a variety of nonpharmacologic treatments for headache.13 Religious activity may be one of several pain coping strategies to manage suffering.14 In the present study, we examined the effect of prayer as a non pharmacologic method in alleviating migraine pain. According to finding of present study prayer have positive effect on reducing migraine pain.
According to definition of the National Center for Complementary and Alternative Medicine, “prayer is an active process of communicating with and appealing to a higher spiritual power.”15 The word of “prayer” and its derivatives, which have been mentioned several times in the Holy Quran (holy book of the Muslims), are rooted in “pray” and means “asking for something,” “making a request for a need,” and “seeking help.”16 There are several types of prayer, including conversational prayer, meditative prayer, ritual prayer, and intercessory prayer.17 Intercessory prayer is one type of prayer that is organized, regular, and committed to setting time aside with the belief that the prayers are communicating with God.18 Results of previous studies showed that religious activity have positive effect on physical and mental health. In a review study in this regards, Coruh et al19 reported that religious intervention such as intercessory prayer may improve success rates of in vitro fertilization, decrease length of hospital stay and duration of fever in septic patients, increase immune function, improve rheumatoid arthritis, and reduce anxiety and complications in patients with heart disease.
The use of complementary and alternative medicine among migraine patients is a growing phenomenon.20 Results of one study in this regard showed that 31.4% of migraine patients used complementary and alternative medicine. This study also showed that most common reason for deciding to try a complementary and alternative medicine therapy was that it offered a “potential improvement of headache” (47.7%).20 Although use of prayer tested in different clinical setting, previous studies about use of prayer for migraine pain are limited. Recently, in one study, researchers examined the effect of different meditation types on headache frequency, headache severity, and pain medication among patients with migraine headache. They randomly assigned 92 patients to 1 of 4 groups: (1) spiritual meditation, (2) internally focused secular meditation, (3) externally focused secular meditation, and (4) progressive muscle relaxation. Results of this study showed that migraine frequency and migraine medication usage decreased in patients who received the spiritual meditation in compared to patients who received other type of meditation.21 In another study in this regard, Wachholtz and Pargament22 compared effect of spiritual meditation, internally focused secular meditation, externally focused secular meditation, and muscle relaxation on pain tolerance, headache frequency, and mental and spiritual health variables. Results of Wachholtz and Pargament22 showed that spiritual meditation had greater effect in decreasing patients frequency of migraine headaches, anxiety, and negative effect, as well as greater increases in pain tolerance, headache-related self-efficacy, daily spiritual experiences, and existential well-being.
Conclusion
Migraine pain is bad experiences that affect patients quality of life negatively. The present study revealed that prayer can be used as a nonpharmacologic pain coping strategy in addition to pharmacologic intervention for this group of patients.
Footnotes
Author Contributions: The work presented here was carried out through collaboration between all authors. HT and NZ defined the research theme. HT, NZ and KD designed methods, ZE and HR collected data, HS analyzed the data, interpreted the results. All authors have contributed to, seen, and approved the article.
Declaration of Conflicting Interests: The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval: The work was approved by the Ethics Committee of Kerman University of Medical Sciences.
References
- 1. Barnes P, Powell-Griner E, McFann K, Nahin R. CDC Advance Data Report #343: Complementary and Alternative Medicine Use Among Adults: United States. Washington, DC: National Center for Complementary and Alternative Medicine; 2002. [PubMed] [Google Scholar]
- 2. Matthews DA, Marlowe SM, MacNutt FS. Effects of intercessory prayer on patients with rheumatoid arthritis. South Med J. 2000;93:1177–1186. [PubMed] [Google Scholar]
- 3. Coleman CL, Holzemer WL, Eller LS, et al. Gender differences in use of prayer as a self-care strategy for managing symptoms in African Americans living with HIV/AIDS. J Assoc Nurses AIDS Care. 2006;17(4):16–23. [DOI] [PubMed] [Google Scholar]
- 4. Olver IN, Dutney A. A randomized, blinded study of the impact of intercessory prayer on spiritual well-being in patients with cancer. Altern Ther Health Med. 2012;18(5):18–27. [PubMed] [Google Scholar]
- 5. Burch RC, Loder S, Loder E, Smitherman TA. The prevalence and burden of migraine and severe headache in the United States: updated statistics from government health surveillance studies. Headache. 2015;55:21–34. [DOI] [PubMed] [Google Scholar]
- 6. Turkcuer I, Serinken M, Eken C, et al. Intravenous paracetamol versus dexketoprofen in acute migraine attack in the emergency department: a randomised clinical trial. Emerg Med J. 2014;31:182–185. [DOI] [PubMed] [Google Scholar]
- 7. Bigal ME, Lipton RB, Stewart WF. The epidemiology and impact of migraine. Curr Neurol Neurosci Rep. 2004;4:98–104. [DOI] [PubMed] [Google Scholar]
- 8. Tepper SJ. A pivotal moment in 50 years of headache history: the first American Migraine Study. Headache. 2008;48:730–731. [DOI] [PubMed] [Google Scholar]
- 9. Dittrich SM, Günther V, Franz G, Burtscher M, Holzner B, Kopp M. Aerobic exercise with relaxation: influence on pain and psychological well-being in female migraine patients. Clin J Sport Med. 2008;18:363–365. [DOI] [PubMed] [Google Scholar]
- 10. Masters KS, Spielmans GI, Goodson JT. Are there demonstrable effects of distant intercessory prayer? A meta-analytic review. Ann Behav Med. 2006;32:21–26. [DOI] [PubMed] [Google Scholar]
- 11. Masters KS, Spielmans GI. Prayer and health: review, meta-analysis, and research agenda. J Behav Med. 2007;30:329–338. [DOI] [PubMed] [Google Scholar]
- 12. Headache Classification Committee of the International Headache Society. Classification and diagnostic criteria for headache disorders, cranial neuralgia and facial pain. Second edition. Cephalalgia. 2004;(suppl 1):1–160. [PubMed] [Google Scholar]
- 13. Nicholson RA, Buse DC, Andrasik F, Lipton RB. Nonpharmacologic treatments for migraine and tension-type headache: how to choose and when to use. Curr Treat Options Neurol. 2011;13:28–40. [DOI] [PubMed] [Google Scholar]
- 14. Tronvik E, Sørensen T, Linde M, et al. The relationship between headache and religious attendance (the Nord-Trøndelag health study–HUNT). J Headache Pain. 2014;15:1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Prayer and spirituality in health: ancient practices, modern science. CAM NIH. 2005;12:1–5. http://nccam.nih.gov/news/newsletter/2005_winter/prayer.htm. Accessed March 2007. [Google Scholar]
- 16. Atarodi AR, Mottaghi MR, Atarodi F. Comparative study on the effect of prayer and praise on peace of mind and physical health from male and female students’ points of view in Gonabad’s guidance schools in 2011. Islamic Life Center Health. 2013;1(2):34–39. [Google Scholar]
- 17. Jantos M, Kiat H. Prayer as medicine: how much have we learned? Med J Aust. 2007;186(10 suppl): S51–S53. [DOI] [PubMed] [Google Scholar]
- 18. Dusek JA, Sherwood JB, Friedman R, et al. Study of the Therapeutic Effects of Intercessory Prayer (STEP): study design and research methods. Am Heart J. 2002;143:577–584. [DOI] [PubMed] [Google Scholar]
- 19. Coruh B, Ayele H, Pugh M, Mulligan T. Does religious activity improve health outcomes? A critical review of the recent literature. Explore (NY). 2005;1:186–191. [DOI] [PubMed] [Google Scholar]
- 20. Rossi P, Di Lorenzo G, Malpezzi MG, et al. Prevalence, pattern and predictors of use of complementary and alternative medicine (CAM) in migraine patients attending a headache clinic in Italy. Cephalalgia. 2005;25:493–506. [DOI] [PubMed] [Google Scholar]
- 21. Wachholtz AB, Malone CD, Pargament KI. Effect of different meditation types on migraine headache medication use [published online April 11, 2015]. Behav Med. doi:10.1080/08964289.2015.1024601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Wachholtz AB, Pargament KI. Migraines and meditation: does spirituality matter? J Behav Med. 2008;31:351–366. [DOI] [PubMed] [Google Scholar]