

1. BACKGROUND
The European Medicines Agency (EMA) has the responsibility for the scientific evaluation, supervision, and safety monitoring of medicines in the European Union (EU) to ensure that their benefits outweigh their risks. While the roots of medicines' safety monitoring lie in the development of mechanisms for spontaneous reporting of suspected adverse reactions by health‐care professionals and patients, the importance of using the full spectrum of evidence including observational studies has long been acknowledged.1, 2, 3 The risk management system introduced in the EU in 2006 highlighted the need to build capacity and to facilitate the conduct of multicenter independent postauthorization studies to investigate important risks or missing information in European populations.4 In March 2006, the EMA contacted more than 90 academic centers in Europe identified through the International Society for Pharmacoepidemiology (ISPE) and national drug regulatory authorities to request information on their expertise and activities in pharmacoepidemiology and pharmacovigilance. Over the following 12 months, possible models for collaboration on independent observational studies were discussed with representatives of academic and other research centers, pharmaceutical industry, other existing clinical networks, EMA scientific committees, and the European Commission.5 The European Network of Centres for Pharmacoepidemiology and Pharmacovigilance (ENCePP; www.encepp.eu) was launched on June 28, 2007 with 79 participants who agreed to develop an active research network based on principles of transparency, scientific independence, and common quality standards. The European Network of Centres for Pharmacoepidemiology and Pharmacovigilance was presented in a symposium at the 24th International Conference on Pharmacoepidemiology and Therapeutic Risk Management in August 2008.6 Ten years on, we review ENCePP's main achievements, discuss its impact on the benefit‐risk evaluation of medicinal products in Europe, and outline future perspectives.
2. WHY WAS ENCEPP NEEDED?
Although collaborations for multicenter studies have long existed, the pharmacoepidemiology landscape in Europe has been heterogeneous and based on researchers using stand‐alone data sources with limited sample sizes and applying differing quality standards. This heterogeneity was compounded by differences between health‐care systems, uncertainty about available databases, and uncertainty on existing collaborations with sufficient expertise and capacity to conduct multicenter observational studies. It was often considered easier for industry to conduct postauthorization studies requested by EU regulators in the United States, despite differences in characteristics of study populations, clinical practice, and prescription patterns. There was a need to foster a network of researchers able to perform large observational studies in Europe and for a pool of experts providing clear guidance on best practices in pharmacoepidemiology. At the same time, rules and principles for quality standards and transparency of research were also needed to ensure that these studies would be performed according to the best possible level of scientific quality.5 New EU pharmacovigilance legislation entered into force in July 2012 provided a legal framework for postauthorization safety studies (PASS). This enabled regulators to impose PASS on pharmaceutical companies as a condition of the marketing authorization and established a review process for PASS study protocols and results by the EMA's Pharmacovigilance Risk Assessment Committee (PRAC).7 In this context, ENCePP has assumed a triple role: (a) to increase capacity for pharmacoepidemiology research in Europe, (b) to define common methodological standards, and (c) to propose governance principles for the conduct of collaborative studies.
3. WHAT HAS BEEN ACHIEVED BY ENCEPP IN 10 YEARS?
3.1. A strong scientific network supporting evaluation of medicines
Initially, ENCePP foresaw nomination of coordinating centers taking responsibility for research within defined therapeutic areas. However, besides the organizational challenges posed by the differing interests and expertise of centers and the diverse nature of research questions to be addressed, most centers were also concerned that in a competitive environment, a structure with predefined subnetworks overseen by a coordinating center would be too rigid and give too much prominence to such center. They preferred a flexible approach whereby centers would be characterized in a public, transparent, and searchable electronic inventory and could enter into ad hoc collaborations for specific projects underpinned by common transparency and research standards. As of July 31, 2017, ENCePP included 168 centers from 18 European countries, 126 (75%) of them being not for profit organizations (eg, universities, hospitals, foundations, or charities) and 42 (25%) for‐profit organizations (ie, contract research organizations). The largest numbers of centers are located in the United Kingdom (35 centers), Italy (24), France and Germany (18 each), Spain (17), and the Netherlands (10).8 Centers applying to join the network undergo a check by the ENCePP Secretariat to determine their focus on pharmacoepidemiology or pharmacovigilance. This is based on a description of their activities and a list of publications, but level of expertise or quality of research is not assessed. At an early stage, ENCePP discussed implementation of a self‐accreditation system but considered that it would not guarantee the quality of the studies performed by the centers.
Through the centers, ENCePP provides access to a large pool of experts in pharmacoepidemiology and pharmacovigilance across Europe and to other relevant specialists such as clinical pharmacologists, statisticians, specialist clinicians, and members of health technology assessment (HTA) bodies, pediatric networks, and pharmacogenomic groups. Since 2010, this expertise provides a strong support to the operation of the new pharmacovigilance legislation by complementing regulatory guidance with methodological recommendations.
Although one of the aims of creating ENCePP was to increase the capacity for large pharmacoepidemiology studies in Europe, the flexible approach adopted by ENCePP for collaborations and the multiple sources of public and private funding do not allow to confirm to date that multicenter studies were initiated with the support of ENCePP. However, feedback received from members suggests that the new culture of collaboration, the common scientific standards, and the common governance principles introduced by the ENCePP have greatly facilitated the establishment of research consortia, for example, in the context of the EMA‐funded studies (Table 1) and the European Commission's Seventh Framework Program for drug safety studies (Table 2).3 Consortia were also created in the context of public‐private partnerships established by the Innovative Medicines Initiative.9 In addition, ENCePP members provided occasionally to EMA data that could support drug safety reviews. This information covered topics such as combined hormonal contraceptive and the risk of venous thromboembolism, strontium ranelate in the treatment of osteoporosis, bromocriptine‐containing medicines indicated in the suppression of lactation postpartum, ambroxol‐ and bromhexine‐containing medicines and allergic reactions, codeine‐containing medicines and the risk of morphine toxicity, or hydroxyzine‐containing medicines and pro‐arrhythmogenic potential.
Table 1.
Studies funded by European Medicines Agency (EMA) to support the benefit‐risk evaluation of medicinal products (2010‐2017)a
| Study Title | EUPAS Register Numberb | Number of Databases | Number of Countries | Link to Publication of Results |
|---|---|---|---|---|
| A/H1N1 pandemic vaccines and pregnancy outcomes | 1705 | 1 | 1 | Link to study report included in EU PAS Register |
| Impact of risk minimization in patients treated with rosiglitazone‐containing products | 1777 | 2 | 2 | https://www.ncbi.nlm.nih.gov/pubmed/24068766 |
| Isotretinoin and the effectiveness of the pregnancy prevention program in Europe | 2474 | 5 | 3 | Link to study report included in EU PAS Register |
| Patterns and determinants of use of oral contraceptives in the EU | 2738 | 5 | 3 | https://www.ncbi.nlm.nih.gov/pubmed/26492444 |
| Monitoring the effectiveness of risk minimization in patients treated with pioglitazone‐containing products | 2765 | 3 | 3 | Link to study report included in EU PAS Register |
| Risk of cardiac valve disorders associated with the use of biphosphonates | 2616 | 6 | 3 | https://www.ncbi.nlm.nih.gov/pubmed/26694594 |
| Association between anxiolytic or hypnotic drugs and total mortality | 3772 | 2 | 2 | https://www.ncbi.nlm.nih.gov/pubmed/26256008 |
| Metformin use in renal impairment | 5249 | 2 | 2 |
http://bmjopen.bmj.com/content/5/9/e008531.full
https://www.ncbi.nlm.nih.gov/pubmed/27504911 |
| Study of regulatory communication and risk awareness following the article 31 referral of combined hormonal contraceptives in relation to thromboembolism | 21356 | n/ac | 6 | Study ongoing |
| Characterizing the risk of major bleeding in patients with nonvalvular atrial fibrillation: noninterventional study of patients taking direct oral anticoagulants in the EU | 16014 | 9 | 6 | Study ongoing |
| Study of utilization of combined hormonal contraceptives in Europe | 21352 | 3 | 3 | Study ongoing |
| Antimicrobial resistance: choice of therapeutic interventions and outcomes for the treatment of infections caused by multidrug (MDR) Gram‐negative pathogens | 21359 | 1 | 5 | Study ongoing |
| Methods and data sources for determining long‐term effects of drug exposure during pregnancy, with application to antiepileptic medicines | 21171 | n/ad | 28 | Study ongoing |
| Impact of EU label changes for systemic diclofenac products: postreferral prescribing trends | Study planned | 4 | 3 | |
| Impact of EU label changes for hydroxyzine products: postreferral prescribing trends | Study planned | 4 | 3 |
Studies listed in chronological order.
The EU PAS Register search page is available at http://www.encepp.eu/encepp/studySearch.htm.
Not applicable: study using a survey design.
Not applicable: survey of available data sources in all EU Member states.
Table 2.
Studies funded by the European Commission's Seventh Framework Program for drug safety studies to support the benefit‐risk evaluation of medicinal products (2007‐2013)a
| Study Title | EUPAS Register Numberb | No. of Data Sources (D, Database; R, Registry) | No. of Countries | Link to Information on CORDIS Websitec |
|---|---|---|---|---|
| SOS: Safety of nonsteroidal antiinflammatory drugs | D: 8 | 4 | http://cordis.europa.eu/project/rcn/89349_en.html | |
| ARITMO: arrhythmogenic potential of drugs | 2361 | D: 7 | 5 | http://cordis.europa.eu/project/rcn/94061_en.html |
| ADDUCE: attention deficit hyperactivity disorder drug chronic effects | 3985, 4551 | D: 3 | 2 | http://cordis.europa.eu/project/rcn/96780_en.html |
| EUROmediCAT: safety of medication use in pregnancy in relation to risk of congenital malformations | 2221 | D: 7 | 5 | http://cordis.europa.eu/project/rcn/98223_en.html |
| PHARMACHILD: long‐term pharmacovigilance for adverse effects in childhood arthritis focusing on immuno‐modulatory drugs | 1974 | R: 4 | 4 | http://cordis.europa.eu/project/rcn/96819_en.html |
| STOP: suicidality: treatment occurring in pediatrics | D: 3 | http://cordis.europa.eu/project/rcn/97369_en.html | ||
| CARING: cancer risks and insulin analogues | 5383 | D: 3 R: 2 | 5 | http://cordis.europa.eu/project/rcn/100436_en.html |
| SAFEGUARD: safety evaluation of adverse reactions in diabetes | 2895, 4364 | D: 9 | 6 | http://cordis.europa.eu/project/rcn/100121_en.html |
| Astro‐Lab: assessment of safety of LABAs in asthma in routine care by combining health‐care databases and direct patient follow‐up | 3099 | D: 2 | 2 | http://cordis.europa.eu/project/rcn/101108_en.html |
| EpoCan: assessing long‐term risks and advancing toward better epoetin‐driven treatment modalities | D: 3 | 2 | http://cordis.europa.eu/project/rcn/100286_en.html | |
| PREDICTION‐ADR: personalization of treatment in cardiovascular disease through next‐generation sequencing in adverse drug reactions | n/ad | n/a | http://cordis.europa.eu/project/rcn/109336_en.html |
Studies listed in chronological order.
The EU PAS Register search page is available at http://www.encepp.eu/encepp/studySearch.htm.
CORDIS: European Commission's Community Research and Development Information Service.
Not applicable: the study objective was the development of genetic risk assessment and diagnostic tools.
The long‐term success of the network will depend on its capacity to keep current members engaged and involve new members to take‐up future methodological challenges, taking into account that new data sources such as social media and big data will likely play an increasing role in the benefit‐risk evaluation of medicinal products. In this regard, a concept paper on methodological aspects associated with use of different models for data extraction and analysis from electronic health records, their validation, and their regulatory applications is being developed.
3.2. Better knowledge and accessibility of data sources
An objective of ENCePP is to identify data from clinical or administrative electronic databases available in Europe, coordinate these data in a comprehensive and public inventory, and facilitate their access to researchers. Database holders and professionals with expertise in use of specific data sources are invited to provide a description of their core data (eg, coding systems and dictionaries used, type of events, and medicinal products covered), demographic information, information on data linkage and data access, and a list of relevant publications derived from the data.8 Since 2017, disease registries are also registered in the context of the EMA Patient Registry Initiative.10 As of July 31, 2017, the inventory included 83 data sources (Figure 1). The inventory provides key information on a large number of databases and helps investigators identify relevant data sources available to answer specific research questions. It represents a core source of information on data available for the benefit‐risk evaluation of medicines.11
Figure 1.
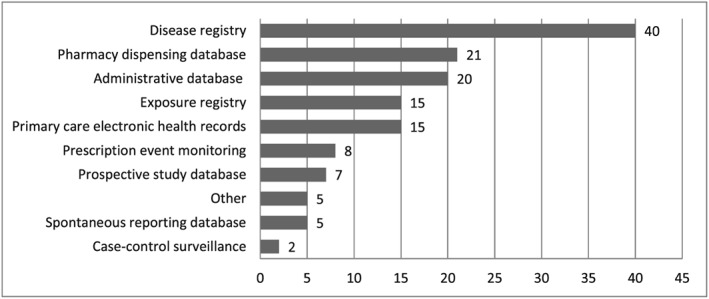
Distribution of 83 data sources registered in ENCePP (as of 31/07/2017), by type chosen by the center registering the study (the total is 138 as a same data source may be of several types)
3.3. Increased transparency for studies
In November 2010, the ENCePP e‐Register of Studies was launched to increase the transparency of observational postauthorization studies and maximize the availability and accessibility of postauthorization evidence on medicines.1 The idea of the registration of observational studies in pharmacoepidemiology or other areas of epidemiology was controversial in 2010. Some authors did not favor it,12, 13, 14 while others considered that the ability to upload the study protocols, study interim and final reports, and other relevant documents increase transparency, facilitate collaborations, allow feedback by peer‐reviewers, and may ultimately lead to better science. 15, 16 The ENCePP e‐Register was adopted as the EU electronic Register of Postauthorization Studies (EU PAS Register®) following the new EU pharmacovigilance legislation, which made it mandatory for marketing authorization holders to register PASS imposed as a legal obligation by regulators—the so‐called Risk Management Plan (RMP) category 1 and category 2 studies, and subsequently the recommendation made in the EU Good pharmacovigilance practices to register other PASS included in the RMP (RMP category 3 studies).7 It therefore became an essential tool for the implementation of the legislation. As of July 31, 2017, 1,145 studies had been registered (Figure 2); 368 of them (30.4%) had been finalized, and more than half of them (n = 583, 50.9%) were studies requested by a regulatory authority, of which 95 (16.3%) have been imposed as a legal obligation and 316 (54.2%) are included in an EU RMP (Figure 3). Risk assessment and effectiveness evaluation have been the main purpose of 49.7% and 26.7% of studies, respectively (Figure 4). Both objectives are mentioned for 13.5% of the studies.
Figure 2.
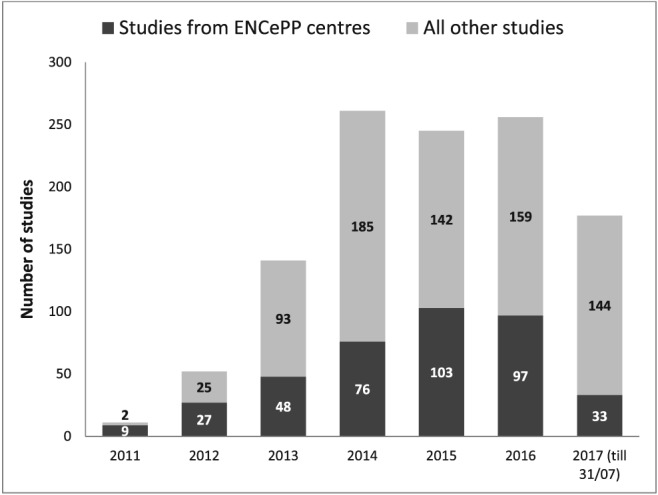
Number of studies registered in the EU PAS Register by ENCePP centers and other centers, 2011 to 2017 (total: 1145)
Figure 3.
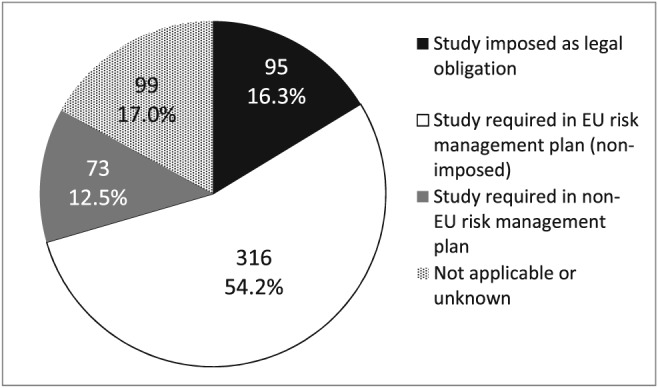
Distribution of studies registered in the EU PAS Register as of 31/07/2017 and requested by a regulatory authority (n = 583), by regulatory status
Figure 4.
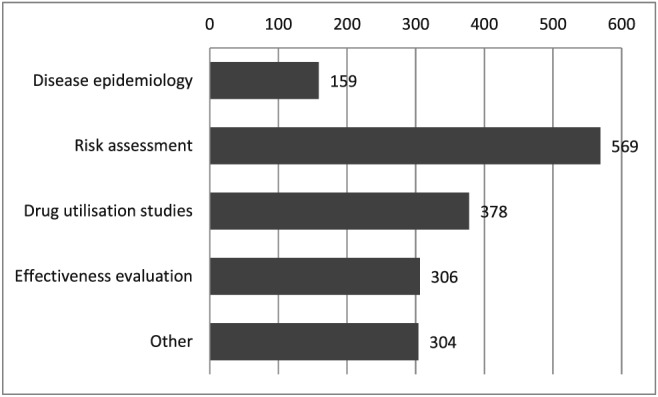
Distribution of 1145 studies registered in the EU PAS Register as of 31/07/2017 according to the main scope(s) (the total is 1716 as more than 1 scope is mentioned for some studies)
Registration of studies in the EU PAS Register has changed the landscape of pharmacoepidemiology and pharmacovigilance by giving public access to evaluations carried out on specific drugs and safety concerns and providing visibility on investigators, data availability, methods, and funding sources. The register has become a must‐go‐to source to learn about studies addressing specific research questions and learn about their design as a tool to plan new studies.
With the exception of imposed PASS, study registration is voluntary. It has been shown that up to July 2015 49% of the PASS reviewed by PRAC in the context of regulatory procedures had been entered in the EU PAS Register and only 43% of these entries had a protocol available.17 This limitation may affect the usefulness of the registration to judge the quality of the studies on the basis of a detailed description of the design and analytical approach.18
On June 29, 2011, a workshop with medical journal editors sought their views toward upload of study results before their acceptance and appearance in print. Although the editors accepted in principle that study results of public health relevance could be shared without delay, this confirmation did not reassure many investigators reluctant to upload the study protocol and report in the EU PAS Register prior to the publication in a scientific journal online or in print.19 A way forward could be that medical journal editors would require the EU PAS Register number for all manuscripts reporting results of postauthorization studies (even if study results have not yet been uploaded) as a means to decrease publication bias, similarly to the existing requirement for clinical trials.
3.4. Better methods for studies
In early discussions, ENCePP agreed that, rather than establishing an accreditation system for centers, research quality would be best supported by providing recommendations on the practical implementation of pharmacoepidemiological principles based on published guidance and illustrative examples. The first ENCePP Guide on Methodological Standards in Pharmacoepidemiology was published in May 2011 and has been updated annually by structured review to maintain its dynamic nature. The sixth revision in July 2017 has 31 authors and 424 electronic references.20 The guide offers a concise, dynamic, and publicly available Web resource for methodological English language guidance in pharmacoepidemiology. An electronic version was introduced for the third revision in 2013, and the number of times each revision has been viewed has since steadily increased to about 50,000 for revision 5 (2015‐2016), while the entire document has been downloaded about 10,000 times during the same period (Figure 5). The guide is used for training in many institutions including research centers and industry and cited as a reference source of methodological best practice in several regulatory documents such as the EU good pharmacovigilance practice.7
Figure 5.
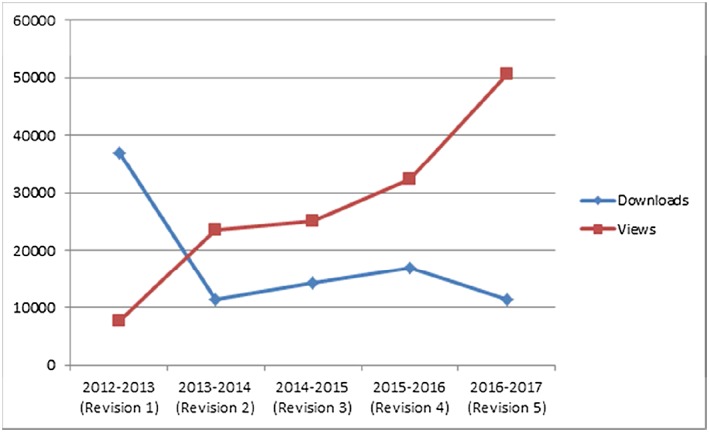
Number of times the electronic ENCePP Guide on Methodological Standards in Pharmacoepidemiology was viewed and downloaded from July 2012 to July 2017 [Colour figure can be viewed at wileyonlinelibrary.com]
In parallel, ENCePP developed a Checklist for Study Protocols to stimulate researchers' consideration of important principles when designing and writing a pharmacoepidemiological study protocol, to facilitate protocol review by other parties, and to promote transparency regarding methodologies and design used in studies. To assist regulatory authorities in identifying whether such principles have been applied in PASS protocols, pharmaceutical companies have to append the checklist to protocols submitted to regulators.7, 21
3.5. Better governance for studies including management of interests
In line with its aim to promote transparency and scientific independence, the ENCePP developed a Code of Conduct laying out best practice in the relationship between investigators and study funders, irrespective of whether the study funder is a public body, industry, or a regulatory authority.22 At the core of scientific independence is the provision that no person with a financial, commercial, or personal interest in a particular outcome of the study shall take part in any study activity that could influence the results or their interpretation in any particular direction. To ensure transparent research, the code requires registration of the study in a public registry (for instance, the EU PAS Register) and agreement to make public relevant information including the Checklist for Study Protocols, study data specified in the guidance for sharing of ENCePP Study Data,23 and the content of the research contract or a declaration on the use of own resources.
To confirm a commitment to comply with the provisions of the code, the lead investigator may apply for an ENCePP Seal. This requires the provision of a signed checklist and signed declaration of compliance with the Code of Conduct, the signed Checklist for Study Protocols, and a signed Declaration of Interests to the ENCePP Secretariat prior to study start. The study has also to be registered in the EU PAS Register, and the full protocol must be uploaded prior to data collection or extraction. Once the ENCePP Secretariat has confirmed the a priori eligibility for the seal, it adds the ENCePP Seal logo to the registration record and the investigators can use this logo on materials and publications. The lead investigator may, however, ask to postpone the publication of the protocol until the study is finalized. As of July 31, 2017, 45 studies had an ENCePP Seal. The protocol and final study report have been published for all of the 15 finalized studies, while the study protocol has been published for 7 of the 22 ongoing studies (31.8%) and for 2 of 8 planned studies (25.0%).
The ENCePP Code of Conduct has been a landmark document defining the relationships between study sponsors and investigators willing to conduct studies with full scientific independence. It became a key reference for the conduct of studies and underpinned the development of guidance by other groups,24 but it has shown some limitations: the key principle of scientific independence is not explicitly defined and, even though many provisions of the code are written as obligations, their application is a matter of commitment without verification that they have been implemented. The ENCePP Seal, which was developed to formalize this commitment, has a low uptake, and the publication of the protocol was often postponed until the study end. Furthermore, the wording of the code may be interpreted as suggesting that some of its provisions do not apply if the seal is not requested. A working group is currently evaluating the need to improve the ENCePP Code of Conduct and the ENCePP Seal concept in light of the experience and to better define and implement the principle of scientific independence.
3.6. Other activities
To answer specific questions or respond to consultations, different ad hoc working groups have been created over time (information on www.encepp.eu). A concept paper addressed the legal definition of “noninterventional trials,” and a collaboration with representatives of HTA bodies looked at specific HTA‐related methodological aspects of studies. A special interest group (SIG) on Drug Safety in Pregnancy was created to inform future activities of ENCePP in medicines used in pregnancy and lactation, to liaise with other relevant groups in this field, and to develop an overview of data sources for drug safety in pregnancy research. A SIG on Measuring the Impact of Pharmacovigilance Activities was created to provide recommendations to the PRAC on key methodologies for measuring health outcomes of pharmacovigilance measures in the context of the overall evaluation of the impact of pharmacovigilance systems.25
4. LESSONS LEARNED
The ENCePP has been created in a heterogeneous landscape of academic centers, research organizations and database owners, and a changing regulatory environment in pharmacovigilance and pharmacoepidemiology. There was therefore a risk that differing priorities and constraints would lead to divergent routes after an initial period of collaboration. We believe that several factors explain that ENCePP achieved important outcomes from its onset and remained a coherent, dynamic, and active network over 10 years: (1) a recognized need for collaboration to address limitations in the pharmacoepidemiological landscape and keep abreast of methodological, regulatory, and organizational developments (eg, increased use of existing data sources, new legislation on PASS, new funding opportunities); (2) a firm commitment to common guiding principles of transparency, scientific independence, and quality standards; (3) an acknowledgment of the diversity in the centers' domain of expertise and capacity to collaborate; (4) a strong governance based on an elected Steering group and several working groups, with the support from EMA; (5) last but not least, the ability to meet face to face in plenary meetings on a periodic basis and to actively contribute to the development of good practice and regulatory guidance. All these factors have been instrumental to foster and accelerate partnership between research centers and improve the implementation of collaborative studies.
5. FUTURE PERSPECTIVES
Table 3 lists priorities proposed for the next years of ENCePP based on the further development of existing activities described in this article.
Table 3.
Future perspectives for the next years of ENCePP network
| (1) Facilitate the initiation and conduct of observational research in Europe and propose mechanisms to support multinational and multidatabase studies |
| (2) Improve the ENCePP code of conduct with additional tools to promote transparency, scientific independence, and good governance of pharmacoepidemiological research |
| (3) Ensure that the ENCePP network remains focused on public health and supports health decision‐makers such as regulatory authorities, health technology assessment bodies, and public health institutions |
| (4) Ensure that the network embraces relevant innovative data sources and areas of activity, eg, social media information and big data |
| (5) Continue to support best methodological practices in the conduct of pharmacoepidemiology |
| (6) Further develop the “pharmacovigilance” component of ENCePP and develop a methodological framework for measuring the public health impact of pharmacovigilance activities |
The integration of the “pharmacovigilance” component into the network's activities has not been fully realized so far. This may be because a well‐structured network of national and/or regional pharmacovigilance centers has existed for a long time in Europe with a coordination of activities at national and European levels and that a 5 year research project on methods in pharmacovigilance (the IMI PROTECT project) was started in September 2009 with the objective to review and develop if necessary methods for signal detection,26 and its results were integrated into the ENCePP Guide on methodological standards. An ENCePP SIG has been initiated to review the application of pharmacoepidemiological methods to measure the public health impact of pharmacovigilance activities (information on www.encepp.eu), and ENCePP will work together with the PRAC, the International Society of Pharmacovigilance, and other networks to identify other areas where a collaboration will strengthen the benefit‐risk evaluation of medicines.
A Joint Task Force of ISPE and the International Society for Pharmacoeconomics and Outcome Research recently published recommendations to enhance decision‐makers' confidence in evidence derived from real‐world studies.27, 28 The principles of transparency in the process for database studies, transparency in study execution, and good procedural practices they promote are very close to those recommended in the ENCePP Code of Conduct, Checklist for Study Protocols, and Guide for Methodological Standards. Close collaboration among ISPE, IPOR, and ENCePP, for example, through cross‐reference to each other's recommendations, common publications, and collaboration in the annual updating of the ENCePP Guide on Methodological Standards, would provide a unique opportunity to promote common principles and standards on a global scale.
An important challenge remains: studies still take a long time to be finalized, often because of administrative aspects, slow access to available health data often due to data protection concerns, heterogeneous systems, or lack of resources. The European Network of Centres for Pharmacoepidemiology and Pharmacovigilance will need to address the challenges by using innovative tools and designs and new data sources to conduct faster studies through collaborations.
6. CONCLUSIONS
In 10 years, the ENCePP has made a major contribution to the benefit‐risk evaluation of medicinal products in Europe and beyond by providing methodological recommendations complementing regulatory guidance on postauthorization safety studies. The development of the EU PAS Register also changed the landscape of pharmacoepidemiology in Europe by increasing transparency of observational research, giving access to study protocols and results and supporting the implementation of the pharmacovigilance legislation. The ENCePP Code of Conduct aims to promote transparency and scientific independence in research, but its implementation depends on researchers' commitment and it is being reviewed in light of the constraints imposed in transparency and restriction of study funders' involvement in the study. Perhaps most importantly, ENCePP has created a strong European community supporting methodological standards, transparency, and scientific independence in pharmacoepidemiological research.
DISCLAIMER
The views expressed in this article are the personal views of the authors and may not be understood or quoted as being made on behalf of or reflecting the positions of their employer organization.
CONFLICT OF INTEREST
X.K. is an employee of the EMA, the chair of the ENCePP Steering Group, and the co‐chair of ENCePP WG1 on Research Standards. S.P.G. is the vice president and global head of epidemiology at RTI‐HS, a former co‐chair of the ENCePP Steering Group, and a former co‐chair of ENCePP WG1 on Research Standards.
ACKNOWLEDGEMENTS
The authors gratefully acknowledge Kevin Blake, Henry Fitt, Thomas Goedecke, Alexandra Pacurariu, and Dagmar Vogl for their assistance in the preparation of this article.
Besides the members of the ENCePP Steering Group, the following persons played an important role in the establishment and development of ENCePP (in alphabetic order):
ENCePP members: Eric Abadie, Francisco De Abajo, Lucien Abenhaim, Deborah Ashby, Helen Dolk, Stephen Evans, David Haerry, Joan‐Ramon Laporte, Hubert Leufkens, Jytte Lyngvig, Nicholas Moore, Ingemar Persson, June Raine, Gonzalo Calvo Rojas, Saad Shakir, Miriam Sturkenboom, and Mary Teeling.
Former or current EMA employees: Stella Blackburn, Kevin Blake, Henry Fitt, Thomas Goedecke, Veronika Jekerle, Thomas Lönngren, Stefanie Prilla, Eeva Rossi, Camilla Smeraldi, Panos Tsintis, Dagmar Vogl, and Noël Wathion.
Kurz X, Perez‐Gutthann S, the ENCePP Steering Group . Strengthening standards, transparency, and collaboration to support medicine evaluation: Ten years of the European Network of Centres for Pharmacoepidemiology and Pharmacovigilance (ENCePP). Pharmacoepidemiol Drug Saf. 2018;27:245–252. https://doi.org/10.1002/pds.4381
REFERENCES
- 1. Blake KV, de Vries CS, Arlett P, Kurz X, Fitt H. Increasing scientific standards, independence and transparency in post‐authorisation studies: the role of the European Network of Centres for Pharmacoepidemiology and Pharmacovigilance. Pharmacoepidemiol Drug Saf. 2012;21(7):690‐696. [DOI] [PubMed] [Google Scholar]
- 2. Laporte JR. Fifty years of pharmacovigilance—medicines safety and public health. Pharmacoepidemiol Drug Saf. 2016;25(6):725‐732. [DOI] [PubMed] [Google Scholar]
- 3. Arlett P, Sarac SB, Thomson A, et al. The European Medicines Agency's use of prioritised independent research for best evidence in regulatory action on diclofenac. Pharmacoepidemiol Drug Saf. 2014;23(4):431‐434. [DOI] [PubMed] [Google Scholar]
- 4. Blake KV, Prilla S, Accadebled S, et al. European Medicines Agency review of post‐authorisation studies with implications for the European Network of Centres for Pharmacoepidemiology and Pharmacovigilance. Pharmacoepidemiol Drug Saf. 2011;20(10):1021‐1029. [DOI] [PubMed] [Google Scholar]
- 5. Persson I, Fitt H, Jekerle V. Model for ENCePP. European Medicines Agency, May 2007. http://www.encepp.eu/publications/documents/ENCePPConceptPaper_May07.pdf [last accessed on 12/10/2017]
- 6. Wathion NA, Blackburn S, Kurz X, Persson IR, Moride Y, Sturkenboom MCJM. A European Network of Centres for Pharmacovigilance and Pharmacoepidemiology (ENCePP). Pharmacoepidemiol Drug Saf. 2008;17:S26 [Google Scholar]
- 7. European Medicines Agency. Good pharmacovigilance practice. Module VIII. Post‐authorisation safety studies (Rev 2), 2016. http://wema/docs/en_GB/document_library/Scientific_guideline/2012/06/WC500129137.pdf [last accessed on 12/10/2017]
- 8. ENCePP. Resources database. http://www.encepp.eu/encepp/resourcesDatabase.jsp [last accessed on 12/10/2017]
- 9. Goldman M, Seigneuret N, Eichler HG. The innovative medicines initiative: an engine for regulatory science. Nat Rev Drug Discov. 2015;14(1):1‐2. [DOI] [PubMed] [Google Scholar]
- 10. European Medicines Agency. Patient registries. http://www.ema.europa.eu/ema/index.jsp?curl=pages/regulation/general/general_content_000658.jsp%26mid=WC0b01ac0580961211 [last accessed on 12/10/2017]
- 11. Santoro A, Genov G, Spooner A, Raine J, Arlett P. Promoting and protecting public health: how the European Union pharmacovigilance system works. Drug Saf. 2017;40(10):855‐869. https://doi.org/10.1007/s40264‐017‐0572‐8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Sorensen HT, Rothman KJ. The prognosis for research. Br Med J. 2010;340(feb17 2):c703 [DOI] [PubMed] [Google Scholar]
- 13. Vandenbroucke JP. Preregistration of epidemiologic studies: an ill‐founded mix of ideas. Epidemiology. 2010;21(5):619‐620. [DOI] [PubMed] [Google Scholar]
- 14. Chavers S, Fife D, Wacholtz M, Stang P, Berlin J. Registration of observational studies: perspectives from an industry‐based epidemiology group. Pharmacoepidemiol Drug Saf. 2011;20(10):1009‐1013. [DOI] [PubMed] [Google Scholar]
- 15. Schneeweiss S, Avorn J. Postmarketing studies of drug safety. A European initiative could help bring more transparency and rigour to pharmacoepidemiology. Br Med J. 2011;342(feb08 1):d342 [DOI] [PubMed] [Google Scholar]
- 16. Loder E, Groves T, MacAuley D. Registration of observational studies. Br Med J. 2010;340(feb18 2):c950 [DOI] [PubMed] [Google Scholar]
- 17. Engel P, Almas MF, De Bruin ML, Starzyk K, Blackburn S, Dreyer NA. Lessons learned on the design and the conduct of post‐authorization studies: review of 3 years of PRAC oversight. Br J Clin Pharmacol. 2017;83(4):884‐893. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Blake KV, Smeraldi C, Kurz X, Arlett P, Blackburn S, Fitt H. The European Network of Centres for Pharmacoepidemiology and Pharmacovigilance: application to diabetes and vascular diseases. Br J Diabetes Vasc Dis. 2011;11(6):304‐307. [Google Scholar]
- 19. European Medicines Agency. ENCePP Workshop with Medical Journal Editors. 29 June 2011. http://www.encepp.eu/events/documents/Minutes_Journaleditorsworkshop_29Jun2011.pdf [last accessed on 12/10/2017]
- 20. ENCePP. Standards and guidance. http://www.encepp.eu/standards_and_guidances/index.shtml [last accessed on 12/10/2017]
- 21. European Medicines Agency. Guidance for the format and content of the protocol of non‐interventional post‐authorisation safety studies. http://www.ema.europa.eu/docs/en_GB/document_library/Other/2012/10/WC500133174.pdf [last accessed on 12/10/2017]
- 22. ENCePP. Code of conduct. http://www.encepp.eu/code_of_conduct/index.shtml [last accessed on 12/10/2017]
- 23. ENCePP. Code of conduct—implementation guidance for sharing of ENCePP study data. http://www.encepp.eu/code_of_conduct/documents/Annex4_SharingData.pdf [last accessed on 12/10/2017]
- 24. Kurz X, Bauchau V, Mahy P, Glismann S, van der Aa LM, Simondon F. The ADVANCE code of conduct for collaborative vaccine studies. Vaccine. 2017;35(15):1844‐1855. [DOI] [PubMed] [Google Scholar]
- 25. European Medicines Agency. PRAC strategy on measuring the impact of Pharmacovigilance activities. 11 January 2016. http://www.ema.europa.eu/docs/en_GB/document_library/Other/2016/01/WC500199756.pdf [last accessed on 12/10/2017]
- 26. Wisniewski AF, Bate A, Bousquet C, et al. Good signal detection practices: evidence from IMI PROTECT. Drug Saf. 2016;39(6):469‐490. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Wang SV, Schneeweiss S, Berger ML, et al. Reporting to improve reproductibility and facilitate validity assessment for healthcare database studies V1.0. Pharmacoepidemiol Drug Saf. 2017;26(9):1018‐1032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Berger ML, Sox H, Willke RJ, et al. Good practices for real‐world data studies of treatment and/or comparative effectiveness: recommendations from the joint ISPOR‐ISPE Special Task Force on real‐world evidence in health care decision making. Pharmacoepidemiol Drug Saf. 2017;26(9):1033‐1039. [DOI] [PMC free article] [PubMed] [Google Scholar]