

Corticotropin-releasing hormone binding protein (CRHBP) plays a modulatory role in regulating the function of the canonical stress-responsive HPA axis. It is also found throughout the brain where it functions to regulate the availability of neuronally released corticotropin-releasing hormone (CRH) in relation to the activation of CRH receptors located in extrahypothalamic brain regions. In this issue, O’Connell, Goldstein-Piekarski et al. (1), report a novel and potentially important finding demonstrating that variation in the CRHBP gene (single nucleotide polymorphism (SNP rs28365143)) predicts effective antidepressant treatment response. This effect was selective to serotonin reuptake inhibitor (SSRI) treatment and was not observed in relation to serotonin/norepinephrine reuptake inhibitor (SNRI) treatment. While much additional work and validation needs to be performed, these findings point to the possibility that genetically determined differences in the function of CRHBP are mechanistically involved in mediating the antidepressant effects of SSRI antidepressants. CRHBP is an important member of the CRH system but it has been relatively understudied in relation to psychopathology, and this finding adds to others suggesting that more in depth studies of CRHBP may be fruitful.
Since the early work of Hans Selye, cortisol and the HPA axis have been associated with adaptive and maladaptive responses to stress (2). In response to stress, CRH is released from neurons in the paraventricular nucleus of the hypothalamus, which stimulates the release of adrenocorticotropin hormone (ACTH) from the anterior pituitary, which in turns stimulates the secretion of cortisol from the adrenal cortex. For years, evidence has been accumulating linking various alterations in the function of the HPA axis to depression. Early studies focused on cortisol and, after the characterization of CRH by Wylie Vale in 1981 (3), researchers intensely focused on CRH as a possible candidate underlying the pathophysiology of depression and accompanying HPA alterations. Subsequent basic research established that CRH was not only found in the hypothalamus where it functions to stimulate the release of ACTH, but was also found throughout the brain in key regions that are involved in mediating behaviors, emotions, and physiological responses (4). CRH acting as a neurotransmitter was found to play an integrative role across these domains in coordinating adaptive responses to stress. In addition to CRH, its two receptors (CRHR1 and CRHR2) were identified as well as the CRHBP (5, 6). Additional discoveries, included the characterization of the urocortins, 3 additional endogenous ligands that are members of the CRH family with differing affinities for CRHR1 and CRHR2. All of the components of the CRH system are differentially but strategically located throughout the brain such that they are positioned to modulate the neural circuitry associated with stress and coping responses. Identification of the CRH receptors led to the development of numerous small molecule antagonists aimed at targeting the CRHR1 receptor. Unfortunately, after numerous clinical trials, these antagonists were not found to be effective for the treatment of depression or anxiety disorders (7). In the face of substantial preclinical data suggesting probable efficacy, it remains unclear as to why this strategy has not been successful. In part, the lack of efficacy of CRHR1 antagonists may be due to the capacity of the other components of the CRH system, including CRHBP, to rapidly adapt when perturbed. This suggests the possibility that targeting more than one of the CRH system components might be a more effective treatment strategy. Despite efforts, no small molecule antagonists selective for CRHR2 have been identified and no strategies aimed at altering the CRHBP have been explored for clinical utility.
The findings reported in the current O’Connell, Goldstein-Piekarski et al., (1) paper point to a potentially important role of the CRHBP in modulating SSRI antidepressant treatment response and also suggest that alterations in CRHBP function could be important in the pathophysiology of stress-related psychopathology. CRHBP was originally isolated from human plasma and is hypothesized to function as a secreted protein modulating the actions of CRH (8). Subsequently, CRHBP was found to be expressed in the brain, pituitary and other peripheral tissues. Notably, CRHBP is expressed in key brain regions implicated in the pathophysiology of anxiety and depression including the hippocampus, ventral tegmental area (VTA), bed nucleus of the stria terminalis and the central nucleus of the amygdala (6, 8). CRHBP is thought to function by sequestering CRH thereby reducing its availability to activate CRH receptors (see figure 1). However, some studies indicate additional roles for CRHBP. For example, data suggests that CRHBP may facilitate the actions of CRH at CRHR2 receptors in the VTA. In addition, CRHBP has been suggested to enhance CRH signaling through CRH receptor-independent mechanisms and to potentially aid in the trafficking of the CRHR2 to the cell surface (8). Numerous studies in rodents have shown that levels of CRHBP in various brain regions are highly responsive to psychological stressors (for review see (8)). Additionally, one CRHBP SNP was previously associated with treatment response (differing from the SNP associated with treatment response reported in the current study) and two additional SNPs have been associated with depression (9). Finally, we reported a non-significant decrease in CRHBP mRNA levels in postmortem amygdala tissue in males suffering from major depression, and significant decreases in CRHBP expression in males with schizophrenia and bipolar disorder (10).
Figure 1.
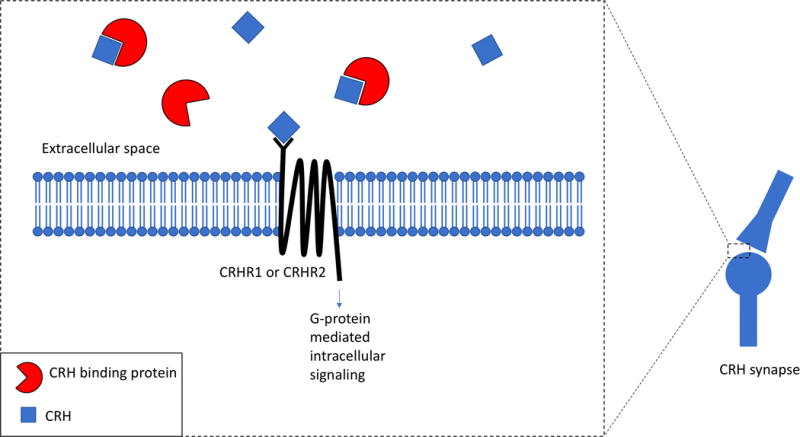
CRH binding protein can reduce the actions of CRH on its constituent receptors by binding free CRH molecules, thereby reducing its availability.
Together, this evidence makes CRHBP an interesting candidate in conceptualizing mechanisms by which acute and long-term stress influence the development of psychopathology. From the current report, it appears that genetic variation in CRHBP may be involved with mediating treatment response to SSRIs and may serve as a predictor for antidepressant treatment selection. As the authors point out, if these findings stand the test of time, they may be useful from a “personalized medicine” approach to enhance the likelihood of successful antidepressant treatment. Finally, these and other data, suggest that it is reasonable to consider the development of new antidepressant treatment strategies focused on modulating CRHBP function.
Acknowledgments
This work was supported by National Institute of Mental Health grants: P50-MH100031, R01-MH046729, and R01-MH081884.
References
- 1.O’Connell CP, Goldstein-Piekarski A, Nemeroff CB, Schatzberg AF, Debattista C, Carrillo-Roa T, Binder EB, Dunlop BW, Craighead WE, Mayberg HS, Williams LM. Genetic variation in corticotropin-releasing hormone binding protein predicts antidepressant outcomes. The American journal of psychiatr. 2018 doi: 10.1176/appi.ajp.2017.17020172. In press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Selye H. The evolution of the stress concept. Am Sci. 1973;61:692–699. [PubMed] [Google Scholar]
- 3.Vale W, Spiess J, Rivier C, Rivier J. Characterization of a 41-residue ovine hypothalamic peptide that stimulates secretion of corticotropin and beta-endorphin. Science. 1981;213:1394–1397. doi: 10.1126/science.6267699. [DOI] [PubMed] [Google Scholar]
- 4.Owens MJ, Nemeroff CB. Physiology and pharmacology of corticotropin-releasing factor. Pharmacol Rev. 1991;43:425–472. [PubMed] [Google Scholar]
- 5.Takahashi LK. Role of CRF(1) and CRF(2) receptors in fear and anxiety. Neurosci Biobehav Rev. 2001;25:627–636. doi: 10.1016/s0149-7634(01)00046-x. [DOI] [PubMed] [Google Scholar]
- 6.Potter E, Behan DP, Linton EA, Lowry PJ, Sawchenko PE, Vale WW. The central distribution of corticotropin-releasing factor (CRF)-binding protein predicts multiple sites and modes of interaction with CRF. Proceedings of the National Academy of Sciences of the United States of America. 1992;89:4192–4196. doi: 10.1073/pnas.89.9.4192. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Murrough JW, Charney DS. Corticotropin-Releasing Factor Type 1 Receptor Antagonists for Stress-Related Disorders: Time to Call It Quits? Biological psychiatry. 2017;82:858–860. doi: 10.1016/j.biopsych.2017.10.012. [DOI] [PubMed] [Google Scholar]
- 8.Ketchesin KD, Stinnett GS, Seasholtz AF. Corticotropin-releasing hormone-binding protein and stress: from invertebrates to humans. Stress. 2017;20:449–464. doi: 10.1080/10253890.2017.1322575. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Binder EB, Nemeroff CB. The CRF system, stress, depression and anxiety-insights from human genetic studies. Molecular psychiatry. 2010;15:574–588. doi: 10.1038/mp.2009.141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Herringa RJ, Roseboom PH, Kalin NH. Decreased amygdala CRF-binding protein mRNA in post-mortem tissue from male but not female bipolar and schizophrenic subjects. Neuropsychopharmacology : official publication of the American College of Neuropsychopharmacology. 2006;31:1822–1831. doi: 10.1038/sj.npp.1301038. [DOI] [PubMed] [Google Scholar]