

Abstract
BACKGROUND:
Robinow Syndrome is an extremely rare genetic disorder characterised by abnormalities in head, face and external genitalia. This disorder exists in dominant pattern with moderate symptoms and recessive pattern with more physical and skeletal abnormalities. It was first introduced by Menihard Robinow in 1969. It was related to chromosome 9q22 ROR2 gene related to bone and cartilage growth aspects.
CASE PRESENTATION:
A 17-year-old Egyptian male presented to National Research Centre Orodental genetics Clinic with typical features of short stature and facial dysmorphism weighted 50 Kg and measured 150 cm height complaining of facial dis figurement. There was no significant prenatal history, and family history was negative for congenital disabilities and genetic disorders. Clinical examination revealed macrocephaly and special facial features as prominent forehead, deformed ear pinna, hypertelorism, flat nasal tongue tie, deficient malar bone, bow-shaped upper and lower lips and dimpled chin. Orally the patient suffered from tonetie, gingival hypertrophy and dental malalignment. The orthopantomogram showed multiple impacted teeth. The physical examination revealed that the patient had deformed spine, short limbs with ectrodactyly, micropenis & hypospadias. Surgical management included correction of midface deficiency with zygomatic augmentation, closed rhinoplasty for the broad nose, lips muscles release and tongue tie relief. The patient is currently undergoing orthodontic treatment for his teeth.
CONCLUSION:
Improvement of facial features and a good psychological impact on the patient and his family.
Keywords: Robinow Syndrome, Genetic disorder, Zygomatic Augmentation, Closed Rhinoplasty
Introduction
Robinow syndrome is an extremely rare genetic disorder characterised by abnormalities in the head, face, stature, extremities and external genitalia. This disorder exists in dominant pattern with moderate symptoms and the recessive pattern with more physical and skeletal abnormalities.
Robinow Syndrome was first introduced by Menihard Robinow in 1969 [1]. It was related to a gene on chromosome 9q22. Tyrosine Kinase-like orphan receptor 2 ROR2 gene was related to bone and cartilage growth aspects [2].
Case presentation
A 17 year - old Egyptian male, born of unrelated parents had presented to National Research Center Orodental Genetics clinic with short stature, and facial dysmorphism weighted 50 Kg and measured 150 cm height complaining from facial disfigurement. There was no significant prenatal history, and family history was negative for any previous congenital disabilities or genetic abnormalities. Clinical examination revealed macrocephaly and special facial features as the prominent forehead, deformed ear pinna, hypertelorism, flat nasal bridge, deficient malar bone, bow-shaped upper and lower lips (Figure 1).
Figure 1.
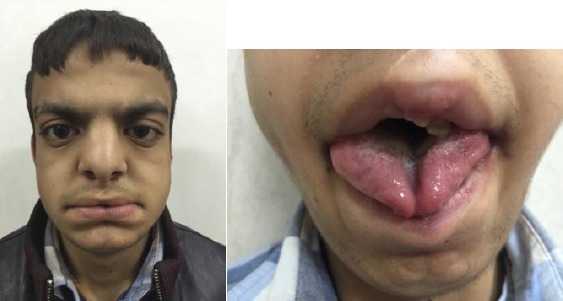
Facial features of Robinow syndrome (left); Abnormal tongue (right)
Orally the patient suffered from tongue tie (Fig. 1 right), dental malalignment (Fig. 2a) and gum hypertrophy (Fig. 2b).
Figure 2.
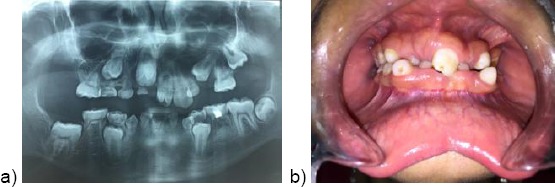
a) Panoramic X-ray showing dental crowding; b) Gum hypertrophy
The orthopantogram showed multiple impacted teeth. General physical examination revealed that the patient had deformed spine, short limbs with ectrodactyly (Fig. 3), micropenis and hypospadias.
Figure 3.

Ectrodactyly
Surgical Management
Soft tissue surgical repair was made for this patient to correct lip muscles (upper & lower) deficiency in midline resembling whistle deformity in bilateral cleft lip cases, with dissection of orbicularis oris muscle fibers intraorally using VY technique to increase the mucosal tissue with plication suture in order to have muscle continuity & approximation of levator labii superioris fibers.
Lip surgery included V-Y incisions on the mucosal surface of the upper & lower lips. Through this approach, the two lateral bulges of the orbicularis muscle were reached, dissected and repositioned with a more medial position using 3 0 vicryl sutures to compensate for midline muscle bulk deficiency.
In the upper lip, the levator labii superioris was reached on both sides and approximated together and suspended to ANS periosteum to achieve lengthening and eversion of the lip. The V incision was closed in Y technique to help in formation of lip tubercle.
As regards the lower lip V - Y technique was inverted to help in increasing the height of mucosal surface and decreasing the eversion of the lip laterally through excision of the excess mucosa towards the midline and suturing it medially. The accentuated labiomental groove was improved just following the lower lip surgery (Figure 4 a, b).
Figure 4.

a) Upper lip surgery; b) Lower lip surgery
Closed surgical rhinoplasty was performed for the nasal bridge to correct the broad nose. The surgical approach to the nose was reached through a bilateral marginal incision. Reductive tip plasty was performed through resection of small tip of the cephalic part of the lower bilateral cartilages and applying an interdorsal suture to refine the tip and intercrural sutures to approximate the medial crura. Two lateral para medial osteotomies together with two lateral osteotomies were done to narrow the wide bony pyramids.
The patient had to wear a gypsum surgical stent over the nose with plasters for almost a month till complete healing and some oedema was clinically noticed that was treated afterwards with anti-inflammatory and took some time to subside (Figure 5a, 5b).
Figure 5.
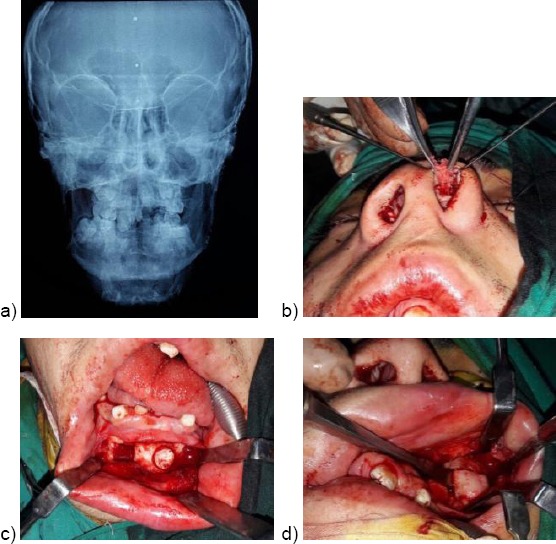
a) PA radiographic view; b) Closed surgical rhinoplasty; c) Harvesting chin bone; d) Zygomatic augmentation
Zygomatic bone augmentation was made by harvesting autogenous cortical cancellous bone block from the chin intraorally via vestibular incision about 1 cm2 to correct midface depression bilaterally. This technique was preferred over using alloplastic graft material to avoid tissue interaction or the possibility of body rejection (Figure 5c, 5d). There was a noticeable improvement in the facial features and profile appearance as well as the positive psychological impact (Figure 6, 7 and 8). The patient is currently undergoing orthodontic treatment for dental arch continuity.
Figure 6.

a) Lip before surgery; b) Lip after surgery
Figure 7.

a) Face Before; b) Face after surgery
Figure 8.
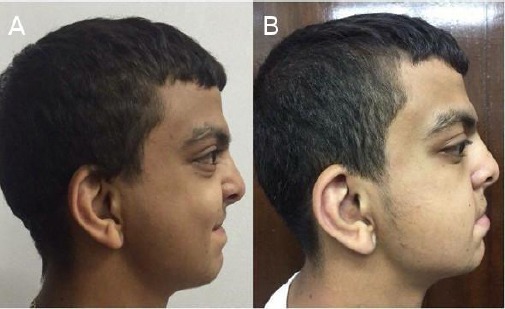
a) Profile before; b) Profile after surgery
Discussion
Robinow Syndrome is an extremely rare genetic disorder characterised by short stature, fetal face, abnormalities in the head, and external genitalia, as well as vertebral segmentation. It was introduced by Menihard Robinow in 1969 [1].
Based on the initial pedigree, this syndrome was attributed to be an autosomal dominant inherited syndrome [Online Mendelian Inheritance in Man (OMIM) 180700] with high penetrance [1] [2]. Researchers linked the gene for the autosomal recessive Robinow syndrome to chromosome 9q22. The gene is responsible for cartilage and bone growth [3]. The male to female ratio of patients with Robinow syndrome is 1:1. Although the incidence is about 1:500,000, however, the prevalence is slightly less due to the death of 5 - 10 % of patients during infancy [4].
Two forms of the disorder exist the dominant & recessive form which occurs more common. Patients with the dominant form often suffer from moderate symptoms [5]. While patients with a recessive form that is more aggressive, are usually more physically affected, and individuals may exhibit severe skeletal abnormalities particularly in Turkey, Oman & Czechoslovakia [6] [7].
In 2002 a case of 10 years male patient was presented by Holsakar HS et al. [8] born of unrelated parents after a normal pregnancy, presented with facial dysmorphism and short stature.
There was no significant peri-natal history, and family history was negative for congenital disabilities and genetic disorders. The patient who was 6 months old weighed 43 Kg, measured 54 cm height and head circumference 36 cm. Management includes orthodontic treatment for dental malalignment and facial reconstruction in selected cases also surgical repair of vertebral deformity and growth hormone therapy occasionally.
In the present case, we did some facial reconstruction including nose, lips and midface using autogenous bone block harvested from the chin rather than using alloplastic graft material as polycaprolactone PCL for fear of tissue interaction and the possibility of graft rejection. In 2009 an 8 years old female patient was reported by Eronat N. et al. [9]. The patient was born to consanguineous parents and had typical recessive type anomalies such as short stature & dysmorphic facial features, besides the typical orodental findings. No surgical interference was made for that case. However, In the current study, the decision was made for surgical management concerning the facial features trying to convert the looks of the patient from syndromic to non-syndromic look.
After the soft tissue surgery reconstruction especially for the nose using closed rhinoplasty with no extra nasal scars for removal of the nasal hump and zygomatic augmentation, the patient looked different. In 2008 Grothe R et al. [10] introduced an interesting case of Robinow with severe hyperplastic gingival tissue impeding both normal tooth eruption as well as orthodontic movement. Growth hormone GH therapy has been proved to cause improvement in the growth rate in children with Robinow syndrome and GH deficiency.
The prognosis for Robinow syndrome is good with more than 80% of patients having normal intelligence [11] [12]. A fetal ultrasound can provide a parental diagnosis at 19 weeks of pregnancy. However, it’s not always easy to differentiate between a fetus suffering from the milder dominant form from the serious recessive form. Radiographs are useful for assessment of rib or spinal deformities anomalies and may also help to document face and hand anomalies [13]. The patient still needs further plastic surgery for ears and digits. Also, there is still undergoing orthodontic treatment for teeth malalignment correction.
In conclusion, improvement of facial features as well as the psychological impact on the patient and his family.
Footnotes
Funding: This research did not receive any financial support
Competing Interests: The authors have declared that no competing interests exist
References
- 1.Robinow M, Silverman FN, Smith HD. A newly recognized dwarfing syndrome. Am J Dis Child. 1969;117:645. doi: 10.1001/archpedi.1969.02100030647005. https://doi.org/10.1001/archpedi.1969.02100030647005. [DOI] [PubMed] [Google Scholar]
- 2.Daniella F, Ivete P. Orofacial manifestations of Robinow’s Syndrome: a case report in a pediatric patient. J Oral Surg, Oral Med, Oral Path, Oral Radiol. 2008;105:353. doi: 10.1016/j.tripleo.2007.05.032. https://doi.org/10.1016/j.tripleo.2007.05.032. PMid:18061493. [DOI] [PubMed] [Google Scholar]
- 3.Patton M, Afzal A. Robinow Syndrome Journal of Medical Genetics. 2002;39:305. doi: 10.1136/jmg.39.5.305. https://doi.org/10.1136/jmg.39.5.305. PMid:12011143. PMCid:PMC1735132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Robinow M. Robinow syndrome. In: Buyse ML, editor. Birth Defects Encyclopedia. Massachusettes: Blackwell scientific publications; 1990. pp. 1499–1500. [Google Scholar]
- 5.Soman C, Lingappa A. Robinow Syndrome: A Rare Case Report and Review of Literature. Int J Clin Pediatr Dent. 2015;8:149. doi: 10.5005/jp-journals-10005-1303. https://doi.org/10.5005/jp-journals-10005-1303. PMid:26379386. PMCid:PMC4562051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Wang LY, Hsu CH, Shih SL, Lin SP. Robinow syndrome: report of one case. 1997;38:235. [PubMed] [Google Scholar]
- 7.Van Bokhoven H, Celli J, Kayserili H, van Beusekom E. Mutation of the gene encoding the ROR2 tyrosine kinase causes autosomal recessive Robinow syndrome. Nature Genetics. 2000;25:423. doi: 10.1038/78113. https://doi.org/10.1038/78113. PMid:10932187. [DOI] [PubMed] [Google Scholar]
- 8.Hosalkar HS, Gerardi J, Shaw BA. Robinow syndrome. J Postgrad Med. 2002;48:50. PMid:12082331. [PubMed] [Google Scholar]
- 9.Eronat N, Cogulu D, Ozkinay F. A case report on an autosomal recessive Robinow syndrome. Eur J Paediatric Dent. 2009;10:147. PMid:19761290. [PubMed] [Google Scholar]
- 10.Grothe R, Anderson-Cermin C, Beiraghi S. Autosomal recessive Robinow syndrome: a case report. J Dent Child. 2008;75:48. [PubMed] [Google Scholar]
- 11.Castells S, Chakurkar A, Qazi Q, Bastian W. Robinow syndrome with growth hormone deficiency: treatment with growth hormone. J Pediatr Endocrinol Metab. 1999;12:565. doi: 10.1515/jpem.1999.12.4.565. https://doi.org/10.1515/JPEM.1999.12.4.565. PMid:10417975. [DOI] [PubMed] [Google Scholar]
- 12.Soliman AT, Rajab A, Alsalmi I, Bedair SM. Recessive Robinow syndrome: with emphasis on endocrine functions. Metabolism. 1998;47:1337. doi: 10.1016/s0026-0495(98)90301-8. https://doi.org/10.1016/S0026-0495(98)90301-8. [DOI] [PubMed] [Google Scholar]
- 13.Patton M, Afzal A. Robinow Syndrome Journal of Medical Genetics. 2002;39:305. doi: 10.1136/jmg.39.5.305. https://doi.org/10.1136/jmg.39.5.305. PMid:12011143. PMCid:PMC1735132. [DOI] [PMC free article] [PubMed] [Google Scholar]