

Abstract
OBJECTIVE:
This study aimed to evaluate maximum bite forces (mBF) in dominant (DS) and non-dominant sides (NDS) at certain time periods after the insertion of new complete dentures based on prior experience and gender.
MATERIALS AND METHODS:
A total of 88 patients, complete denture wearers (CDWs), were examined. The maximum bite force at the intercuspal position between the first molars in 3 seconds was registered and recorded with piezoelectric gnathodynamometer. The procedure was repeated 3 times in identical conditions, with relaxation intervals of 1 minute between repeats and the limiting factor was the subjective feeling of pain. Testing of parametric data was performed with One Way Repeated Measurement of ANOVA test.
RESULTS:
The average mBF values increased during the observational period, both on the DS and NDS, with significant difference in DS, which was greater. The analysis of one-factor variance showed that there were differences of average mBF values in DS and NDS during six consecutive measurements (mBF–DS = 11.3, p = 0.0001, and mBF-NDS = 2.26, p = 0.047). Significant changes in the masticatory force (mBF) on the DS and NDS is explained by different measurement times and with the prior experience with complete dentures, BF–DS = 11.76, p = 0.0000; mBF–NDS = 2.42, p = 0.0351; mBFe–DS = 40.48; P = 0.0000 mBFe–NDS = 39.93, p = 0.0000.
CONCLUSION:
mBF represents a significant discriminating variable of the level of functional adaptation of new complete denture wearers (nCDWs) about the initial measurements.
Keywords: Maximum Bite Force, Complete Denture, Gnathodynamometer
Introduction
Being edentulous is considered a handicap, both concerning the oral function and psychological impact. The restoration of masticatory function and aesthetics is an important aim in dentistry mainly when patients present with extensive tooth loss. The loss of teeth in elderly patients not only impairs the stomatognathic system but also their psychological status and quality of life [1] [2].
Complete dentures should, biologically, establish the relationship with the living tissues. During rehabilitation with prosthetic treatment, forces acting in the oral cavity should be considered, as well as, the way these forces are distributed through the dentures on the denture bearing areas [3]. Distribution of masticatory forces under physiological conditions is as follows: occlusal - articular complex → periodontium → bone foundation. However, the biological organisation of the orofacial system responsible for the distribution of bite forces is complex and differs from the physiological mode of pressure conveyance.
Various methods have been used to numerically assess the masticatory forces while chewing various foods [4]. It is thought that Black was the first researcher who used measurements and estimates of masticatory forces as well as having researched in vitro feeding with an instrument, which he nominated a phagodynamometer. Obtained values ranged between 90N and 360N [5]. Howell and Brudevold presented the method for direct measurement of masticatory forces in the oral cavity [6].
The influence of biting forces (BF) on the masticatory system is profound. Incomplete denture wearers (CDWs) consuming tough foods, bite forces are reduced by 15% to 20% compared to healthy dentate patients, that is 40% [7]. The masticatory load in natural teeth is 200N while the maximum forces during mastication of CDWs range between 60N and 80N [8]. Tooth loss and its consequent prosthetic replacement not only decrease the BF between 20% to 50% compared to the natural dentition but is also associated with other problems such as eventual bone loss [9]. According to De Boever, only 4% of functional forces are utilised, while the maximum bite force (mBF) values during mastication do not exceed 22% of their capacity [10]. Muscle force and the number of functional teeth are determinant factors in mastication. Measuring mBF is an attempt to quantify the force that mandibular elevator muscles can make [11]. The magnitude of bite force has shown to be correlated to the patients’ satisfaction with complete dentures, type of food, and the amount of bone resorption under prostheses [12].
This study aimed to evaluate the maximum bite force (mBF) in the dominant side (DS) and non-dominant (NDS) at specific time periods after fitting of new complete dentures based on patient’s prior experience and gender.
Material and Methods
A total of 88 patients with complete dentures were included in this study. The research was accepted and approved by the Ethics Committee, School of Dental Medicine, University of Prishtina, Kosovo, and written consent was obtained from each subject.
The research was divided into two experimental groups and compared to experienced complete denture wearers (eCDW). Group 1 consisted of inexperienced (first time) complete denture wearing patients (iCDW) fitted with maxillary and mandibular complete dentures; Group 2 consisted of experienced patients with complete dentures (eCDW). The patients were pooled at the Department of Prosthodontics, Dental School, Faculty of Medicine, the University of Prishtina in Kosovo. After fitting the new complete dentures, all patients were tested for mBF at the intercuspal position. Patients were followed for 6 months. During this period, stabilisation of complete dentures was expected. During the observation period, each subject was measured six times within six months. The first measurement was performed one week after the fitting of the complete dentures, and successive recalls at 2 to 5 weeks, 3 to 10 weeks, 4 to 15 weeks, 5 to 10 weeks and 6 to 25 weeks.
During measurements, patients were invited to sit on a chair in a quiet room so that the Frankfurter plane was approximately horizontal. This test included recordings of the mBF at the intercuspal position between the first molars for 3 seconds with a piezoelectric gnathodynamometer. The procedure was repeated 3 times in identical conditions, with relaxation intervals of 1 minute between repeats and the limiting factor was the subjective feeling of pain.
During each measurement of one side of the jaw, to stabilise the complete dentures during the test, the rubber cylinder was applied on the contralateral side at the first molar region, with 75% hardness according to Shore with the same width as the Gnathodynamometer probe (6 mm). The piezoelectric gnathodynamometer was directly connected to a Dyno Figure printer. In this way, apart from the numerical values of the bite forces, Figural data were recorded as well. In the Figural data, the mBF was represented by a basic line of deflection. For the evaluation of the results, the highest expressed value of mBF was recorded. The jaw side, showing greater mBF during measurement was referred as the dominant side (DS), while the opposite as the non-dominant side (NDS).
Statistical analysis was performed using standard software package BMSP (BioMedical Statistical Package), dedicated to research in the biomedical sciences, which included all methods of statistical procedures, (Dixon, 62.). Testing of parametric data was done with One Way Repeated Measurement of ANOVA test.
Results
The basic parameters of bite forces at defined time intervals (N) were presented in tabulated and Figural forms. It can be concluded that the average values increased during the observational period, both on the DS and NDS. Higher values were recorded for the DS with a significant statistical difference. The analysis of one - factor variance showed that there were differences in average values between DS and NDS for the six measurements (mBF - DS = 11.3, p = 0.0001, and mBF - NDS = 2.26, p = 0.047). This indicator showed that on both sides the initial value of mBF changed over time (Table 1, Figure 1).
Table 1.
Basic parameters of Maximum Bite Force (mBF) in Set Time Intervals on Dominant (DS) and Non - Dominant Sides (NDS) of the sample (N)
| Maximum Bite Force (mBF) Dominant Side (DS) | Maximum Bite Force (mBF) Non-Dominant Side (NDS) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Measur. | 1 | 2 | 3 | 4 | 5 | 6 | 1 | 2 | 3 | 4 | 5 | 6 |
| N | 88 | 88 | 88 | 87 | 88 | 88 | 88 | 88 | 88 | 87 | 88 | 88 |
| X | 138 | 178 | 200 | 208 | 211 | 202 | 102 | 111 | 121 | 119 | 127 | 126 |
| Xmin | 24 | 48 | 64 | 40 | 52 | 60 | 24 | 30 | 34 | 30 | 40 | 44 |
| Xmax | 348 | 392 | 412 | 526 | 416 | 448 | 312 | 290 | 300 | 356 | 320 | 360 |
| DS | 90.1 | 74.3 | 74.8 | 83.9 | 75.7 | 73.2 | 3.5 | 54.2 | 55.0 | 55.7 | 54.2 | 50.8 |
| GS | 9.6 | 7.9 | 8.0 | 9.0 | 8.1 | 7.8 | 6.8 | 5.8 | 5.9 | 6.0 | 5.8 | 5.4 |
Figure 1.
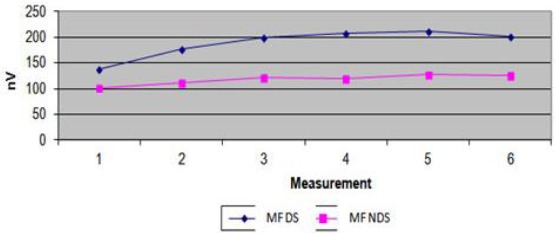
Masticatory Force in Set Time Interval (STI)
By analysing two variance factors (Gender and Time [of mesurement]), the influence of masticatory forces on DS and NDS were investigated. The resulting masticatory forces, for both sides, were influenced by the same factors, with significant difference (Table 2, Figure 2).
Table 2.
Maximum Bite Force (mBF) in six Set Time Intervals (STI) in Females (F) and Males (M) on Dominant (DS) and Non -Dominant Sides (NDS)
| Sex | Meas | Masticatory Force (mBF) | Masticatory Force (mBF) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Dominant Side (DS) | Non-Dominant Side (NDS) | ||||||||||||
| F | N | 42 | 42 | 42 | 42 | 42 | 42 | 42 | 42 | 42 | 42 | 42 | 42 |
| X | 61 | 133 | 156 | 153 | 162 | 170 | 53 | 84 | 85 | 88 | 95 | 101 | |
| Min | 24 | 48 | 64 | 40 | 52 | 60 | 24 | 30 | 34 | 30 | 40 | 44 | |
| Max | 100 | 202 | 270 | 282 | 290 | 288 | 100 | 160 | 150 | 140 | 160 | 150 | |
| DS | 16.9 | 40.7 | 44.7 | 57 | 54.2 | 51.9 | 17.7 | 28.9 | 25.2 | 27.4 | 26.7 | 25.4 | |
| GS | 2.6 | 6.3 | 6.9 | 8..8 | 2.7 | 4.4 | 3.9 | 4.2 | 4.1 | 3.9 | 3.2 | 3.0 | |
| M | N | 46 | 46 | 46 | 46 | 46 | 46 | 46 | 46 | 46 | 46 | 46 | 46 |
| X | 207 | 219 | 240 | 247 | 249 | 249 | 147 | 150 | 153 | 148 | 155 | 149 | |
| Min | 84 | 80 | 108 | 128 | 120 | 122 | 66 | 76 | 80 | 90 | 76 | 80 | |
| Max | 348 | 392 | 412 | 416 | 416 | 448 | 312 | 290 | 300 | 356 | 321 | 360 | |
| DS | 70.3 | 74.8 | 79.7 | 68.4 | 69.7 | 55.8 | 53.3 | 55.1 | 59.7 | 57.3 | 57.0 | 57.4 | |
| GS | 10.4 | 11.0 | 11.0 | 11.9 | 10.1 | 10.3 | 8.2 | 7.9 | 8.1 | 8.9 | 8.4 | 8.4 | |
Figure 2.
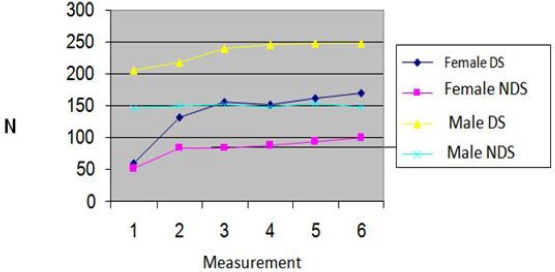
mBF at STI by Gender
Gender: mBF - DS (gender) = 318.43, p=0.0000; mBF - NDS (gender) = 219.89, p = 0.0000. Time: mBF - DS (time) = 18.74, p = 0.0000; BF - NDS (time) = 3.83, p = 0.0020. Interaction: mBF - DS (inter) = 3.68, p = 0.0208, BF- NDS (inter) = 2.7, p = 0.201.
Significant differences in the masticatory forces on DS and NDS is explained by different measurement times and with the prior experience wearing complete dentures. However, the interaction of these two factors had a significant impact on the variations in the masticatory force (Table 3, Figure 3).
Table 3.
Maximum Bite Force (mBF) in six Set Time Intervals (STI) in Experienced Complete Denture Wearers (eCDW) and Inexperienced Complete Denture Wearers (iCDW) on Dominant (DS) and Non - Dominant Sides (NDS)
| mBF (DS) | mBF (NDS) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Msr | 1 | 2 | 3 | 4 | 5 | 6 | 1 | 2 | 3 | 4 | 5 | 6 | |
| iCDW | N | 45 | 45 | 45 | 44 | 45 | 45 | 45 | 45 | 45 | 44 | 45 | 45 |
| X | 155 | 194 | 221 | 229 | 230 | 232 | 118 | 132 | 136 | 131 | 143 | 140 | |
| Min | 30 | 58 | 78 | 50 | 64 | 74 | 28 | 38 | 42 | 36 | 50 | 54 | |
| Max | 348 | 392 | 412 | 416 | 416 | 448 | 312 | 290 | 300 | 356 | 320 | 360 | |
| DS | 96.9 | 82.5 | 80.2 | 88.1 | 77.6 | 77.1 | 69.3 | 56.8 | 60.0 | 63.1 | 61.2 | 60.5 | |
| ES | 14.4 | 12.3 | 11.9 | 13.3 | 11.6 | 11.5 | 10.3 | 8.5 | 8.9 | 9.5 | 9.1 | 9.0 | |
| eCDW | N | 43 | 43 | 43 | 43 | 43 | 43 | 43 | 43 | 43 | 43 | 43 | 43 |
| X | 119 | 162 | 178 | 175 | 184 | 189 | 86 | 104 | 104 | 107 | 110 | 112 | |
| Min | 24 | 48 | 64 | 40 | 52 | 60 | 24 | 30 | 34 | 30 | 40 | 44 | |
| Max | 278 | 302 | 320 | 338 | 324 | 334 | 218 | 248 | 216 | 232 | 218 | 196 | |
| DS | 79.3 | 61.3 | 62.3 | 70.3 | 66.6 | 62.6 | 52.7 | 47.9 | 44.1 | 44.3 | 39.9 | 33.1 | |
| ES | 12.1 | 9.4 | 9.5 | 10.7 | 10.2 | 9.6 | 8.0 | 7.3 | 6.7 | 6.8 | 6.1 | 5.0 | |
Figure 3.
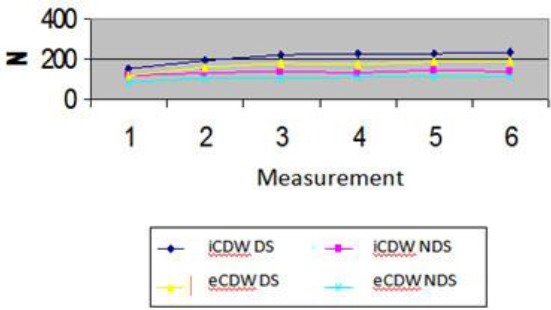
mBF at STI by Experienced and Inexperienced Complete Denture
Time: mBF - DS (time) = 11.76, p = 0.0000; mBF - NDS (time) = 2.42, p = 0.0351; mBF - DS (experience) = 40.48; P = 0.0000; mBF - NDS (experience) = 39.93, p = 0.0000; Interaction: mBF - DS (inter) = 0.22, p = 0.9533; mBF - NDS (inter) = 0.09, p = 0.9941
The measurement time refers to the increase in average values of the masticatory forces in relation to the initial values and since the interaction was insignificant, this means that the same or approximate increase of masticatory forces occurs in eCDW and iCDW.
Experienced Complete Denture Wearers (eCDW) sooner reach the stationary state than Inexperienced Denture Wearers (iCDW) that reach it at their third measurement. The decrease of the values of the masticatory forces in CDW is explained by the fact that the patients lack their natural teeth. Patient age seems to be the cause of the reduction of masticatory forces.
Discussion
For over a century, conventional dentures were the sole treatment option for compromised dentitions. However, the rehabilitation of these patients using conventional dentures, regardless the quality, failed to completely solve either functional or psychological problem [13].
Most authors agree that the mBF increases significantly with newly fit complete dentures. However, the period towards reaching stationary state varies greatly. The results of this study indicate that after fitting of complete dentures the stationary state is reached after the 15th week, and it remains the same until the end of the observation period. Our results support previous findings which state that this period is between 12 and 24 months [14]. A stationary state is influenced by internal factors (fitness, the degree of reduction of the mucosal base, soft tissue condition, the presence of dysfunction) and external factors (related to prosthetic treatment). Niwatcharoenchaikul et al. concluded that complete dentures with bilateral balanced occlusion had no significant difference between masticatory performance and move [15].
Various authors (1944) concluded that people prefer unilateral mastication lean towards lateralisation of bite forces. Thus, in these patients, the masticatory force is higher on the preferred side versus the opposing side of the jaw [16] [17] [18] Some authors failed to observe the latter phenomenon [19], nevertheless it has been verified that people with full intact dental arches present with both Ds and NDS, as was also the case with our paper. This fact indicates that there is a preferred side in the functional sense even though the individual is unaware of it. Based on these findings it may be concluded that in the region of the first molar (centre of mastication), in CDW, the bite forces and the duration of the functional loads are greater on the DS versus the NDS. The speed of achievement of masticatory balance in DS and NDS varies. Bite forces in the DS reach the stationary state at the third measurement with no significant changes by the end of the measurements.
Gender does influence the variations in the dynamics of biting. Average values of masticatory forces are lower in females than males. At the time of measurement, there is a difference in the masticatory forces compared to initial values, followed by the stationary state. The influence of combined factors (interaction) is a more pronounced interval between initial and stationary ranges (DS = 109N, NDS = 48N) in females, while in males this change is less pronounced (DS = 42N, NDS = 38N). Probably, males respond faster to newly fit complete dentures regarding functional adaptation compared to females. This is consistent with the previous findings, which revealed a significant difference in gender. Higher mBF in males may be attributed to the larger size of their teeth and the greater muscular potential, therefore anatomical features may come in play. Larger teeth have larger periodontal ligament areas yielding greater biting forces [20] [21] [22]. In contrast, Wichelhaus et al. [23] have found no significant difference in mBF between males and females. Most studies have confirmed the differences of mBF values between males and females [20] [24] [25]. In the dynamics of maximum bite forces during observation period, a significant impact was experienced by CDWs. The results of this research have shown that eCDWs have higher initial values of maximum bite force (~ 40 N), and they consequently have better functional adaptation versus new CDWs. Over time, eCDWs have developed regulatory control mechanisms (memory paradigm of previous experience) which are used to compare e test new complete dentures. This minimizes the inhibitory impact of psychological factors and ensures imminent acceptance of complete dentures. Conversely, iCDWs are more cautious during neuromuscular adaptation period, although at the end of the observational period they have higher mBF. Dentists tend to believe that eCDWs, if positive, may readily adapt to new dentures; if negative, may poorly respond to adaptation. Furthermore, duration of denture use was associated with higher satisfaction rates [26].
Rehabilitation of edentulous patients with implant supported dentures is a very invasive and expensive long treatment option [27]. However, the biting forces and masticatory performance increased probably due to improved denture retention and stability [28]. Measurement of bite force has been a reliable method for assessment of the biomechanical properties of the masticatory system and prosthetic treatment. However, one should consider other effective factors when comparing bite force measurement in research [29]. The role of Prosthodontists is to have an understanding of the changes in the orofacial form, function and behavioural consequences and the possible social impact emerging from the complete loss of teeth [30].
Maximum bite force (mBF) represents a significant discriminating variable of the functional adaptation level to new complete dentures. The highest value of this variable is featured by the longer time intervals of function about the initial measurements and is the indicator of better adaptation to the new complete dentures. The region of the centre of occlusion on the DS has greater potential regarding transferring maximum physiological loads relative to the homologous part of the NDS. For the dynamics of this indicator, the progressive increase of values about the initial values with a tendency of restoring the stationary condition after the seventh week of delivery of the new complete dentures is remarkable.
Footnotes
Funding: This research did not receive any financial support
Competing Interests: The authors have declared that no competing interests exist
References
- 1.Soboleva U, Laurina L, Slaidina A. The masticatory system-an overview. Stomatologija Baltic Dental and Maxillofacial Journal. 2005;7:77–80. PMid:16340271. [PubMed] [Google Scholar]
- 2.Zmudzki J, Chladek G, et al. The stimulation of mastication efficiency mucous-borne complete dentures. Achievements in Materials and Engineering. 2013;63:75–86. [Google Scholar]
- 3.Divaris K, Ntounis A, Marinis A, Polyzois G, Polychronopoulou A. Loss of natural dentition: multi-level effects among a geriatric population. Gerodontology. 2012;29:e192–9. doi: 10.1111/j.1741-2358.2010.00440.x. https://doi.org/10.1111/j.1741-2358.2010.00440.x. PMid:21083739. [DOI] [PubMed] [Google Scholar]
- 4.Fontijn-Tekamp FA, Slagter AP, Der Bilt A, et al. Biting and chewing in overdentures, full dentures, and natural dentitions. J Dent Res. 2000;79:1519–1524. doi: 10.1177/00220345000790071501. https://doi.org/10.1177/00220345000790071501. PMid:11005738. [DOI] [PubMed] [Google Scholar]
- 5.Gunne JB, Benbom L, Hogstrem J. Masticatory eficiency of complete denture patients. Acta Odontol Scand. 1992;40:289–297. doi: 10.3109/00016358209024072. [DOI] [PubMed] [Google Scholar]
- 6.Howell AH, Brudevold F. Vertical forces used during chewing of food. J Dent Res. 1950;29:133–136. doi: 10.1177/00220345500290020401. https://doi.org/10.1177/00220345500290020401. PMid:15415485. [DOI] [PubMed] [Google Scholar]
- 7.Mancuso D, Goiato M, Filho H, Gomes E. Bite force and masticatory efficiency in implant-retained dentures. Dentalcetoday magazine. 2009;104:1–6. [PubMed] [Google Scholar]
- 8.Hickey JC, Kleider JA, Boucher CO, Stroz O. A method of styding the influence of occlusal schemes on muscuylar actvity. J Pros Dent. 1989;9:498–506. https://doi.org/10.1016/0022-3913(59)90082-4. [Google Scholar]
- 9.Fontijn-Tekamp FA, Slagter AP, van’t Hof MA, Geertman ME, Kalk W. Bite forces with mandibular implant-retained overdentures. J Dent Res. 1998;77:1832–1839. doi: 10.1177/00220345980770101101. https://doi.org/10.1177/00220345980770101101. PMid:9786640. [DOI] [PubMed] [Google Scholar]
- 10.De Boever J. Experimental occlusal balancing-contact interference and muscle activity. Paradontologie. 1989;23:59–63. [PubMed] [Google Scholar]
- 11.Pereira LJ, Gavião MB, Bonjardim LR, Castelo PM, Andrade Ada S. UltrasonoFigurey and electromyoFigurey of masticatory muscles in a group of adolescents with signs and symptoms of TMD. Journal of Clinical Pediatric Dentistry. 2006;30:314–319. doi: 10.17796/jcpd.30.4.w2t51jh08762648g. https://doi.org/10.17796/jcpd.30.4.w2t51jh08762648g. PMid:16937858. [DOI] [PubMed] [Google Scholar]
- 12.Bakke M, Holm B, Gotfredsen K. Masticatory function and patient satisfaction with implant-supported mandibular overdentures: a prospective 5-year study. Int J Prosthodont. 2002;15:575–581. PMid:12475165. [PubMed] [Google Scholar]
- 13.Pocztaruk RL, Frasca LC, Rivaldo EG, Fernandes Ede L, Mattia PR, Vidal RA, et al. Satisfaction level and masticatory capacity in edentulous patients with conventional dentures and implant-retained overdentures. Braz J Oral Sci. 2006;5:1232–38. [Google Scholar]
- 14.Atkinson HF, Ralph WJ. Tooth loss and biting force in man. J Dent Res. 1973;52:225–228. doi: 10.1177/00220345730520020701. https://doi.org/10.1177/00220345730520020701. PMid:4511303. [DOI] [PubMed] [Google Scholar]
- 15.Niwatcharoenchaikul W, Tumrasvin W, Arksornnukit M. Effect of complete denture occlusal schemes on masticatory performance and maximum occlusal force. J Prosthet Dent. 2014;112(6):1337–42. doi: 10.1016/j.prosdent.2014.06.003. https://doi.org/10.1016/j.prosdent.2014.06.003. PMid:25062582. [DOI] [PubMed] [Google Scholar]
- 16.Carlsson GE, Ericson S. Postural face height in full dentures wearers. Acta Odont Scand. 1967;25:145–162. doi: 10.3109/00016356709028744. https://doi.org/10.3109/00016356709028744. PMid:5233922. [DOI] [PubMed] [Google Scholar]
- 17.Worner HK. Gnathodynamics, the Measurment of Biting Forcës with a New Design of Gnathodynamometer. Aust Dent J. 1939;43:381–388. [Google Scholar]
- 18.Andersson DJ. Measurment of stress in mastication I. J Dent Res. 1986;26:21–29. [Google Scholar]
- 19.Helkimo E. Bite force and state of dentition. Acta Odontol Scand. 1003;35:297–303. doi: 10.3109/00016357709064128. https://doi.org/10.3109/00016357709064128. [DOI] [PubMed] [Google Scholar]
- 20.Ferrario VF, Sforza C, Serrao G, Dellavia C, Tartagilia GM. Single tooth bite forces in healthy young adults. J Oral Rehabil. 2004;31:18–22. doi: 10.1046/j.0305-182x.2003.01179.x. https://doi.org/10.1046/j.0305-182X.2003.01179.x. PMid:15125591. [DOI] [PubMed] [Google Scholar]
- 21.Bonakdarchian M, Askari N, Askari M. Effect of face form on maximal molar bite force with natural dentition. Arch Oral Biol. 2009;54:201–204. doi: 10.1016/j.archoralbio.2008.11.009. https://doi.org/10.1016/j.archoralbio.2008.11.009. PMid:19131047. [DOI] [PubMed] [Google Scholar]
- 22.Olthoff LW, Van Der Glas W, Van Der Blit A. Influence of occlusal vertical dimension on the masticatory performance during chewing with maxillary splints. J Oral Rehabil. 2007;34:560–565. doi: 10.1111/j.1365-2842.2007.01730.x. https://doi.org/10.1111/j.1365-2842.2007.01730.x. PMid:17650165. [DOI] [PubMed] [Google Scholar]
- 23.Wichelhaus A, Hüffmeier S, Sander FG. Dynamic functional force measurements on an anterior bite plane during the night. J Orofac Orthop. 2003;64:417–425. doi: 10.1007/s00056-003-0316-5. https://doi.org/10.1007/s00056-003-0316-5. PMid:14628133. [DOI] [PubMed] [Google Scholar]
- 24.Shinogaya T, Bakke M, Thomsen CE, Vilmann A, Sodeya-ma A, Matsumoto M. Effects of ethnicity, gender and age on clenching force and load distribution. Clin Oral Invest. 2001;5:63–68. doi: 10.1007/s007840000099. https://doi.org/10.1007/s007840000099. [DOI] [PubMed] [Google Scholar]
- 25.Waltimo A, Könönen M. A novel bite force recorder and maximal isometric bite force values for healthy young adults. Scand J Dent Res. 1993;101:171–175. doi: 10.1111/j.1600-0722.1993.tb01658.x. https://doi.org/10.1111/j.1600-0722.1993.tb01658.x. [DOI] [PubMed] [Google Scholar]
- 26.Turker SB, Sener ID, Ozkan YK. Satisfaction of the complete denture wearers related to various factors. Arch Gerontol Geriatr. 2009;49(2):e126–9. doi: 10.1016/j.archger.2008.11.003. https://doi.org/10.1016/j.archger.2008.11.003. PMid:19117618. [DOI] [PubMed] [Google Scholar]
- 27.Gallucci GO, Bernard JP, Belser UC. Treatment of completely edentulous patients with fixed implant-supported restorations: three consecutive cases of simultaneous immediate loading in both maxilla and mandible. The International Journal of Periodontics & Restorative Dentistry. 2005;25:27–37. [PubMed] [Google Scholar]
- 28.Caloss R, Al-Arab M, Finn RA, Lonergan O, Throckmorton GS. Does long-term use of unstable dentures weaken jaw muscles? Journal of Oral Rehabilitation. 2010;37:256–261. doi: 10.1111/j.1365-2842.2009.02046.x. https://doi.org/10.1111/j.1365-2842.2009.02046.x. PMid:20050986. [DOI] [PubMed] [Google Scholar]
- 29.Koc D, Dogan A, Bek B. Bite force and influential factors on bite force measurements: a literature review. Eur J Dent. 2010;4(2):223–32. PMid:20396457. PMCid:PMC2853825. [PMC free article] [PubMed] [Google Scholar]
- 30.Kumar L. Biomechanics and clinical implications of complete edentulous state. Journal of Clinical Gerontology &Geriatrics. 2014;5:101–104. https://doi.org/10.1016/j.jcgg.2014.03.001. [Google Scholar]