

Portal vein thrombosis (PVT) in cirrhosis is a relatively frequent complication with a 5-year cumulative incidence of 10.7%[1] to 20%.[2] In contrast to non-cirrhotic PVT, which is almost always caused by a thrombophilic factor, cirrhotic PVT is related to a decelerated blood flow through the portal vein and the presence of a thrombophilic factor is an exception.[1,3,4,5] In addition, advanced disease and large varices with a high flow are related to PVT.[1,2] The varices may further reduce the portal vein flow velocity and cause turbulent flow at the junction with the portal or splenic vein.
The clinical manifestation of cirrhotic PVT is often mild or lacking. In many patients, clinical symptoms are missing and diagnosis of PVT is set up by chance during regular outpatient visits for HCC screening.[1] A study including 79 patients demonstrated that PVT was asymptomatic in 43% of patients, 39% presented with variceal bleeding and only 18% had acute abdominal pain due to intestinal ischemia or infarction.[6] The high incidence of variceal bleeding may not be due to PVT but rather be a coincidental manifestation of the two interrelated phenomena, PVT and varices. As shown in a large, longitudinal French study including 1,243 patients, PVT developed in 118 patients and was associated neither with progression of the liver disease nor with survival.[1] These findings seem to conflict with those of a previous Italian study demonstrating that prevention of PVT by enoxaparin reduced decompensation of the liver disease, and improved survival.[7] However, the effect of enoxaparin on disease progression was much more marked than on prevention of PVT. suggesting a complex action of the drug on coagulation factors, platelets and fibrinogenesis.[1,7]
The mild clinical manifestation of PVT may be explained by the dual blood supply of the liver, where either the hepatic artery or the portal vein provides sufficient oxygen and nutrition to the hepatocytes. In case of reduced portal vein flow, a mechanism termed “the hepatic-arterial buffer response” augments the arterial blood flow to maintain liver perfusion and function.[8] With respect to portal hypertension, PVT may have little effect since it only terminates the gradual increase in portal pressure and decrease in blood flow. Thus, the development of PVT did not correlate with ascitesor variceal bleeding.[1] Extrahepatic PVT may even reduce the sinusoidal pressure and diminish the filtration pressure across the liver capsule. As for non-cirrhotic PVT where ascites is exceptionally rare, patients with cirrhosis may also be capable to drain the possibly higher mesenteric filtrate into the lymphatic system, which is not compromised by the liver disease.[9]
The morphology of PVT differs from patient to patient. PVT may appear as partial or complete/occlusive, limited or extended and it may involve the extrahepatic portal system or the intrahepatic portal branches in isolation or in combination (Figure 1–4). The great variance of thrombosis may be the result of variable flow patterns in the portal vein, portal tributaries and collaterals. For example, a large collateral flow may prevent thrombus formation in peripheral branches but induce thrombosis of the main stem of the portal vein (Figure 1). On the other hand, a critical portal flow velocity may cause lining thrombosis of the main stem of the portal vein. The narrowing of the vascular bed may then accelerate the blood flow limiting further thrombus formation and maintaining some degree of patency (Figure 2). Intrahepatic PVT may be a result of stagnant or reversed intrahepatic blood flow. It may, however, also be due to thrombus migration from an extrahepatic source thatmay still be detectable or resolved (Figure 2). The lack of collaterals or their presence may inform about the age of the thrombus (Figure 3, 4). It can be assumed that detailed information such as given in Figure 1–4 can only be obtained by direct angiography. Neither computed tomography (CT), nor magnetic resonance imaging (MRI) or duplex sonography is capable to provide the exact information of thrombus extension and grade of occlusion. This may particularly be true for intrahepatic thrombosis and for the determination of thrombus age.
Figure 1.
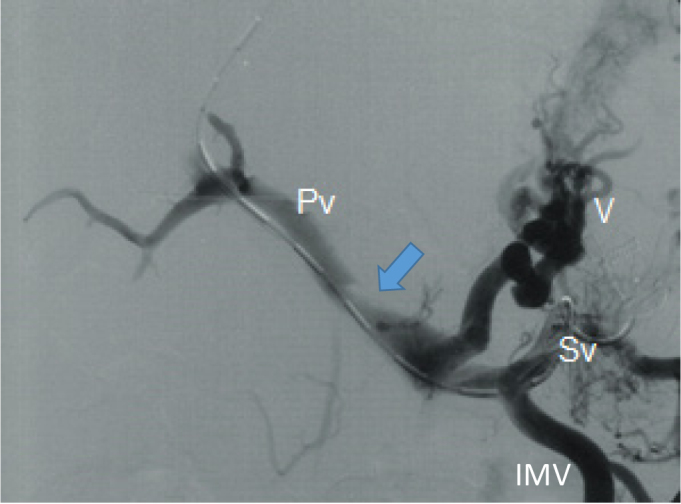
Partial portal vein thrombosis (arrow) in the presence of hugh varices (V) and retrograde flow in the splenic (Sv) and inferior mesenteric (IMV) veins
Figure 4.
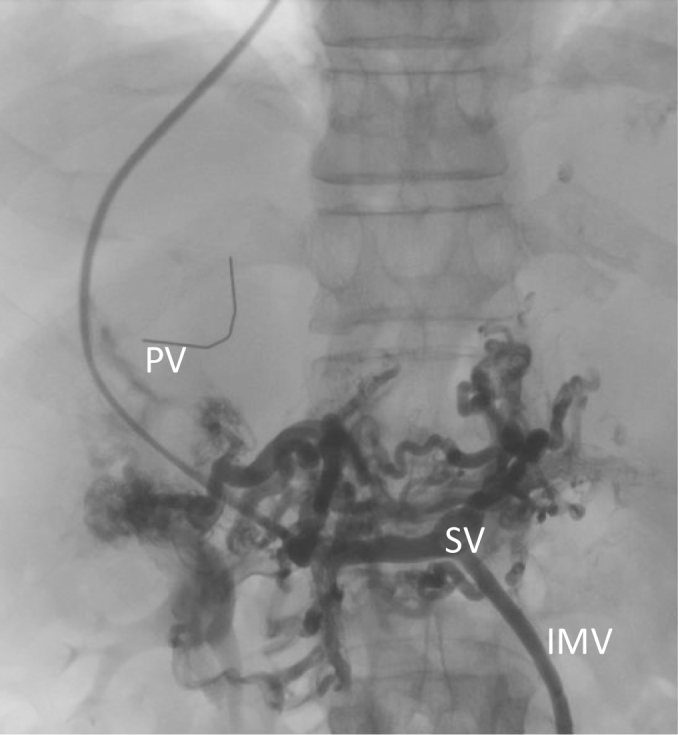
Complete chronic thrombosis of the portal trunc with collaterals and cavernoma. PV: occluded trunc of portal vein with catrheter, SV: splenic vein, IMV: inferior mesenteric vein
Figure 2.
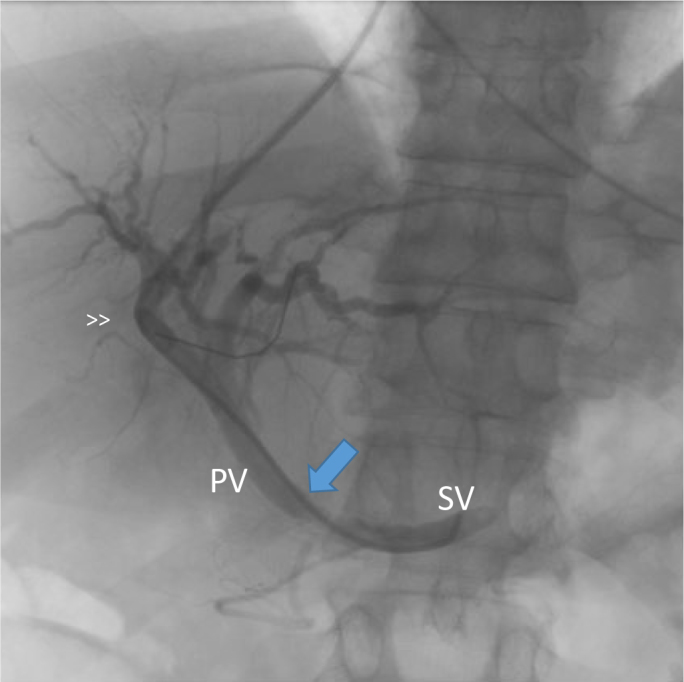
Lining thrombosis of the portal vein with a diameter of 5 mm. A right intrahepatic branch may be embolized (>>). This changes have not been detected by a CT-scan performed 3 days prior to the transjugular intervention. PV: portal vein, SV: splenic vein.
Figure 3.
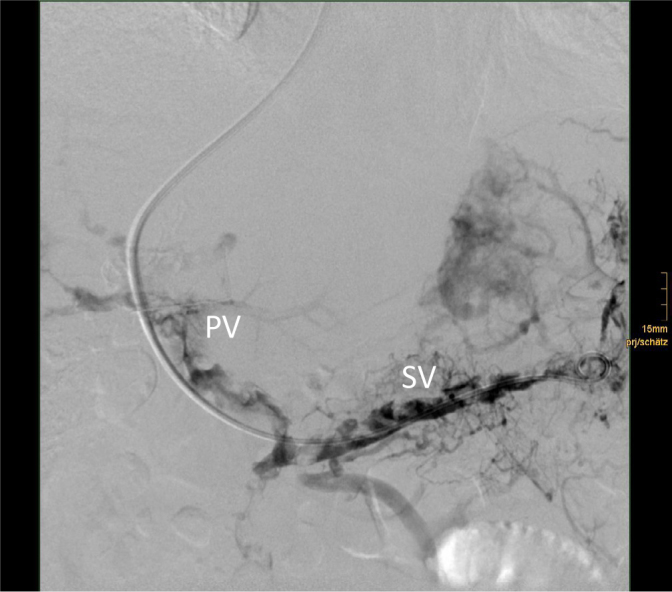
Complete and extended recent thrombosis without collateral formation. PV: occluded portal vein, SV: thrombosed splenic vein.
The indication of treatment of non-malignant PVT in cirrhosis is still under debate. Interventional treatment can be performed via a transjugular, percutaneous transhepatic or transsplenic access. Studies using a transjugular access to the thrombus together with the implantation of a transjugular intrahepatic portosystemic shunt (TIPS) are summarized in Table 1. They included variable proportions of patients with partial or complete thrombosis and patients with or without cavernoma. Treatment was effective in 65% to 100% of patients with complete resolution of the thrombus in 33–100%. Treatment success depended on the grade (partial/complete) and the age of the thrombosis. The age of the thrombosis was defined by imaging as acute (no collaterals, visible thrombus), chronic (collaterals) or cavernoma. Most of the patients included had chronic thrombosis. With 2 exceptions, the studies did not specify the exact interval between thrombus formation/diagnosis and treatment. These 2 studies included patients with intervals between the diagnosis of the thrombosis and treatment of a mean of 4.7 (0–66) months[10] and 5.5 (0.5–24) months.[11] In patients with a fibrotic cord of the portal vein or with cavernoma, a transsplenic access together with a TIPS may provide successful recanalization.[12] Several studies investigated the effect of anticoagulation with low molecular weight heparin or Vit K antagonists. As summarized in Table 2, anticoagulation is less effective as compared to TIPS and harbors the danger of thrombus progression with mesenteric infarction in almost 20% and thrombus recurrence after treatment cessationin up to 38% of patients.[13] Again, the exact time interval between the development of the thrombus and the treatment is given only in 2 studies with a median of 9 (0–298) days[14] and 40 (0–1,800) days.[15] Treatment was often delayed by varices, which were ligated ahead. Unfortunately, randomized trials comparing treatment with no treatment are still lacking. Therefore, the benefit of treatment on survival remains unclear. However, on the basis of the available cohort studies on the natural course of PVT,[1,2,16] PVT may not impact survival questioning the general indication for treatment, although it is effective. However, in patients in whom the clinical symptoms of portal hypertension dominate the disease, the development of PVT may trigger the decision for TIPS treatment if suitable (bilirubin < 3 mg/dL, hepatic encephalopathy < Grade 1). Second, in candidates for liver transplantation, PVT should be prevented or treated in any case since PVT negatively affects survival after transplantation.[17,18,19] This can be achieved by long-term anticoagulation or TIPS implantation.[20,21]
Table 1.
TIPS treatment for portal vein thrombosis in patients with cirrhosis
| Author, year, (Ref.) | Number of patients, study design | Age of thrombosis | Grade of PVT partial/occlusive/cavernoma** (n) | Resolution of PVT partial/complete/any (%) |
|---|---|---|---|---|
| Van Ha, 2006[22] | 15, retrospective | Acute 11 Chronic 4 | 7/8/4 | n.d.∗/n.d.*/77 |
| Bauer, 2006[23] | 9, retrospective | Chronic 9 | 0/9/4 | 11/56/67 |
| Senzolo, 2006[11] | 13, retrospective | 5.5 months (0.5–24) | 5/8/3 | n.d.* |
| Perarnau, 2010[24] | 123, retrospective | Acute 15 Chronic 108 | 94/29/14 | n.d.* |
| Han, 2011[25] | 57, retrospective | Acute 0 Chronic 57 | 35/22/30 | n.d.*/n.d.*/100*** |
| Luca, 2011[10] | 70, prospective | 4.7 months (0–66) | 46/24/2 | 30/57/87 |
| Senzolo, 2012[13] | 7, prospective | n.d.* | n.d.* | 67/33/100*** |
| Avola, 2012[20] | 15, retrospective | Chronic 15 | 15/0/0 | 0/100/100 |
| Salem, 2015[12] | 44, retrospective | Chronic 44 | 0/44/13 | 16/74/90 |
| Luo, 2015[26]§ | 37, prospective | Chronic 37 | 24/13/0 | 13/52/65 |
| Zhao, 2016[27] | 191, retrospective | n.d.* | 143/48/? | 31/69/100*** |
| Lv, 2017[28] | 212, retrospective | Acute 17 Chronic 195 | 150/62/47 | n.d.* |
| Lv, 2017[29] § | 24, randomized | Acute 2 Chronic 22 | 16/8/11 | 9/86/95 |
Patients with a cavernoma are a subgroup of patients with occlusive thrombosis;
n.d.: no sufficient data;
Only for patients with successful TIPS intervention;
randomized study, TIPS versus medical treatment (banding ligation and propranolol). All patients received Vit K antagonists. TIPS: transjugular intrahepatic portosystemic shunt; PVT: portal vein thrombosis.
Table 2.
Anticoagulation for portal vein thrombosis in patients with cirrhosis
| Author, year, (Ref) | Number of patients, study design | Age of thrombosis | Grade of PVT partial/occlusive (n) | Resolution of PVT partial/complete/any (%) |
|---|---|---|---|---|
| Francoz, 2005[21] | 19, prospective | n.d.* | 8/11 | 0/42/42 |
| Amitrano, 2010[30] | 28, prospective | n.d.* | 23/5 | 50/33/83 |
| Delgado, 2012[14] | 55, prospective | Acute 31 Chronic 24 median 9 days (0-298) | 41/14 | 15/40/55 |
| Senzolo, 2012[13] | 35, prospective | n.d.* | 24/11 | 27/36/63 |
| Werner, 2013[31] | 28, retrospective | n.d.* | n.d.* | 43/39/82 |
| Naeshiro, 2014[15] | 26, retrospective | 40 days (0-1800) | n.d.* | 62/15/77 |
| Qi, 2015[19] | 430, (16 studies) meta-analysis | n.d.* | n.d.* | 25.1/41.5/66.6 |
PVT: portal vein thrombosis.
n.d.: no sufficient data;
Is timing of the treatment of PVT worth the effort? As discussed above, timing may be impossible, unnecessary, or even useless. It may be impossible because the onset of thrombosis is often obscure due to the mild or lacking clinical manifestation. Timing of treatment would require high frequent clinical visits with possibly only a marginal advantage. It may be unnecessary because both TIPS as well as anticoagulation achieved good results in patients with chronic thrombosis. Finally, timing may be useless, since treatment of PVT may not influence survival. These statements may not be valid for two groups of patients: first, patients with an increased risk of or with existing portal vein thrombosis presenting with severe symptoms of portal hypertension, and second, candidates for liver transplantation. These patients may benefit from early TIPS treatment which prevents and resolves PVT. It should be emphasized that the present knowledge is limited because results of studies are heterogeneous and no randomized studies with no treatment are available.
Footnotes
Conflict of Interests: None declared.
References
- 1.Nery F, Chevret S, Condat B, De Raucourt E, Boudaoud L, Rautou P-E. et al. Causes and consequences of portal vein thrombosis in 1,243 patients with cirrhosis: Results of a longitudinal study. Hepatology. 2015;61:660–7. doi: 10.1002/hep.27546. [DOI] [PubMed] [Google Scholar]
- 2.Maruyama H, Okugawa H, Takahashi M, Yokosuka O.. De novo portal vein thrombosis in virus related cirrhosis: Predictive factors and long-term outcomes. Am J Gastroenterol. 2013;108:568–74. doi: 10.1038/ajg.2012.452. [DOI] [PubMed] [Google Scholar]
- 3.Stine JG, Wang J, Shah PM, Argo CK, Intagliata N, Uflacker A. et al. Decreased portal vein velocity is predictive of the development of portal vein thrombosis: A matched case-control study. Liver Int. 2018;38:94–101. doi: 10.1111/liv.13500. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Chen H, Qi X, He C, Yin Z, Fan D, Han G.. Coagulation imbalance may not contribute to the development of portal vein thrombosis in patients with cirrhosis. Thromb Res. 2013;131:173–77. doi: 10.1016/j.thromres.2012.11.003. [DOI] [PubMed] [Google Scholar]
- 5.Zocco MA, Di Stasio E, De Cristofaro R, Novi M, Ainora ME, Ponziani F. et al. Thrombotic risk factors in patients with liver cirrhosis: Correlation with MELD scoring system and portal vein thrombosis development. J. Hepatol. 2009;51:682–9. doi: 10.1016/j.jhep.2009.03.013. [DOI] [PubMed] [Google Scholar]
- 6.Amitrano L, Guardascione MA, Ames PR, Margaglione M, Antinolfi I, Iannaccone L. et al. Risk factors and clinical presentation of portal vein thrombosis in patients with liver cirrhosis. Am J Hematol. 2003;72:75–81. [Google Scholar]
- 7.Villa E, Camma C, Marietta M, Luongo M, Critelli R, Colopi S. et al. Enoxaparin prevents portal vein thrombosis and liver decompensation in patients with advanced cirrhosis. Gastroenterology. 2012;143:1253–60. doi: 10.1053/j.gastro.2012.07.018. [DOI] [PubMed] [Google Scholar]
- 8.Gülberg V, Haag K, Rössle M, Gerbes AL.. Hepaticarterialbufferresponse in patients with advanced cirrhosis. Hepatology. 2002;35:630–34. doi: 10.1053/jhep.2002.31722. [DOI] [PubMed] [Google Scholar]
- 9.Levitt DG, Levitt MD.. Quantitative modelling of the physiology of ascites in portal hypertension. BMC Gastroenterology. 2012;12:26. doi: 10.1186/1471-230X-12-26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Luca A, Miraglia R, Caruso S, Milazzo M, Sapere C, Maruzzelli L. et al. Short- and long-term effects of the transjugular intrahepatic portosystemic shunt on portal vein thrombosis in patients with cirrhosis. Gut. 2011;60:846–52. doi: 10.1136/gut.2010.228023. [DOI] [PubMed] [Google Scholar]
- 11.Senzolo M, Tibbals J, Cholongitas E, Triantos CK, Burroughs AK, Patch D.. Transjugular intrahepatic portosystemic shunt for portal vein thrombosis with and without cavernous transformation. Aliment Pharmacol Ther. 2006;23:767–75. doi: 10.1111/j.1365-2036.2006.02820.x. [DOI] [PubMed] [Google Scholar]
- 12.Thornburg B, Desai K, Hickey R, Hohlastos E, Kulik L, Ganger D. et al. Pretransplantation Portal Vein Recanalization and Transjugular Intrahepatic Portosystemic Shunt Creation for Chronic Portal VeinThrombosis: Final Analysis of a 61-Patient Cohort. J Vasc Interv Radiol. 2017;28:1714–21. doi: 10.1016/j.jvir.2017.08.005. [DOI] [PubMed] [Google Scholar]
- 13.Senzolo MM, Sartori T, Rossetto V, Burra P, Cillo U, Boccagni P. et al. Prospective evaluation of anticoagulation and transjugular intrahepatic portosystemic shunt for the management of portal vein thrombosis in cirrhosis. Liver int. 2012;32:919–27. doi: 10.1111/j.1478-3231.2012.02785.x. [DOI] [PubMed] [Google Scholar]
- 14.Delgado MG, Seijo S, Yepes I, Achécar L, Catalina MV, García-Criado A. et al. Efficacy and safety of anticoagulation on patients with cirrhosis and portal vein thrombosis. Clin Gastroenterol Hepatol. 2012;10:776–83. doi: 10.1016/j.cgh.2012.01.012. [DOI] [PubMed] [Google Scholar]
- 15.Naeshiro N, Aikata H, Hyogo H, Kan H, Fujino H, Kobayashi T. et al. Efficacy and safety of the anticoagulant drug, danaparoid sodium, in the treatment of portal vein thrombosis in patients with liver cirrhosis. Hepatol Res. 2015;45:656–62. doi: 10.1111/hepr.12400. [DOI] [PubMed] [Google Scholar]
- 16.Luca A, Caruso S, Milazzo M, Marrone G, Mamone G, Crino F. et al. Natural course of extrahepatic non-malignant partial portal vein thrombosis in patients with cirrhosis. Radiology. 2012;265:124–32. doi: 10.1148/radiol.12112236. [DOI] [PubMed] [Google Scholar]
- 17.Montenovo M, Rahnemai-Azar A, Reyes J, Perkins J.. Clinical impact and risk factors of portal vein thrombosis for patients on wait list for liver transplant. Experimental and Clinical Transplantation. 2017 doi: 10.6002/ect.2016.0277. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 18.Francos C, Valla D, Durand F.. Portal vein thrombosis, cirrhosis, and liver transplantation. J Hepatol. 2012;57:203–12. doi: 10.1016/j.jhep.2011.12.034. [DOI] [PubMed] [Google Scholar]
- 19.Qi X, Dai J, Jia J, Ren W, Yang M, Li H. et al. Association between portal vein thrombosis and survival of liver transplant recipients: A systematic review and meta-analysis of observational studies. J Gastrointestin Liver Dis. 2015;24:51–9. doi: 10.15403/jgld.2014.1121.qix. [DOI] [PubMed] [Google Scholar]
- 20.D'Avola D, Bilbao JI, Zozaya G, Pardo F, Rotellar F, Inarrairaegui M. et al. Efficacy of transjugular intrahepatic portosystemic shunt to prevent total portal vein thrombosis in cirrhotic patients awaiting for liver transplantation. Transplantation Proceedings. 2012;44:2603–5. doi: 10.1016/j.transproceed.2012.09.050. [DOI] [PubMed] [Google Scholar]
- 21.Francoz C, Belghiti J, Vilgrain V, Sommacale D, Paradis V, Condat B. et al. Splanchnic vein thrombosis in candidates for liver transplantation: usefulness of screening and anticoagulation. Gut. 2005;54:691–97. doi: 10.1136/gut.2004.042796. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Van Ha TG, Hodge J, Funaki B, Lorenz J, Rosenblum J, Straus C. et al. Transjugular intrahepatic portosystemic shunt placement in patients with cirrhosis and concomitant portal vein thrombosis. Cardiovasc Intervent Radiol. 2006;29:785–90. doi: 10.1007/s00270-005-0090-4. [DOI] [PubMed] [Google Scholar]
- 23.Bauer J, Johnson S, Durham J, Ludkowski M, Trotter J, Bak T. et al. The role of TIPS for portal vein patency in liver transplant patients with portal vein thrombosis. Liver Transplantation. 2006;12:1544–51. doi: 10.1002/lt.20869. [DOI] [PubMed] [Google Scholar]
- 24.Perarnau J-M, Baju A, D'alteroche L, Viguier J, Ayoub J.. Feasibility and long-term evolution of TIPS in cirrhotic patients with portal vein thrombosis. Eur J Gastroenterol Hepatol. 2010;22:1093–8. doi: 10.1097/MEG.0b013e328338d995. [DOI] [PubMed] [Google Scholar]
- 25.Han G, Qi X, He C, Yin Z, Wang J, Xia J. et al. Transjugular intrahepatic portosystemic shunt for portal vein thrombosis with symptomatic portal hypertension in liver cirrhosis. J Hepatol. 2011;54:78–88. doi: 10.1016/j.jhep.2010.06.029. [DOI] [PubMed] [Google Scholar]
- 26.Luo X, Wang Z, Tsauo J, Zhou B, Zhang H, Li X.. Advanced cirrhosis combined with portal vein thrombosis: A randomized trial of TIPS versus endoscopic band ligation plus propranolol for the prevention of recurrent esophageal variceal bleeding. Radiology. 2015;276:286–93. doi: 10.1148/radiol.15141252. [DOI] [PubMed] [Google Scholar]
- 27.Zhao M, Yue Z, Zhao H, Wang L, Fan Z, He F. et al. Techniques of TIPS in the treatment of liver cirrhosis combined with incompletely occlusive main portal veinthrombosis. Sci Rep. 2016;6:33069. doi: 10.1038/srep33069. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Lv Y, He C, Wang Z, Guo W, Wang J, Bai W. et al. Association of Nonmalignant Portal Vein Thrombosis and Outcomes after Transjugular Intrahepatic Portosystemic Shunt in Patients with Cirrhosis. Radiology. 2017;285:999–1010. doi: 10.1148/radiol.2017162266. [DOI] [PubMed] [Google Scholar]
- 29.Lv Y, Qi X, He C, Wang Z, Yin Z, Niu J. et al. Covered TIPS versus endoscopic band ligation plus propranolol for the prevention of variceal rebleeding in cirrhotic patients with portal vein thrombosis: a randomised controlled trial. Gut. 2017 Sep 28; doi: 10.1136/gutjnl-2017-314634. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 30.Amitrano L, Guardascione MA, Menchise A, Martino R, Scaglione M, Giovine S. et al. Safety and efficacy of anticoagulation therapy with low molecular weight heparin for portal vein thrombosis in patients with liver cirrhosis. J Clin Gastroenterol. 2010;44:448–51. doi: 10.1097/MCG.0b013e3181b3ab44. [DOI] [PubMed] [Google Scholar]
- 31.Werner KT, Sando S, Carey EJ, Vargas HE, Byrne TJ, Douglas DD. et al. Portal vein thrombosis in patients with end stage liver disease awaiting liver transplantation: Outcome of anticoagulation. Dig Dis Sci. 2013;58:1776–80. doi: 10.1007/s10620-012-2548-y. [DOI] [PubMed] [Google Scholar]