

Abstract
Grid therapy is a treatment technique that has been introduced for patients with advanced bulky tumors. The purpose of this study is to investigate the effect of the radiation sensitivity of the tumors and the design of the grid blocks on the clinical response of grid therapy. The Monte Carlo simulation technique is used to determine the dose distribution through a grid block that was used for a Varian 2100C linear accelerator. From the simulated dose profiles, the therapeutic ratio (TR) and the equivalent uniform dose (EUD) for different types of tumors with respect to their radiation sensitivities were calculated. These calculations were performed using the linear quadratic (LQ) and the Hug‐Kellerer (H‐K) models. The results of these calculations have been validated by comparison with the clinical responses of 232 patients from different publications, who were treated with grid therapy. These published results for different tumor types were used to examine the correlation between tumor radiosensitivity and the clinical response of grid therapy. Moreover, the influence of grid design on their clinical responses was investigated by using Monte Carlo simulations of grid blocks with different hole diameters and different center‐to‐center spacing. The results of the theoretical models and clinical data indicated higher clinical responses for the grid therapy on the patients with more radioresistant tumors. The differences between TR values for radioresistant cells and radiosensitive cells at 20 Gy and 10 Gy doses were up to 50% and 30%, respectively. Interestingly, the differences between the TR values with LQ model and H‐K model were less than 4%. Moreover, the results from the Monte Carlo studies showed that grid blocks with a hole diameters of 1.0 cm and 1.25 cm may lead to about 19% higher TR relative to the grids with hole diameters smaller than 1.0 cm or larger than 1.25 cm (with 95% confidence interval). In summary, the results of this study indicate that grid therapy is more effective for tumors with radioresistant characteristics than radiosensitive tumors.
PACS number(s): 87.55.‐x
Keywords: grid therapy, clinical response, Geant4 simulation, grid block design
I. INTRODUCTION
Local control of bulky tumors with standard radiation therapy is a challenging topic because this treatment will involve a large volume of normal tissues. (1) Spatially fractionated radiation therapy (also known as grid therapy) is a technique that has been introduced for treatment of patients with advanced bulky tumors. (2) In this technique, an open X‐ray field is being converted to a set of pencil beam type radiation fields using an external block. (3) This block is normally made of lead or Cerrobend, and also it could be created using an multileaf collimator (MLC) system in the linear accelerators. (3) Several investigators have reported that this technique has the advantage of a higher potential to repair normal tissues. 4 , 5 , 6 Different kinds of tumors have been treated using this technique and significant tumor responses have been observed without serious toxicities. (7)
Looking at the clinical experiences on the treatment of several hundred patients indicates dramatic effects of this radiotherapy technique on the regression of bulky tumors. Some radiotherapy centers have begun the routine use of spatially fractionated radiotherapy in the management of malignant disease for tumors larger than 6 cm. Despite these promising clinical outcomes, there is a lack of a protocol in the clinical references on selection of appropriate patient or disease for this type of treatment technique. Introduction of a guideline and/or recommendations for selecting the proper tumor type for this treatment technique would be highly beneficial. Furthermore, there is a missing recommendation for the geometrical design of a grid block with appropriate hole size (i.e., diameter) and hole center‐to‐center distances, which could provide an optimum therapeutic result.
In this project, the effectiveness of the grid therapy is being evaluated for tumors with different radiation sensitivities. In addition, the impact of the geometrical design of the grid blocks on their therapeutic ratios (TR) has been investigated. These investigations are based on the Monte Carlo simulations of the dose distribution of the grid fields. The TR values are calculated using linear quadratic (LQ) model, as well as the Hug‐Kellerer (H‐K) model. The integrity of these evaluations has been validated by comparison of the model‐based data with the clinically published values.
II. MATERIALS AND METHODS
Figure 1 shows the flow chart of the process of this project that would be described in details in the following subsections.
Figure 1.
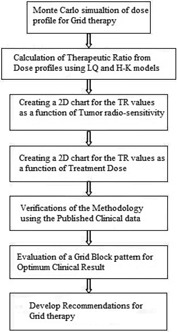
The flow chart of the process of this project.
A. Monte Carlo simulation
In this study, the Geant4 (Version 9.6) Monte Carlo code (8) was used to simulate the photon spectrum of a 6 MV X‐ray beam emitted by a Varian 2100C linear accelerator. The simulations were performed in two steps. First, the accelerator head and the primary collimator were simulated to create the photon spectrum in a phase space (Phs) defined before the jaws (Fig. 2(a)). A total number of 109 events were generated from the initial electron source to collect 50 million particles in the phase space as a scored plane with dimension of . The second part of the simulations included the Phs file that served as a source for simulating the dose distribution in the water phantom located after the grid block. A 1 mm range cutoff in water was selected, which corresponds to a 350 keV energy cutoff for electrons and positrons, and a 5 keV energy cutoff for photons. The water phantom that was used for these simulations had a dimension of . The center of the water phantom was modeled to be along the central axis of the beam. This phantom was divided into a set of voxels with dimensions of . The accuracy of the simulation was verified by comparison of the simulated data for a open field size with the experimental data obtained with the same field geometry. The measurements were performed with a calibrated PTW‐31010 Semiflex ionization chamber (PTW‐Freiburg, Germany). The measured percentage depth dose (PDD) and the dose profiles at the depth of 5 cm in a water phantom were compared with the Monte Carlo simulated data.
Figure 2.
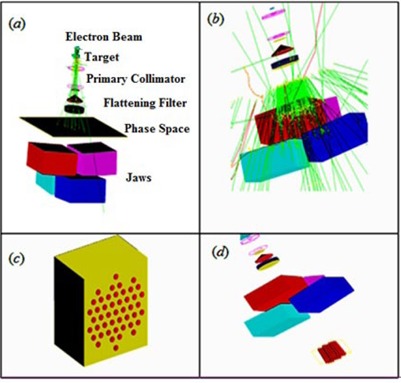
Step one (a) in medical linac simulation using phase space (Phs), different parts in the simulation are represented: electron beam, target, primary collimator, beryllium window, flattening filter, ion chamber, Phs and jaws. Step two in simulation using Phs as a source (b), the hexagonal pattern of modeled grid block (c), and the schematic diagram of the modeled linear accelerator with a grid (d).
In addition, the comparisons were performed with the published clinical data which were based on the grid block treatments with hole diameter of 1.0 cm and center‐to‐center distances of 1.8 cm at the isocenter. 9 , 10 Therefore, for these comparisons a similar grid pattern (i.e., distribution of grid holes) has been used for the simulations. The grid block was designed to
have a hexagonal pattern (11) with divergent holes. The thickness of the grid block was chosen to be 7.5 cm of lead. This grid block was mounted on the block tray holder of the linear accelerator. Figure 2 shows the schematic diagram of the entire pathway of the radiation outside of the water phantom that was used for the simulations in this project.
B. Therapeutic ratio calculation
A dose profile from Monte Carlo simulation, across a single hole of the grid, with 6 MV X‐ray beam at the depth of 5 cm in water phantom has been utilized to calculate therapeutic ratio of the grid block. In these calculations, it has been assumed that the volume of tissues under each grid holes could be divided into segments of circular rings shape with 0.1 mm thickness. The tissue cells in these rings are assumed to receive nearly identical irradiation dose . Equation (1) shows the survival fraction (SF) calculation of the cells under a grid field using LQ model: (6)
| (1) |
where the represents the relative number of cells which are receiving a dose ranging from and . Figure 3 is a schematic diagram for the beam profile of a single grid hole.
Figure 3.
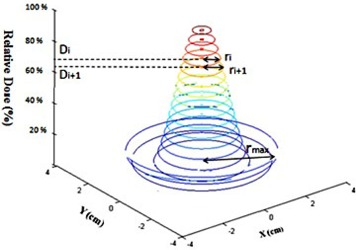
Schematic diagram of the dose profile under a single hole in a grid field with the related parameters that were considered for TR calculations.
Assuming the uniform distribution of the cells within the irradiation area, the is calculated as the ratio of the area of each ring to the total area under a grid hole:
| (2) |
where is the radius of the largest circle under one hole (Fig. 3). This radius is the same as the half of the center‐to‐center distances between the holes.
In grid therapy, the absorbed dose from a single fraction of open field that creates the same tumor survival fraction as the grid field is called equivalent uniform dose (EUD) as shown below:
| (3) |
Therefore, by taking logarithm (ln) from both side of this equation one can find the Eq. (4) as:
| (4) |
The therapeutic advantage of the grid irradiation was related to increase of the normal tissue survival fractions as a ratio of the normal tissue cell survival fraction under grid field irradiation to the normal tissue survival fraction under an open field with equivalent dose of EUD, for the same tumor cell survival.
| (5) |
In the above equation, (Grid) and (EUD) are the survival fractions of the normal tissue for the grid therapy dose and open field with equivalent uniform dose (EUD), respectively.
Recently, some studies have discussed about the suitability of the LQ model when describing cell killing at high doses . 12 , 13 , 14 Kirkpatrick et al. (14) have shown that the LQ model underestimates the surviving fraction in the high‐dose range. However, until now there was no evidence of problems when LQ has been used clinically. (12) In this study, in order to validate the radiobiological modeling results, in addition to the LQ model, a Hug‐Kellerer (H‐K) model (15) was used to recalculate TR and EUD of the same cell lines for grid therapy.
The H‐K model can be expressed as:
| (6) |
where:
| (7) |
In the above equations, , and are the parameters of H‐K model which can be derived for a tumor type considering its SF2 value, α, and β parameters (Eq. (7)).
In this project, tumors were divided into three groups, based on their radiation sensitivities which are assumed to be directly related to their surviving fraction values for 2 Gy dose (SF2). These three groups are composed of radiosensitive tumors , semisensitive tumors , and radioresistant tumors . The value of 0.4 has been determined based on the clinical study by Bjork‐Eriksson et al. (16) In addition, it was assumed that the SF2 value for normal tissue is constant . The values of α/β ratios for tumor cells and normal cells were considered to be 10 Gy and 2.5 Gy, respectively. (17) The values of the SF2 and α/β ratios for both normal tissue and tumor were used in the linear quadratic model to extract the α and β values (Table 1). The therapeutic ratios are calculated based on the single‐fraction grid therapy. A combination of TR and SF2 values were utilized to evaluate the benefit of the grid therapy for different tumor histology. In addition, various prescription doses (2 Gy, 10 Gy, 15 Gy, and 20 Gy) were used to evaluate relationship between maximum dose and therapeutic ratio.
Table 1.
α and β values of tumor and normal cells for three different types of tumors cells
| (Tumor) |
|
|
(Normal) |
|
|
|||||
|---|---|---|---|---|---|---|---|---|---|---|
| Radiosensitive Tumor | 0.2 | 0.670 | 0.067 | 0.4 | 0.254 | 0.101 | ||||
| Semisensitive Tumor | 0.4 | 0.381 | 0.038 | 0.4 | 0.254 | 0.101 | ||||
| Radioresistant Tumor | 0.5 | 0.288 | 0.028 | 0.4 | 0.254 | 0.101 |
C. Clinical reports
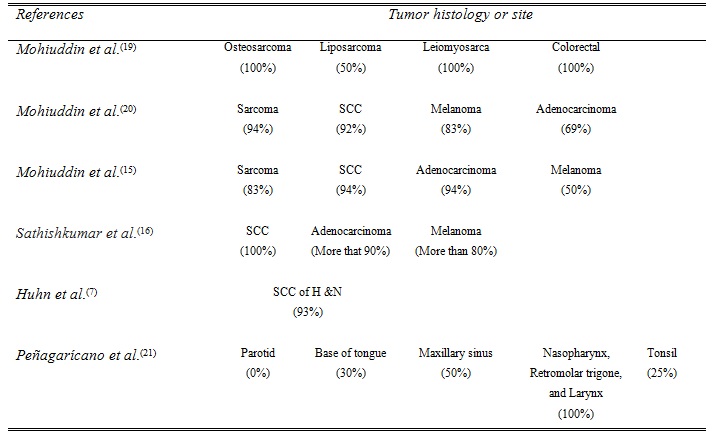
The clinical responses of the patients from different publications, which were treated with grid therapy, have been used to validate the results of the model introduced in this investigation. 7 , 9 , 10 , 18 , 19 , 20 Since the correlation of the responses of the grid therapy with the radiation sensitivity of tumors that were needed from each publication, we focused on the total responses of the treatments, based on the tumor histology and treatment site. The publications which had compatible results with the objectives of this study are briefly described in Table 2.
Table 2.
Clinical total response of grid therapy for tumors with different histological characteristics and treatment sites. The numbers in the parentheses for each tumor type represent the total response under grid therapy
| References | Tumor Histology or Site | ||||
|---|---|---|---|---|---|
| Mohiuddin et al. (18) | Osteosarcoma (100%) | Liposarcoma (50%) | Leiomyosarca (100%) | Colorectal (100%) | |
| Mohiuddin et al. (19) | Sarcoma (94%) | SCC (92%) | Melanoma (83%) | Adenocarcinoma (69%) | |
| Mohiuddin et al. (9) | Sarcoma (83%) | SCC (94%) | Adenocarcinoma (94%) | Melanoma (50%) | |
| Sathishkumar et al. (10) | SCC (100%) | Adenocarcinoma (More that 90%) | Melanoma (More than 80%) | ||
| Huhn et al. (7) | SCC of H&N (93%) | ||||
| Peñagarícano et al. (20) | Parotid (%) | Base of tongue (30%) | Maxillary sinus (50%) | Nasopharynx, Retromolar trigone, and Larynx (100%) | Tonsil (25%) |
In all of the above noted clinical studies, the investigators tried to avoid as much as possible irradiating the normal tissues and critical organs. No margin was added to the GTV and 10 Gy to 20 Gy were prescribed at the depth of maximum dose using a single treatment field. All of these publications have used similar pattern for the grid blocks. Their grids had 1 cm hole diameters with center‐to‐center spacing of 1.8 cm. However, in the clinical report by Peñagarícano et al. (20) which was based on MLC system for grid therapy, the hole spacing was 1 cm. All the clinical reports of grid therapy referred to curative or palliative advanced tumors (mostly stage III/IV) with sizes larger than 6 cm. The patients in the publications had chemotherapy, except in the clinical report by Huhn et al. (7) in which 7 of 27 patients were treated with chemoradiation in grid technique for advanced SCC of head and neck (H&N) tumors. Moreover, these patients normally received full standard radiotherapy after a few days from completion of the grid therapy.
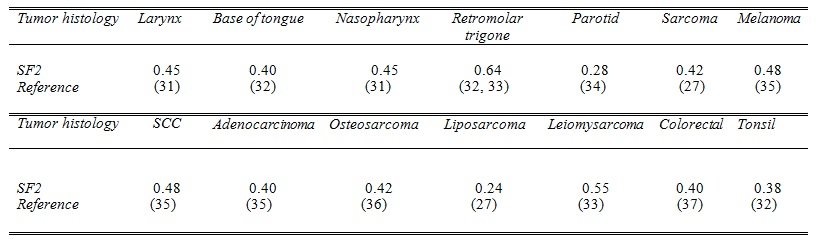
Table 3 shows the list of the SF2 values that were noted in the publications of the clinical data mentioned in Table 2.
Table 3.
SF2 value for different tumors and their corresponding references
| Tumor Histology | Larynx | Base of Tongue | Nasopharynx | Retromolar Trigone | Parotid | Sarcoma | Melanoma |
|---|---|---|---|---|---|---|---|
| SF2 | 0.45 (21) | 0.40 (22) | 0.45 (21) | 0.64 22 , 23 | 0.28 (24) | 0.42 (25) | 0.48 (26) |
| Tumor histology | SCC | Adenocarcinoma | Osteosarcoma | Liposarcoma | Leiomysarcoma | Colorectal | Tonsil |
| SF2 | 0.48 (26) | 0.40 (26) | 0.42 (27) | 0.24 (25) | 0.55 (23) | 0.40 (28) | 0.38 (22) |
D. The grid design
The influences of the hole diameters and center‐to‐center spacing of the holes in a grid block on the therapeutic ratio of the grid therapy were evaluated in these investigations. The dose distributions of grid block with hole diameters of 0.5 cm, 0.75 cm, 1.0 cm, 1.25 cm, and 1.5 cm with constant center‐to‐center spacing of 1.8 cm, were calculated separately using the Monte Carlo simulation technique. Since the prescription dose of 15 Gy per fraction in megavoltage grid therapy is widely accepted, 9 , 10 , 19 , 29 this dose was considered in comparison of the TR values for different grid blocks. Equivalent uniform dose (EUD) for a grid with hole diameter of 1.0 cm and center‐to‐center distance of 1.8 cm was calculated. As suggested by Zwicker et al., (6) for all other grid geometries with different hole diameters and center‐to‐center distances the maximum doses were adjusted such that the value of the EUD remains fixed.
III. RESULTS
A. Monte Carlo simulation
Figure 4 shows the comparison between Monte Carlo simulation and measured relative doses along the central axis (PDD) and transverse direction (dose profile) for 6 MV X‐ray beam. These results show a good agreement between the two sets of data. Simulation has a statistical uncertainty of 1%. More than 90% of the points passed the gamma comparison to within clinical criterion.
Figure 4.
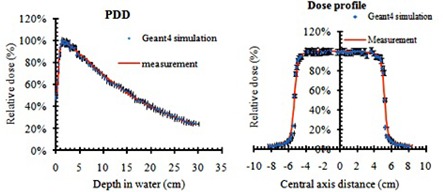
A comparison between the simulated and measured PDD and dose profile of 6 MV X‐ray beam (with 3% error bar).
Figure 5 shows a Monte Carlo simulated 2D dose distribution of a grid field at the depth of 5 cm in water. The grid block was design with 1.0 cm hole diameter and 1.8 center‐to‐center distances. The valley to peak ratio is about 22%.
Figure 5.
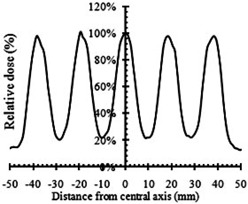
The Monte Carlo simulated beam profile of a 6 MV spatially fractionated photon beam at 5 cm depth in water.
B. Therapeutic ratio calculation
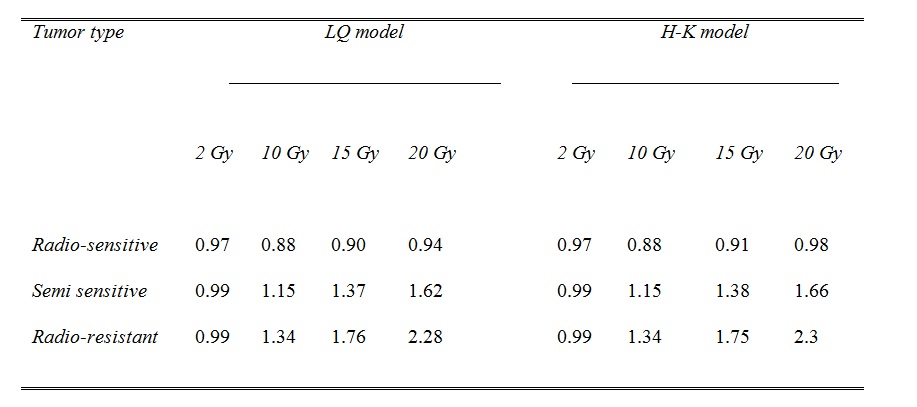
Figure 6 presents the comparison between the survival fraction of the tumor and normal cells irradiated with grid technique and open radiation field. These results confirm the therapeutic advantages of grid therapy compared to conventional radiotherapy regimen. Table 4 shows the therapeutic ratios of the grid fields, calculated by LQ and H‐K models, using the simulated dose profiles as shown in Fig. 5. These results indicate that the TR values of the radioresistant tumors are larger than radiosensitive tumors. In addition, the TR values of the radioresistant and semisensitive tumors increases by increasing the maximum dose per fraction for grid therapy. However, no significant changes are seen on the TR values of the radiosensitive tumors. At the 2 Gy dose, there is about 2% difference in therapeutic ratio between tumors with different radiosensitivities. Therefore, there is no therapeutic advantage of grid therapy with 2 Gy maximum doses. In addition, these results demonstrate that the therapeutic advantage of the grid therapy is more pronounced for radioresistant tumors. Interestingly, the data in Table 4 indicate that, for 20 Gy dose, the differences between the calculated TR values by the LQ and H‐K models for radioresistant and radiosensitive tumors are 1% and 4%, respectively.
Figure 6.
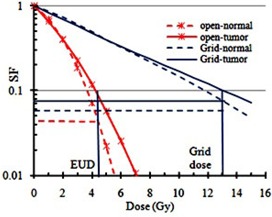
The horizontal thin solid blue line shows SF value for the tumor. The cross point of this line with the survival curve of the tumor with open field reflects the SF for equivalent uniform dose. The horizontal thick solid blue line indicates SF for the normal cell in grid technique. The horizontal red dashed line indicates SF for the normal cell in an open field. The ratio of the survival fraction of normal cells with grid therapy to the open field is called therapeutic ratio.
Table 4.
Therapeutic ratio of different tumor types as a function of the maximum dose
| LQ Model | H‐K Model | |||||||
|---|---|---|---|---|---|---|---|---|
| Tumor Type | 2 Gy | 10 Gy | 15 Gy | 20 Gy | 2 Gy | 10 Gy | 15 Gy | 20 Gy |
| Radiosensitive | 0.97 | 0.88 | 0.90 | 0.94 | 0.97 | 0.88 | 0.91 | 0.98 |
| Semisensitive | 0.99 | 1.15 | 1.37 | 1.62 | 0.99 | 1.15 | 1.38 | 1.66 |
| Radioresistant | 0.99 | 1.34 | 1.76 | 2.28 | 0.99 | 1.34 | 1.75 | 2.3 |
C. Clinical response based on tumor sensitivity
Figures 7(a) and (b) show the changes of therapeutic ratio as a function of the SF2 values of the tumors for three different maximum doses of 10 Gy, 15 Gy, and 20 Gy, using the LQ and H‐K models, respectively. As shown in these figures, the TR value increases by increasing SF2 values (or by decreasing radiosensitivity). In addition, the differences between the TR values are more apparent at larger doses and in more radioresistant (higher SF2) tumors. Figure 7(c) presents the relation between the clinical responses of the tumors treated with grid therapy, using either grid block or MLC, as a function of SF2 values. This figure shows that the clinical responses of the data are better for tumors with larger SF2 values. These results are consistent with Figs. 7(a) and (b). Figure 7(d) indicates the linear function between clinical responses of grid therapy as a function of model based TR values for 15 Gy grid therapy and tumor SF2 values. These results show how similar these two graphs are (i.e., 1SF2 is equivalent to 3.49 TR).
Figure 7.
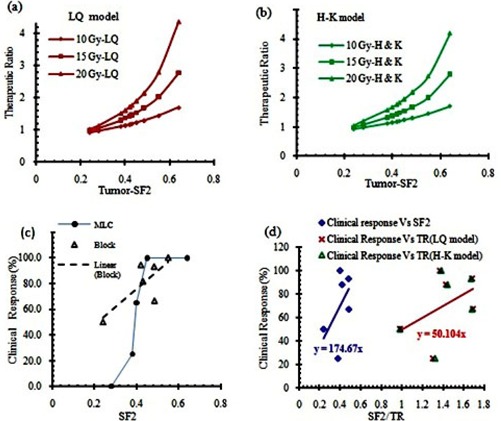
Comparison between therapeutic ratios as a function of the tumor survival fraction at 2 Gy dose (SF2), using LQ model (a) and H‐K model (b); clinical response of different tumors as a function of SF2 for blocked grid (open symbol) and MLC (solid symbol) (c). Clinical response of grid therapy from publications vs. calculated TRs and tumors SF2 value (d).
D. The grid design
Figure 8 shows half of the Monte Carlo simulated dose profiles of grid blocks at a depth of 5 cm in water phantom. These profiles are calculated for grids with hole diameters of 0.5 cm, 0.75 cm, 1.0 cm, 1.25 cm, and 1.5 cm, with a constant center‐to‐center spacing of 1.8 cm. Similar profiles were created for grids with different center‐to‐center spacing.
Figure 8.
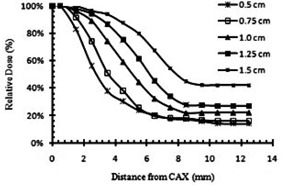
Comparison of the Monte Carlo simulated dose semiprofiles of the grid blocks with different hole diameters, at a depth of 5 cm in water.
Figures 9(a) and 9(b) show the impact of the grid hole diameter and hole center‐to‐center spacing on therapeutic ratio of the grid therapy, respectively. Figure 9(a) indicates that grid blocks with hole diameters of 1.0 cm and 1.25 cm may lead to about 19% higher TR relative to the grids with hole diameters smaller than 1.0 cm or larger than 1.25 cm (with 95% confidence interval).
Figure 9.

Influence of grid hole diameter (a) and center‐to‐center spacing (b) on the therapeutic ratio (TR).
Figure 9(b) shows that the TR of the grid block for a given hole diameter remained nearly unchanged by increasing the spacing between the grid holes.
IV. DISCUSSION
In this study, we have provided the dosimetric simulation of grid therapy and assessment of the radiobiological responses of tumors with different radiosensitivities using the LQ and H‐K models. The validity of results was examined using the available retrospective clinically reported data. Although the clinical experiences with grid therapy are limited, an overview of the published reports might provide a guideline for developing a new strategy in this treatment technique. The biological advantages of grid therapy for different tumor histology have been evaluated. For TRs and EUDs calculations, the LQ and H‐K models have been used. In addition, the impact of the grid design as an effective parameter on therapeutic ratio was investigated.
Comparisons between calculated TRs of different tumors and their SF2 values with clinical data indicate the need for a comprehensive guideline and/or recommendations for tumor selection in order to achieve the optimum treatment result. Although some of the previous clinical and theoretical investigations have demonstrated that it is expected to see a better therapeutic response for radioresistant tumors in grid therapy, 5 , 7 there was no systematic proof of that. The results of the present study emphasize that even for radioresistant tumors, clinical responses of grid therapy may vary with the SF2 value. Some authors 25 , 30 have reported that tumors with different histology may have different SF2 values. Also, they have noted that, for a given tumor with a specific histology, there may be different radiosensitivity characteristics at different anatomical sites. For instance, for sarcoma tumors, various SF2 values ranging from 0.22 to 0.54 have been introduced. It should be noted that for some tumors such as melanoma, all cell lines have the SF2 value in radioresistant range . (31) In general, outstanding clinical responses are expected for these types of tumors (i.e., radioresistant) in grid therapy. From available clinical data, the local control of 79% in H&N SCC was reported in the grid therapy technique. In contrast, for conventional fractionation regimen, the most recent and largest randomized trial (RTOG 9003) reported local‐regional control rate of 33%‐48% for stage III/IV nonmetastatic SCC of head and neck cancer. (32) The overall results of this data shown in Fig. 7 demonstrate the increase of therapeutic response with SF2 of tumor for both MLC‐based and block‐based grids.
As shown in Figs. 7(a) and (b), the TR is increasing with prescribed dose in grid therapy. For a radioresistant tumor with , the calculated TR value for prescribed dose 20 Gy, 15 Gy, and 10 Gy was 2.80, 2.03, and 1.45, respectively. However, for a radiosensitive tumor with , the calculated TR value for those prescribed doses was 1.15, 1.06, and 0.98, respectively. Therefore, there is not as much benefit of grid therapy for the radiosensitive tumors as for the radioresistant tumors.
Comparison between the calculated TRs in Table 4 and Fig. 9 indicates that the radiosensitivity of tumors and the prescribed dose are more efficient than grid design in clinical advantages of grid therapy. From this Monte Carlo study, a grid designs with the hole diameters between 1.0 cm and 1.25 cm are recommended as they have the optimal TR value. The value of EUD for a grid with hole diameters of 1.0 cm and a center‐to‐center distance of 1.8 cm was 4.41 Gy. In order to compare TRs values for all other grids with different designs, maximum doses were adjusted in order to maintain EUD constant at 4.41 Gy. In a study (6) which was about therapeutic advantages of grid therapy, the authors worked on a grid with a specific hole size of 1.3 cm. They calculated EUD for this grid with hole center‐to‐center distance of 1.8 cm and maximum dose of 15 Gy. They kept EUD value constant to examine TR variations with different hole center‐to‐center distances. The hole separation distance of 1.7 cm was suggested for their grid to reach a maximum TR value. The results of our study (Fig. 9) also indicate that, for a grid with hole diameter size of 1.25 cm (which is very close to the Zwicker study (6) ), the center‐to‐center distance of 1.8 cm has the maximum TR value. We couldn't find through previous publications a grid block with hole diameter smaller than 1 cm or larger than 1.5 cm to compare the impact of hole diameter and spacing design on clinical output or therapeutic ratio calculations. Recently, some studies have introduced virtual grid technique using new technologies. (33) For example, recently Jin et al. (34) have introduced a virtual grid using IMRT technique. They considered a lattice of spheres with diameters of 0.5 cm to create dose distributions of the grid. But they did not report about their grid therapeutic ratio calculations or clinical outcome.
One of the challenges that might arise involves using a radiobiological model which is more appropriate for high dose per fraction in grid therapy. Recently a study (35) has reported a 1% difference in the TR calculation for grid therapy of melanoma using both a LQ and MLQ models. This finding is consistent with the results of these investigations. This could be attributed to the small volume of the tissues that receives higher doses under the grid hole. In addition, the value of the equivalent uniform dose (EUD) in grid therapy is in the dose range that the LQ model is valid. (36)
V. CONCLUSIONS
The correlation between the therapeutic ratios of different tumors in grid therapy with their radiation sensitivities was demonstrated in this project by a LQ and H‐K models. These results were then conceded by a comparison with the published clinical data. In this study, it was demonstrated that grid therapy is most beneficial for the radioresistant tumors. In addition, there is no clinical benefit of the grid therapy for the radiosensitive tumors. Moreover, it has been shown that the grid blocks with hole diameters ranging from 1.0 to 1.25 may provide the optimum clinical results.
In summary, our results in this study point out the following which could be used as guidelines:
Knowing the SF2 values of the tumors which are directly related to their radiation sensitivities could be very helpful in selection of the patients for grid therapy.
Grid blocks with hole diameters between 1.0 and 1.25 cm could be utilized to achieve an optimum clinical result.
In our future study, these findings will be tested by the means of in vitro cell survival experiments using appropriate cell lines.
ACKNOWLEDGMENTS
This research has been supported by Tehran University of Medical Sciences and Health Services with grant number 93‐01‐30‐25092.
COPYRIGHT
This work is licensed under a Creative Commons Attribution 4.0 International License.
Supporting information
Supplementary Material Files
{kind=link}
Supplementary Material Files
{kind=link}
Supplementary Material Files
{kind=link}
Supplementary Material Files
{kind=link}
Supplementary Material Files
{kind=link}
Supplementary Material Files
{kind=link}
Supplementary Material Files
Supplementary Material Files
Supplementary Material Files
{kind=link}
Supplementary Material Files
{kind=link}
Supplementary Material Files
{kind=link}
Supplementary Material Files
{kind=link}
Supplementary Material Files
REFERENCES
- 1. Reddy SP, Hong RL, Nagda S, Emami B. Effect of tumor bulk on local control and survival of patients with T1 glottic cancer: a 30‐year experience. Int J Radiat Oncol Biol Phys. 2007;69(5):1389–94. [DOI] [PubMed] [Google Scholar]
- 2. Neuner G, Mohiuddin MM, Vander Walde N, et al. High‐dose spatially fractionated GRID radiation therapy (SFGRT): a comparison of treatment outcomes with Cerrobend vs. MLC SFGRT. Int J Radiat Oncol Biol Phys. 2012;82(5):1642–49. [DOI] [PubMed] [Google Scholar]
- 3. Ha JK, Zhang G, Naqvi SA, Regine WF, Yu CX. Feasibility of delivering grid therapy using a multileaf collimator. Med Phys. 2006;33(1):76–82. [DOI] [PubMed] [Google Scholar]
- 4. Zhang H, Johnson EL, Zwicker RD. Dosimetric validation of the MCNPX Monte Carlo simulation for radiobiologic studies of megavoltage grid radiotherapy. Int J Radiat Oncol Biol Phys. 2006;66(5):1576–83. [DOI] [PubMed] [Google Scholar]
- 5. Zhang H, Wang JZ, Mayr N, et al. Fractionated grid therapy in treating cervical cancers: conventional fractionation or hypofractionation? Int J Radiat Oncol Biol Phys. 2008;70(1):280–88. [DOI] [PubMed] [Google Scholar]
- 6. Zwicker RD, Meigooni A, Mohiuddin M. Therapeutic advantage of grid irradiation for large single fractions. Int J Radiat Oncol Biol Phys. 2004;58(4):1309–15. [DOI] [PubMed] [Google Scholar]
- 7. Huhn JL, Regine WF, Valentino JP, Meigooni AS, Kudrimoti M, Mohiuddin M. Spatially fractionated GRID radiation treatment of advanced neck disease associated with head and neck cancer. Technol Cancer Res Treat. 2006;5(6):607–12. [DOI] [PubMed] [Google Scholar]
- 8. Agostinelli GS, Allison J, Amako K, et al. Geant4‐a simulation toolkit. Nucl Instrum Meth Phys Res A. 2003;506(3):250–303. [Google Scholar]
- 9. Mohiuddin M, Fujita M, Regine WF, Megooni AS, Ibbott GS, Ahmed MM. High‐dose spatially‐fractionated radiation (GRID): a new paradigm in the management of advanced cancers. Int J Radiat Oncol Biol Phys. 1999;45(3):721–27. [DOI] [PubMed] [Google Scholar]
- 10. Sathishkumar S, Dey S, Meigooni AS, et al. The impact of TNF‐alpha induction on therapeutic efficacy following high dose spatially fractionated (GRID) radiation. Technol Cancer Res Treat. 2002;1(2):141–47. [DOI] [PubMed] [Google Scholar]
- 11. Buckey C, Stathakis S, Cashon K, et al. Evaluation of a commercially‐available block for spatially fractionated radiation therapy. J Appl Clin Med Phys. 2010;11(3):3163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Brenner DJ. The linear‐quadratic model is an appropriate methodology for determining isoeffective doses at large doses per fraction. Sem Radiat Oncol. 2008;18(4):234–39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Chapman JD and Gillespie CJ. The power of radiation biophysics—let's use it. Int J Radiat Oncol Biol Phys. 2012;84(2):309–11. [DOI] [PubMed] [Google Scholar]
- 14. Kirkpatrick JP, Meyer JJ, Marks LB. The linear‐quadratic model is inappropriate to model high dose per fraction effects in radiosurgery. Sem Radiat Oncol. 2008;18(4):240–43. [DOI] [PubMed] [Google Scholar]
- 15. Ekstrand KE. The Hug‐Kellerer equation as the universal cell survival curve. Phys Med Biol. 2010;55(10):N267–N273. [DOI] [PubMed] [Google Scholar]
- 16. Björk‐Eriksson T, West C, Karlsson E, Mercke C. Tumor radiosensitivity (SF2) is a prognostic factor for local control in head and neck cancers. Int J Radiat Oncol Biol Phys. 2000;46(1):13–19. [DOI] [PubMed] [Google Scholar]
- 17. Thames H, Bentzen S, Turesson I, Overgaard M, Van den Bogaert W. Time‐dose factors in radiotherapy: a review of the human data. Radiother Oncol. 1990;19(3):219–35. [DOI] [PubMed] [Google Scholar]
- 18. Mohiuddin M, Curtis DL, Grizos WT, Komarnicky L. Palliative treatment of advanced cancer using multiple nonconfluent pencil beam radiation: a pilot study. Cancer. 1990;66(1):114–18. [DOI] [PubMed] [Google Scholar]
- 19. Mohiuddin M, Stevens JH, Reiff JE, Huq MS, Suntharalingam N. Spatially fractionated (GRID) radiation for palliative treatment of advanced cancer. Radiat Oncol Investi. 1996;4(1):41–47. [Google Scholar]
- 20. Peñagarícano JA, Moros EG, Ratanatharathorn V, Yan Y, Corry P. Evaluation of spatially fractionated radiotherapy (GRID) and definitive chemoradiotherapy with curative intent for locally advanced squamous cell carcinoma of the head and neck: initial response rates and toxicity. Int J Radiat Oncol Biol Phys. 2010;76(5):1369–75. [DOI] [PubMed] [Google Scholar]
- 21. Björk‐Eriksson T, West CM, Cvetskovska E, et al. The lack of correlation between proliferation (Ki‐67, PCNA, LI, Tpot), p53 expression and radiosensitivity for head and neck cancers. Br J Cancer. 1999;80(9):1400–04. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Weichselbaum RR, Beckett MA, Schwartz JL, Dritschilo A. Radioresistant tumor cells are present in head and neck carcinomas that recur after radiotherapy. Int J Radiat Oncol Biol Phys. 1988;15(3):575–79. [DOI] [PubMed] [Google Scholar]
- 23. Weichselbaum RR, Beckett MA, Simon MA, et al. In vitro radiobiological parameters of human sarcoma cell lines. Int J Radiat Oncol Biol Phys. 1988;15(4):937–42. [DOI] [PubMed] [Google Scholar]
- 24. Haikonen J, Rantanen V, Pekkola K, Kulmala J, Grénman R. Does skin fibroblast radiosensitivity predict squamous cancer cell radiosensitivity of the same individual? Int J Cancer. 2003;103(6):784–88. [DOI] [PubMed] [Google Scholar]
- 25. Mundt AJ, Awan A, Sibley GS, et al. Conservative surgery and adjuvant radiation therapy in the management of adult soft tissue sarcoma of the extremities: clinical and radiobiological results. Int J Radiat Oncol Biol Phys. 1995;32(4):977–85. [DOI] [PubMed] [Google Scholar]
- 26. Guerrero M and Li XA. Extending the linear‐quadratic model for large fraction doses pertinent to stereotactic radiotherapy. Phys Med Biol. 2004;49(20):4825–35. [DOI] [PubMed] [Google Scholar]
- 27. Deschavanne PJ and Fertil B. A review of human cell radiosensitivity in vitro. Int J Radiat Oncol Biol Phys. 1996;34(1):251–66. [DOI] [PubMed] [Google Scholar]
- 28. Rödel C, Haas J, Groth A, Grabenbauer GG, Sauer R, Rödel F. Spontaneous and radiation‐induced apoptosis in colorectal carcinoma cells with different intrinsic radiosensitivities: survivin as a radioresistance factor. Int J Radiat Oncol Biol Phys. 2003;55(5):1341–47. [DOI] [PubMed] [Google Scholar]
- 29. Reiff JE, Huq MS, Mohiuddin M, Suntharalingam N. Dosimetric properties of megavoltage grid therapy. Int J Radiat Oncol Biol Phys. 1995;33(4):937–42. [DOI] [PubMed] [Google Scholar]
- 30. Amundson SA, Do KT, Vinikoor LC, et al. Integrating global gene expression and radiation survival parameters across the 60 cell lines of the National Cancer Institute Anticancer Drug Screen. Cancer Res. 2008;68(2):415–24. [DOI] [PubMed] [Google Scholar]
- 31. Marshall E, Matthews J, Shaw J, et al. Radiosensitivity of new and established human melanoma cell lines: comparison of [3H]thymidine incorporation and soft agar clonogenic assays. Eur J Cancer. 1994;30(9):1370–76. [DOI] [PubMed] [Google Scholar]
- 32. Fu KK, Pajak TF, Trotti A, et al. A Radiation Therapy Oncology Group (RTOG) phase III randomized study to compare hyperfractionation and two variants of accelerated fractionation to standard fractionation radiotherapy for head and neck squamous cell carcinomas: first report of RTOG 9003. Int J Radiat Oncol Biol Phys. 2000;48(1):7–16. [DOI] [PubMed] [Google Scholar]
- 33. Zhang X, Penagaricano J, Yan Y, et al. Application of Spatially Fractionated Radiation (GRID) to Helical Tomotherapy using a novel TOMOGRID template. Technol Cancer Res Treat. 2013. Accessed 2014: tcrtexpress. 2013.600261. [DOI] [PubMed]
- 34. Jin J‐Y, Zhao B, Kaminski JM, et al. A MLC‐based inversely optimized 3D spatially fractionated grid radiotherapy technique. Radiother Oncol. 2015;117(3):483–86. [DOI] [PubMed] [Google Scholar]
- 35. Zhang H, Zhong H, Barth RF, Cao M, Das IJ. Impact of dose size in single fraction spatially fractionated (grid) radiotherapy for melanoma. Med Phys. 2014;41(2):021727. [DOI] [PubMed] [Google Scholar]
- 36. Gholami S, Nedaie H, Meigooni A, Longo F. Grid therapy: impact of radiobiological models on calculation of therapeutic ratio. In: Jaffray DA, editor. World Congress on Medical Physics and Biomedical Engineering, June 7‐12, 2015, Toronto, Canada. Cham, Switzerland: Springer; 2015. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplementary Material Files
Supplementary Material Files
Supplementary Material Files
Supplementary Material Files
Supplementary Material Files
Supplementary Material Files
Supplementary Material Files
Supplementary Material Files
Supplementary Material Files
Supplementary Material Files
Supplementary Material Files
Supplementary Material Files
Supplementary Material Files