

Abstract
Background and Objectives:
Patients’ satisfaction of anesthesia outcomes is a major part of the overall quality of health care. The aim of this study is to evaluate patient's satisfaction whether pre- or post-operative as well as overall impression using a multicenter prespecified survey tool.
Methods:
Three hundred and three patients who underwent surgery regardless the type of anesthesia were surveyed. The interview conducted face-to-face before surgery then within the first 24 h of surgery. We recorded all basic demographics of patients, the quality of postoperative symptoms control, and the impression about anesthesia team.
Results:
The overall satisfaction level was moderate (56.5%) with nearly half of the patients dissatisfied with their anesthetic care due to different reasons. Nausea and vomiting control was the most common postoperative reasons for dissatisfaction followed by pain control with 35.6% and 31.7%, respectively.
Conclusion:
Type of anesthesia, giving an informative visit to the patient, and the control of postoperative symptoms are the most important predictors of patients’ satisfaction.
Keywords: Anesthesia, nausea, pain, patient satisfaction, vomiting
Introduction
In the late 1980's and early 1990's, the quality assurance movement in health care began to gather momentum.[1] One of the major aspects of this quality is patients’ experience in surgical and anesthesia care. The perception of anesthesia care has been always poor, and even some patients do not consider them real physicians.[2] As early as 1996, an editorial on patient satisfaction showed the emerging need for the assessment of patient satisfaction with anesthesia care and urged anesthesiologists to figure out a reliable assessment methodologies.[3] Hence, patients’ satisfaction has identified as a major target for many studies and nonseparable gear needed for the integrity of health service quality.[4,5] Furthermore, its measurement is required to validate and measure health-care improvement in general.[6] However, the current clinical experience tells us that all tools used for the assessment are not highly reliable or accurately designed.
Patient satisfaction as defined by Pascoe[7] is the patient's reaction consisting of an “emotional response” and “cognitive evaluation” to the care he receives. Consequently, it seems unwise to involve patients in the development of the assessment tools because it is highly subjective and cofounded by many factors such as the socioeconomic standard, demographic data, cultural level, patients’ preferences, quality of tool used, and cognitive ability of the patients.[8] In the same context, there is a reputable tool in Europe for measuring patient satisfaction called “Te Picker inpatient survey;”[9] however, many flaws and drawbacks have been found in the design process which done without true patients’ involvement.[10] Similarly, another tool which underwent a better extensive development is “Hospital Consumer Assessment of Healthcare Providers and Systems Survey;” being used by Press Ganey in the United States.[11]
However, it is still so hard to assess the quality of service in preoperative and intraoperative occasions. The aim of this survey is to evaluate both pre- and post-operative patient satisfaction during the patient stay at five different hospitals in Saudi Arabia.
Methods
Study design
This is a cross-sectional study using a predesigned questionnaire administered during September 2017.
Study setting and site
The survey was undertaken among the patients undergoing surgery in 5 hospitals in Saudi Arabia (Prince Mohammad Bin Abdulaziz Hospital – Madinah, National Guard Health Affairs, Dammam maternity and child hospital, King Saud hospital in Unaizah, Armed Forces Hospital Southern Region, and Prince Mutaib Bin Abdulaziz hospital in sakaka).
Research instrument
We conducted a cross-sectional survey study using a prespecified questionnaire, distributed as hard copies by research collaborators. The questionnaire contains questions categorized into four domains, including demographics characteristic, preoperative visit/satisfaction, postoperative treatment/satisfaction, and overall impression about anesthesia team.
Responses to the opening questions for both pre- and post-operative experience were “yes” and “no.” Format of 5-point Likert scale including “Strongly disagree,” “Disagree,” “Neither agree nor disagree,” “Agree,” and “Strongly agree” were responses for opinion questions with a score ranging from 1 to 5, respectively. On the other hand, a 6-point Likert scale including “Very dissatisfied,” “Dissatisfied,” “Slightly dissatisfied,” “Slightly satisfied,” “Satisfied,” and “Very satisfied” were used to assess satisfaction with a score ranging from 0 to 5, respectively. The first question was designed as written consent for the questionnaire. One pilot surveys were distributed to a pilot group of 50 patients to ensure the validity of questionnaire. The results from the pilot survey and respondents’ solicited comments were used to additionally perfect the questionnaire. The complete research questionnaire is provided in the Supplementary Table 1 (112.7KB, tif) .
Raw data for Figure 1
Testing reliability
We used the most popular reliability test, Cronbach's alpha[12] to measure the internal consistency of our survey on the 50 patients (value >0.70 suggests adequate internal consistency).
Data collection
Surveys were conducted by local teams at each hospital. The survey packet contained a cover letter and a questionnaire with Arabic and English versions. The survey has been handed to each patient to read and decide whether to participate or not. Patients were interviewed preoperative and again within 24-h postoperatively.
Participants
The study aimed to recruit all potential all patients undergoing anesthesia in throughout September 2017 with no restrictions on type of anesthesia or surgery, race, gender, or age. We have excluded patients admitted to Intensive Care Unit postoperatively.
Ethical approval
This study strictly followed the Declaration of Helsinki and was approved by the IRB at each participating hospital. Informed consent was obtained voluntarily from each participant and participants were able to withdraw from the survey at any point. No identifying information of any respondent was obtained during the survey, and all collected data were exclusively used for statistical analysis. The response of study participants was kept confidentially. All potential participants were given information about the study and who volunteer to join will include in the study.
Data analysis
All collected data were transferred into a spreadsheet for further analysis. Standard descriptive measures were calculated for each question/item individually. For data analysis, SPSS 24 for Windows (SPSS Inc., Chicago, IL, USA) were used. Chi-square test was used to measure the significance of difference between different groups. We have measured satisfaction score with maximum score of 5 for each question. For easy interpretation of patients’ satisfaction, “Very dissatisfied,” “Dissatisfied,” and “Slightly dissatisfied” were merged into “Dissatisfied” and the others as “Satisfied.” Similarly, “Strongly disagree” and “Disagree” were merged into “Disagree” while “Strongly agree” and “Agree” were merged into “Agree.” Descriptive and frequency statistics, as well as regression analysis, were used to assess patients’ satisfaction.
Results
Pilot study
Cronbach's alpha for the pilot 50 patients was 0.75 suggesting adequate internal consistency, giving our questionnaire a satisfactory reliability. Comments given by patients were used to improve the questionnaire to get the current final version.
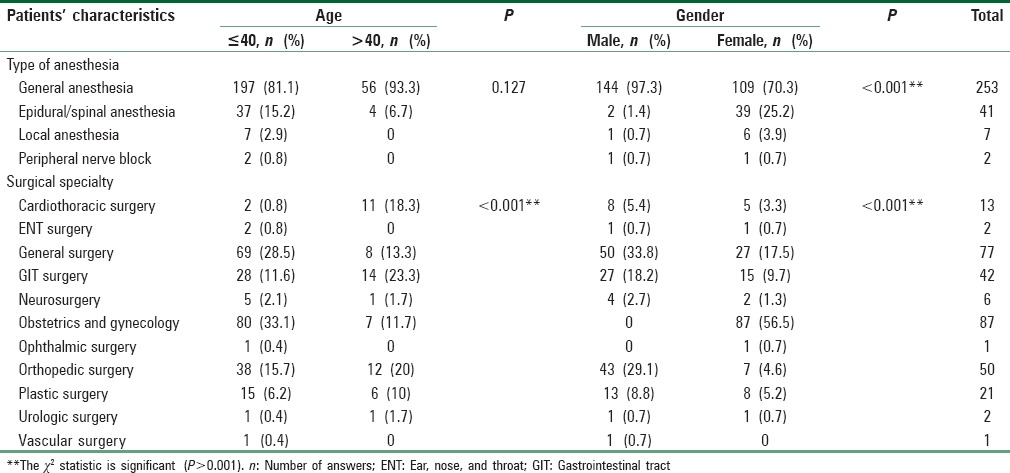
Patients’ characteristics
The response rate of the study was 100% and with total of 303 participants of different types of anesthesia and surgeries. The mean (standard deviation) age was 32.8 (11.8) with age of patients ranging from 15 to 71 years old [Table 1].
Table 1.
Basic characteristics of all patients included in the survey
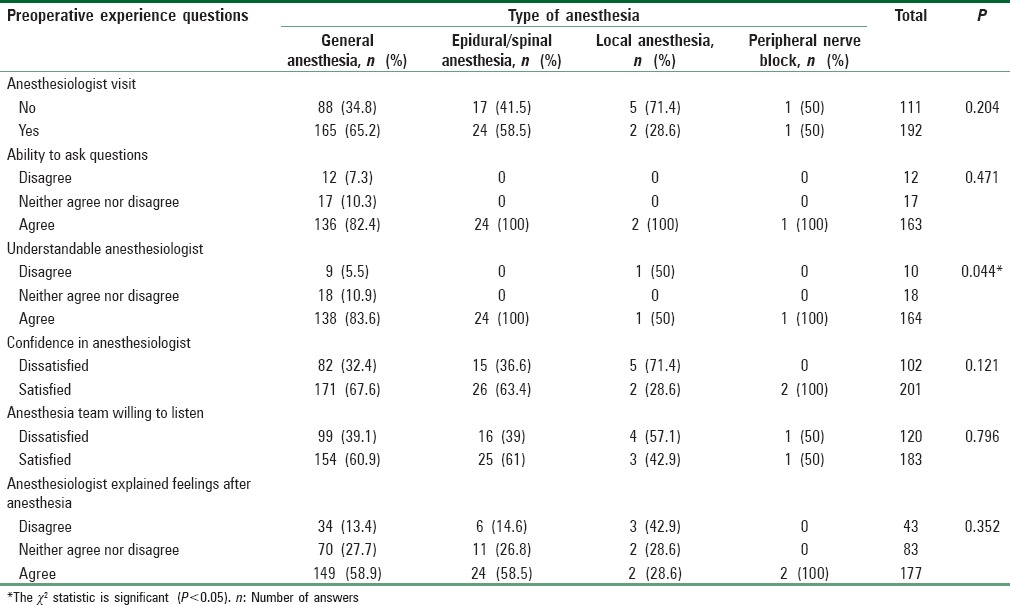
Preoperative experience and satisfaction
Most of the patients (63.4%) got a visit by the anesthesiologist with the obvious predominance of patients’ satisfaction. The results showed a significant interaction between type of anesthesia and level of satisfaction using Chi-square test (P = 0.044). However, this interaction was not present in other items of measurement [Table 2].
Table 2.
Preoperative experience of patients included in the survey
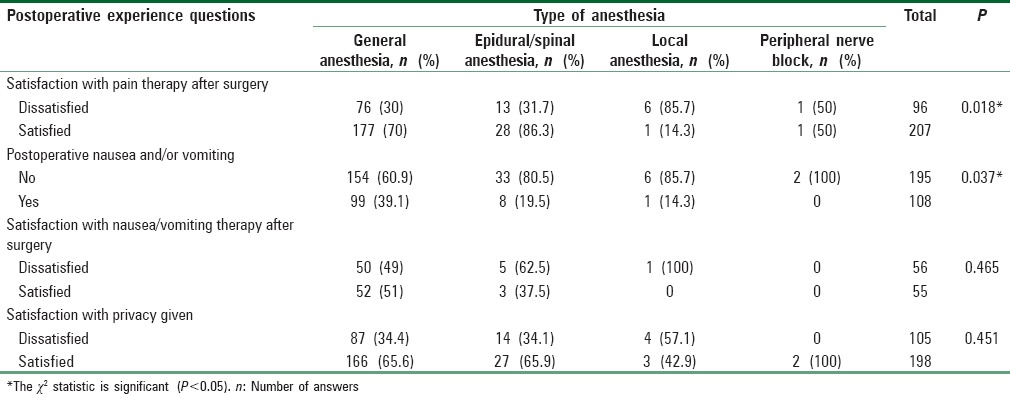
Postoperative experience and satisfaction
Most of the patients were satisfied with pain and nausea/vomiting treatment after surgery with percentages of 66% and 49.5%, respectively. The results showed a significant interaction between type of anesthesia and level of satisfaction with pain treatment (P = 0.018) with the most satisfaction level with epidural/spinal anesthesia (83.6%). Similarly, a significant interaction found with frequency of nausea/vomiting (P = 0.037) and the highest incidence in general anesthesia (39.1%) [Table 3].
Table 3.
Postoperative experience of patients included in the survey
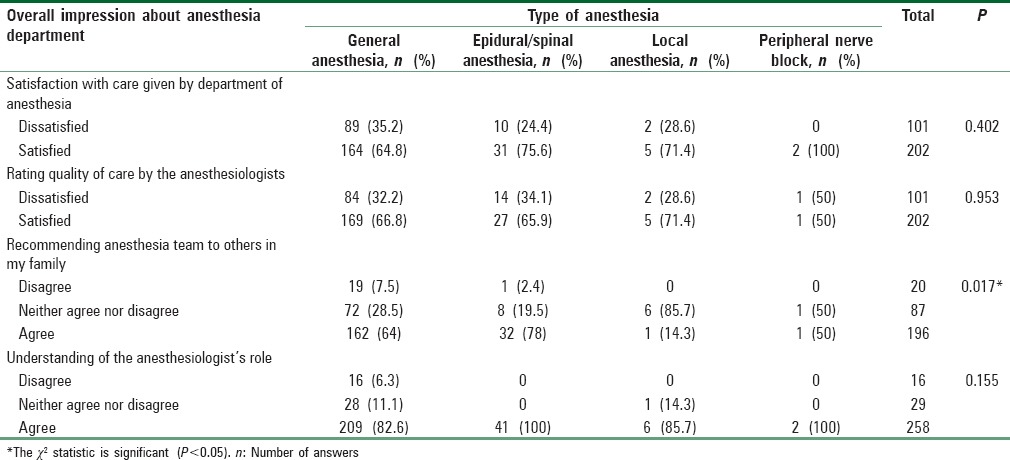
Overall impression about anesthesia team
Majority of patients (66.7%) were satisfied with overall care given by anesthesia department with 64.7% of patients will recommend the anesthesia team to family members. Interestingly, this recommendation was found to have a statistical significant (P = 0.017) interaction with the anesthesia type when Chi-square used [Table 4].
Table 4.
Overall impression of patients included in the survey about anesthesia department
Variations in the average satisfaction percentages have been found between different types of anesthesia. The highest average overall satisfaction was found in general anesthesia with 57%. In the contrary, the lowest percentages were observed in local anesthesia cases with average of 41% only [Figure 1].
Figure 1.
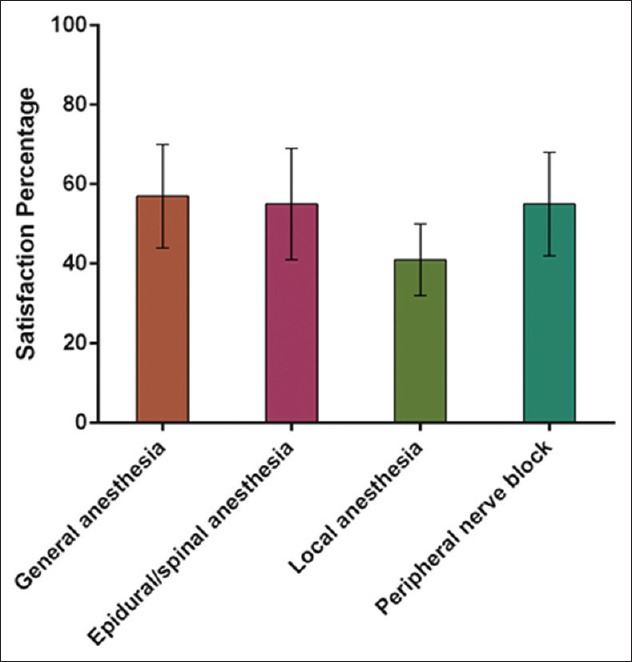
Mean and standard deviation (error bars) of satisfaction percentages grouped by type of anesthesia
Multivariate linear regression
Multiple regression analysis was conducted to predict the overall satisfaction score. The predictors were age, gender, type of anesthesia, and surgical specialty. The linear combination of all these predictors was significantly related to satisfaction score F(4,297) = 5.5, P > 0.001 [Table 5].
Table 5.
Multivariate linear regression models between different predictors and satisfaction score

We have also plotted predicted values using our regression model against actual observed satisfaction scores grouped by anesthesia type to show how successful was the model in the prediction process [Figure 2].
Figure 2.
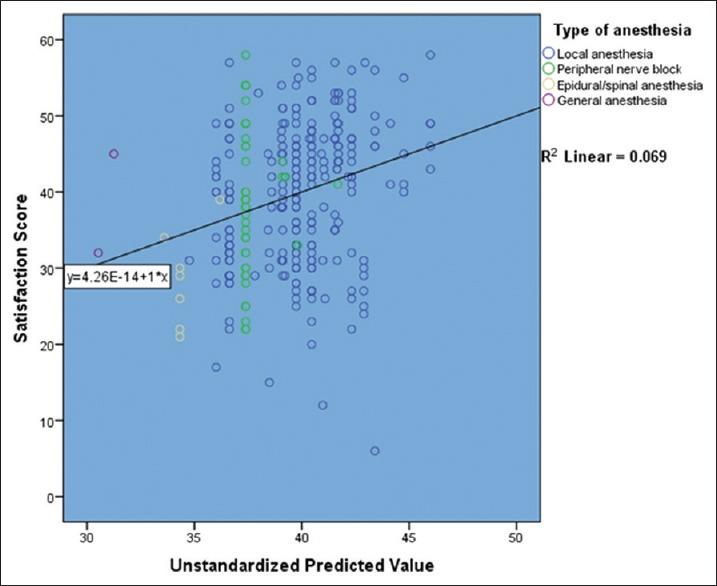
Scatter plot of predicted versus observed satisfaction score
Discussion
Patient satisfaction is the balance between prior expectations, and later, perceptions of the health care receive so, the poor quality will repel patients from the using the service with ease as it should be. Any concerns or problems identified by patients must be taken into consideration with the trail of studying, analyzing, and then implements appropriate solutions.[4]
Our survey found a moderate overall satisfaction of patients (56.5%) which is less than another survey conducted in Saudi patients showing an overall satisfaction of 95.2%.[13] In the same context, another study conducted in Canada with 2730 patient showed overall anesthesia satisfaction as high as 98.9% of the patients.[14] These high rates were present in other studies with dissatisfaction rates down to >15%.[15,16,17] However, these high rates may be giving a false impression because some patients may be biased by the fear of getting a lower quality of care with giving negative appraisals.[18,19] This can be furtherly proved by the results of a multicenter study conducted in 803 Saudi patients showing a reasonable satisfaction rate in only 21.5% of patients.[20]
Our results also showed a great contribution of type of anesthesia in the degree of patients’ satisfaction which was present in both pre- and post-operative as well as overall impression of anesthesia team. The highest satisfaction rate was present with both general and epidural/spinal anesthesia. About 60% of patients underwent both types got visited by an anesthesiologist which seems to have a great impact on patients with average satisfaction of both types being around 60% too. This shows that the interpersonal relationship between patients and anthologists as well as amount of information provided to patients plays a great role too. These results were confirmed by many studies which showed a superiority and higher satisfaction of patients with both local and nerve block methods.[21,22,23,24,25]
It is also well-proved by many studies that postoperative symptoms’ control (pain nausea and vomiting) plays a great role in patients’ satisfaction.[26,27,28,29] This may explain the better reviews on the aforementioned types of anesthesia which usually associated with procedures has much less frequent symptoms. It also can explain the effect of specialty of the results with lower satisfaction in major and abdominal surgeries, hence more postoperative symptoms amplified by the lack of patients’ ability to differentiate between anesthesia and surgery outcomes. A similar effect of age and gender was found with higher satisfaction in males and older patients which was proved by some studies too.[30,31,32,33]
This study, with 303 respondents, is one of the largest satisfaction surveys conducted in Saudi population so far. We conducted for the first time effect of the type of anesthesia in overall satisfaction along with all other demographic characteristics such as age, sex, and surgical specialty.
The major limitations of this study were the low response rate, the small sample of some types of anesthesia and refusal of patients to respond to some questions. Furthermore, the conceptual problems with patient satisfaction might be insurmountable, because perceptions of quality of care are subjective. In the future studies, the reasons for dissatisfaction should be asked of both satisfied and dissatisfied patients, to give a validity check of the global satisfaction questions for both groups. To obtain a more complete picture, other aspects of the experience that reflect the efficiency of the service delivery should also be assessed, such as the operating room turnover time and the time between the fulfillment of discharge criteria and actual discharge. We also recommend an assessment before discharge when patient is more oriented to differentiate surgical from anesthesia complications.
Conclusion
Type of anesthesia, giving an informative visit to the patient, and the control of postoperative symptoms are the most important predictors of patients’ satisfaction. Demographic and subjective differences between patients are effective but to a lesser extent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Eagle CJ, Davies JM. Current models of “quality” – An introduction for anaesthetists. Can J Anaesth. 1993;40:851–62. doi: 10.1007/BF03009257. [DOI] [PubMed] [Google Scholar]
- 2.Klock PA, Roizen MF. More or better – Educating the patient about the anesthesiologist's role as perioperative physician. Anesth Analg. 1996;83:671–2. doi: 10.1097/00000539-199610000-00001. [DOI] [PubMed] [Google Scholar]
- 3.Sheffer MB, Greifenstein FE. The emotional responses of patients of surgery and anesthesia. Anesthesiology. 1960;21:502–7. doi: 10.1097/00000542-196009000-00007. [DOI] [PubMed] [Google Scholar]
- 4.Fung D, Cohen MM. Measuring patient satisfaction with anesthesia care: A review of current methodology. Anesth Analg. 1998;87:1089–98. doi: 10.1097/00000539-199811000-00020. [DOI] [PubMed] [Google Scholar]
- 5.Bell DM, Halliburton JR, Preston JC. An evaluation of anesthesia patient satisfaction instruments. AANA J. 2004;72:211–7. [PubMed] [Google Scholar]
- 6.Moonesinghe SR, Tomlinson AA. Quality improvement and revalidation: Two goals, same strategy? Br J Anaesth. 2011;106:447–50. doi: 10.1093/bja/aer052. [DOI] [PubMed] [Google Scholar]
- 7.Pascoe GC. Patient satisfaction in primary health care: A literature review and analysis. Eval Program Plann. 1983;6:185–210. doi: 10.1016/0149-7189(83)90002-2. [DOI] [PubMed] [Google Scholar]
- 8.Heidegger T, Saal D, Nuebling M. Patient satisfaction with anaesthesia care: What is patient satisfaction, how should it be measured, and what is the evidence for assuring high patient satisfaction? Best Pract Res Clin Anaesthesiol. 2006;20:331–46. doi: 10.1016/j.bpa.2005.10.010. [DOI] [PubMed] [Google Scholar]
- 9.Cleary PD, Edgman-Levitan S, Roberts M, Moloney TW, McMullen W, Walker JD, et al. Patients evaluate their hospital care: A national survey. Health Aff (Millwood) 1991;10:254–67. doi: 10.1377/hlthaff.10.4.254. [DOI] [PubMed] [Google Scholar]
- 10.Cleary PD, Edgman-Levitan S, Walker JD, Gerteis M, Delbanco TL. Using patient reports to improve medical care: A preliminary report from 10 hospitals. Qual Manag Health Care. 1993;2:31–8. [PubMed] [Google Scholar]
- 11.Drain M, Clark P. Measuring experience from the patient's perspective: Implications for national initiatives. J Healthc Qual. 2004;26:W4–16. [Google Scholar]
- 12.Cronbach LJ. Coefficient alpha and the internal structure of tests. Psychometrika. 1951;16:297–334. [Google Scholar]
- 13.Alshehri AA, Alomar YM, Mohammed GA, Al-Fozan MS, Al-Harbi MS, Alrobai KA, et al. A survey on postanesthetic patient satisfaction in a university hospital. Saudi J Anaesth. 2015;9:303–5. doi: 10.4103/1658-354X.158499. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Tong D, Chung F, Wong D. Predictive factors in global and anesthesia satisfaction in ambulatory surgical patients. Anesthesiology. 1997;87:856–64. doi: 10.1097/00000542-199710000-00020. [DOI] [PubMed] [Google Scholar]
- 15.Ward SE, Gordon D. Application of the American Pain Society quality assurance standards. Pain. 1994;56:299–306. doi: 10.1016/0304-3959(94)90168-6. [DOI] [PubMed] [Google Scholar]
- 16.Pineault R, Contandriopoulos AP, Valois M, Bastian ML, Lance JM. Randomized clinical trial of one-day surgery. Patient satisfaction, clinical outcomes, and costs. Med Care. 1985;23:171–82. doi: 10.1097/00005650-198502000-00008. [DOI] [PubMed] [Google Scholar]
- 17.Fitzpatrick R. Surveys of patient satisfaction: II – Designing a questionnaire and conducting a survey. BMJ. 1991;302:1129–32. doi: 10.1136/bmj.302.6785.1129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Pearson A, Durant I, Punton S. Determining quality in a unit where nursing is the primary intervention. J Adv Nurs. 1989;14:269–73. doi: 10.1111/j.1365-2648.1989.tb03413.x. [DOI] [PubMed] [Google Scholar]
- 19.Raphael W. Do we know what the patients think? A survey comparing the views of patients, staff and committee members. Int J Nurs Stud. 1967;4:209–23. doi: 10.1016/0020-7489(67)90026-0. [DOI] [PubMed] [Google Scholar]
- 20.Baroudi DN, Nofal WH, Ahmad NA. Patient satisfaction in anesthesia: A modified iowa Satisfaction in Anesthesia Scale. Anesth Essays Res. 2010;4:85–90. doi: 10.4103/0259-1162.73513. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Quigley TM, Ryan WR, Morgan S. Patient satisfaction after carotid endarterectomy using a selective policy of local anesthesia. Am J Surg. 2000;179:382–5. doi: 10.1016/s0002-9610(00)00371-8. [DOI] [PubMed] [Google Scholar]
- 22.McCarthy RJ, Trigg R, John C, Gough MJ, Horrocks M. Patient satisfaction for carotid endarterectomy performed under local anaesthesia. Eur J Vasc Endovasc Surg. 2004;27:654–9. doi: 10.1016/j.ejvs.2004.03.010. [DOI] [PubMed] [Google Scholar]
- 23.Shabashev S, Fouad Y, Huncke TK, Roland JT. Cochlear implantation under conscious sedation with local anesthesia; safety, efficacy, costs, and satisfaction. Cochlear Implants Int. 2017;18:297–303. doi: 10.1080/14670100.2017.1376423. [DOI] [PubMed] [Google Scholar]
- 24.Ironfield CM, Barrington MJ, Kluger R, Sites B. Are patients satisfied after peripheral nerve blockade? Results from an international registry of regional anesthesia. Reg Anesth Pain Med. 2014;39:48–55. doi: 10.1097/AAP.0000000000000038. [DOI] [PubMed] [Google Scholar]
- 25.Jeon YT. Peripheral nerve block for anesthesia in patients having knee arthroplasty. Korean J Anesthesiol. 2012;62:403–4. doi: 10.4097/kjae.2012.62.5.403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Klafta JM, Roizen MF. Current understanding of patients’ attitudes toward and preparation for anesthesia: A review. Anesth Analg. 1996;83:1314–21. doi: 10.1097/00000539-199612000-00031. [DOI] [PubMed] [Google Scholar]
- 27.Jenkins K, Grady D, Wong J, Correa R, Armanious S, Chung F, et al. Post-operative recovery: Day surgery patients’ preferences. Br J Anaesth. 2001;86:272–4. doi: 10.1093/bja/86.2.272. [DOI] [PubMed] [Google Scholar]
- 28.Beauregard L, Pomp A, Choinière M. Severity and impact of pain after day-surgery. Can J Anaesth. 1998;45:304–11. doi: 10.1007/BF03012019. [DOI] [PubMed] [Google Scholar]
- 29.Gan T, Sloan F, Dear Gde L, El-Moalem HE, Lubarsky DA. How much are patients willing to pay to avoid postoperative nausea and vomiting? Anesth Analg. 2001;92:393–400. doi: 10.1097/00000539-200102000-00022. [DOI] [PubMed] [Google Scholar]
- 30.Cohen G. Age and health status in a patient satisfaction survey. Soc Sci Med. 1996;42:1085–93. doi: 10.1016/0277-9536(95)00315-0. [DOI] [PubMed] [Google Scholar]
- 31.Jaipaul CK, Rosenthal GE. Are older patients more satisfied with hospital care than younger patients? J Gen Intern Med. 2003;18:23–30. doi: 10.1046/j.1525-1497.2003.20114.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Woods SE, Heidari Z. The influence of gender on patient satisfaction. J Gend Specif Med. 2003;6:30–5. [PubMed] [Google Scholar]
- 33.Weisman CS, Rich DE, Rogers J, Crawford KG, Grayson CE, Henderson JT, et al. Gender and patient satisfaction with primary care: Tuning in to women in quality measurement. J Womens Health Gend Based Med. 2000;9:657–65. doi: 10.1089/15246090050118189. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Raw data for Figure 1