

Abstract
Background
The high level of obesity in Latino children, especially in farmworker families, may be partly attributed to feeding styles of parents. Feeding styles used in Latino farmworker families have not been well characterized.
Objective
This study sought to identify and describe feeding styles used by mothers in farmworker families with 2.5–3.5 year-old children, describe how styles change over time, and characterize the relationship of feeding styles to dietary outcomes and measures of overweight and obesity.
Design
This was a longitudinal cohort study, with families participating for a two-year period; surveys were administered to mothers with varying frequency depending on the instrument, and dietary measurements were collected at baseline, 12 and 24 months.
Participants/setting
Eligible participants were self-identified Latino women with a co-resident child aged 2.5–3.5 years and at least one household member engaged in farm work during the previous year. The sample included 248 farmworker families enrolled between 2011 and 2012 in the Niños Sanos study, a longitudinal investigation of Latino mothers and their young children in rural North Carolina. Eleven families provided incomplete dietary data, so analysis included 237 families. Fifteen families were lost to follow-up and 12 withdrew over the course of the study.
Main outcome measures
Feeding style was assessed using items from the Caregiver’s Feeding Style Questionnaire (CFSQ), selected dietary components were assessed using the Revised Children’s Diet Quality Index (RC-DQI), and weight outcomes were determined using BMI-for-age percentile. Performance on the CFSQ items was used to assign mothers to one of four feeding style states.
Statistical analyses performed
Exploratory factor analysis was conducted on baseline data to verify the replicability of the factor structure of the instrument CFSQ. Hidden Markov model analysis (HMM) was used to delineate different subtypes of feeding style. Multi-variable mixed effects regression models were used to assess the impact of feeding style on selected dietary components, energy intake, and BMI-for-age percentile.
Results
Four distinct states emerged from HMM: low parent-centered (PC)/moderate child-centered (CC) feeding style (28% at baseline), high PC/CC without physical control (24%), high PC/CC (26%), and moderate PC/CC (22%). The low PC/moderate CC state increased in prevalence over time. Compared to high PC/CC, the low PC/moderate CC state was associated with greater intake of added sugars (p < 0.01), lower intake of whole grains and vegetables (p < 0.01), and lower overall diet quality (p < 0.05). Children in low PC/moderate CC also had higher mean BMI percentiles (76.2 percentile vs 66.7 percentile in high PC/CC, p < 0.001).
Conclusions
High parent-centered feeding along with high child centered feeding is associated with improved diet quality and weight outcomes for children in the study.
Keywords: BMI percentile, children, farmworker, feeding style, Latino
Introduction
Recent findings from the 2011–2014 National Health and Nutrition Examination Study indicate that 8.9% of all children ages 2–5 were obese (≥ 95th percentile body mass index [BMI] for age and sex).1 Approximately twice as many Hispanic children in this age group (15.6%) met criteria for obesity. Some groups of Latino children, such as those in farmworker families, may be even more vulnerable. A recent study examining 495 Latino children in a migrant farmworker community, ranging from 3 to 16 years of age, found that 27% were obese.2 A study of 52 migrant farmworker children 6 to 11 years of age, nearly all of whom were Latino, found 41% were obese.3 The number of Latino farmworkers in the United States is substantial, and they are estimated to have over 800,000 children.4 Given that agricultural work often serves as the portal through which Latino immigrants enter the United States, understanding potential determinants of obesity in this population is likely to benefit the broader Latino community.5
The high level of obesity found in Latino farmworker children appears multifactorial in nature. Cultural factors such as beliefs and values about proper food and physical activity for children and preferred body shapes, as well as buffering children from hardship, may play a role.6–9 These children often reside in low-income, rural, immigrant households, a context that may limit access to nutritious food and hinder safe and appropriate forms of physical activity.10 Given that many farmworkers are undocumented and migrate, some parents may be unable to utilize government safety net programs intended to ensure children’s access to healthy foods and health care.3,11,12 Parents may receive little guidance regarding children’s diet and fail to recognize children with excess weight as being at risk for health issues.13
An important influence on children’s diet is feeding style, which describes how parents interact with their children in feeding situations.14 Like parenting style, feeding style is often described in terms of two underlying dimensions – demandingness and responsiveness. In this context, demandingness refers to the extent to which parents encourage eating, and responsiveness refers to the manner in which parents encourage eating.15 Dichotomizing demandingness (D) and responsiveness (R) as high and low gives rise to a four-fold classification system – authoritative (high D, high R), authoritarian (high D, low R), indulgent (low D, high R), and uninvolved (low D, low R).14,16 An authoritarian parent does little to consider the needs of the child and imposes strict rules regarding food, typically enforced by a system of rewards and punishments.14 An authoritative parent is sensitive to the child and negotiates appropriate food selection while setting firm limits. The indulgent parent is “nice” and acquiesces to the wishes of the child with few conditions. The uninvolved parent allows the child to do as he or she wishes with minimal engagement. Feeding style is distinct from feeding practices, which are specific behaviors used to influence children’s eating, such as pressure to eat or restriction of certain foods.17 However, style can moderate the association between practices and outcomes such as weight-for-age.18
As the body of research on caregivers’ feeding styles has increased, some trends have emerged in the literature. The authoritarian and indulgent feeding styles appear to be more common than authoritative and uninvolved feeding styles.14,15,18–21 Indulgent feeding styles have been associated with less ideal dietary outcomes among racial/ethnic minority children.14,15,17–20,22 There is less evidence regarding the benefits of an authoritative versus authoritarian feeding style17, though one study did find an authoritative feeding style was associated with greater vegetable and dairy consumption.23 Although low-income racial/ethnic minority children have been examined in terms of feeding style,16,18 Latino farmworker children may differ in important ways. Cultural values related to parenting in Latino families may produce different dimensions of feeding styles, particularly in recent immigrants.24 For example, Mexican culture values warmth and closeness of families, but also respect, which may be reflected in dimensions of indulgence and authority.25,26 Better understanding of the relationship between feeding style and obesity risk may help to explain this population’s high rate of obesity.27
This study is unique in several aspects: (1) the presence of longitudinal data for understanding the dynamic of feeding style as the child develops, (2) a data-driven approach to examine the heterogeneity of feeding styles in a population of children of Latino farmworker families, and (3) the use of extensive dietary and anthropometric outcomes collected at multiple time points. For (2), an extended version of latent class analysis, the hidden Markov model (HMM) was applied to the longitudinal data. The HMM was used for two reasons. First, in exploratory data analysis, it was found that feeding style patterns could not be fully captured by the sum-score approach of traditional methods. For example, there existed a group of mothers that tended to physically struggle with child to get the child to eat. This kind of nuanced information could not be made available using a sum-score approach. Second, previous work for forming feeding style topology was based on cutoff scores. As a result, findings may be sensitive to cut-points and not robust. The data-driven HMM approach is able to offer insightful information into feeding style. Insight into the benefits of one feeding style relative to the others could form the basis for parental interventions. Although many factors contribute to Latino children’s high prevalence of obesity, feeding style may represent an important modifiable factor for mitigating this disparity.
The purpose of this study is to determine what feeding styles Latino farmworkers use with their young (2.5 to 3.5 year-old) children, the dynamic of these feeding styles over an extended period of time, and whether or not feeding style is related to a broad set of dietary and weight-related outcomes. The primary hypothesis of the current study is that children whose parents regulate feeding more closely will have better selected dietary components and lower risk of overweight and obesity.
Methods
This analysis included 248 families enrolled in the Niños Sanos study. Niños Sanos is a longitudinal two-year study designed to describe the dietary and physical activity patterns of young children of Latino farmworkers in North Carolina.6,10 Eligible participants were self-identified Latino women with a co-resident child aged 2.5 to 3.5 years and at least one member of the household engaging in farm work during the previous year. The study focused on 2.5 to 3.5 year old children because this is an age when eating and feeding practices are established. Children with special healthcare needs limiting physical activity were excluded.
Sampling and Recruitment
A site-based sampling plan with a large contact base was developed to recruit participants. This approach was chosen due to the narrow age range of children and lack of sampling frame for Latino farmworker families in North Carolina. “Sites” are organizations or locations with which members of the target community are associated. Sites used in this study include Head Start and Migrant Head Start programs (n = 7), migrant education programs (n = 15), community health centers (n = 4), Special Supplemental Nutrition Program for Women, Infants, and Children (n = 1), community partner nonprofit organizations (n = 2), and stores, churches, and events serving predominantly farmworkers (n = 7). Community data collectors also conducted door-to-door recruitment in multiple Latino neighborhoods and farmworker camps, and they contacted previous participants in Latino health studies regarding participation.
A trained bilingual data collector contacted potential participants. Organizations subject to privacy regulations (i.e., Head Start) used staff members to solicit permission to contact parents. After making contact, the data collector introduced the study and screened for inclusion criteria. Requirements and incentives of study participation were explained and eligible families were invited to participate. Those who agreed to participate were scheduled to complete enrollment and baseline data collection. All participants provided signed informed consent. The Wake Forest School of Medicine Institutional Review Board approved the study, and a certificate of confidentiality28 was obtained from the National Institutes of Health to protect subject anonymity.
Data Collection
Nine trained study staff interviewed participants in Spanish quarterly over 24 months, typically at the participant’s home or another convenient location. Some data, including dietary data, were only collected at selected quarters. Data used in this longitudinal study were collected at baseline, 12 months, and 24 months during the period of April 19, 2011, to July 30, 2014. Participants responded to an interviewer-administered survey designed to collect information regarding demographic, family, and household characteristics as well as feeding style. Additional surveys for dietary data and other measures are described below.
Child dietary data were collected from mothers by bilingual staff members using three 24-hour recalls during a seven day period, including one weekend day and two weekdays. The Nutrition Data System for Research (NDSR) software was used.29 This approach utilizes “multiple passes.” The first recall was conducted face-to-face, and subsequent interviews were conducted by telephone or, when possible, in person. Participants were given an incentive of $10 per completed recall. Mothers without telephone access were loaned a cell phone programmed only for study use. Mothers were given a printed serving size guide, and the interviewer measured the size or volume of their child’s usual bowl, plate, and cup to help facilitate calculation of serving sizes. For children enrolled in preschools or daycares, with mothers’ permission, food intake data were collected directly from the caregivers. Because some mothers needed to obtain intake data from caregivers, the random day procedure usually used for repeated recalls was modified. The initial recall was unannounced, because it was part of the interview. Subsequent interviews were negotiated at that time to fit the mother’s availability, although the weekday/weekend distribution of days was maintained.
Child weight was quarterly measured using a Tanita model BSB800 digital scale capable of determining weight to the nearest 0.1 kilogram. Also quarterly, child height was determined twice using a portable stadiometer without shoes; measurements were averaged.
Measures
Caregiver’s Feeding Style Questionnaire (CFSQ)
Parental feeding style was measured at baseline, 12 months, and 24 months using the Caregiver’s Feeding Style Questionnaire (CFSQ).14 The CFSQ was designed specifically for use with low income African Americans and Hispanics. Development of the CFSQ included literature review, videotaped observations of feeding interactions, cognitive interviewing, and back translations.16 Acceptable test-retest reliability (Pearson’s correlation of 0.73–0.79) and internal consistency (Cronbach’s alpha of 0.71–0.86) have been demonstrated.14–16 Convergent validity has been established via comparison to subscales of related instruments.14
The CFSQ has been refined since its debut. Initial factor analysis revealed parent-centered and child-centered feeding strategies, along with a third factor related to second helpings that was dropped due to small size and low coefficient alpha.14 Subsequently, Hughes et al. presented an updated version with improved model fit.16 They removed six cross-loading items and split the parent-centered factor into parent-centered and contingency management factors, resulting in a total of 13 items distributed along three factors. This iteration16 of the CFSQ formed the basis of the present analysis.
Each of the 13 items was rated on a five point Likert scale ranging from one (never) to five (always). The items measure use of strategies that are either “parent-centered” or “child-centered” in nature. A parent-centered strategy influences children’s eating externally through use of demands and rewards (e.g., spoon-feed the child to get him or her to eat dinner). A child-centered strategy fosters internalization of parental values through reasoning and discussion (e.g., compliment the child for eating certain food).
All items on the CFSQ are intended to measure the extent to which parents try to get their children to eat. Therefore, the mean score of all items constitutes the level of demandingness. Responsiveness is determined by dividing the mean of the child-centered items by the mean score of the entire instrument (in other words, dividing the mean of child-centered items by the level of demandingness). Researchers have suggested that demandingness scores > 2.8 and responsiveness scores > 1.16 be considered high.30 By rating participants as either or high or low in these regards, one can determine adherence to a particular feeding style (e.g., authoritarian – high demandingness, low responsiveness). In various studies that have used the CFSQ, mean demandingness score has been found to vary between 2.6 and 2.8, while mean responsiveness score has varied between 1.14 and 1.16.15
Revised Children’s Diet Quality Index (RC-DQI)
A Revised Children’s Diet Quality Index (RC-DQI), specifically developed for use among preschoolers, was used to evaluate adequacy of children’s dietary intake at baseline, 12 months, and 24 months.31 This index uses 13 dietary components, such as added sugar and fat intake, to determine diet quality. The range of possible scores extends from 0 to 90, with higher values indicating higher quality. Points are deducted for each component according to the degree of deviation from the ideal. These ideal targets were determined using recommendations from several expert sources, such as the National Academy of Sciences, United States Department of Agriculture, and the American Academy of Pediatrics.31 Although the RC-DQI contains 13 components and these have been included in prior analyses with this sample,5 only selected components (sugar, fat, whole grains, fruit, vegetables, and dairy) and a composite RC-DQI score were used in the present analysis for the sake of brevity.
Other measures
Energy intake was calculated as the mean of total kilocalories per day from the three 24-hour dietary recalls collected at each time point.
Mothers reported their own age and the child’s age and sex. Family migrant status was based on maternal characterizations of herself and another household member’s involvement in farm work at baseline: if she classified either person as a “migrant worker who moves from place to place to do farm work,” the family was classified as migrant. Farmworkers who stayed in one place to work were considered seasonal. Each mother reported whether she or her spouse/partner had documents allowing legal residence in the United States; if either did, the family was classified as “documented.” Education was measured in terms of years of school completed.
BMI-for-age percentile was derived for analysis. To allow for separating the possible confounding effect of heterogeneity in adiposity rebound at this age range of the children, weight-for-age percentile was also derived. Adiposity rebound refers to the age at which BMI reaches its nadir and increases thereafter, typically between the ages of 3–7.32
Statistical Analysis
Statistical analysis comprised several stages. First, exploratory factor analysis was conducted on baseline data to verify the replicability of the CFSQ factor structure from previous studies. Given the possibility that the factor structure of the CFSQ for this special population was different from those of populations assessed in previous studies, the factor analysis identified a set of relevant items for measuring feeding style useful for comparison. Recently, Kiang and Ip used a similar approach of using factor analysis to select items from a previously validated measure and applying the method to a novel cultural setting.33 Maximum likelihood factor analysis was used alongside an oblique/correlated factor rotation. The threshold to consider an item as belonging to a factor was set at 0.5.
The second stage of the statistical analysis involved the delineation of different styles of feeding in the Latino farmworker population and the dynamic of change over time. A data-driven approach to the classification of feeding styles, HMM, was adopted, which made use of the results of factor analysis from the first stage. While factor analysis is intended to examine which items group together, the HMM identifies which families are similar in terms of feeding behaviors. Selected CFSQ items from the factor analysis formed the profile of feeding style for HMM.
The HMM categorizes each family into one of the latent (hidden) classes (states) and estimates a trajectory of the states of the individual families over time. Thus, the HMM can be considered a longitudinal extension of latent class analysis. Instead of using cut-points for creating categories, the HMM uses a data-driven approach to delineate distinct states and avoids some of the problems with the cut-point approach.34 Computationally the HMM is able to handle a large number of time points as well as extend in different directions including accommodation of complex relationships between variables.35,36 Families could change state over the course of the study period, and the likelihood of transitioning into other states was captured using a transition probability table estimated from the data.
In the third stage of statistical analysis, multi-variable mixed effects regression models were used to examine longitudinally whether or not feeding style could predict outcomes such as selected dietary components, energy intake, and BMI-for-age percentile. The following covariates were included in the models: sex of the child, migrant status, and age of child at baseline.
A 2-sided test with a specified significance level of 0.05 was used consistently. Matlab-based HMM software, which can be downloaded without fee,37 was used for the HMM analysis; and Proc Mixed and Proc Glimmix from SAS version 9.338 were used for longitudinal regression analyses.
Results
Sample Characteristics
The majority of the 248 enrolled mothers were between the ages of 26 and 35, and three-quarters had less than a tenth grade education. Most families participated in seasonal agricultural work, and nearly 85% lacked documentation permitting legal residence (Table 1). Of the 248 mother–child dyads enrolled in the Niños Sanos study, eight failed to complete any 24-hour recall; and three provided incomplete dietary data. Therefore, subsequent analyses are based on 237 dyads. Retention was high, with only 15 families lost to follow-up and 12 families withdrawing over the course of the study. On average, 86.3% of families completed each quarterly assessment.
Table 1.
Baseline sociodemographic characteristics of Latino mothers and their children (all participants) in the Niños Sanos study, North Carolina, 2011–2014
| Personal Characteristics | Total Sample (N=248) | |
|---|---|---|
| N | % | |
| Mother’s Age | ||
| 18 to 25 years | 72 | 29.0 |
| 26 to 35 years | 138 | 55.7 |
| 36 to 45 years | 38 | 15.3 |
| Educational Attainment | ||
| 0 to 6 years | 108 | 43.6 |
| 7 to 9 years | 76 | 30.7 |
| 10+ years | 64 | 25.8 |
| Farmworker Statusa | ||
| Migrant | 68 | 27.4 |
| Seasonal | 180 | 72.6 |
| Household Immigration Statusb | ||
| Any adult documented | 38 | 15.4 |
| No adult documented | 209 | 84.6 |
| Child’s Age at Baseline | ||
| 2.5 to <3.0 years old | 131 | 52.8 |
| 3.0 to 3.5 years old | 117 | 47.2 |
| Child’s sex | ||
| Male | 119 | 48.0 |
| Female | 129 | 52.0 |
If a mother classified herself or another household member as a “migrant worker who moves from place to place to do farmwork,” the family was classified as migrant. Otherwise, if the mother classified both herself (if relevant) and other household members as “a seasonal farmworker, someone who lives here all the time,” the family was classified as being seasonal.
Data is missing for one individual
Construction of CFSQ Factors and HMM
The factor analysis of the 13-item version of the CFSQ resulted in a three-factor solution. Table 2 illustrates factor loadings identified using Niños Sanos data and compares these with previous results reported in the development of the instrument.16 Factors 1 through 3 were identified to correspond to the parent-centered, contingency management, and child-centered factors, respectively. To find the maximal set of items that are consistent with the original factor structure, the largest absolute value of the factor loadings that exceeded 0.5 identified the items. Three parent-centered items were identified as belonging to factor 1. Two contingency-management items loaded onto factor 2, and three child-centered items loaded onto factor 3.
Table 2.
Exploratory factor analysis (rotated factor pattern, standardized regression coefficients) for the Caregiver’s Feeding Style Questionnaire (CFSQ)16 in the Niños Sanos study, North Carolina, 2011–2014a
| Item | Factor 1b | Factor 2 | Factor 3 | |
|---|---|---|---|---|
| Parent-Centeredc | ||||
| 1 | Beg your child to eat dinnerd | 0.681 | 0.092 | 0.048 |
| 2 | Spoon-feed the child to get him or her to eat dinnerd | 0.788 | −0.073 | −0.030 |
| 3 | Physically struggle with the child to get him or her to eatd | 0.535 | 0.014 | −0.073 |
| Parent-Centered/Contingency Managementc | ||||
| 4 | Warn the child that you will take away something other than food if he or she doesn’t eat | 0.587 | 0.214 | 0.018 |
| 5 | Promise the child something other than food if he or she eatsd | −0.018 | 0.722 | 0.129 |
| 6 | Encourage the child to eat something by using food as a rewardd | 0.057 | 0.783 | −0.050 |
| 7 | Warn the child that you will take a food away if the child doesn’t eat | 0.375 | 0.139 | 0.071 |
| Child-Centeredc | ||||
| 8 | Say something positive about the food the child is eating during dinnerd | 0.067 | 0.064 | 0.505 |
| 9 | Reason with the child to get him or her to eat | 0.757 | 0.095 | −0.033 |
| 10 | Help the child to eat dinner | 0.806 | −0.133 | 0.031 |
| 11 | Compliment the child for eating foodd | −0.015 | 0.062 | 0.608 |
| 12 | Encourage the child to eat by arranging the food to make it more interesting | 0.513 | 0.011 | 0.186 |
| 13 | Ask the child questions about the food during dinnerd | −0.010 | −0.055 | 0.855 |
n=237
Bolded values indicate the highest loading with factor analysis; threshold 0.5 used to determine the factor to which an item belongs
Factors identified in previous work16
Items selected for subsequent hidden Markov analysis
Eight items were selected to create the profile for feeding style, which formed the basis of the HMM analysis. Since each type of item (parent-centered, contingency management, child-centered) should ideally load on its own factor, all three parent-centered items that loaded on factor 1, the two contingency items that loaded onto factor 2, and the three child-centered items that loaded onto factor 3 were included. Contingency items and child-centered items that loaded onto factor 1 were dropped.
HMM indicated that a 5-state model was most appropriate, statistically. However, upon examination of the individual states, two states were noted to be very similar and one of these was very small. Therefore, a 4-state model was deemed most appropriate for subsequent analyses.
State 1 (low parent-centered/moderate child-centered) was characterized by low use of parent-centered strategies and contingency management, and moderate use of child-centered techniques (Figure 1). State 2 (high parent-centered/high child-centered without physical control) featured high use of parent-centered strategies and contingency management and high use of child-centered strategies. However, the use of physical force to get children to eat (item 3) was notably absent. In contrast, state 3 (high parent-centered/high child-centered) was shown to use all forms of parent-centered control, including physical force, as well as high levels of child-centered feeding. State 4 (moderate parent-centered/moderate child-centered) included low-to-moderate levels of parent-centered control and moderate levels of child-centered control, higher than state 1 but lower than states 2 and 3. Therefore, state 4 was considered “balanced” in approach. At baseline, the prevalences of these 4 states were, respectively, 28%, 24%, 26%, and 22%.
Figure 1.
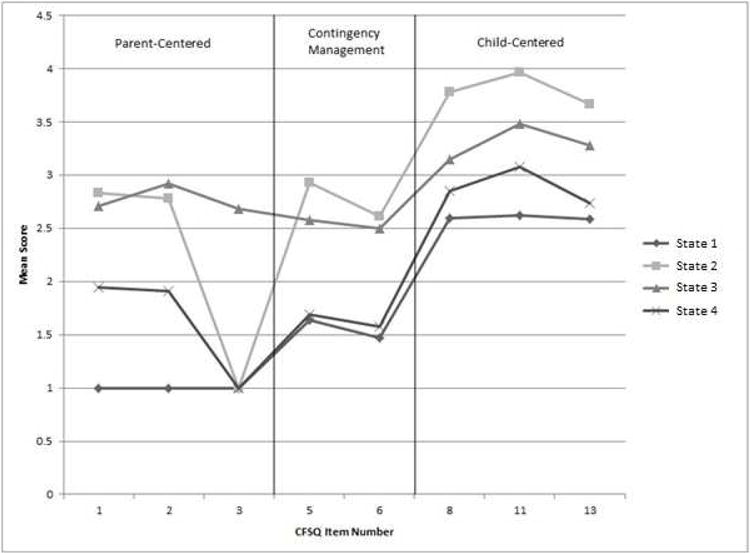
State Characteristics by Caregiver’s Feeding Style Questionnaire (CFSQ) Item in the Niños Sanos Study, North Carolina, 2011–2014·(n=237) Note. Scores by CFSQ item are shown for the four states – State 1 = low levels of parent-centered feeding and moderate levels of child-centered feeding, State 2 = high levels of parent and child-centered feeding, with the absence of physically struggling to get the child to eat, State 3 = high levels of both parent and child-centered feeding, and State 4 = moderate usage of both parent and child-centered feeding strategies; the CFSQ contains items that measure use of parent-centered, parent-centered/contingency management, and child-centered feeding strategies. The numbers on the x-axis refer to these items as listed in Table 2.
Feeding states were contrasted with the four-fold demandingness/responsiveness typology. Figure 2 shows the mean score of demandingness and responsiveness across the 4 feeding states identified in this study. Using suggested cutoff scores, the high PC/CC without physical control and high PC/CC states demonstrated high levels of demandingness (>2.8); and the low PC/moderate CC, high PC/CC without physical control, and moderate PC/CC states were high in terms of responsiveness (>1.16). The cutoff scores were rescaled CFSQ summary scores. While not a perfect one-to-one correspondence, the low PC/moderate CC state would be considered indulgent, the high PC/CC without physical control state authoritative, the high PC/CC state authoritarian, and the moderate PC/CC state indulgent as well, although less so than the low PC/moderate CC state.
Figure 2.
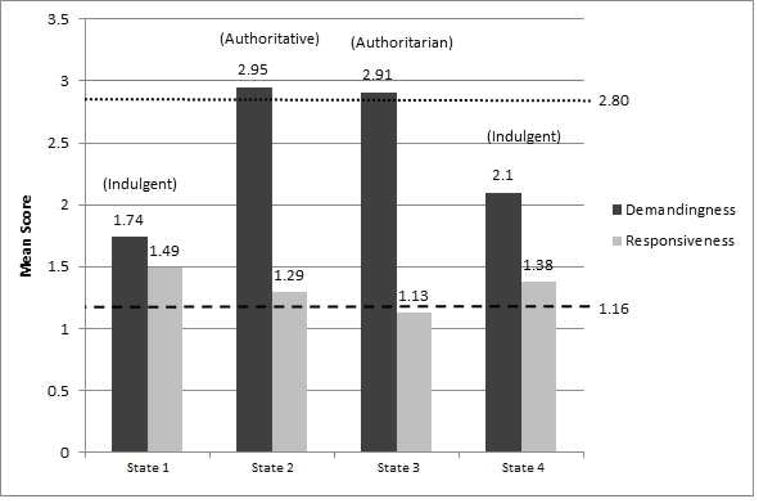
Demandingness and Responsiveness Scores by State at Baseline in the Niños Sanos Study, North Carolina, 2011–2014 · (n=237). Note. Each state can be characterized in terms of demandingness and responsiveness. Demandingness scores > 2.80 (dotted line) can be considered “high,” and responsiveness scores > 1.16 (dashed line) can also be considered “high.” For example, a state that features a high level of demandingness and low level of responsiveness, such as state 3, is considered to be authoritarian in nature. State 1 = low levels of parent-centered feeding and moderate levels of child-centered feeding, State 2 = high levels of parent and child-centered feeding, with the absence of physically struggling to get the child to eat, State 3 = high levels of both parent and child-centered feeding, and State 4 = moderate usage of both parent and child-centered feeding strategies.
Change in state prevalence over the course of the study is shown in Figure 3. The low PC/moderate CC state increased in prevalence, while the other three states gradually decreased. The HMM provides insight into state dynamics, as reflected by the probability of moving from one state into another. The low PC/moderate CC state was stable in the sense that mothers who belonged to that state at baseline or year 1 were unlikely to transition into a different state. In fact, 80% of mothers in this state remained so between any two consecutive time points. Members of the high PC/CC state had approximately equal likelihood of moving into any of the other states versus remaining in the same state. Additionally, at any given time point, approximately 1/3 of high PC/CC without physical control mothers stayed in the same state, with about half moving to either the low PC/moderate CC or moderate PC/CC states and 12% moving to high PC/CC. Members of the moderate PC/CC state were most likely to transition to the low PC/moderate CC state (62% chance) with a smaller number (24%) not changing.
Figure 3.
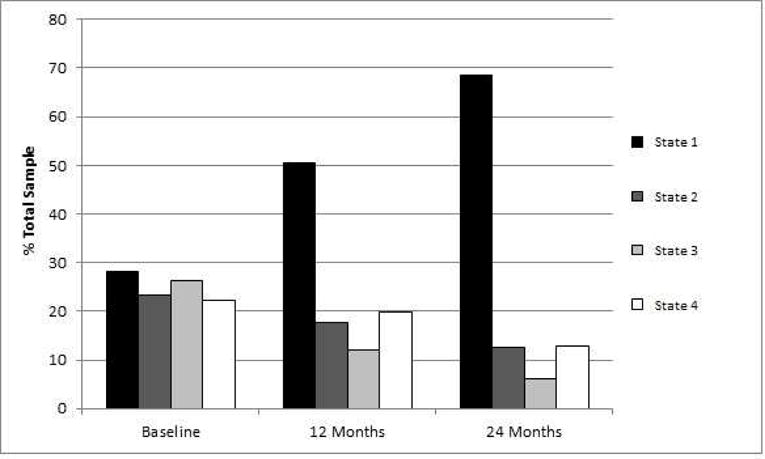
Distribution of State Membership over Time in Percentage in the Niños Sanos Study, North Carolina, 2011–2014 · (n=237). Note. State 1 = low levels of parent-centered feeding and moderate levels of child-centered feeding, State 2 = high levels of parent and child-centered feeding, with the absence of physically struggling to get the child to eat, State 3 = high levels of both parent and child-centered feeding, and State 4 = moderate usage of both parent and child-centered feeding strategies
Results for Outcome Analysis
At baseline, 59% of children received all meals at home. Mean RC-DQI score for each state and individual dietary component scores at baseline are shown in Table 3. Higher scores indicate higher quality. The high PC/CC state had a significantly higher RC-DQI composite score compared to the low PC/moderate CC state (p < .05). The high PC/CC state also had higher component scores for added sugar, whole grains, and vegetable consumption relative to low PC/moderate CC (p < .01). This trend was reversed for fat intake (p < .001). The high PC/CC without physical control and moderate PC/CC states showed scores for added sugar, whole grains, and vegetables that were between the values of the low PC/moderate CC and high PC/CC states, and most differences were not statistically significant. No significant differences were found for fruit and dairy intake (p values range 0.1–0.8).
Table 3.
Hidden Markov State differences in Revised Children’s Diet Quality Index (RC-DQI) mean composite score and selected components, energy intake, weight percentile, and BMI percentilea in the Niños Sanos study, North Carolina, 2011–2014b
| State 1c,d | State 2 | State 3 | State 4 | Total | |
|---|---|---|---|---|---|
| RC/DQI componente | |||||
| Composite RC-DQI score (0–90) | 60.0 | 59.3 | 61.3* | 61.4 | 60.2 |
| CIf | (−1.6, 2.2) | (0.6, 4.6) | (−0.2, 3.3) | ||
| Added sugar (0–10) | 4.31 | 4.43 | 5.69** | 5.23 | 4.72 |
| CI | (−0.5, 1.2) | (0.5, 2.2) | (−0.1, 1.4) | ||
| Fat (0–5) | 2.35 | 2.28* | 2.23*** | 2.30 | 2.31 |
| CI | (−0.1, −0.02) | (−0.2, −0.06) | (−0.1, 0.01) | ||
| Whole grains (0–5) | 2.57 | 2.55 | 3.10** | 2.86* | 2.70 |
| CI | (−0.2, 0.5) | (0.2, 0.9) | (0.01, 0.7) | ||
| Fruit (0–10) | 4.32 | 4.45 | 4.63 | 4.81 | 4.49 |
| CI | (−0.3, 0.8) | (−0.2, 4.0) | (−0.1, 1.0) | ||
| Vegetables (0–10) | 3.18 | 3.55 | 4.03** | 3.37 | 3.42 |
| CI | (−0.2, 0.9) | (0.3, 1.4) | (−0.4, 0.7) | ||
| Dairy (0–10) | 7.16 | 7.50 | 7.40 | 7.31 | 7.29 |
| CI | (−0.2, 0.8) | (−0.1, 0.8) | (−0.4, 0.6) | ||
| Other measures | |||||
| Energy intake (kcal/day)g | 1233 | 1194 | 1153 | 1158 | 1199 |
| CI | (−125, 14) | (−131, 16) | (−129, 1) | ||
| Weight-for-age percentile | 66.5 | 59.9 | 59.4** | 61.8 | 63.3 |
| CI | (−5.5, 1.2) | (−8.8, −2.0) | (−4.6, 1.3) | ||
| BMI-for-age percentile | 76.2 | 70.2 | 66.7*** | 72.0 | 72.8 |
| CI | (−5.9, 3.0) | (−12.6, −3.5) | (−5.1, 2.9) | ||
| Percent overweight/obese | 50.2 | 34.4 | 41.8 | 41.2 | 44.1 |
| CI | (−1, 34) | (−10, 26) | (−10, 27) |
Values shown are from the baseline measurement adjusted for covariates of sex, migrant status, and age
n=237
State 1 = low levels of parent-centered feeding and moderate levels of child-centered feeding, State 2 = high levels of parent and child-centered feeding, with the absence of physically struggling to get the child to eat, State 3 = high levels of both parent and child-centered feeding, and State 4 = moderate usage of both parent and child-centered feeding strategies
State 1 = referent; asterisks indicate significant difference compared to State 1 with
p <0 .05,
p <0 .01, and
p <0 .001
Higher scores indicate healthier diet and less deviation from the ideal standard
CI: 95% confidence interval for the difference from referent group
Total kilocalories per day from three 24-hour dietary recalls
The mean BMI percentile of the total sample at baseline was 72.8 (95% CI=(70.0, 75.6)). However, the mean BMI percentile of the high PC/CC state was significantly lower compared to the low PC/moderate CC state (66.7 percentile versus 76.2 percentile, p < 0.001). Although the difference did not reach statistical significance, 50.2% of children in the low PC/moderate CC state were overweight or obese compared to 34.4% in high PC/CC without physical control, 41.8% in high PC/CC, and 41.2% in the moderate PC/CC state. States did not differ significantly in terms of energy intake.
Discussion
Dietary Guidelines for Americans two years and older recommend consumption of fruits, vegetables, whole grains, low-fat dairy, and lean meats without excessive calories from saturated fat or sugar.39 A significant percentage of children in the United States do not meet recommendations, and this is particularly true for Latinos.6,40–42 Recent data indicate low intake of fruit and vegetables.5,42,43 Consumption of sugar-sweetened beverages and fast food has also been reported to be significantly higher among young Latino children relative to white children.44
To study the dynamic between feeding style and dietary outcomes as well as obesity, the HMM was applied to the data and four distinct states – low PC/moderate CC, high PC/CC without physical control, high PC/CC, and moderate PC/CC – were delineated. The HMM approach revealed qualitatively different states of feeding style and possible transitions. This type of information is not available when the scaled score is used to order the families on a continuum. Based on the degree of responsiveness and demandingness, the low PC/moderate CC state was deemed indulgent in nature. The low PC/moderate CC style was most prevalent and increased in size over the course of the study. It was associated with several poor dietary outcomes, including high intake of added sugar and low consumption of whole grains and vegetables, although fat intake showed the opposite relationship. This group also had the highest BMI-percentile and weight-percentile.
In the first study to use the CFSQ, 231 children (130 Hispanic, 101 African American) enrolled in Head Start were surveyed.14 In this sample, most Hispanic parents were considered to use either authoritarian (n=49) or indulgent (n=50) feeding styles. They observed that children fed in an indulgent manner had higher BMI z scores relative to children whose parents practiced an authoritarian feeding style. Although there were differences in terms of the proportion of families that could be considered indulgent versus authoritarian, an association with increased BMI and indulgent feeding style was also found among the children enrolled in the Niños Sanos study.
In the years since Hughes et al. initially developed the CFSQ, multiple studies have observed that an indulgent feeding style is associated with overweight and obesity,17,27,45 and with unfavorable intake of specific types of food. At least one study has indicated children of indulgent parents consume fewer fruits, vegetables, and dairy products compared to children of authoritarian parents.20 In a study of United States immigrants, children of low demanding/high responsive mothers consumed less whole grains than children whose mothers were high demanding/high responsive, but only if mothers had been in the country for less than 5 years.46 A permissive feeding style has also been linked to higher intake of low-nutrient-dense foods.47 The results here generally support these findings and add to the cohesiveness of research on feeding style.17,27,45
The fact that fat intake was more favorable for low PC/moderate CC families was surprising. Fat intake showed the opposite trend of other dietary outcomes and may have been modified by age. Older children were both significantly more likely to have more favorable fat intake and to belong to the low PC/moderate CC state (p < .05) (data not shown). Why older children had better fat intake is not yet clear, but may reflect their enrollment in preschools and schools that regulate fat content of meals.
The finding that the relatively authoritarian high PC/CC feeding style was not associated with less favorable intake of vegetables and whole grains, and higher BMI, compared to the relatively authoritative high PC/CC without physical control feeding style was surprising, although high PC/CC without physical control did have the lowest percentage of overweight and obese children. An authoritative parenting style has consistently been associated with best outcomes for children in a variety of outcomes ranging from school achievement to drug use to weight status.48–50 An authoritative parenting style sets firm limits on children’s behavior, but also uses reasoning and negotiation with the child.51,52 This leads to internalization of parental values and beliefs and guides the child even when parents are absent. In contrast, the authoritarian parenting style uses demands, threats, rewards and punishments to ensure child compliance. This may lead to externalization of parental values – the child does as the parent wants to avoid punishment but may act differently when parents are absent. Evidence suggests that authoritarian feeding practices (e.g., restriction, pressure to eat) may lead to poor outcomes regarding children’s diet; for example, a child may not learn to respond to her internal sense of hunger and satiety, leading to overeating53, or, a child may actually learn to prefer “forbidden foods” and select these foods when parents are absent.54 Studies have linked authoritarian practices to poor dietary outcomes.50,55
Given the similarity in responsiveness and demandingness scores, the most notable difference between the two high PC/CC states was the use of physical struggling to get children to eat. This approach may ensure short-term compliance in young children, but it may lead to long-term negative consequences for the child.56 It is unlikely sustainable, given the findings here on state dynamics and trajectories (as the child develops physically, struggling is less viable). It is also possible that parents who practice an authoritarian feeding style are not authoritarian in other parenting contexts. Evidence suggests certain parental feeding practices are predictive of general parenting style57, but in one study, parenting style and feeding style only matched in one third of families.18 An authoritarian feeding style may not share the negative connotations of an authoritarian parenting style. Alternatively, the authoritarian feeding style may be beneficial primarily for young children and lose effectiveness as children age. The different outcomes between the high PC/CC states in this study must be interpreted cautiously, and further research is needed to better understand the implications of these feeding styles in different populations, such as older children.
Another notable finding was the change in state prevalence over time. Several studies have noted that indulgent and authoritarian feeding styles are most common; however, at the end of the study it was noted that very few parents belonged to the relatively authoritarian State 3. Children entered the study between the ages of 2.5 and 3.5 and completed the study between the ages of 4.5 and 5.5. Undoubtedly, many significant developmental milestones occur during these years, and the declining authoritarian state may reflect the development process – as children grow more autonomous and make more decisions independently, parental control wanes. However, some studies using the CFSQ measured children over the age of 6 and still identified the authoritarian style as relatively common.15,18 For example in the Live Well study,15 15% mothers were found to be authoritative and 32% authoritarian. The discrepant findings may be due to methodological differences in the classification of feeding style or differences in the population studied. Previous studies tended to use median splits to classify parents as high or low in terms of demandingness and responsiveness, while cutoff scores were used in the present study. Median splits may force parents into high and low categories such that some parents who are actually fairly low in terms of demandingness are classified as high demanding, because the sample as a whole is low in demandingness and they are only relatively higher in this regard.
It is worth pointing out that the HMM-based method, unlike earlier methods, does not require pre-specified criteria such as median split for categorizing feeding styles. As a data driven method, the HMM delineates heterogeneity in feeding style using longitudinal data. While the method can bring new insight into feeding style typology, findings from HMM may not be directly comparable to other studies. Although there are similarities (e.g., high PC/CC without physical control is authoritative in nature), no state was identified as “uninvolved” using cutoff scores. All four states used at least moderate levels of child-centered strategies, limiting insight into the effects of low versus high levels of child-centered feeding.
Other limitations of this study should be noted. First, the study was limited to the use of a questionnaire in its ability to capture the dynamics of the caregiver’s interaction with the child. Second, measuring children’s dietary intake is known to be challenging.58,59 Recall bias and social desirability bias may have affected mothers’ reporting. In some instances, mothers relied upon children’s other caregivers to report diet. Direct observation, use of food diaries, or other methods might be more valid, but also create opportunities for parental distortion of diet from usual intake, and were not suitable to the study. Third, only mothers’ and not the other parents’ feeding styles were measured. Fourth, the use of multiple strategies for study recruitment could have resulted in a sample not representative of the farmworker population.
Although findings may not generalize to different populations, a strength of the study is the inclusion of a large sample of North Carolina Latino farmworker families, an underserved and understudied population. Another strength of the study is the application of novel methodology (HMM) to an extensive longitudinal dataset, illuminating change in feeding style over time. Given that few studies have examined feeding style longitudinally, future studies should explore this topic in other populations. Future research should also seek to elucidate parental characteristics that predict feeding style, such as level of education.60
Conclusions
Consistent with a growing body of evidence, Latino farmworker children whose parents exhibited little parent-centered feeding and were relatively indulgent in nature had lower diet quality and higher mean BMI percentiles relative to children whose parents fed them in a high parent/high child-centered fashion. Encouraging indulgent parents to incorporate more high parent/high child-centered feeding strategies could potentially improve children’s diet quality and lower their risk of obesity. Future research should determine the degree to which feeding style is mutable, and whether encouraging high parent/high child-centered strategies benefits children’s weight and dietary outcomes. Such research should account for the unique circumstances of Latino farmworker families, many of which contend with poverty, lack of education, discrimination, limited accessed to nutrition food, deficiency of safe play spaces, frequent relocation, and acculturative stress.
Acknowledgments
Sources of funding:
This research was supported by grant R01HD059855 from the National Institute for Child Health and Human Development, grant 1R01HL101066 from the National Heart, Lung, and Blood Institute, UL1TR001420 from the National Center for Advancing Translational Sciences, and grant SES-1229549 from the National Science Foundation.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Contributor Information
Edward H. Ip, Department of Biostatistical Sciences, Division of Public Health Sciences, Wake Forest School of Medicine, Address: Medical Center Blvd, Winston-Salem NC, 27157, Phone number: (336) 716-9833, Fax number: eip@wakehealth.edu.
Sarah A. Marshall, Department of Biostatistical Sciences, Division of Public Health Sciences, Wake Forest School of Medicine, Address: 525 Vine St, Winston-Salem NC, 27101, Phone number: (336) 345-4465, Fax number: samarsha@wakehealth.edu.
Thomas A. Arcury, Department of Family and Community Medicine, Wake Forest School of Medicine, Address: Medical Center Blvd, Winston-Salem NC, 27157, Phone number: (336) 716-9438, Fax number: (336) 716-3206, tarcury@wakehealth.edu.
Cynthia K. Suerken, Department of Biostatistical Sciences, Division of Public Health Sciences, Wake Forest School of Medicine, Address: Medical Center Blvd, Winston-Salem NC, 27157, Phone number: (336) 713-1348, Fax number: (336) 713-5308, csuerken@wakehealth.edu.
Grisel Trejo, Wake Forest School of Medicine, Address: Medical Center Blvd, Winston-Salem NC, 27157, Phone number: (336) 716-2830, Fax number: gtrejo@wakehealth.edu.
Joseph A. Skelton, Department of Pediatrics, Wake Forest School of Medicine, Address: Medical Center Blvd, Winston-Salem NC, 27157, Phone number: (336) 713-2348, Fax number: (336) 713-7841, jskelton@wakehealth.edu.
Sara A. Quandt, Department of Epidemiology and Prevention, Division of Public Health Sciences, Wake Forest School of Medicine, Address: Medical Center Blvd, Winston-Salem NC, 27157, Phone number: (336) 716-6015, Fax number: (336) 713-4300, squandt@wakehealth.edu.
References
- 1.Ogden CL, Carroll MD, Lawman HG, Fryar CD, Kruszon-Moran D, Kit BK, Flegal KM. Trends in obesity prevalence among children and adolescents in the United States, 1988–1994 through 2013–2014. JAMA. 2016;315(21):2292–2299. doi: 10.1001/jama.2016.6361. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Rosado JI, Johnson SB, McGinnity KA, Cuevas JP. Obesity among Latino children within a migrant farmworker community. Am J Prev Med. 2013;44(3, Suppl 3):S274–S281. doi: 10.1016/j.amepre.2012.11.019. [DOI] [PubMed] [Google Scholar]
- 3.Kilanowski JF, Ryan-Wenger NA. Health status in an invisible population: carnival and migrant worker children. West J Nurs Res. 2007;29(1):100–120. doi: 10.1177/0193945906295484. [DOI] [PubMed] [Google Scholar]
- 4.Mines R. Children in immigrant and nonimmigrant farmworker families. In: Hernandez DJ, editor. Children of immigrants: health, adjustment and public assistance. Washington: National Academy Press; 1999. pp. 620–658. [PubMed] [Google Scholar]
- 5.Quandt SA, Trejo G, Suerken CK, Pulgar CA, Ip EH, Arcury TA. Diet quality among preschool-age children of Latino migrant and seasonal farmworkers in the United States. J Immigr Minor Health. 2016;18(3):505–512. doi: 10.1007/s10903-015-0304-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Quandt SA, Grzywacz JG, Trejo G, Arcury TA. Nutritional stategies of Latino farmworker families with preschool children: identifying leverage points for obesity prevention. Soc Sci Med. 2014;123:72–81. doi: 10.1016/j.socscimed.2014.10.029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Grzywacz JG, Arcury TA, Trejo G, Quandt SA. Latino mothers in farmworker families’ beliefs about preschool children’s physical activity and play. J Immigr Minor Health. 2016;18(1):234–242. doi: 10.1007/s10903-014-9990-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Caidez V, Townsend M, Kaiser LL. Toddler-feeding practices among Mexican American mothers. A qualitative study. Appetite. 2011;56:629–632. doi: 10.1016/j.appet.2011.02.015. [DOI] [PubMed] [Google Scholar]
- 9.Contento IS, Basch C, Zybert P. Body image, weight, and food choices of Latina women and their children. J Nutr Behav. 2003;35(5):236–248. doi: 10.1016/s1499-4046(06)60054-7. [DOI] [PubMed] [Google Scholar]
- 10.Ip EH, Saldana S, Arcury TA, Grzywacz JG, Trejo G, Quandt SA. Profiles of food security for US farmworker households and factors related to dynamic of change. Am J Public Health. 2015;105(10):e42–47. doi: 10.2105/AJPH.2015.302752. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Weathers A, Minkovitz C, O’Campo P, Diener-West M. Access to care for children of migratory agricultural workers: factors associated with unmet need for medical care. Pediatrics. 2004;113(4):e276–282. doi: 10.1542/peds.113.4.e276. [DOI] [PubMed] [Google Scholar]
- 12.Weathers AC, Minkovitz CS, Diener-West M, O’Campo P. The effect of parental immigration authorization on health insurance coverage for migrant Latino children. J Immigr Minor Health. 2008;10(3):247–254. doi: 10.1007/s10903-007-9072-8. [DOI] [PubMed] [Google Scholar]
- 13.Arcury TA, Skelton JA, Ip EH, Suerken CK, Trejo G, Quandt SA. Anticipatory guidance about child diet and physical activity for Latino farmworker mothers. J Health Care Poor Underserved. 2016;27(3):1064–1079. doi: 10.1353/hpu.2016.0136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Hughes SO, Power TG, Orlet Fisher J, Mueller S, Nicklas TA. Revisiting a neglected construct: parenting styles in a child-feeding context. Appetite. 2005;44(1):83–92. doi: 10.1016/j.appet.2004.08.007. [DOI] [PubMed] [Google Scholar]
- 15.Tovar A, Hennessy E, Pirie A, Must A, Gute DM, Hyatt RR, et al. Feeding styles and child weight status among recent immigrant mother-child dyads. Int J Behav Nutr Phys Act. 2012 doi: 10.1186/1479-5868-9-62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Hughes SO, Anderson CB, Power TG, Micheli N, Jaramillo S, Nicklas TA. Measuring feeding in low-income African-American and Hispanic parents. Appetite. 2006;46(2):215–223. doi: 10.1016/j.appet.2006.01.002. [DOI] [PubMed] [Google Scholar]
- 17.Shloim N, Edelson LR, Martin N, Hetherington MM. Parenting styles, feeding styles, feeding practices, and weight status in 4–12 year-old children: a systematic review of the literature. Front Psychol. 2015 doi: 10.3389/fpsyg.2015.01849. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Hennessy E, Hughes SO, Goldberg JP, Hyatt RR, Economos CD. Parent behavior and child weight status among a diverse group of underserved rural families. Appetite. 2010;54(2):369–377. doi: 10.1016/j.appet.2010.01.004. [DOI] [PubMed] [Google Scholar]
- 19.Hughes SO, Shewchuk RM, Baskin ML, Nicklas TA, Qu H. Indulgent feeding style and children’s weight status in preschool. J Dev Behav Pediatr. 2008;29(5):403–410. doi: 10.1097/DBP.0b013e318182a976. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Hoerr SL, Hughes SO, Fisher JO, Nicklas TA, Liu Y, Shewchuk RM. Associations among parental feeding styles and children’s food intake in families with limited incomes. Int J Behav Nutr Phys Act. 2009 doi: 10.1186/1479-5868-6-55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Ventura AK, Gromis JC, Lohse B. Feeding practices and styles used by a diverse sample of low-income parents of preschool-age children. J Nutr Educ Behav. 2010;42(4):242–249. doi: 10.1016/j.jneb.2009.06.002. [DOI] [PubMed] [Google Scholar]
- 22.Hughes SO, Power TG, Papaioannou MA, Cross MB, Nicklas TA, Hall SK, et al. Emotional climate, feeding practices, and feeding styles: an observational analysis of the dinner meal in Head Start families. Int J Behav Nutr Phys Act. 2011 doi: 10.1186/1479-5868-8-60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Patrick H, Nicklas TA, Hughes SO, Morales M. The benefits of authoritative feeding style: caregiver feeding styles and children’s food consumption patterns. Appetite. 2005;44(2):243–249. doi: 10.1016/j.appet.2002.07.001. [DOI] [PubMed] [Google Scholar]
- 24.Kaiser LL, Melgar-Quinonez HR, Lamp CL, Johns MC, Harwood JO. Acculturation of Mexican-American mothers influences child feeding strategies. J Am Dietet Assoc. 101(5):542–547. doi: 10.1016/S0002-8223(01)00136-5. [DOI] [PubMed] [Google Scholar]
- 25.White RMB, Roosa MW, Weaver SR, Nair RL, McBride Murry V. Cultural and contextual influences on parenting in Mexican American families. J Marriage Fam. 2009;71(1):61–79. doi: 10.1111/j.1741-3737.2008.00580.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Martinez SM, Rhee K, Blanco E, Boutelle K. Maternal attitudes and behaviors regarding feeding practices in elementary school-aged Latino children: A pilot qualitative study on the impact of the cultural role of mothers in the US-Mexican border region of San Diego, California. J Acad Nutr Diet. 2014;114(2):230–237. doi: 10.1016/j.jand.2013.09.028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Vollmer RL, Mobley AR. Parenting styles, feeding styles, and their influence on child obesogenic behaviors and body weight. A Review. Appetite. 2013;71:232–241. doi: 10.1016/j.appet.2013.08.015. [DOI] [PubMed] [Google Scholar]
- 28.NIH Certificates of Confidentiality. https://humansubjects.nih.gov/coc/index. Accessed March 2, 2017.
- 29.NDS-R. Version 2011. Minneapolis, MN: Nutrition Coordinating Center; 2011. [Google Scholar]
- 30.Hughes SO, Cross MB, Hennessy E, Tovar A, Economos CD, Power TG. Caregiver’s Feeding Styles Questionnaire. Establishing cutoff points. Appetite. 2012;58(1):393–395. doi: 10.1016/j.appet.2011.11.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Kranz S, Hartman T, Siega-Riz AM, Herring AH. A diet quality index for American preschoolers based on current dietary intake recommendations and an indicator of energy balance. J Am Diet Assoc. 2006;106(10):1594–1604. doi: 10.1016/j.jada.2006.07.005. [DOI] [PubMed] [Google Scholar]
- 32.Ohlsson C, Lorentzon M, Norjavaara E, Kindblom JM. Age at adiposity rebound is associated with fat mass in young adult males—The GOOD Study. PLoS One. 2012;7(11):e49404. doi: 10.1371/journal.pone.0049404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Kiang L, Ip EH. Longitudinal profiles of eudaimonic well-being in Asian American adolescents cultural diversity and ethnic minority psychology. Cultur Divers Ethnic Minor Psychol. doi: 10.1037/cdp0000156. In press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Naggara O, Raymond J, Guilbert F, Roy D, Weill A, Altmann DG. Analysis by categorizing or dichotomizing continuous variables is inadvisable: an example from the natural history of unruptured aneurysms. AJNR Am J Neuroradiol. 2011;32(3):437–440. doi: 10.3174/ajnr.A2425. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Ip EH, Zhang Q, Rejeski J, Harris T, Kritchevsky S. Partially ordered mixed hidden Markov model for the disablement process of older adults. J Am Stat Assoc. 2013;108(502):370–384. doi: 10.1080/01621459.2013.770307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Ip EH, Zhang Q, Schwarz R, Tooze J, Leng X, Hong M, et al. Multi-profile hidden Markov model for mood, dietary intake, and physical activity in an intervention study of childhood obesity. Stat Med. 2013;32(19):2213–2241. doi: 10.1002/sim.5719. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Dynamic Multichain Graphical Modeling Tool. website http://dmgm.wfuhs.arane.us/. Updated January 20, 2017. Accessed March 2, 2017.
- 38.SAS (for Windows) [computer program]. Version 9.3. Cary, NC.: SAS Inc.; 2017. [Google Scholar]
- 39.U.S. Department of Health and Human Services and U.S. Department of Agriculture. 2015–2020 Dietary Guidelines for Americans. (8th) http://health.gov/dietaryguidelines/2015/guidelines/. Accessed December 15, 2015.
- 40.Muñoz KA, Krebs-Smith SM, Ballard-Barbash R, Cleveland LE. Food intakes of US children and adolescents compared with recommendations. Pediatrics. 1997;100(3, pt 1):323–329. doi: 10.1542/peds.100.3.323. [DOI] [PubMed] [Google Scholar]
- 41.Krebs-Smith SM, Cook A, Subar AF, Cleveland L, Friday J, Kahle LL. Fruit and vegetable intakes of children and adolescents in the United States. Arch Pediatr Adolesc Med. 1996;150(1):81–86. doi: 10.1001/archpedi.1996.02170260085014. [DOI] [PubMed] [Google Scholar]
- 42.Erinosho TO, Berrigan D, Thompson FE, Moser RP, Nebeling LC, Yaroch AL. Dietary intakes of preschool-aged children in relation to caregivers’ race/ethnicity, acculturation, and demographic characteristics: results from the 2007 California Health Interview Survey. Matern Child Health J. 2012;16(9):1844–1853. doi: 10.1007/s10995-011-0931-5. [DOI] [PubMed] [Google Scholar]
- 43.Dave JM, Evans AE, Saunders RP, Watkins KW, Pfeiffer KA. Associations among food insecurity acculturation, demographic factors, and fruit and vegetable intake at home in Hispanic children. J Am Diet Assoc. 2009;109(4):697–701. doi: 10.1016/j.jada.2008.12.017. [DOI] [PubMed] [Google Scholar]
- 44.de Hoog ML, Kleinman KP, Gillman MW, Vrijkotte TG, van Eijsden M, Taveras EM. Racial/ethnic and immigrant differences in early childhood diet quality. Public Health Nutr. 2014;17(6):1308–1317. doi: 10.1017/S1368980013001183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.El-Behadili AF, Sharp C, Hughes SO, Obasi EM, Nicklas TA. Maternal depression, stress and feeding styles: towards a framework for theory and research in child obesity. Br J Nutr. 2015;113:855–871. doi: 10.1017/S000711451400333X. [DOI] [PubMed] [Google Scholar]
- 46.Tovar A, Choumenkovitch SF, Hennessy E, Boulos R, Must A, Hughes SO, et al. Low demanding parental feeding style is associated with low consumption of whole grains among children of recent immigrants. Appetite. 2015;95:211–218. doi: 10.1016/j.appet.2015.06.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Hennessy E, Hughes SO, Goldberg JP, Hyatt RR, Economos CD. Permissive parental feeding behavior is associated with an increase in intake of low-nutrient-dense foods among American children living in rural communities. J Acad Nutr Diet. 2012;112:142–148. doi: 10.1016/j.jada.2011.08.030. [DOI] [PubMed] [Google Scholar]
- 48.Steinberg L, Dornbusch SM, Brown BB. Ethnic differences in adolescent achievement. An ecological perspective. Am Psychol. 1992;47(6):723–729. doi: 10.1037//0003-066x.47.6.723. [DOI] [PubMed] [Google Scholar]
- 49.Hoffman JP, Bahr SJ. Parenting style, religiosity, peer alcohol use, and adolescent heavy drinking. J Stud Alcohol Drugs. 2014;75(2):222–227. doi: 10.15288/jsad.2014.75.222. [DOI] [PubMed] [Google Scholar]
- 50.Rhee KE, Lumeng JC, Appugliese DP, Kacirot N, Bradley RH. Parenting styles and overweight status in first grade. Pediatrics. 2006;117(6):2047–2054. doi: 10.1542/peds.2005-2259. [DOI] [PubMed] [Google Scholar]
- 51.Baumrind D. Effects of authoritative parental control on child behavior. Child Development. 1966;37(4):887–907. [Google Scholar]
- 52.Maccoby E, Martin J. Socialization in the context of the family: parent-child interaction. In: Hetherington E, editor. Handbook of Child Psychology: Socialization, Personality and Social Development. New York, NY: Wiley; 1983. pp. 1–101. [Google Scholar]
- 53.Birch LL. The acquisition of food acceptance patterns in children. In: Boakers RA, Popplewell DA, Burton MJ, editors. Eating habits: Food, physiology and learned behavior. London: Wiley; 1987. [Google Scholar]
- 54.Fisher JO, Birch LL. Restricting access to palatable food affects children’s behavioral response, food selection, and intake. Am J Clin Nutr. 1999;69(6):1264–1272. doi: 10.1093/ajcn/69.6.1264. [DOI] [PubMed] [Google Scholar]
- 55.Birch LL, Fisher JO. Mothers’ child-feeding practices influence daughters’ eating and weight. Am J Clin Nutr. 2000;71(5):1054–1061. doi: 10.1093/ajcn/71.5.1054. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Ateah CA, Secco ML, Woodgate RL. The risks and alternatives to physical punishment use with children. J Pediatr Health Care. 2003;17(2):126–132. doi: 10.1067/mph.2003.18. [DOI] [PubMed] [Google Scholar]
- 57.Hubbs-Tait L, Kennedy TS, Page MC, Topham GL, Harrist AW. Parental feeding practices predict authoritative, authoritarian, and permissive parenting styles. J Am Diet Assoc. 2008;108(7):1154–1161. doi: 10.1016/j.jada.2008.04.008. [DOI] [PubMed] [Google Scholar]
- 58.Cade JE, Burley VJ, Warm DL, Thompson RL, Margetts BM. Food-frequency questionnaires: a review of their design, validation and utilisation. Nutr Res Rev. 2004;17(1):5–22. doi: 10.1079/NRR200370. [DOI] [PubMed] [Google Scholar]
- 59.Christian MS, Evans CE, Nykjaer C, Hancock N, Cade JE. Measuring diet in primary school children aged 6–11 years: validation of the Child and Diet Evaluation Tool (CADET) with an emphasis on fruit and vegetable intake. Eur J Clin Nutr. 2015;69(2):234–241. doi: 10.1038/ejcn.2014.160. [DOI] [PubMed] [Google Scholar]
- 60.Saxton J, Carnell S, van Jaarsveld CH, Wardle J. Maternal education is associated with feeding style. J Am Diet Assoc. 2009;109(5):894–898. doi: 10.1016/j.jada.2009.02.010. [DOI] [PubMed] [Google Scholar]