

Abstract
Background
An extensive body of literature has demonstrated that many patients who have been asked to participate in clinical trials do not fully understand the informed consent forms. A parallel independent study has demonstrated that opposites have a special status in human cognitive organization: they are common to all-natural languages and are intuitively and naturally understood and learnt.
Purpose
The study investigates whether, and how, the use of opposites impacts on doctor–patient communication: does using the terms “small–large” to describe a nodule (ie, bipolar communication) rather than speaking in terms of centimeters (ie, unipolar communication) affect a patient’s understanding of the situation? And is it better to speak of “common–rare” side effects (ie, bipolar communication) instead of the number of people who have suffered from particular side effects (ie, unipolar communication)?
Methods
Two questionnaires were created and used, one presenting the information in terms of opposites (ie, bipolar communication) and another using unipolar communication.
Results
The participants’ perception of their situation (in terms of feeling healthy–ill, being at high–low risk, and their treatment requiring high–low commitment) varied in the two conditions. Moreover, self-reported levels of understanding and satisfaction with how the information was communicated were higher when opposites were used.
Limitations
Since this is the first study that addresses the merits of using bipolar structures versus unipolar structures in doctor–patient communication, further work is needed to consolidate and expand on the results, involving not only simulated but also real diagnostic contexts.
Conclusion
The encouraging results imply that further testing of the use of opposites in informed consent forms and in doctor–patient communication is strongly advisable.
Keywords: opposites, bipolar, unipolar, informed consent, doctor–patient communication, understanding, satisfaction
Introduction
Clinical trials have a central role in terms of providing evidence to support oncologic treatments. In the USA, the National Cancer Institute (NCI) National Clinical Trials Network has estimated that between 19,000 and 20,000 patients enrolled in clinical trials in 2016, and the number of participants in the European Union has substantially increased over the past decade (revision of the “Clinical Trials directive”, 2011).1 Informed consent is an important part of the enrollment process. Ethical aspects related to informed consent include the completeness and adequacy of the information provided. An extensive body of literature has demonstrated that many people do not understand the detailed information contained in informed consent forms and therefore are also to some extent unaware of the risks incurred by their exposure to the treatments.2–8 Comprehension of and satisfaction with informed consent forms are, in general, particularly limited in the case of people with a lower standard of secondary education, even when simple language is used.9–11
Deciding to take part in a clinical trial is an individual choice. However, participation rates in clinical trials for cancer treatments are affected not only by a patient’s attitudes toward the trial but also by the organizer’s ability to communicate with the patient.12–14 A variety of strategies such as short films, phone- or web-based decision aiding tools, and supplementary discussions with a member of the research team who is not a physician have been proposed as a way of improving patient knowledge and increasing their understanding of informed consent forms.15–25 In any case, it has been generally acknowledged that it is necessary to develop strategies to improve the communication skills of the organizers of clinical trials.9,16,26
From cognitive dimensions to communication: the role of opposites
The way in which information is presented for the purposes of informed consent, and in doctor–patient communication in general, usually ignores the fact that humans perceive,27–32 conceptualize,33–35 and linguistically describe36–38 their experiences in terms of opposites.
It has been widely acknowledged that opposites have a special status in human cognitive organization. They play a significant role in the mental lexicon and are intuitively and naturally understood and learnt.39–43 They are primal schemas in cognitive development,44–48 and they constitute a primal relation in the perceptual experiences of adults.28,49–51
Given that opposites are primal and pervasive in direct experiences and natural language, our hypothesis is that they might also enhance the comprehension of information provided in a diagnostic context. If naïve subjects naturally process information in terms of polarized dimensions, they might also re-elaborate in terms of opposites what a doctor is saying. This would mean, for example, that when a doctor conveys information concerning the extent of an area affected by a disease in terms of centimeters, patients might carry out a real-time transformation in their minds in terms of small (at various gradations) versus big (at various gradations). Similarly, when information concerning the number of treatment sessions that are required or the duration of the treatment or the number of instances when serious side effects occur is given, patients might recode these pieces of information in terms of few–many sessions, long–short duration, and rare–common incidences of serious side effects, respectively. If this is the picture that they mentally establish while listening to the doctor, it will probably also be the internal mind-set they will use to re-narrate the situation to themselves and to their relatives and friends, thus consolidating this mental representation. The latter is, of course, a hypothesis that can and should be tested experimentally. In the context of this study, we take this hypothesis as a general framework and will also test some related hypotheses. But before presenting these in detail, we want to clarify that in this paper, when we speak of bipolar dimensions or opposites, we do not mean binary dimensions or binary oppositions (ie, dimensions formed by only two values). From a perceptual and cognitive point of view, bipolar dimensions are usually mentally graded at one or both poles, and in most of the cases, there are also intermediate experiences that are identified as being “neither one pole, nor the other”, for example, neither big nor small, neither long nor short, neither painful nor pleasant, etc.27,29–31 In this sense, opposites are not simplistic structures that cannot support intensity gradations. As such, they do not contrast the modulated communication required in oncological diagnoses; they simply locate these modulations in a polarized frame which is more natural and therefore easier to understand.
The study
Aims
To the best of our knowledge, the present study is the first to evaluate the role of opposites in modeling the understanding of medical information. Specifically, using a simulated oncologic diagnostic context, we investigated how a person’s perception of his/her health condition and the risks and commitment relating to any treatment required varies when information is communicated using opposite terms (eg, rare–common, small–big) as opposed to unipolar linguistic structures (see below the two different types of unipolar structures commonly associated with “4-item configurations” and “3-item configurations”). If a doctor talks of a small–large nodule (ie, a bipolar structure) instead of talking in terms of centimeters (ie, a unipolar structure) or of common–rare side effects (ie, bipolar) instead of talking of the number of people who suffer a particular side effect (ie, unipolar), how does this impact on the patient’s understanding?
In particular, we will investigate the following:
Any changes in the patient’s perception of being healthy versus ill, at low versus high risk, and feeling slightly versus maximally committed to the treatment when information is provided with as compared to without reference to opposites.
Any differences between the two cases in the overall satisfaction with how the information was communicated and in self-reported levels of understanding.
Since clear understanding of the situation is essential not only for ethical reasons but also to guarantee the patient’s conscious involvement in all the phases of the treatment, higher ratings of self-reported understanding and satisfaction with how the information is conveyed will be regarded as desirable results. Similarly, since the patient’s active engagement is considered essential in cases of oncologic diseases in terms of facing the situation and making decisions regarding the treatment, enhancing the person’s “arousal” (within a reasonable range) has to be considered desirable.
Methods
Preliminary phase
A set of basic information to be communicated was defined, and two questionnaires to be used in the main research phase were created.
Using inter-observation sessions (with a total of 22 hours of inter-observation), three experts (U Savardi, I Bianchi and R Burro, all authors of this paper) analyzed the contents of various standard informed consent forms and studied a series of videos produced by the psychology department and medical staff of the National Cancer Institute CRO (Aviano, Italy). These videos simulate typical, realistic dialogues between doctors and patients in diagnostic and follow-up settings. The “patient” was an adult female (an actress) who interacted with 10 real doctors (employed at the CRO Institute) in various role-play settings corresponding to first diagnosis, treatment, and follow-up. The videos were judged by the members of the research group working in the CRO institution (Drs M A Annunziata and P De Paoli) to be highly realistic in that they represented typical conversations. The analysis revealed a systematic lack of attention with regard to whether information was conveyed using bipolar or unipolar structures. Other aspects were clearly important to the doctors as seen in the videos, such as their desire to convey information concerning the patient’s situation and the proposed treatment and to establish the right empathic approach with a view to actively involve patients in the decision-making process. But the two types of structure (bipolar and unipolar) varied randomly within the conversations.
A list of statements were drawn up by the three experts, which included the various types of information frequently referred to by the doctors and enquired about by the patients in the videos in addition to the information found in standard informed consent forms. In order to establish a set of stimuli, corresponding versions of each piece of information were created following two criteria as described below using the terms “4-item configuration” and “3-item configuration”. These correspond to the two alternative ways in which one can give information without mentioning opposites. For example, instead of saying that “the tests revealed the existence of a large nodule” or “of a small nodule”, that is, communicating by means of opposites, the doctor might report the size of the nodule in centimeters (in this way to avoid any references to opposites) or he/she might simply say that “the tests revealed the existence of a nodule”, without mentioning the size, and again avoiding any references to opposites. But in the latter case, by not providing any information which would shift the balance toward one or the other pole, the communications remains – at least in theory – in a neutral position.
1. 4-item configuration (Figure 1A). For each two bipolar item, there were two items expressing the same information using a unipolar scale, hence the term “4-item configuration”. For example, the two items with information concerning the size of a nodule which are expressed in bipolar terms by means of small–large (eg, “The medical tests have revealed the presence of a small nodule”; “The medical tests have revealed the presence of a large nodule”) were expressed in centimeters in the corresponding unipolar version (eg, “The medical tests have revealed the presence of a nodule of 1 cm”; “The medical tests have revealed the presence of a nodule of 7 cm”). Information concerning survival rates which was expressed in terms of high–low in the bipolar version (eg, “There are low survival rates associated with this disease”; “There are high survival rates associated with this disease”) was expressed in percentages in the unipolar version (eg, “There is a 30% survival rate associated with this disease”; “There is a 70% survival rate associated with this disease”). The incidence of the disease in the population which was expressed in bipolar terms by rare–common (eg, “The nodule that you have is rare”; “The nodule that you have is common”) was expressed in the unipolar version as a proportion (eg, “The nodule that you have affects 1 in a million people”; “The nodule that you have affects 1 in a thousand people”).
Figure 1.

The two types of “correspondence” between unipolar and bipolar communication: the 4-item configuration (A) and the 3-item configuration (B). When opposites are used, one relates to the positive pole (+), the other to the negative pole (−).
Abbreviations: UNI, unipolar; BIP, bipolar.
2. 3-item configuration (Figure 1B). This is again a unipolar communication in that any references to either of the two poles is avoided. For example, the doctor informs the patient about the existence of a nodule (“The medical tests have revealed the presence of a nodule”) without specifying whether the nodule is benign or malignant. Similarly, the presence of side effects associated with the treatment is mentioned without any statement concerning whether the side effects are minor or severe (“The standard treatment for this tumor produces side effects”). Here we see that there is a single item in the unipolar version and two items in the bipolar version, hence the term “3-item configuration”.
Two different questionnaires were drawn up from this list of items, one containing only information expressed using unipolar structures (from now on, UNI) and comprising 34 items (20 items belonging to the 4-item configuration and 14 items belonging to the 3-item configuration) and the other containing only information expressed using bipolar structures (from now on, BIP) and comprising 48 items (20 items belonging to the 4-item configuration and 28 items belonging to the 3-item configuration).
The two sets of items are presented in Table S1. The issues addressed concerned the nature of the disease, the characteristics of the treatment, and the quality of life to be expected during and after treatment. In the BIP version, the statements included:
For the disease (nodule): small–large, benign–malignant, localized–widespread, common–rare, slow–quick progressing, high–low genetic predisposition, easy–hard to treat, high–low survival rates.
For the treatment: definitive–palliative, high–low efficacy, advisable–necessary, short–long duration, one–many cycle(s), outpatient–inpatient (hospitalization), high–low probability of side effects, minor–severe side effects, immediate–delayed onset of side effects, temporary–permanent duration of side effects.
For the quality of life: autonomous–assisted living during the treatment, autonomous–assisted living after the treatment, invariant–changed lifestyle during the treatment, invariant–changed lifestyle after the treatment, yes–no effect on the ability to work during the treatment, yes–no effect on the ability to work after the treatment.
Main phase
The two questionnaires (UNI, BIP) were presented individually to two different groups of Italian participants.
A hypothetical scenario was described in the instructions:
“Imagine that your doctor has recommended that you have some medical tests at a center specialized in oncologic diagnosis in order to ascertain whether or not you have a health problem. You have done the tests and now you are talking to the doctor who tells you what the situation is.
During the interview, he/she gives you various pieces of information. Express your judgment of each piece of information received in terms of
how healthy–ill you are
how high–low the risks involved in the treatment are
how high–low the commitment required by the treatment will be”.
Three ratings were given by participants using three continuous bipolar scales (100 mm long) which were defined at the extremes by the following labels: completely healthy–extremely ill (referring to the perception of the state of health, from now on H); zero risk–extremely high risk (referring to perception of risk, from now on R); low commitment–high commitment (referring to the perception of the commitment required by the treatment, from now on T).
Participants were instructed to consider each piece of information individually, in isolation from the previous statements and not cumulatively. “For example, if one sentence says something about the size of the nodule (eg, it’s small) and then the following sentence says something about whether it is benign/malignant (eg, it’s malignant), do not add this second piece of information to the first (ie, the doctor was saying that you have a small malignant nodule)”.
At the end of the questionnaire, participants were asked to rate (using a scale from 0% to 100%) how far they had understood the information provided (“How much of the information provided by the doctor do you think you understood?”) and their overall satisfaction regarding the clarity of the communication (“How satisfied are you with the clarity of communication?”).
Participants
A total of 470 Italian undergraduate students and adults were divided into two groups: 235 participated in the BIP condition, with the bipolar questionnaire (136 female and 99 male participants; mean age: 26.3 years, SD =8.44) and 235 participated in the UNI condition, with the unipolar questionnaire (143 female and 92 male participants; mean age: 25.5 years, SD =9.21). The study complied with the Helsinki ethics protocol and was approved by the Ethics Committee of the University of Verona (where the data were collected). Participants volunteered in the study. They were recruited in non-medical university faculties (in libraries, study halls, and the campus) and randomly assigned to one of the two conditions. Written informed consent was provided by each participant.
Statistical analyses
Responses were analyzed using mixed-effect models,52 with Gaussian family and identity link functions. In cases involving significant main effects or interactions, post hoc tests using the Bonferroni correction were conducted and estimates of the nonstandardized size of the effect (EST, ie, the regression coefficient) and Cohen’s index (d) as the standardized size of the effect were reported.53–56 Mixed regression assumptions (including the assumption that residuals are normally distributed and homoscedastic) were checked using quantile comparison and residual diagnostic plots. The goodness-of-fit of the linear mixed models (LMMs) was assessed using the conditional R2 index.57
All the analyses were carried out using the statistical software program R 3.3.1, with the “lme4”, “car”, “lsmeans”, and “effects” packages. We performed mixed model ANOVA tables (type 3 tests) via likelihood ratio tests implemented in the “afex” package.
Results
A series of analyses were conducted to assess whether changes in the participants’ perception of being healthy versus ill (health axis, H), at low versus high risk (risk axis, R), and feeling slightly versus maximally committed to the treatment (treatment axis, T) occurred when information was provided with or without reference to opposites.
General analysis
First, we studied whether and how the rating given by participants depended on the variables used in the study, that is, type of communication (BIP, UNI), the axes used for evaluating the information provided (H, R, T) and the configuration type (3-, 4-item configurations). A linear mixed model (Gaussian family) was carried out on the ratings given by participants to the entire set of items presented in the questionnaires, with type of communication, axes, and configuration type as fixed effects and participants as random effects. The assumptions of mixed regression models were verified (Figure 2). The conditional R2 index was equal to 0.34.
Figure 2.

Diagnostic plots used for testing the mixed regression assumptions concerning the analysis of the ratings (linear mixed model) as described in the main text.
Various significant effects emerged (Figure 3). The main effect of axes (χ2(2, N=470) =610.1556, p<0.0001; Figure 3A) suggested that the items elicited in general higher ratings on the axis relating to commitment to the treatment than on the other two axes.
Figure 3.

Effects of axes (H, R and T) and type of communication (BIP; UNI) on the ratings. The main effects are reported in (A and C). The interactions of each effect with configuration type (3-item, 4-item configuration) are shown in (B and D). Error bars represent a 95% confidence interval.
Abbreviations: BIP, bipolar; H, health; R, risk; T, commitment to the treatment; UNI, unipolar.
The interaction between axes and configuration type (χ2(2, N=470) =51.5146, p<0.0001, Figure 3B) revealed that for items with a 3-item configuration structure, the ratings in terms of risk and health did not differ (3R-3H: EST =0.053, SE =0.324, t-ratio =0.166, p=1.000, d=0.007; 3T-3H: EST =5.876, SE =0.324, t-ratio =18.132, p<0.0001, d=0.836; 3T-3R: EST =5.822, SE =0.324, t-ratio =17.966, p<0.0001, d=0.828), whereas in the 4-item configuration, structure ratings related to risk were higher than those given in the health axis (4R-4H: EST =1.238, SE =0.313, t-ratio =3.957, p<0.001, d=0.200; 4T-4H: EST =3.987, SE =0.313, t-ratio =12.735, p<0.0001, d=0.587; 4T-4R: EST =2.748, SE =0.313, t-ratio =8.777, p<0.0001, d=0.405).
Significantly (in terms of the hypothesis underlying this study), a main effect of type of communication also emerged (χ2(1, N=470) =11.089, p=0.0008, Figure 3C) suggesting that BIP ratings were higher than UNI ratings. However, there was a significant interaction between type of communication and configuration type (χ2(1, N=470) =323.025, p<0.0001), and this indicated that in the case of 4-item configurations, BIP communication was specifically associated with higher ratings than UNI communication (4-item: BIP vs UNI = EST =6.794, SE =1.096, t-ratio =6.198, p<0.0001, d=0.290) whereas with 3-item configurations no overall difference emerged (Figure 3D).
This initial analysis provided first indications that the ratings varied depending on whether a BIP or UNI communication type was used, but it also showed that the effect was modulated by the configuration type used. Further in-depth analyses were thus carried out separately on the subset of items characterized by a 4-item configuration and on the subset of items characterized by a 3-item configuration.
Analysis of the 4-item configuration type
By analyzing the responses to 4-item configurations, it was possible to test, first, whether information relating to the positive pole of a dimension elicited (as expected) a different perception in terms of health, risk, and commitment as compared to information relating to the negative pole of a dimension, and second, whether this depended on how the information was communicated, that is, by means of opposite terms (BIP) or without opposite terms (UNI). The ratings given to the 4-item configuration subset were analyzed using a linear mixed model (Gaussian family) with type of communication (UNI, BIP), axes (H, R, T), and type of information (positive, negative) as fixed effects and participants as random effect (conditional-R2 index =0.39).
Two main effects emerged, while none of the interactions turned out to be significant. The first main effect concerns type of information (χ2(1, N=470) =2,233.665, p<0.0001; Figure 4A), and this is, in a sense, an obvious result. The items that comprised negative news (ie, those which referred to the negative pole) led to higher ratings – a perception of greater risk, a more serious illness and a greater degree of commitment – than those which related to positive news (ie, those which referred to the positive pole).
Figure 4.

Plot of the main effect of type of information (negative pole, positive pole) on the ratings given by participants (A) and the interaction between type of communication (BIP, UNI) and type of information (B). Error bars represent a 95% confidence interval.
Abbreviations: BIP, bipolar; UNI, unipolar.
The second main effect is less obvious and is more central to the hypothesis being tested in this study. The ratings differed depending on the type of communication used (χ2(1, N=470) =38.097, p<0.0001). When polarized information was communicated by means of opposite terms (BIP), this led in general to higher ratings. This was true when information pertaining to both the positive and negative poles was concerned, as shown in Figure 4B. Indeed, the interaction between type of communication and type of information did not turn out to be significant: (χ2(1, N=470) =0.166, p=0.683).
A new analysis was conducted to further explore the differences between the two types of communication (BIP vs UNI). They were analyzed in more detail, and the ratings given to the corresponding BIP and UNI versions (ie, UNI positive pole vs BIP positive pole; UNI negative pole vs BIP negative pole) were matched item by item. This was done using Student’s t-test after assessing the normality of distributions by means of Shapiro’s test and the homogeneity/nonhomogeneity of variance by means of Levene’s parametric and Kruskal–Wallis’s non-parametric test. The outcomes of the tests were used to create a new categorical variable (items matching) on three levels: BIP>UNI (when the Student’s t-test turned out to be significant, with the UNI version receiving a significantly lower rating than the BIP version), BIP<UNI (when the Student’s t-test turned out to be significant, with the UNI version receiving a significantly higher rating than the BIP version), UNI=BIP (when the Student’s t-test turned out to be not significant, indicating that the two versions produced similar ratings). Mosaic plots58,59 were used to study and represent the frequency of the three categories of item matching (BIP>UNI, BIP=UNI, BIP<UNI), in association with the type of information (positive, negative) and axes (H, R, T) (Figure 5). A mosaic plot represents 1) the observed frequencies of a contingency table by means of the size of the tiles – in Figure 5, the raw frequencies are also reported by numbers on the tiles; 2) the interaction between variables by means of the asymmetrical non-alignment of the tiles; and 3) the significance of the difference between observed and expected frequencies according to a specific model (in our case a log-linear model of independence between variables) by means of the color of the tiles. The color of the tiles corresponds to Pearson residuals and the bars to the right of each mosaic show which color corresponds to residuals greater than the cutoff point |2| (corresponding to a p<0.05).
Figure 5.

Mosaic plot showing the frequency of the three possible outcomes when corresponding items in the BIP and UNI versions of the questionnaire are matched, with 4-item configurations (BIP>UNI, BIP=UNI, BIP<UNI). Twenty matches for the ratings given to corresponding items (10 referring to the positive pole, p; and 10 to the negative pole, n) were studied for each axis (H, R and T).
Abbreviations: BIP, bipolar; H, health; R, risk; T, commitment to the treatment; UNI, unipolar.
As the size of the tiles in Figure 5 clearly reveals, in only very few cases (namely, in 11 out of the 60 matches considered, ie, 18%) did the BIP and UNI versions of the corresponding items have similar ratings (BIP=UNI). In the remaining 82% of matches (ie, 49 out of 60), “corresponding” polarized information produced different ratings. As indicated by the largest tiles in the mosaic, this generally meant that information communicated using opposites led to higher ratings than the “corresponding” unipolar version (ie, BIP>UNI). This finding emerged both when the positive pole (p in Figure 5) and the negative pole (n in Figure 5) were concerned. However, as the significant Pearson’s residuals indicate, this was even more true in the case of “bad news”, where in fact BIP>UNI in 70% of the matches analyzed (ie, 21 out of 30). For example, “survival ratings associated with this tumor are low” prompted higher ratings in terms of H, R, or T than “survival ratings associated with this tumor are 30%”. Similarly, “the probability of side effects associated with the treatment are high” produced higher ratings than “the probability of side effects associated with the treatment is 1 out in a hundred”, and “The side effects related to the treatment for this disease usually have an immediate onset” had higher ratings than “The side effects related to the treatment for this disease usually appear 1 day after the treatment”.
Also in the case of “positive news”, items in which opposites were used frequently rated higher than the unipolar equivalent, as indicated by the size of the tiles (BIP>UNI =53%, ie, 16 out of the 30 total item matches). However, the frequency of cases in which the ratings did not differ (BIP=UNI) increased for at least two of the axes, as indicated by the significant Pearson’s residuals (BIP=UNI: 26% of the total number of matched items). For instance, “the probability of side effects associated with the treatment are low” got higher ratings in terms of H, R, or T than “the probability of side effects associated with the treatment is 1 in a hundred thousand”. Similarly, “The treatment has high efficacy” got higher ratings than “The treatment has 70% efficacy”, whereas “Survival rates associated with this tumor are high” elicited a similar rating to “Survival rates associated with this tumor are 70%”.
Analysis of the 3-item configuration type
Investigating the “correspondence” between BIP and UNI ratings in 3-item configurations enabled us to assess people’s understanding when the information given consists of opposites as compared to information which is not unbalanced toward one or the other pole (which we will refer to with the expression “non-polarized”). If non-polarized information is in effect understood as in between the poles, then the ratings to the UNI version are expected to be in-between those received by the two BIP version. If the non-polarized information is understood in terms of one or the other pole, then the ratings are expected to be similar to one of the two BIP versions, either the positive or the negative pole. If the non-polarized information is understood as more extreme than one or the other pole, then the ratings should be either higher or lower than both poles.
In order to study how the ratings varied for the three levels of communication/information studied (BIP positive, BIP negative, and UNI non-polarized), we first conducted a linear mixed model (Gaussian family) on the ratings given to the 3-item configuration subset. Type of communication/information turned out to be significant (χ2(2, N=470) =1,947, p<0.0001; conditional-R2 index =0.49). As shown in Figure 6 and confirmed by post hoc tests, the ratings given for the non-polarized version were overall at an intermediate point between the two BIP versions, that is, lower than the average ratings associated with BIP negative (EST =−6.523, SE =1.15, t-ratio =5.672; p<0.0001; d=0.516) and higher than the average ratings associated with BIP positive (EST =6.160, SE =1.15, t-ratio =5.356; p<0.0001; d=0.487).
Figure 6.
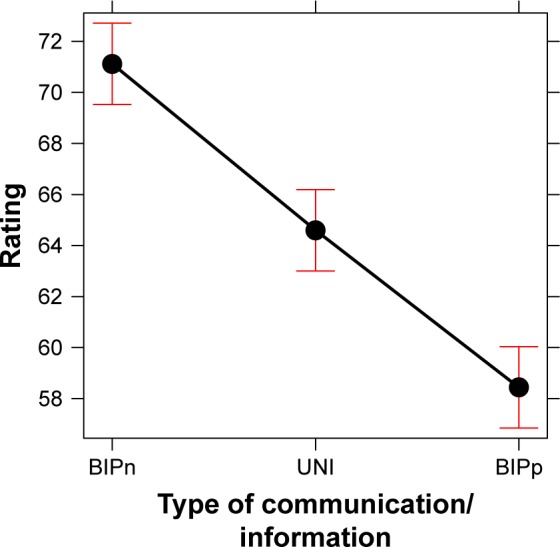
Plot of the main effect of type of communication/information – UNI BIPn, and BIPp – on the ratings given by participants to the items with a 3-item configuration. Error bars represent a 95% confidence interval.
Abbreviations: BIPn, bipolar negative; BIPp, bipolar positive; UNI, unipolar.
Also in this case, it was possible to look more in detail at the relationship between the various communication types by matching the ratings given to the corresponding BIP and UNI versions item by item. Each rating given to a UNI item was matched with two BIP ratings, which corresponded, respectively, to the BIP positive (p) and BIP negative (n) items. We applied the same procedure described in the previous section, that is, we matched the ratings using Student’s t-test and then used the outcomes of the tests to create a new categorical variable (item matching) which in this case had seven levels, corresponding to the seven combinations found (BIPn, BIPp<UNI; BIPn, BIPp=UNI; UNI<BIPn, BIPp; BIPp<UNI<BIPn; BIPp<UNI=BIPn; BIPp=UNI<BIPn; BIPp=UNI>BIPn). The frequency of these seven combinations in the three axes was then analyzed by means of the mosaic plot represented in Figure 7. As the color of the plot indicates, there was no significant interaction between the seven categories of item matching and the three axes. The size of the tiles reveals that there were two more frequent categories. One refers to the case in which the UNI version was in effect associated with an intermediate rating as compared to when the same information was given in terms of the BIP type communication referring to positive or negative poles (indicated by BIPp<UNI<BIPn in Figure 7). This condition in-between the two opposites was found in 33.3% of the total number of matched items analyzed (ie, 14 out of 42). For example, a statement such as “the medical tests have revealed the presence of a nodule” led to significantly higher ratings than “the medical tests have revealed the presence of a benign nodule”, but lower ratings than “the medical tests have revealed the presence of a malignant nodule”.
Figure 7.

Mosaic plot showing the frequency of the seven outcomes of the matching between corresponding items in the BIP and UNI polar versions of the questionnaire, with 3-item configurations. Fourteen matches were studied for each axis (H, R and T).
Abbreviations: BIP, bipolar; BIPn, bipolar negative; BIPp, bipolar positive; H, health; R, risk; T, commitment to the treatment; UNI, unipolar.
Except for only seven cases (16%) in which the UNI version led to lower or higher ratings than both of the BIP versions (indicated by BIPn, BIPp<UNI and UNI<BIPn, BIPp in Figure 7), in all other cases the participants reacted to the non-polarized UNI version in the same way as when the information was given in terms of one or the other pole, which in the majority of cases was the positive pole. The second most frequent category (ie, 26% of the total number of matches analyzed) refers to 11 cases in which the UNI version was understood as “positive news” (indicated by BIPp=UNI<BIPn in Figure 7). This means that, for example, the statement “This is a possible treatment” elicited ratings which were similar to those relating to the statement “This treatment is recommended”, and both the ratings were lower than those elicited by the statement “This treatment is necessary”. In the same way, the ratings for “Once the treatment is completed some people need assistance from a third party (family or other)” were similar to those for “Once the treatment is completed, no assistance is needed from a third party (family or other)”. The statement “Once the treatment is completed, there is need of assistance from a third party (family or other)” was rated higher.
Self-reported comprehension and satisfaction with the communication
Two separate LMMs (Gaussian family), with type of communication (UNI, BIP) and gender (male, female) as fixed effects and participants as a random effect, were conducted to analyze the final ratings for comprehension of the information communicated and satisfaction with the way it was communicated, as expressed by the participants at the end of the questionnaire (the conditional-R2 index of the model was 0.94 for comprehension and 0.92 for satisfaction). For both judgments, a significant effect of type of communication emerged (with no difference for males and females). As shown in Figure 8, the participants reported higher average ratings for comprehension with the bipolar as compared to the UNI form of communication (χ2(1, N=470) =49.929, p<0.0001, EST =13.883, d=0.582). The same hold for self-reported level of satisfaction (χ2(1, N=470) =66.658, p<0.0001, EST =16.902, d=0.700). A strong positive correlation between ratings of comprehension and ratings of satisfaction emerged in both the questionnaires (UNI: r=0.81; BIP: r=0.79).
Figure 8.

Mean ratings (self-reported) for comprehension and satisfaction with the way the information was communicated – either BIP or UNI. Error bars represent a 95% confidence interval.
Abbreviations: BIP, bipolar; UNI, unipolar.
Final remarks
In a worldwide survey on cancer patients, around 40% of those surveyed desired more knowledge and involvement concerning decision making.60 The informed consent form is a crucial document in that it enables patients to make an informed decision.61 Providing accurate information does not suffice if it is provided in a language that people do not understand. A plethora of previous studies have demonstrated that a large number of people did not fully understand the basic information regarding clinical trials6,7,16,62 and that those with a lower standard of literacy were particularly exposed to the risk of poor comprehension.9,63 The findings presented in this paper add to previous studies that confirmed positive effects in terms of the degree of comprehension due to simplifying the informed consent form.10,18,64–68 In the present study, however, instead of simplifying the form in terms of reducing its length, using plain language and short sentences, providing diagrams and pictures and making use of formatting techniques (such as a bold font, highlighting, and bullet points), we focused on whether opposites can play a role. In particular, we explored how communicating in terms of opposites (in the context of information relating to informed consent for oncology trials) rather than avoiding polarization (3-item configuration) or masking polarization (3-item configuration) impacts on people’s understanding and their perception of being healthy–ill, at low–high risk, and of the high–low commitment required to undergo any treatment necessary.
The results demonstrated, in general, that the ratings given by participants depended on which of the two forms of communication types was used. First, when polarized information was concerned (ie, items with a 4-item configuration), speaking in terms of opposites led to higher ratings, both when “bad” and “good” news was given. Taking into account the fact that positive poles in any case concerned the existence of a disease, active commitment and perception of a certain amount of illness and risk are important. The ratings associated with the positive pole expressed in BIP terms were however moderate and in any case lower than those associated with the negative pole, however, the latter was expressed. This confirms that we should interpret this higher rating associated with the BIP version not in terms of an exaggerated reaction, but rather of a positive activation.
Second, in the case of the 3-item configuration, when non-polarized information was provided, the UNI version was not univocally interpreted. Sometimes it led to an intermediate rating such as when the information given was in between bad and good news and sometimes it was understood as pertaining to one of the two poles, which in the majority of cases was the “positive pole”. One can think of this result in terms of a bias toward an optimistic interpretation of non-polarized information, but it might also indicate a bias toward underestimation of the severity of the disease.
Lastly, a difference emerged in terms of the participants’ self-reported impression of whether they understood the information provided and whether they were satisfied with the form of communication used. Their impressions in both the cases were more favorable for the BIP communication type as compared to the UNI version. It should be noted that in both the versions of the questionnaire (UNI and BIP), the statements were expressed in simple everyday language which avoided technical terms. Therefore, the difference that was found has nothing to do with the participants finding it difficult to understand the language used. It seems to suggest rather that a better isomorphism was found between the way in which the information was presented in the bipolar version and the way in which it was processed (ie, understood) by the listener. Of course, we are well aware that these results do not mean that the idea the patient gets of the gravity of the situation and of the commitment required by the treatment (subjective comprehension) is closer to what the doctor is trying to convey (objective understanding). A different study would be necessary to test this by collecting ratings from a sample of doctors in addition to a sample of patients. However, since encouraging patients to take care of their health is an important aim for a doctor and the patient’s understanding is important in order for he/she to be actively engaged in the process,14 the results of this study represent an important starting point.
Other limitations of our study are that 1) our participants were adults (either young or middle aged) in a simulated context and not real patients (of various ages) in a real diagnostic context; using students as a sample and simulating cases of course limit extrapolation to actual clinical contexts; 2) our participants were Italian, and it cannot be excluded that patient preferences and understanding in other countries might be different; 3) individual differences and contextual differences (relating to the family of the patient and to various social aspects) are inevitable components of the complex story relating to coping with a real disease. Further studies are therefore needed which extend the investigation cross-linguistically and use real clinical settings. However, the aim of this study was to explore the hypothesis that another reasonable aspect to consider in terms of how to encourage active decision making and improve communication and comprehension of information relating to informed consent in medical contexts is linked to the cognitive and linguistic primacy of opposites in natural languages35,39–42 as well as in human perception and conceptualization.28,31,33 We consider the findings collected in this initial study (with all the abovementioned limitations) to be encouraging.
Supplementary material
Table S1.
Bipolar and unipolar items used in the study in English with Italian translation in square brackets
| Type | Items |
|---|---|
| BIP | Medical tests have shown the presence of a small nodule [Le analisi hanno rivelato la presenza di un piccolo nodulo] |
| BIP | Medical tests have shown the presence of a large nodule [Le analisi hanno rivelato la presenza di un grosso nodulo] |
| BIP | Medical tests have revealed the existence of a benign nodule [Le analisi hanno rivelato la presenza di un nodulo benigno] |
| BIP | Medical tests have revealed the existence of a malignant nodule [Le analisi hanno rivelato la presenza di un nodulo maligno] |
| BIP | The MRI scan has revealed some nodules localized in a circumscribed region of your body [La risonanza magnetica ha rivelato la presenza di alcuni noduli localizzati in una zona circoscritta del tuo corpo] |
| BIP | The MRI scan has revealed some nodules in various regions of your body [La risonanza magnetica ha rivelato la presenza di alcuni noduli diffusi in varie zone del tuo corpo] |
| BIP | This type of tumor is common [Questo tipo di tumore è comune] |
| BIP | This type of tumor is rare [Questo tipo di tumore è raro] |
| BIP | This tumor is easy to treat [Questo tumore è facilmente curabile] |
| BIP | This tumor is hard to treat [Questo tumore è difficilmente curabile] |
| BIP | This type of tumor has a slow progression and takes a long time before it becomes serious enough to cause death [Questo tumore ha una progressione lenta (impiega molto tempo a diventare così grave da condurre alla morte)] |
| BIP | This type of tumor has a quick progression and takes very little time to become serious enough to cause death [Questo tumore ha una progressione veloce (impiega poco tempo a diventare così grave da condurre alla morte)] |
| BIP | This tumor is always linked to a genetic predisposition [Questo tumore è sempre connesso con una predisposizione genetica] |
| BIP | This tumor is never linked to a genetic predisposition [Questo tumore non è mai connesso con una predisposizione genetica] |
| BIP | This tumor is associated with high survival rates [Questo tumore è associato ad alti tassi di sopravvivenza] |
| BIP | This tumor is associated with low survival rates [Questo tumore è associato a bassi tassi di sopravvivenza] |
| BIP | This treatment will cure this tumor; ie, it will eliminate all of the tumor cells [Questo trattamento curerà il tumore, vale a dire che eliminerà tutte le cellule tumorali] |
| BIP | This treatment is palliative in nature; ie, it eliminates the symptoms associated with the tumor [Questo trattamento è palliativo, vale a dire che eliminerà i sintomi associati al tumore] |
| BIP | This treatment has high efficacy [Questo trattamento ha un’alta efficacia] |
| BIP | This treatment has low efficacy [Questo trattamento ha una bassa efficacia] |
| BIP | This treatment is necessary [Questo trattamento è necessario] |
| BIP | This treatment is advisable [Questo trattamento è consigliabile] |
| BIP | The standard treatment for this tumor has minor adverse side effects [Il trattamento per questo tumore hai dei lievi effetti collaterali] |
| BIP | The standard treatment for this tumor has severe adverse side effects [Il trattamento per questo tumore ha dei seri effetti collaterali] |
| BIP | The probability of adverse side effects linked to the treatment is very low [La probabilità di effetti collaterali associati al trattamento per questo tumore è molto bassa] |
| BIP | The probability of adverse side effects linked to the treatment is very high [La probabilità di effetti collaterali associati al trattamento per questo tumore è molto alta] |
| BIP | The adverse side effects related to the standard treatment for this tumor have an immediate onset [Gli effetti collaterali associati al trattamento per questo tumore hanno un’insorgenza immediata] |
| BIP | The adverse side effects related to the standard treatment for this tumor have a delayed onset [Gli effetti collaterali associati al trattamento per questo tumore hanno un’insorgenza ritardata nel tempo] |
| BIP | The adverse side effects related to the standard treatment are temporary [Gli effetti collaterali associati al trattamento per questo tumore sono temporanei] |
| BIP | The adverse side effects related to the standard treatment are permanent [Gli effetti collaterali associati al trattamento per questo tumore sono permanenti] |
| BIP | This treatment requires a short period of time to complete [Il trattamento ha una durata breve] |
| BIP | This treatment requires a long period of time to complete [Il trattamento ha una durata lunga] |
| BIP | This treatment is administered in a single cycle [Il trattamento prevede un unico ciclo di somministrazione] |
| BIP | This treatment is administered over many cycles [Il trattamento prevede molti cicli di somministrazione] |
| BIP | This treatment is administered on an outpatient basis [Il trattamento è somministrato in day hospital] |
| BIP | This treatment is administered on an inpatient basis [Il trattamento prevede ricovero e degenza in ospedale] |
| BIP | During treatment, you can live by yourself, you will not need assistance [Durante il trattamento puoi gestirti autonomamente, non avrai bisogno di assistenza] |
| BIP | During treatment, you will need assistance [Durante il trattamento avrai bisogno di assistenza] |
| BIP | Once the whole treatment cycle is completed, you can live by yourself, you will not need assistance [Una volta che il trattamento è completato, potrai gestirti autonomamente, non avrai bisogno di assistenza] |
| BIP | Once the whole treatment cycle is completed, you will need assistance [Una volta che il trattamento è completato, avrai bisogno di assistenza] |
| BIP | During treatment, your lifestyle will remain identical to what it was before treatment [Durante il trattamento il tuo stile di vita non subirà cambiamenti (rimarrà identico a com’era prima del trattamento)] |
| BIP | During treatment, your lifestyle will differ from what it was before the treatment [Durante il trattamento il tuo stile di vita subirà dei cambiamenti (non potrà più essere com’era prima del trattamento)] |
| BIP | After treatment is completed, your lifestyle will go back to what it was prior to the disease [Dopo il trattamento il tuo stile di vita tornerà identico a com’era prima della malattia] |
| BIP | After treatment is completed, your lifestyle will change from what it was prior to the disease [Dopo il trattamento il tuo stile di vita subirà dei cambiamenti rispetto a com’era prima della malattia] |
| BIP | The treatment does not impact on your ability to work (ie, during the treatment phase, you can keep working) [Il trattamento, mentre lo fai, non avrà ripercussioni sulla tua possibilità di lavorare (durante il trattamento potrai continuare ad andare al lavoro)] |
| BIP | The treatment impacts on your ability to work (ie, during the treatment phase, you cannot go to work) [Il trattamento, mentre lo fai, avrà ripercussioni sulla tua possibilità di lavorare (durante il trattamento non potrai andare a lavorare)] |
| BIP | Once the entire treatment cycle is completed, the treatment will have no impact on your ability to work (you can return to work as you did before the disease) [Una volta che l’intero ciclo di trattamento è finito, non avrai ripercussioni sulla tua attività lavorativa (potrai tornare a lavorare come prima della malattia)] |
| BIP | Once the entire treatment cycle is completed, the treatment will have an impact on your ability to work (you will not be able to return to work) [Una volta che l’intero ciclo di trattamento è finito, avrai ripercussioni sulla tua attività lavorativa (non potrai tornare a lavorare come prima della malattia)] |
| UNI | Medical tests have shown the presence of a 0.5 inch long nodule (1.3 cm) [Le analisi hanno rivelato la presenza di un nodulo di 1.3 cm] |
| UNI | Medical tests have shown the presence of a three inch long nodule (7.6 cm) [Le analisi hanno rivelato la presenza di un nodulo di 7.6 cm] |
| UNI | Medical tests demonstrated the existence of a nodule [Le analisi hanno rivelato la presenza di un nodulo] |
| UNI | The MRI scan has revealed some nodules in your body [La risonanza magnetica ha rivelato la presenza di alcuni noduli nel tuo corpo] |
| UNI | This tumor affects 1 in a thousand people [Questo tipo di tumore colpisce 1 persona su 1,000] |
| UNI | This tumor affects 1 in a million people [Questo tipo di tumore colpisce 1 persona su 1,000,000] |
| UNI | This tumor is curable in 10% of all cases [Questo tumore è curabile nel 10% dei casi] |
| UNI | This tumor is curable in 80% of all cases [Questo tumore è curabile nell’ 80% dei casi] |
| UNI | This type of tumor usually leads to death within 2 years of the time of diagnosis [Questo tumore generalmente conduce alla morte in 2 anni dalla diagnosi] |
| UNI | This type of tumor usually leads to death within 10 years of diagnosis [Questo tumore generalmente conduce alla morte in 10 anni dalla diagnosi] |
| UNI | This tumor is determined by a specific genetic predisposition in 5 out of 5 cases [Questo tumore ha una predisposizione genetica in 5 casi su 5] |
| UNI | This tumor is determined by a specific genetic predisposition in 0 out of 5 cases [Questo tumore ha una predisposizione genetica in O casi su 5] |
| UNI | This tumor has a 70% survival rate [Questo tumore ha un tasso di sopravvivenza del 70%] |
| UNI | This tumor has a 30% survival rate [Questo tumore ha un tasso di sopravvivenza del 30%] |
| UNI | This treatment will be of some help with this tumor [Questo trattamento sarà di qualche aiuto in questa situazione] |
| UNI | This treatment has 70% efficacy rate [Questo trattamento ha un’efficacia del 70%] |
| UNI | This treatment has 30% efficacy rate [Questo trattamento ha un’efficacia del 30%] |
| UNI | This is a possible course of treatment [Questo è un possibile trattamento] |
| UNI | The standard treatment for this tumor has adverse side effects [Il trattamento per questo tumore ha degli effetti collaterali] |
| UNI | The probability of adverse side effects relating to the treatment is 1 in 100,000 [La probabilità di effetti collaterali associati al trattamento per questo tumore è di 1 su 100,000] |
| UNI | The probability of adverse side effects relating to the treatment is 1 in 100 [La probabilità di effetti collaterali associati al trattamento per questo tumore è di 1 su 100] |
| UNI | The adverse side effects related to the standard treatment for this tumor usually appear 1 day after treatment [Gli effetti collaterali associati al trattamento per questo tumore generalmente appaiono un giorno dopo il trattamento] |
| UNI | The adverse side effects related to the standard treatment for this tumor usually appear years after treatment [Gli effetti collaterali associati al trattamento per questo tumore generalmente appaiono diversi anni dopo il trattamento] |
| UNI | The duration of the adverse side effects related to the standard treatment varies over time [Gli effetti collaterali associati al trattamento per questo tumore hanno una durata variabile nel tempo] |
| UNI | This treatment takes 15 days to complete [Il trattamento si completa in 15 giorni] |
| UNI | This treatment takes 1 year to complete [Il trattamento si completa in 1 anno] |
| UNI | This treatment is administered in cycles [Il trattamento è somministrato in cicli] |
| UNI | This treatment is administered in a medical facility [Il trattamento è somministrato in una struttura ospedaliera] |
| UNI | During treatment, assistance might or might not be required [Durante il trattamento qualcuno ha, qualcun altro non ha bisogno di assistenza] |
| UNI | Once the whole treatment cycle is completed, assistance might or might not be required [Una volta che il trattamento è completato qualcuno ha, qualcun altro non ha bisogno di assistenza] |
| UNI | During treatment, your lifestyle might or might not be affected [Durante il trattamento il tuo stile di vita potrebbe subire dei cambiamenti (qualcuno riesce a fare la vita che faceva prima, qualche altro no)] |
| UNI | After treatment is completed, your lifestyle might or might not change from what it was prior to the disease [Dopo il trattamento il tuo stile di vita potrebbe subire dei cambiamenti rispetto a com’era prima della malattia (qualcuno riesce a fare la vita che faceva prima, qualche altro no)] |
| UNI | The treatment might or not impact on your ability to work (during the treatment phase) [Il trattamento, mentre lo fai, potrebbe influire sulla tua possibilità di andare a lavorare (qualcuno durante il trattamento non riesce ad andare a lavorare, qualcuno invece sì)] |
| UNI | Once the entire treatment cycle is completed, the treatment might or not impact on your ability to work… [Una volta che l’intero ciclo di trattamento è finito, potresti avere (ma anche no) ripercussioni sulla tua attività lavorativa (qualcuno non riesce ad tornare a lavorare come prima, qualcuno invece sì)] |
Abbreviations: BIP, bipolar; MRI, magnetic resonance imaging; UNI, unipolar.
Acknowledgments
We wish to thank Ricardo Pietrobon for stimulating us to develop this research, Michael Kubovy for his input and suggestions on a previous version of this paper, and the undergraduate students, Nasko Bressan, Annachiara Teboni, and Eliana Orlandini, for their help in data collection.
Footnotes
Disclosure
The authors report no conflicts of interest in this work.
References
- 1.European Commission Health and Consumers Directorate-General Revision of the Clinical Trials Directive 2001/20/EC. Brussels, 09/02/2011. SANCO/C/8/PB/SF D(2011) 143488. [Accessed March 16, 2018]. Available from: https://ec.europa.eu/health/sites/health/files/files/clinicaltrials/ctresp_2011-06/leti_pharma.pdf.
- 2.Aaronson NK, Visser-Pol E, Leenhouts GH, et al. Telephone-based nursing intervention improves the effectiveness of the informed consent process in cancer clinical trials. J Clin Oncol. 1996;14(3):984–996. doi: 10.1200/JCO.1996.14.3.984. [DOI] [PubMed] [Google Scholar]
- 3.Brown RF, Butow PN, Ellis P, Boyle F, Tattersall MH. Seeking informed consent to cancer clinical trials: describing current practice. Soc Sci Med. 2004;58(12):2445–2457. doi: 10.1016/j.socscimed.2003.09.007. [DOI] [PubMed] [Google Scholar]
- 4.Jenkins V, Fallowfield L, Souhami A, Satwell M. How do doctors explain randomised clinical trials to their patients? Eur J Cancer. 1999;35(8):1187–1193. doi: 10.1016/s0959-8049(99)00116-1. [DOI] [PubMed] [Google Scholar]
- 5.Hietanen P, Aro AR, Holli K, Absetz P. Information and communication in the context of a clinical trial. Eur J Cancer. 2000;36(16):2096–2104. doi: 10.1016/s0959-8049(00)00191-x. [DOI] [PubMed] [Google Scholar]
- 6.Holland J, Browman G, McDonald M, Saginur R. Protecting human research participants: reading vs understanding the consent form. J Natl Cancer Inst. 2013;105(13):927–928. doi: 10.1093/jnci/djt152. [DOI] [PubMed] [Google Scholar]
- 7.Paasche-Orlow MK, Taylor HA, Brancati FL. Readability standards for informed consent forms as compared with actual readability. N Engl J Med. 2003;348(8):721–726. doi: 10.1056/NEJMsa021212. [DOI] [PubMed] [Google Scholar]
- 8.Schumacher A, Sikov WM, Quesenberry MI, et al. Informed consent in oncology clinical trials: a Brown University Oncology Research Group prospective cross-sectional pilot study. PLoS One. 2017;12(2):e0172957. doi: 10.1371/journal.pone.0172957. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Breese P, Burman W, Goldberg S, Weis S. Education level, primary language, and comprehension of the informed consent process. J Empir Res Hum Res Ethics. 2007;2(4):69–79. doi: 10.1525/jer.2007.2.4.69. [DOI] [PubMed] [Google Scholar]
- 10.Dresden GM, Levitt MA. Modifying a standard industry clinical trial consent form improves patient information retention as part of the informed consent process. Acad Emerg Med. 2001;8(3):246–252. doi: 10.1111/j.1553-2712.2001.tb01300.x. [DOI] [PubMed] [Google Scholar]
- 11.Joffe S, Cook EF, Clearly PD, Clark JW, Weeks JC. Quality of informed consent: a new measure of understanding among research subjects. J Natl Cancer Inst. 2001;93(2):139–147. doi: 10.1093/jnci/93.2.139. [DOI] [PubMed] [Google Scholar]
- 12.Brandberg Y, Johansson H, Bergenmar M. Patients’ knowledge and perceived understanding – associations with consenting to participate in cancer clinical trials. Contemp Clin Trials Commun. 2016;2(15):6–11. doi: 10.1016/j.conctc.2015.12.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Miller SM, Hudson SV, Egleston BL, et al. The relationships among knowledge, self-efficacy, preparedness, decisional conflict, and decisions to participate in a cancer clinical trial. Psychooncology. 2013;22(3):481–489. doi: 10.1002/pon.3043. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Pravettoni G, Cutica I, Righetti S, Mazzocco K. Decisions and the involvement of cancer patient survivors: a moral imperative. J Healthc Leadersh. 2016;8:121–125. doi: 10.2147/JHL.S115434. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Byrne MM, Kornfeld J, Vanderpool R, Belanger M. Discussions of cancer clinical trials with NCI’s Cancer Information Service. J Health Commun. 2012;17(3):319–337. doi: 10.1080/10810730.2011.626500. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Byrne MM, Tannenbaum SL, Gluck S, Hurley J, Antoni M. Participation in cancer clinical trials: why are patients not participating? Med Decis Making. 2013;34(1):116–126. doi: 10.1177/0272989X13497264. [DOI] [PubMed] [Google Scholar]
- 17.Des Jarlais DC, Paone D, Milliken J, et al. Audio-computer interviewing to measure risk behaviour for HIV among injecting drug users: a quasi-randomised trial. Lancet. 1999;353(9165):1657–1661. doi: 10.1016/s0140-6736(98)07026-3. [DOI] [PubMed] [Google Scholar]
- 18.Flory J, Emanuel E. Interventions to improve research participants’ understanding in informed consent for research: a systematic review. JAMA. 2004;292(13):593–601. doi: 10.1001/jama.292.13.1593. [DOI] [PubMed] [Google Scholar]
- 19.Jacobsen PB, Wells KJ, Meade CD, et al. Effects of a brief multimedia psychoeducational intervention on the attitudes and interest of patients with cancer regarding clinical trial participation: a multicenter randomized controlled trial. J Clin Oncol. 2012;30(20):2516–2521. doi: 10.1200/JCO.2011.39.5186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Kass NE, Taylor HA, Ali J, Hallez K, Chaisson L. A pilot study of simple interventions to improve informed consent in clinical research: feasibility, approach, and results. Clin Trials. 2015;12(1):54–66. doi: 10.1177/1740774514560831. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Krishnamurti T, Argo N. A patient-centered approach to informed consent: results from a survey and randomized trial. Med Decis Making. 2016;36(6):726–740. doi: 10.1177/0272989X16636844. [DOI] [PubMed] [Google Scholar]
- 22.Nishimura A, Carey J, Erwin PJ, Tilburt JC, Murad MH, McCormick JB. Improving understanding in the research informed consent process: a systematic review of 54 interventions tested in randomized control trials. BMC Med Ethics. 2013;14(28):14–28. doi: 10.1186/1472-6939-14-28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Perlis TE, Des Jarlais DC, Friedman SR, Arasteh K, Turner CF. Audio-computerized self-interviewing versus face-to-face interviewing for research data collection at drug abuse treatment programs. Addiction. 2004;99(7):885–896. doi: 10.1111/j.1360-0443.2004.00740.x. [DOI] [PubMed] [Google Scholar]
- 24.Synnot A, Ryan R, Prictor M, Fetherstonhaugh D, Parker B. Audiovisual presentation of information for informed consent for participation in clinical trials. Cochrane Database Syst Rev. 2014;9(5):CD003717. doi: 10.1002/14651858.CD003717.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Stunkel L, Benson M, McLellan L, et al. Comprehension and informed consent: assessing the effectiveness of a short consent form. IRB. 2010;32(4):1–9. [PMC free article] [PubMed] [Google Scholar]
- 26.Bergenmar M, Johansson H, Wilking N. Levels of knowledge and perceived understanding among participants in cancer clinical trials – factors related to the informed consent procedure. Clin Trials. 2011;8(1):77–84. doi: 10.1177/1740774510384516. [DOI] [PubMed] [Google Scholar]
- 27.Bianchi I, Burro R, Torquati S, Savardi U. The middle of the road: perceiving intermediates. Acta Psychol. 2013;144(1):121–135. doi: 10.1016/j.actpsy.2013.05.005. [DOI] [PubMed] [Google Scholar]
- 28.Bianchi I, Savardi U. The Perception of Contraries. Roma: Aracne; 2008. [Google Scholar]
- 29.Bianchi I, Savardi U, Burro R. Perceptual ratings of opposite spatial properties: do they lie on the same dimension? Acta Psychol. 2011;138(3):405–418. doi: 10.1016/j.actpsy.2011.08.003. [DOI] [PubMed] [Google Scholar]
- 30.Burro R. To be objective in experimental phenomenology: a psychophysics application. SpringerPlus. 2016;5(1):1720. doi: 10.1186/s40064-016-3418-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Bianchi I, Paradis C, Burro R, van de Weijer J, Nyström M, Savardi U. Identification of poles and intermediates by eye and by hand. Acta Psychol. 2017;180:175–189. doi: 10.1016/j.actpsy.2017.08.011. [DOI] [PubMed] [Google Scholar]
- 32.Bianchi I, Savardi U, Kubovy M. Dimensions and their poles: a metric and topological theory of opposites. Lang Cogn Process. 2011;26(8):1232–1265. [Google Scholar]
- 33.Gärdenfors P. Conceptual Spaces: The Geometry of Thought. Cambridge: The MIT Press; 2000. [Google Scholar]
- 34.Gärdenfors P. Semantics Based on Conceptual Spaces. Cambridge: The MIT Press; 2014. The Geometry of Meaning. [Google Scholar]
- 35.Miller GA. The Science of Words. New York: Scientific American Library; 1996. [Google Scholar]
- 36.Jones S, Murphy ML, Paradis C, Willners C. Antonyms in English: Construals, Constructions and Canonicity. Cambridge: Cambridge University Press; 2012. [Google Scholar]
- 37.Paradis C, Hudson J, Magnusson U, editors. The Construal of Spatial Meaning: Windows into Conceptual Space. Oxford: Oxford University Press; 2013. [Google Scholar]
- 38.Paradis C, Willners C, Jones S. Good and bad opposites: using textual and psycholinguistic techniques to measure antonym canonicity. Ment Lex. 2009;4(3):380–429. [Google Scholar]
- 39.Croft W, Cruse DA. Cognitive Linguistics. Cambridge: Cambridge University Press; 2004. [Google Scholar]
- 40.Cruse DA, Pagona T. Towards a cognitive model of antonymy. Lexicology. 1995;1:113–141. [Google Scholar]
- 41.Fellbaum C. Co-occurrence and antonymy. Int J Lex. 1995;8(4):281–303. [Google Scholar]
- 42.Jones S. Antonymy: A Corpus-Based Perspective. London: Routledge; 2002. [Google Scholar]
- 43.Murphy L. Semantic Relations and the Lexicon: Antonyms, Synonyms and Other Semantic Paradigms. Cambridge: Cambridge University Press; 2003. [Google Scholar]
- 44.Casasola M. The development of infants’ spatial categories. Curr Dir Psychol Sci. 2008;17:21–25. [Google Scholar]
- 45.Casasola M, Cohen LB, Chiarello E. Six-month-old infants’ categorization of containment spatial relations. Child Dev. 2003;(74):679–693. doi: 10.1111/1467-8624.00562. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Hespos SJ, Spelke ES. Conceptual precursors to language. Nature. 2014;430(6998):453–456. doi: 10.1038/nature02634. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.McDonough L, Choi S, Mandler JM. Understanding spatial relations: flexible infants, lexical adults. Cog Psychol. 2003;46(3):229–259. doi: 10.1016/s0010-0285(02)00514-5. [DOI] [PubMed] [Google Scholar]
- 48.Quinn PC, Cummins M, Kase J, Martin E, Weisman S. Development of categorical representations for above and below spatial relations in 3- to 7-month-old infants. Dev Psychol. 1996;32(5):942–950. [Google Scholar]
- 49.Bianchi I, Savardi U, Burro R, Martelli MF. Doing the opposite to what another person is doing. Acta Psychol. 2014;151:117–133. doi: 10.1016/j.actpsy.2014.06.003. [DOI] [PubMed] [Google Scholar]
- 50.Kelso JAS, Engstrøm D. The Complementary Nature. Cambridge: The MIT Press; 2006. [Google Scholar]
- 51.Savardi U, editor. The Perception and Cognition of Contraries. Milano: Mc-Graw Hill; 2009. [Google Scholar]
- 52.Bates D, Machler M, Bolker BM, Walker SC. Fitting linear mixed-effects models using lme4. J Stat Softw. 2015;67:1–48. [Google Scholar]
- 53.Lenth RV. Least-squares means: the R package lsmeans. J Stat Softw. 2016;69(1):1–33. [Google Scholar]
- 54.Burro R, Raccanello D, Pasini M, Brondino M. An estimation of a nonlinear dynamic process using latent class extended mixed models: affect profiles after terrorist attacks. Nonlinear Dynamics Psychol Life Sci. 2018;22(1):35–52. [PubMed] [Google Scholar]
- 55.Kuznetsova A, Bruun BP, Haubo BCR. lmerTest: tests in linear mixed effects models. R package version 2.0-32 [serial on the Internet] 2016. [Accessed November 2, 2017]. Available from: https://CRAN.R-project.org/package=lmerTest.
- 56.Cohen J. Statistical Power Analysis for the Behavioral Sciences. 2nd ed. New York: Academic Press; 1988. [Google Scholar]
- 57.Nakagawa S, Schielzeth H. A general and simple method for obtaining R2 from generalized linear mixed-effects models. Methods Ecol Evol. 2013;4(2):133–142. [Google Scholar]
- 58.Friendly M. Mosaic displays for multi-way contingency tables. J Am Stat Ass. 1994;89:190–200. [Google Scholar]
- 59.Friendly M. Visualizing Categorical Data. Carey: SAS Institute; 2000. [Google Scholar]
- 60.Alston C, Paget L, Halvorson G, et al. Discussion Paper. Institute of Medicine; Washington, DC: 2012. Communicating with Patients on Health Care Evidence. Available from: https://nam.edu/wp-content/uploads/2015/06/VSRT-Evidence.pdf. [Google Scholar]
- 61.Rao KHS. Informed consent: an ethical obligation or legal compulsion? J Cutan Aesthet Surg. 2008;1(1):33–35. doi: 10.4103/0974-2077.41159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Cheung WY, Pond GR, Heslegrave RJ, Enright K, Potanina L, Siu LL. The contents and readability of informed consent forms for oncology clinical trials. Am J Clin Oncol. 2010;33(4):387–392. doi: 10.1097/COC.0b013e3181b20641. [DOI] [PubMed] [Google Scholar]
- 63.Sudore RL, Landefeld CS, Williams BA, Barnes DE, Lindquist K, Schillinger D. Use of a modified informed consent process among vulnerable patients: a descriptive study. J Gen Intern Med. 2006;21(8):867–873. doi: 10.1111/j.1525-1497.2006.00535.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Dormandy E, Tsui EY, Marteau TM. Development of a measure of informed choice suitable for use in low literacy populations. Patient Educ Couns. 2007;66:278–295. doi: 10.1016/j.pec.2007.01.001. [DOI] [PubMed] [Google Scholar]
- 65.Choi J. Literature review: using pictographs in discharge instructions for older adults with low-literacy skills. J Clin Nurs. 2011;20:2984–2996. doi: 10.1111/j.1365-2702.2011.03814.x. [DOI] [PubMed] [Google Scholar]
- 66.Tamariz L, Palacio A, Robert M, et al. Improving the informed consent process for research subjects with low literacy: a systematic review. J Gen Intern Med. 2013;28:121–126. doi: 10.1007/s11606-012-2133-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Davis TC, Holcombe RF, Berkel HJ, et al. Informed consent for clinical trials: a comparative study of standard versus simplified forms. J Natl Cancer Inst. 1998;90:668–674. doi: 10.1093/jnci/90.9.668. [DOI] [PubMed] [Google Scholar]
- 68.Kim EJ, Kim SH. Simplification of inform consent improves understanding of informed consent information in clinical trials regardless of health literacy. Clin Trials. 2015;12(3):232–236. doi: 10.1177/1740774515571139. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1.
Bipolar and unipolar items used in the study in English with Italian translation in square brackets
| Type | Items |
|---|---|
| BIP | Medical tests have shown the presence of a small nodule [Le analisi hanno rivelato la presenza di un piccolo nodulo] |
| BIP | Medical tests have shown the presence of a large nodule [Le analisi hanno rivelato la presenza di un grosso nodulo] |
| BIP | Medical tests have revealed the existence of a benign nodule [Le analisi hanno rivelato la presenza di un nodulo benigno] |
| BIP | Medical tests have revealed the existence of a malignant nodule [Le analisi hanno rivelato la presenza di un nodulo maligno] |
| BIP | The MRI scan has revealed some nodules localized in a circumscribed region of your body [La risonanza magnetica ha rivelato la presenza di alcuni noduli localizzati in una zona circoscritta del tuo corpo] |
| BIP | The MRI scan has revealed some nodules in various regions of your body [La risonanza magnetica ha rivelato la presenza di alcuni noduli diffusi in varie zone del tuo corpo] |
| BIP | This type of tumor is common [Questo tipo di tumore è comune] |
| BIP | This type of tumor is rare [Questo tipo di tumore è raro] |
| BIP | This tumor is easy to treat [Questo tumore è facilmente curabile] |
| BIP | This tumor is hard to treat [Questo tumore è difficilmente curabile] |
| BIP | This type of tumor has a slow progression and takes a long time before it becomes serious enough to cause death [Questo tumore ha una progressione lenta (impiega molto tempo a diventare così grave da condurre alla morte)] |
| BIP | This type of tumor has a quick progression and takes very little time to become serious enough to cause death [Questo tumore ha una progressione veloce (impiega poco tempo a diventare così grave da condurre alla morte)] |
| BIP | This tumor is always linked to a genetic predisposition [Questo tumore è sempre connesso con una predisposizione genetica] |
| BIP | This tumor is never linked to a genetic predisposition [Questo tumore non è mai connesso con una predisposizione genetica] |
| BIP | This tumor is associated with high survival rates [Questo tumore è associato ad alti tassi di sopravvivenza] |
| BIP | This tumor is associated with low survival rates [Questo tumore è associato a bassi tassi di sopravvivenza] |
| BIP | This treatment will cure this tumor; ie, it will eliminate all of the tumor cells [Questo trattamento curerà il tumore, vale a dire che eliminerà tutte le cellule tumorali] |
| BIP | This treatment is palliative in nature; ie, it eliminates the symptoms associated with the tumor [Questo trattamento è palliativo, vale a dire che eliminerà i sintomi associati al tumore] |
| BIP | This treatment has high efficacy [Questo trattamento ha un’alta efficacia] |
| BIP | This treatment has low efficacy [Questo trattamento ha una bassa efficacia] |
| BIP | This treatment is necessary [Questo trattamento è necessario] |
| BIP | This treatment is advisable [Questo trattamento è consigliabile] |
| BIP | The standard treatment for this tumor has minor adverse side effects [Il trattamento per questo tumore hai dei lievi effetti collaterali] |
| BIP | The standard treatment for this tumor has severe adverse side effects [Il trattamento per questo tumore ha dei seri effetti collaterali] |
| BIP | The probability of adverse side effects linked to the treatment is very low [La probabilità di effetti collaterali associati al trattamento per questo tumore è molto bassa] |
| BIP | The probability of adverse side effects linked to the treatment is very high [La probabilità di effetti collaterali associati al trattamento per questo tumore è molto alta] |
| BIP | The adverse side effects related to the standard treatment for this tumor have an immediate onset [Gli effetti collaterali associati al trattamento per questo tumore hanno un’insorgenza immediata] |
| BIP | The adverse side effects related to the standard treatment for this tumor have a delayed onset [Gli effetti collaterali associati al trattamento per questo tumore hanno un’insorgenza ritardata nel tempo] |
| BIP | The adverse side effects related to the standard treatment are temporary [Gli effetti collaterali associati al trattamento per questo tumore sono temporanei] |
| BIP | The adverse side effects related to the standard treatment are permanent [Gli effetti collaterali associati al trattamento per questo tumore sono permanenti] |
| BIP | This treatment requires a short period of time to complete [Il trattamento ha una durata breve] |
| BIP | This treatment requires a long period of time to complete [Il trattamento ha una durata lunga] |
| BIP | This treatment is administered in a single cycle [Il trattamento prevede un unico ciclo di somministrazione] |
| BIP | This treatment is administered over many cycles [Il trattamento prevede molti cicli di somministrazione] |
| BIP | This treatment is administered on an outpatient basis [Il trattamento è somministrato in day hospital] |
| BIP | This treatment is administered on an inpatient basis [Il trattamento prevede ricovero e degenza in ospedale] |
| BIP | During treatment, you can live by yourself, you will not need assistance [Durante il trattamento puoi gestirti autonomamente, non avrai bisogno di assistenza] |
| BIP | During treatment, you will need assistance [Durante il trattamento avrai bisogno di assistenza] |
| BIP | Once the whole treatment cycle is completed, you can live by yourself, you will not need assistance [Una volta che il trattamento è completato, potrai gestirti autonomamente, non avrai bisogno di assistenza] |
| BIP | Once the whole treatment cycle is completed, you will need assistance [Una volta che il trattamento è completato, avrai bisogno di assistenza] |
| BIP | During treatment, your lifestyle will remain identical to what it was before treatment [Durante il trattamento il tuo stile di vita non subirà cambiamenti (rimarrà identico a com’era prima del trattamento)] |
| BIP | During treatment, your lifestyle will differ from what it was before the treatment [Durante il trattamento il tuo stile di vita subirà dei cambiamenti (non potrà più essere com’era prima del trattamento)] |
| BIP | After treatment is completed, your lifestyle will go back to what it was prior to the disease [Dopo il trattamento il tuo stile di vita tornerà identico a com’era prima della malattia] |
| BIP | After treatment is completed, your lifestyle will change from what it was prior to the disease [Dopo il trattamento il tuo stile di vita subirà dei cambiamenti rispetto a com’era prima della malattia] |
| BIP | The treatment does not impact on your ability to work (ie, during the treatment phase, you can keep working) [Il trattamento, mentre lo fai, non avrà ripercussioni sulla tua possibilità di lavorare (durante il trattamento potrai continuare ad andare al lavoro)] |
| BIP | The treatment impacts on your ability to work (ie, during the treatment phase, you cannot go to work) [Il trattamento, mentre lo fai, avrà ripercussioni sulla tua possibilità di lavorare (durante il trattamento non potrai andare a lavorare)] |
| BIP | Once the entire treatment cycle is completed, the treatment will have no impact on your ability to work (you can return to work as you did before the disease) [Una volta che l’intero ciclo di trattamento è finito, non avrai ripercussioni sulla tua attività lavorativa (potrai tornare a lavorare come prima della malattia)] |
| BIP | Once the entire treatment cycle is completed, the treatment will have an impact on your ability to work (you will not be able to return to work) [Una volta che l’intero ciclo di trattamento è finito, avrai ripercussioni sulla tua attività lavorativa (non potrai tornare a lavorare come prima della malattia)] |
| UNI | Medical tests have shown the presence of a 0.5 inch long nodule (1.3 cm) [Le analisi hanno rivelato la presenza di un nodulo di 1.3 cm] |
| UNI | Medical tests have shown the presence of a three inch long nodule (7.6 cm) [Le analisi hanno rivelato la presenza di un nodulo di 7.6 cm] |
| UNI | Medical tests demonstrated the existence of a nodule [Le analisi hanno rivelato la presenza di un nodulo] |
| UNI | The MRI scan has revealed some nodules in your body [La risonanza magnetica ha rivelato la presenza di alcuni noduli nel tuo corpo] |
| UNI | This tumor affects 1 in a thousand people [Questo tipo di tumore colpisce 1 persona su 1,000] |
| UNI | This tumor affects 1 in a million people [Questo tipo di tumore colpisce 1 persona su 1,000,000] |
| UNI | This tumor is curable in 10% of all cases [Questo tumore è curabile nel 10% dei casi] |
| UNI | This tumor is curable in 80% of all cases [Questo tumore è curabile nell’ 80% dei casi] |
| UNI | This type of tumor usually leads to death within 2 years of the time of diagnosis [Questo tumore generalmente conduce alla morte in 2 anni dalla diagnosi] |
| UNI | This type of tumor usually leads to death within 10 years of diagnosis [Questo tumore generalmente conduce alla morte in 10 anni dalla diagnosi] |
| UNI | This tumor is determined by a specific genetic predisposition in 5 out of 5 cases [Questo tumore ha una predisposizione genetica in 5 casi su 5] |
| UNI | This tumor is determined by a specific genetic predisposition in 0 out of 5 cases [Questo tumore ha una predisposizione genetica in O casi su 5] |
| UNI | This tumor has a 70% survival rate [Questo tumore ha un tasso di sopravvivenza del 70%] |
| UNI | This tumor has a 30% survival rate [Questo tumore ha un tasso di sopravvivenza del 30%] |
| UNI | This treatment will be of some help with this tumor [Questo trattamento sarà di qualche aiuto in questa situazione] |
| UNI | This treatment has 70% efficacy rate [Questo trattamento ha un’efficacia del 70%] |
| UNI | This treatment has 30% efficacy rate [Questo trattamento ha un’efficacia del 30%] |
| UNI | This is a possible course of treatment [Questo è un possibile trattamento] |
| UNI | The standard treatment for this tumor has adverse side effects [Il trattamento per questo tumore ha degli effetti collaterali] |
| UNI | The probability of adverse side effects relating to the treatment is 1 in 100,000 [La probabilità di effetti collaterali associati al trattamento per questo tumore è di 1 su 100,000] |
| UNI | The probability of adverse side effects relating to the treatment is 1 in 100 [La probabilità di effetti collaterali associati al trattamento per questo tumore è di 1 su 100] |
| UNI | The adverse side effects related to the standard treatment for this tumor usually appear 1 day after treatment [Gli effetti collaterali associati al trattamento per questo tumore generalmente appaiono un giorno dopo il trattamento] |
| UNI | The adverse side effects related to the standard treatment for this tumor usually appear years after treatment [Gli effetti collaterali associati al trattamento per questo tumore generalmente appaiono diversi anni dopo il trattamento] |
| UNI | The duration of the adverse side effects related to the standard treatment varies over time [Gli effetti collaterali associati al trattamento per questo tumore hanno una durata variabile nel tempo] |
| UNI | This treatment takes 15 days to complete [Il trattamento si completa in 15 giorni] |
| UNI | This treatment takes 1 year to complete [Il trattamento si completa in 1 anno] |
| UNI | This treatment is administered in cycles [Il trattamento è somministrato in cicli] |
| UNI | This treatment is administered in a medical facility [Il trattamento è somministrato in una struttura ospedaliera] |
| UNI | During treatment, assistance might or might not be required [Durante il trattamento qualcuno ha, qualcun altro non ha bisogno di assistenza] |
| UNI | Once the whole treatment cycle is completed, assistance might or might not be required [Una volta che il trattamento è completato qualcuno ha, qualcun altro non ha bisogno di assistenza] |
| UNI | During treatment, your lifestyle might or might not be affected [Durante il trattamento il tuo stile di vita potrebbe subire dei cambiamenti (qualcuno riesce a fare la vita che faceva prima, qualche altro no)] |
| UNI | After treatment is completed, your lifestyle might or might not change from what it was prior to the disease [Dopo il trattamento il tuo stile di vita potrebbe subire dei cambiamenti rispetto a com’era prima della malattia (qualcuno riesce a fare la vita che faceva prima, qualche altro no)] |
| UNI | The treatment might or not impact on your ability to work (during the treatment phase) [Il trattamento, mentre lo fai, potrebbe influire sulla tua possibilità di andare a lavorare (qualcuno durante il trattamento non riesce ad andare a lavorare, qualcuno invece sì)] |
| UNI | Once the entire treatment cycle is completed, the treatment might or not impact on your ability to work… [Una volta che l’intero ciclo di trattamento è finito, potresti avere (ma anche no) ripercussioni sulla tua attività lavorativa (qualcuno non riesce ad tornare a lavorare come prima, qualcuno invece sì)] |
Abbreviations: BIP, bipolar; MRI, magnetic resonance imaging; UNI, unipolar.