

Abstract
Introduction
Facial anthropometric measurement is considered an essential concern of surgeons, orthodontists, artists and forensic scientists. The aim of this study is to investigate facial anthropometric norms of the young Iranian population.
Methods
The study participants consisted of 200 healthy Iranian students (100 males, 100 females) aged 18–25 years old. Twenty-three liner and four angular measurements were investigated twice by a dentist. Independent-samples t test was used to compare indices between males and females and also between countries. A p value less than 0.05 was considered statistically significant.
Results
It was found that the mean measurements of c’–sn’ of both sides, nasolabial angle, trichion–gnathion, tragion–tragion and gnathion–gnathion were statistically greater in Iranian males than in females (p < 0.05). Comparing Iranian anthropometric norms with North American Whites, Malays, Turkish and African American women demonstrated that there were statistically significant differences in most anthropometric measurements between Iranians and other populations (p < 0.05).
Conclusion
In Iranians, mean measurements of c’–sn’ of the right and left sides, nasolabial angle, trichion–gnathion, tragion–tragion and gnathion–gnathion were greater in men than in women. Comparing Iranian males and females with different ethnicities indicated several interracial differences, which should be taken into consideration when dealing with patients or also practitioners originated in this region.
Keywords: Anthropometry, Anthropometric norms, Face, Facial
Introduction
One of the major components of orthodontic diagnosis and treatment planning is the evaluation of the patient’s soft tissue profile and detecting departures from the defined norm [1–4]. Knowledge of the normal dentofacial pattern allows the clinician to make correct decisions and enhance treatment success in establishing optimal facial harmony [5, 6]. There have been suggestions for the evaluation of the face both to check the changes induced by the growth or orthodontic treatment, or simply for aesthetic evaluation [6]. Overlooking the esthetics may lead to dissatisfaction of surgeons and patients who are increasingly becoming esthetic-obsessed [4, 7–9]. This indicates a strong need to establish the anthropometric norms in different races to become able to provide better treatments addressing both functional and esthetic needs of patients [2, 4, 5, 10].
Anthropometry is the direct measurement of human body parts [11, 12]. Facial anthropometry measurements could be used in reconstructive and plastic surgeries, orthogenetic surgeries, orthodontic treatments, art and forensic investigations [13]. Most classical norms have been derived from populations with European/American ancestries [3, 5, 14]. Anthropometric measurements derived from Northern American Whites (NAW) is considered as a normal reference in treatments of Iranian population in reconstructive surgery of craniomaxillofacial deformity, facial congenital abnormality, trauma of accident, plastic surgery and orthodontic treatment [15]. However, no ethnical study might be generalized to other races [1, 3, 4, 10, 16–21]. Anthropometric measurements depend on genetic and environmental factors, so it is essential to determine the specific baseline for different races [22–26]. Therefore, anthropometric norms of a race may not be ideal for diagnosis and treatment planning of patients from other racial backgrounds [3–5]. Esthetic surgical and orthodontic treatments should then aim for standards only with considering each race separately and while bearing in mind the opinions of patients [3–5]. One of the essential concerns of maxillofacial surgeons and orthodontists is facial morphology [27]. The beauty of face is a result of harmony between different parts of face [27]. The findings indicate a considerable difference between populations [1, 3, 5, 10, 14, 16, 18, 28–32]. Moreover, most of earlier studies [1, 10, 14, 16, 18, 28–32] are performed on cephalographs [4], and the measurements of soft tissue profiles have played a small part in the majority of the previous studies, and substantial studies on this issue are lacking [3]. Analysis of the soft tissue profile has the benefit of assessing the external appearance and therefore is more relevant to the treatment outcome perceived by an observer [5]. Besides, X-ray exposure for merely research purposes can raise ethical concerns [4]. It was shown that anthropometric measurements are more reliable than photography and paraclinical approaches like cephalometry, computed tomography and magnetic resonance imaging together with anthropometry measurement could be used to achieve better treatment planning in plastic and reconstructive surgeries [11, 12, 15, 33, 34].
Although esthetic surgeries and orthodontic treatments are extremely frequent in Iran, studies regarding direct anthropometric measurements on Iranians are lacking [35]. Furthermore, it can be valuable to compare a population norm with several other ethnicities [3]. Therefore, the aim of this study was to evaluate Iranian anthropometric norms directly in a comprehensive study and compare our results with other ethnicities.
Materials and Methods
The study participants consisted of 200 healthy Iranian students with equal number of males and females and aged between 18 and 25 years. The study group was chosen from students because they were from different geographic parts of Iran. The inclusion criteria included: systematic health, normal growth of maxilla and mandible, class I occlusion, no history of trauma and accident, no history of plastic, reconstructive and orthognathic surgeries, no history of congenital abnormalities, no history of facial tumor, no history of craniomaxillofacial deformity, and no history of orthodontics and prosthodontics treatments. The measurements were taken with a digital caliper [Mitutoyo# 505-635-50, Tokyo, Japan] [Fig. 1] and a protractor rapporteur [transportador, General #29] [Fig. 2].
Fig. 1.
Measurement device: caliper [Mitutoyo# 505-635-50, Tokyo, Japan]
Fig. 2.
Measurement devise: protractor rapporteur transportador [General # 29]
Based on previous literature [11, 12], 22 landmarks (Figs. 3, 4, 5) were pointed on the facial skin (Figs. 1, 2). Then 23 liner and 4 angular measurements in each participant were investigated twice by one dentist, and their mean values reported. Anthropometric landmarks were:
Head: trichion (tr)
Face: zygion (zy), nasion (n), subnasale (sn), gnathion (gn), glabella (g), gonion (go)
Eye: endocanthion (en), exocanthion (ex), palpebrale superius (ps) and palpebrale inferius (pi) on the eye
Nose: alare (al) and pronasale (prn), alare curvature (ac), the point at the top of each columella crest (c’), subnasale’ (sn’)
Orolabial Region: cheilion (ch), labiale (or labrale) superius (ls) and labiale (or labrale) inferius (li) on the orolabial region, stomion (sto)
Ear: superaurale (sa), subaurale (sba), tragion (t)
Fig. 3.
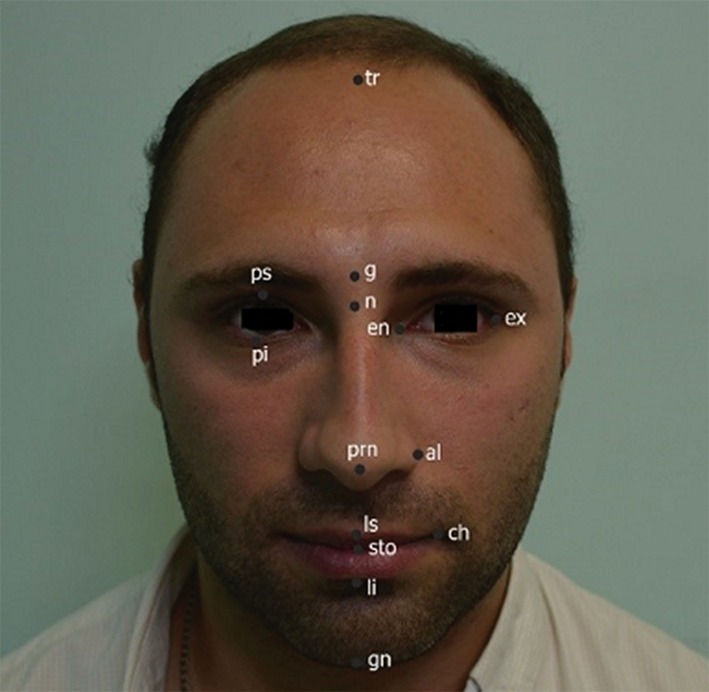
Anatomic point: trichion (tr), gelabella (g), nasion (n), gnathion (gn), endocanthion (en), exocanathion (ex), palpebrale superius (ps), palpebrale inferius (pi), alare (al), pronasale (prn), cheilion (ch), labiale superius (ls), labiale inferius (li), stomion (sto)
Fig. 4.

Anatomic points: zygion (zy), gonion (go), tragion (t), superaurale (sa), subaurale (sba)
Fig. 5.
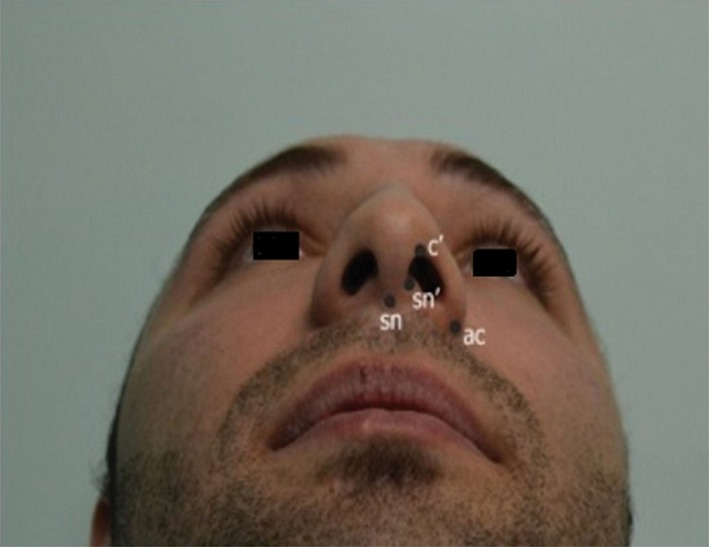
Anatomic points: subnasale (sn), sn’, c’
Liner measurments were:
tragion–tragion (t–t)
trichion–gelabella (tr–g)
trichion–nasion (tr–n)
trichion–gnathion (tr–gn)
nasion–gnathion (n–gn)
subnasale–nasion (sn–n)
zygion–zygion (zy–zy)
gonion–gonion (go–go)
endocanthion–endocanthion (en–en)
exocanthion–exocanthion (ex–ex)
endocanthion–exocanthion of right side (en–ex-r)
palpebrale inferius–superius of right side (ps–pi-r)
Endocanthion–exocanthion of left side (en–ex-l)
palpebrale inferius–superius of left side (ps–pi-l)
alare–alare (al–al)
nasion–subnasale (n–sn)
alare curvature–alare curvature (ac–ac)
columella–sub nasale of right side (c’–sn’-r)
columella–sub nasale of left side (c’–sn’-l)
cheilion–cheilion (ch–ch)
stomion–labiale superius (aso–ls)
stomion–labiale inferius (sto–li)
superaurale, subaurale (sa–sab)
Angular measurments:
Inclination of nasal bridge
Foronto nasal angle
Nasolabial angle
Laibomental angle
Statistical Analysis
Data are presented as mean and standard deviation for numerical variables. Independent-samples t test was used to compare indices between males and females and also between countries. All statistical tests were two sided. A p value less than 0.05 was considered statistically significant.
Results
The facial anthropometric norms of the young Iranian population are shown in Table 1. It was seen that the mean measurements of c’–sn’ of the right and left sides, nasolabial angle, trichion–gnathion, tragion–tragion and gnathion–gnathion were statistically greater in males than in females (p < 0.05).
Table 1.
Craniofacial anthropometric norms of the face, orbit, nose, orolabial and ears of the young Iranian population
| Variable | Male (n = 100) | Female (n = 100) | p | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Min | Max | Mean | SD | Min | Max | ||
| t–t | 168.58 | 6.84 | 155 | 182.61 | 159.51 | 10.70 | 189.72 | 100 | 0.000 |
| tr–g | 51.81 | 7.01 | 32.45 | 67.46 | 53.00 | 8.37 | 40.31 | 99.79 | 0.476 |
| tr–n | 65.07 | 10.10 | 47.96 | 85.35 | 63.25 | 8.5 | 42.59 | 88.28 | 0.317 |
| tr–gn | 191.8 | 6.08 | 181 | 200 | 176.2 | 7.26 | 165 | 190 | 0.000 |
| n–gn | 122.7 | 10.12 | 101 | 134 | 116 | 7.601 | 105 | 132 | 0.111 |
| sn–gn | 76.5 | 9.68 | 60 | 92 | 66.6 | 5.29 | 56 | 76 | 0.011 |
| zy–zy | 130.9 | 4.43 | 122 | 138 | 127.2 | 4.18 | 121 | 134 | 0.071 |
| go–go | 111.9 | 6.72 | 56 | 68 | 97.2 | 13.64 | 56 | 65 | 0.007 |
| en–en | 30.01 | 3.02 | 23.99 | 35.23 | 28.73 | 4.12 | 18.45 | 39.91 | 0.11 |
| ex–ex | 92.59 | 4.8 | 82.32 | 102.37 | 80.19 | 6.47 | 67.03 | 102.63 | 0.6 |
| ex–en-right | 29.55 | 4.69 | 15.26 | 37.70 | 29.54 | 3.90 | 19.50 | 37.85 | 0.983 |
| pi–ps-rt | 13 | 2.88 | 8.69 | 22.68 | 12.93 | 2.12 | 9.79 | 26 | 0.886 |
| ex–en-left | 28.93 | 4.73 | 9.73 | 36.81 | 28.93 | 4.28 | 12.25 | 37 | 0.94 |
| pi–ps-left | 14.96 | 6.86 | 9.26 | 15.45 | 14.01 | 4.8 | 10.22 | 49.78 | 0.384 |
| al–al | 33.10 | 4.9 | 23.16 | 40.30 | 30.11 | 5.67 | 4.50 | 38.46 | 0.09 |
| n–sn | 47.35 | 9.77 | 67.67 | 20.95 | 46.09 | 6.75 | 20.95 | 70.99 | 0.25 |
| ac–ac | 30.30 | 7.80 | 18.78 | 48.51 | 29.50 | 5.40 | 40 | 12.73 | 0.512 |
| c’–sn’-right | 7.19 | 2.20 | 4.15 | 12.15 | 6.17 | 1.49 | 2.95 | 9.28 | 0.03 |
| c’–sn’-left | 7.05 | 2.29 | 3.81 | 14.37 | 6.15 | 1.64 | 10.38 | 2.95 | 0.016 |
| Inclination of nasal bridge | 39.19 | 12.5 | 21 | 65 | 36.81 | 11.91 | 13 | 68 | 0.337 |
| Foronto nasal angle | 153.52 | 14 | 120 | 180 | 156.16 | 10.99 | 64 | 169 | 0.27 |
| Nasolabial angle | 87.30 | 14.27 | 58.09 | 120 | 78.32 | 14.14 | 17.92 | 100 | 0.002 |
| ch–ch | 44.31 | 11.33 | 19.16 | 68.25 | 49.12 | 17.67 | 18.37 | 63 | 0.264 |
| sto–is | 29.65 | 2.36 | 15.34 | 25.53 | 20.47 | 7.45 | 6.12 | 30.95 | 0.898 |
| li–sto | 71.06 | 17.35 | 51.37 | 152.72 | 69.14 | 10.14 | 42.07 | 142.72 | 0.444 |
| Laibomental angle | 87.16 | 17.85 | 53 | 142 | 84.61 | 17.68 | 44 | 150 | 0.484 |
| sa–sab | 61.10 | 4.25 | 104 | 122 | 58.50 | 3.47 | 65 | 114 | 0.152 |
Table 2 demonstrates comparison of anthropometric measurements of the young Iranian males and females with North American Whites (NAW) [22], Turks [33], Malays [36] and African American women [15]. Regarding comparison with Turks [33], it can be noted that all measurements had statistically significant differences except n–gn, al–al, sa–sab in females and n–gn in males (p < 0.05). Regarding comparison with Malays [36], all measurements had statistically significant differences except sa–sab in females, and ex–ex and ex–en in both genders (p < 0.05). African American women [15] had statistically significant differences with Iranians except sn–gn and n–sn (p < 0.05). Comparison between Iranian young adult and NAW showed that n–gn of males and n–sn of females are similar in two populations, but other landmarks had statistically significant differences (p < 0.05).
Table 2.
Comparison of anthropometric measurements of young Iranian population with those of NAW, Malays, Turkish and African American woman
| Variables | Iran | NAW [8] N = 2693 |
Malays [22] | Turkish [23] | African American woman [4] | ||||
|---|---|---|---|---|---|---|---|---|---|
| Male (n = 100) | Female (n = 100) | Male | Female | Male (n = 50) | Female (n = 50) | Male (n = 90) | Female (n = 83) | Female (n = 108) | |
| tr–n | 65.0780 (10.1) | 63.2573 (8.50) | 61.3 (8.9)** | 65.7 (8)* | 68.9 (7.1)*** | ||||
| tr–gn | 191.80 (6.08) | 176.20 (7.26) | 187.2 (12.1)*** | 173.3 (7.8)*** | |||||
| n–gn | 122.7 (10.122) | 116 (7.601) | 121.3 (6.8) | 112 (4.7)*** | 119.3 (6.2)* | 111.8 (5.8)*** | 122.6 (6.0) | 113.4 (6.2)* | |
| sn–gn | 76.5 (9.687) | 66.6 (5.296) | 72.6 (4.5)*** | 64.3 (4)*** | 68.5 (5.2)*** | 63.2 (4.7)*** | 68.0 (6.6)*** | 63.0 (4.5)*** | 67 (4.6) |
| zy–zy | 130.9 (4.433) | 127.2 (4.185 | 139.1 (6.3)*** | 131.1 (5.3)*** | 132.5 (7)*** | 140.1 (4.9)*** | 120.7 (0.1)*** | 113.5 (9.2)*** | 135 (5.3)*** |
| go–go | 122 (6.724) | 97.2 (13.64) | 105.6 (6.7)** | 94.5 (5) | 116.5 (8.4)*** | 110.5 (7.7)*** | |||
| en–en | 30.01 (3.02) | 28.73 (4.12) | 32.9 (2.7)*** | 32.5 (2.4)*** | 33.9 (1.9)** | 32.5 (1.7)*** | 30.4 (3.5)** | 30.3 (2.8)*** | 31.4 (2.6) |
| ex–ex | 92.59 (4.83) | 90.19 (6.47) | 890.7 (3.8)** | 87.6 (4)*** | 92.3 (4.1) | 89.6 (3.2) | |||
| ex–en–right | 29.55 (4.69) | 29.54 (3.90) | 31.2 (1.4)*** | 30.7 (2.2)** | 29.5 (1.5) | 28.7 (1.4) | 34.9 (2.9)*** | 33.9 (2.3)*** | 32.1 (1.8)*** |
| ex–en–left | 28.93 (4.73) | 29.00 (4.28) | 34.4 (2.9)*** | 33.5 (2.4)*** | |||||
| pi-ps-left | 14.96 (6.86) | 14.01 (4.81) | 10.2 (1)*** | 10 (1.1)*** | |||||
| al–al | 33.10 (4.90) | 30.11 (5.67) | 34.8 (2.7)*** | 31.9 (1.9)** | 41 (2)** | 37.3 (2.6)*** | 37.0 (4.0)** | 32.7 (2.8) | |
| n–sn | 47.35 (9.77) | 49.09 (6.75) | 58.2 (3.3)*** | 49.2 (2.9) | 51.6 (3.5)*** | 54.1 (2.9)*** | 56.3 (4.4)*** | 52.8 (3.5)*** | 48 (4.0) |
| Inclination of nasal bridge | 39.19 (12.5) | 36.81 (11.9) | 38.91 (4.7)*** | ||||||
| ch–ch | 44.31 (11.3) | 48.12 (17.6) | 51.6 (3.4)*** | ||||||
| sa–sab | 61.1 (4.254) | 58.5 (3.47) | 62.4 (3.7)** | 59 (3.9) | 63.2 (3.7)*** | 61.2 (4.3)*** | 57.4 (3.9)* | ||
* p < 0.05; ** p < 0.01; *** p < 0.001
Discussion
The first investigation of facial soft tissue was done by the ancient Greeks. After that, it was used in anatomy, art and surgery. Function and beauty of face are results of harmony among lips, nose, and width and height of face [25, 26]. It has been reported in many studies that soft tissue and anthropometric measurements have significant variety in different races [22, 23]. Therefore, it is essential for surgeons and orthodontists to use specific values of each population when planning treatments [11, 15, 37–39]. The appearance plays an important role in esthetic-related fields (plastic, reconstructive, orthogenetic surgeries and orthodontic treatments). Therefore, assessment of correct facial dimensions in treatment planning is necessary [1–4, 7–9, 40].
The present study determined the facial anthropometric dimensions of the young Iranian population, according to direct clinical measurements which can be more reliable than photography and cephalometry [39, 41]. In the current study, it was found that the mean measurements of c’–sn’ of both sides, nasolabial angle, trichion–gnathion, tragion–tragion, and gnathion–gnathion were statistically greater in Iranian males than those of females. The mean values of all measurement were bigger in males except frontonasal angle, tr–g, and ch–ch. Amini et al. [35] investigated anthropometric linear measurements of a group of 100 normal adults in Tehran, Iran, with a method similar to this study. The intercanthal width in Amini et al’s [35] study was almost one third of the biocular width, similar to results of the present study. Observations of Arslan et al. [33] who studied a group of young Turkish population, demonstrated that the mean values of all measurements for men were greater than women, although tr–n and tr–g were greater in females. In Turks, males were similar to females regarding maxillary prognathism, lower lip protrusion, vertical height ratio, lower vertical height–depth ratio, and vertical lip–chin ratio. Turk men had upper lips that were more protruded than women’s upper lips [42]. These differences varied in pattern among white Americans, showing no differences between facial convexity and nasolabial angle, position of lips, and vertical position of lips between nose and chin of American white men and women. Instead, American males had more protruded maxillae and mandibles, and had bigger chins [42]. The study of craniofacial anthropometric norms of the Malays [36] similar to the present findings, demonstrated that the n–gn, n–sto, sn–gn, en–en, ex–en, ex–ex, sa–sab measurements were greater in males. Iranian population had significant differences in many landmarks with NAW [22], Turks [33], Malays [36] and African American women [15].
Regarding Iranian females, sn–gn was similar to African American women [15], go–go was similar to the NAW measurements [23], ex–ex and ex–en of right side were about less than 1 mm different than Malays females [36], n–sn was similar to NAW and African American women, and length of ear was similar to Malaysian females. Regarding Iranian males, the mean n–gn was similar to Turkish males [33], and ex–ex and ex–en of right side were similar to Malays [36].
This study was limited by some factors. The inclusion criterion of normal face is not defined in any anthropometric resources, at least when dealing with populations other than the Caucasians from European root. Therefore, finding participants with normal faces was a subjective challenge, and could differ from person to person. The perception of an ideal face is influenced by various factors such as education and socioeconomic status, current fashions, media, geographic areas, age, gender, and profession of patients or judges, and the facial profiles of judges themselves [4, 10, 16–21, 42–44]. In modern societies, a more convex profile with fuller lips in females might be preferable [4, 16, 18], although some studies have shown a trend for males similar to female profiles with fuller lips and more convex profiles, now being introduced as more attractive by fashion magazines [4, 10, 18]. It should be noted that a normal face is not necessarily an esthetically ideal face. An esthetically pleasing ideal face need not only to be normal but also has to be at ranges called perfectly harmonic. On the other hand, a normal face means a broad range of estimations causing a face looking subjectively normal (but not necessarily beautiful), with no discernible disharmony between its facial features, or no excessive departures from population norms in the eye of the evaluator [44]. This makes selection of normal faces even more difficult, as a broad range of facial properties might be tolerated as normal, and there is no need for perfection, in order to consider a facial pattern as normal. We tried to reduce the influence of such sources of error by recruiting a large number of subjects which was much larger than all other few studies on anthropometric measurements. Moreover, unlike most other studies which had used photographic method, in this study, direct measurements were measured twice, which is much more accurate than photography.
Conclusions
In Iranians, mean measurements of c’–sn’ of the right and left sides, nasolabial angle, trichion–gnathion, tragion–tragion and gnathion–gnathion were greater in men than women. Comparing Iranian males and females with different ethnicities indicated several interracial differences, which should be taken into consideration when dealing with patients or also practitioners originated in this region.
Compliance with Ethical Standards
Conflict of interest
Mohammad Bayat, Mahsa Shariati, Fatemeh Rajaeirad,Mir Saeed Yekaninejad, Fatemeh Momen-heravi, Zeinab Davoudmanesh declare that they have no conflict of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
References
- 1.Uysal T, Baysal A, Yagci A, Sigler LM, McNamara JA., Jr Ethnic differences in the soft tissue profiles of Turkish and European-American young adults with normal occlusions and well-balanced faces. Eur J Orthod. 2012;34:296–301. doi: 10.1093/ejo/cjq165. [DOI] [PubMed] [Google Scholar]
- 2.Oshagh M, Salehi P, Pakshir H, Bazyar L, Rakhshan V. Associations between normative and self-perceived orthodontic treatment needs in young-adult dental patients. Korean J Orthod. 2011;41:440–446. doi: 10.4041/kjod.2011.41.6.440. [DOI] [Google Scholar]
- 3.Hwang HS, Kim WS, McNamara JA., Jr Ethnic differences in the soft tissue profile of Korean and European-American adults with normal occlusions and well-balanced faces. Angle Orthod. 2002;72:72–80. doi: 10.1043/0003-3219(2002)072<0072:EDITST>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 4.Khosravanifard B, Rakhshan V, Raeesi E. Factors influencing attractiveness of soft tissue profile. Oral Surg Oral Med Oral Pathol Oral Radiol. 2013;115:29–37. doi: 10.1016/j.oooo.2012.03.021. [DOI] [PubMed] [Google Scholar]
- 5.Hamdan AM. Soft tissue morphology of Jordanian adolescents. Angle Orthod. 2010;80:80–85. doi: 10.2319/010809-17.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Trevisan F, Gil CTLA. Photogrametric and subjective analysis of the facial profile in young subjects with normal occlusion. Revista Dental Press de Ortodontia e Ortopedia Facial. 2006;11:24–35. doi: 10.1590/S1415-54192006000400004. [DOI] [Google Scholar]
- 7.Bowman SJ. More than lip service: facial esthetics in orthodontics. J Am Dent Assoc. 1999;130:1173–1181. doi: 10.14219/jada.archive.1999.0371. [DOI] [PubMed] [Google Scholar]
- 8.Mohajerani H, Karimi F, Mohajerani A, Rakhshan V. Incidence and risk factors of functional upper airway complications of primary esthetic closed rhinoplasty in two residency programs: a 6-month preliminary prospective cohort study. Dent Res J (Isfahan) 2013;10:74–80. doi: 10.4103/1735-3327.111802. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Sobouti F, Rakhshan V, Chiniforush N, Khatami M. Effects of laser-assisted cosmetic smile lift gingivectomy on postoperative bleeding and pain in fixed orthodontic patients: a controlled clinical trial. Prog Orthod. 2014;15:66. doi: 10.1186/s40510-014-0066-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Sforza C, Laino A, D’Alessio R, Grandi G, Tartaglia GM, Ferrario VF. Soft-tissue facial characteristics of attractive and normal adolescent boys and girls. Angle Orthod. 2008;78:799–807. doi: 10.2319/091207-431.1. [DOI] [PubMed] [Google Scholar]
- 11.Farkas LG, Kolar JC. Anthropometrics and art in the aesthetics of women’s faces. Clin Plast Surg. 1987;14:599–616. [PubMed] [Google Scholar]
- 12.Jimenez DF. Craniofacial anthropometry: practical measurement of the head and face for clinical, surgical and research use. Neurosurgery. 1998;43:1254–1255. doi: 10.1097/00006123-199811000-00152. [DOI] [Google Scholar]
- 13.Argyropoulos E, Sassouni V. Comparison of the dentofacial patterns for native Greek and American-Caucasian adolescents. Am J Orthod Dentofacial Orthop. 1989;95:238–249. doi: 10.1016/0889-5406(89)90054-1. [DOI] [PubMed] [Google Scholar]
- 14.Legan HL, Burstone CJ. Soft tissue cephalometric analysis for orthognathic surgery. J Oral Surg. 1980;38:744–751. [PubMed] [Google Scholar]
- 15.Farkas LG, Hreczko TA, Kolar JC, Munro IR. Vertical and horizontal proportions of the face in young adult North American Caucasians. Plast Reconstr Surg. 1985;75:328–337. doi: 10.1097/00006534-198503000-00005. [DOI] [PubMed] [Google Scholar]
- 16.Matoula S, Pancherz H. Skeletofacial morphology of attractive and nonattractive faces. Angle Orthod. 2006;76:204–210. doi: 10.1043/0003-3219(2006)076[0204:SMOAAN]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 17.Mantzikos T. Esthetic soft tissue profile preferences among the Japanese population. Am J Orthod Dentofacial Orthop. 1998;114:1–7. doi: 10.1016/S0889-5406(98)70230-6. [DOI] [PubMed] [Google Scholar]
- 18.Nguyen DD, Turley PK. Changes in the Caucasian male facial profile as depicted in fashion magazines during the twentieth century. Am J Orthod Dentofacial Orthop. 1998;114:208–217. doi: 10.1053/od.1998.v114.a86137. [DOI] [PubMed] [Google Scholar]
- 19.Scavone H, Jr, Trevisan H, Jr, Garib DG, Ferreira FV. Facial profile evaluation in Japanese–Brazilian adults with normal occlusions and well-balanced faces. Am J Orthod Dentofacial Orthop. 2006;129(721):e1–e5. doi: 10.1016/j.ajodo.2005.10.018. [DOI] [PubMed] [Google Scholar]
- 20.Nomura M, Motegi E, Hatch JP, Gakunga PT, Ng’ang’a PM, Rugh JD, et al. Esthetic preferences of European American, Hispanic American, Japanese, and African judges for soft-tissue profiles. Am J Orthod Dentofacial Orthop. 2009;135:S87–S95. doi: 10.1016/j.ajodo.2008.02.019. [DOI] [PubMed] [Google Scholar]
- 21.Turkkahraman H, Gokalp H. Facial profile preferences among various layers of Turkish population. Angle Orthod. 2004;74:640–647. doi: 10.1043/0003-3219(2004)074<0640:FPPAVL>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 22.Porter JP. Anthropometric facial analysis of the African American woman. Arch Facial Plast Surg. 2001;3:191–197. doi: 10.1001/archfaci.3.3.191. [DOI] [PubMed] [Google Scholar]
- 23.Teck Sim RS. Comparison of the aesthetic facial proportions of Southern Chinese and White women. Arch Facial Plast Surg. 2000;2:113–120. doi: 10.1001/archfaci.2.2.113. [DOI] [PubMed] [Google Scholar]
- 24.Dawei W, Guozheng Q, Mingli Z, Farkas LG. Differences in horizontal, neoclassical facial canons in Chinese (Han) and North American Caucasian populations. Aesthetic Plast Surg. 1997;21:265–269. doi: 10.1007/s002669900123. [DOI] [PubMed] [Google Scholar]
- 25.Kasai K, Kanazawa E, Aboshi H, Tuisuva J, Takahashi M, Matsuno M. Comparative study of craniofacial morphology and bite force in Fijians and Japanese. Am J Hum Biol. 1998;10:63–72. doi: 10.1002/(SICI)1520-6300(1998)10:1<63::AID-AJHB8>3.0.CO;2-D. [DOI] [PubMed] [Google Scholar]
- 26.Kasai K, Richards LC, Brown T. Comparative study of craniofacial morphology in Japanese and Australian aboriginal populations. Hum Biol. 1993;65:821–834. [PubMed] [Google Scholar]
- 27.Lehman JA., Jr Soft-tissue manifestations of aesthetic defects of the jaws: diagnosis and treatment. Clin Plast Surg. 1987;14:767–783. [PubMed] [Google Scholar]
- 28.Foster EJ. Profile preferences among diversified groups. Angle Orthod. 1973;43:34–40. doi: 10.1043/0003-3219(1973)043<0034:PPADG>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 29.Erbay EF, Caniklioglu CM. Soft tissue profile in Anatolian Turkish adults: Part II. Comparison of different soft tissue analyses in the evaluation of beauty. Am J Orthod Dentofacial Orthop. 2002;121:65–72. doi: 10.1067/mod.2002.119573. [DOI] [PubMed] [Google Scholar]
- 30.Czarnecki ST, Nanda RS, Currier GF. Perceptions of a balanced facial profile. Am J Orthod Dentofacial Orthop. 1993;104:180–187. doi: 10.1016/S0889-5406(05)81008-X. [DOI] [PubMed] [Google Scholar]
- 31.Al-Gunaid T, Yamada K, Yamaki M, Saito I. Soft-tissue cephalometric norms in Yemeni men. Am J Orthod Dentofacial Orthop. 2007;132(576):e7–e14. doi: 10.1016/j.ajodo.2007.03.018. [DOI] [PubMed] [Google Scholar]
- 32.Lew KK, Ho KK, Keng SB, Ho KH. Soft-tissue cephalometric norms in Chinese adults with esthetic facial profiles. J Oral Maxillofac Surg. 1992;50:1184–1189. doi: 10.1016/0278-2391(92)90151-O. [DOI] [PubMed] [Google Scholar]
- 33.Arslan SG, Genc C, Odabas B, Kama JD. Comparison of facial proportions and anthropometric norms among Turkish young adults with different face types. Aesthetic Plast Surg. 2008;32:234–242. doi: 10.1007/s00266-007-9049-y. [DOI] [PubMed] [Google Scholar]
- 34.Husein OF, Sepehr A, Garg R, Sina-Khadiv M, Gattu S, Waltzman J, et al. Anthropometric and aesthetic analysis of the Indian American woman’s face. J Plast Reconstr Aesthet Surg. 2010;63:1825–1831. doi: 10.1016/j.bjps.2009.10.032. [DOI] [PubMed] [Google Scholar]
- 35.Amini F, Mashayekhi Z, Rahimi H, Morad G. Craniofacial morphologic parameters in a Persian population. J Craniofac Surg. 2014;25:1874–1881. doi: 10.1097/SCS.0000000000000902. [DOI] [PubMed] [Google Scholar]
- 36.Ngeow WC, Aljunid ST. Craniofacial anthropometric norms of Malaysian Indians. Indian J Dent Res. 2009;20:313. doi: 10.4103/0970-9290.57372. [DOI] [PubMed] [Google Scholar]
- 37.Farkas LG, Katic MJ, Forrest CR. Surface anatomy of the face in Down’s syndrome: age-related changes of anthropometric proportion indices in the craniofacial regions. J Craniofac Surg. 2002;13:368–374. doi: 10.1097/00001665-200205000-00002. [DOI] [PubMed] [Google Scholar]
- 38.Farkas LG, Munro IR, Kolar JC. Abnormal measurements and disproportions in the face of Down’s syndrome patients: preliminary report of an anthropometric study. Plast Reconstr Surg. 1985;75:159–167. doi: 10.1097/00006534-198502000-00002. [DOI] [PubMed] [Google Scholar]
- 39.Arman A, Toygar TU, Abuhijleh E. Profile changes associated with different orthopedic treatment approaches in Class III malocclusions. Angle Orthod. 2004;74:733–740. doi: 10.1043/0003-3219(2004)074<0733:PCAWDO>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 40.Frankel R, Frankel C. Orthodontics in orofacial region with help of function regulators. Inf Orthod Kieferorthop. 1988;20:277–309. [PubMed] [Google Scholar]
- 41.Lundstrom A, Forsberg CM, Peck S, McWilliam J. A proportional analysis of the soft tissue facial profile in young adults with normal occlusion. Angle Orthod. 1992;62:127–133. doi: 10.1043/0003-3219(1992)062<0127:APAOTS>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 42.Uysal T, Baysal A, Yagci A, Sigler LM, McNamara JA Jr. Ethnic differences in the soft tissue profiles of Turkish and European-American young adults with normal occlusions and well-balanced faces. Eur J Orthod. 2012;34(3):296–301. doi: 10.1093/ejo/cjq165. [DOI] [PubMed] [Google Scholar]
- 43.Berneburg M, Dietz K, Niederle C, Goz G. Changes in esthetic standards since 1940. Am J Orthod Dentofacial Orthop. 2010;137(450):e1–e9. doi: 10.1016/j.ajodo.2009.10.029. [DOI] [PubMed] [Google Scholar]
- 44.Sajjadi SH, Khosravanifard B, Moazzami F, Rakhshan V, Esmaeilpour M. Effects of three types of digital camera sensors on dental specialists’ perception of smile esthetics: a preliminary double-blind clinical trial. J Prosthodont. 2015;24:1–7. doi: 10.1111/jopr.12179. [DOI] [PubMed] [Google Scholar]